
Analysis of ABCB1 Gene Polymorphisms and Their Impact on Tacrolimus Blood Levels in Kidney Transplant Recipients
 ,
,
Abstract
1. Introduction
2. Results
2.1. Demographic Data and Gene Frequencies
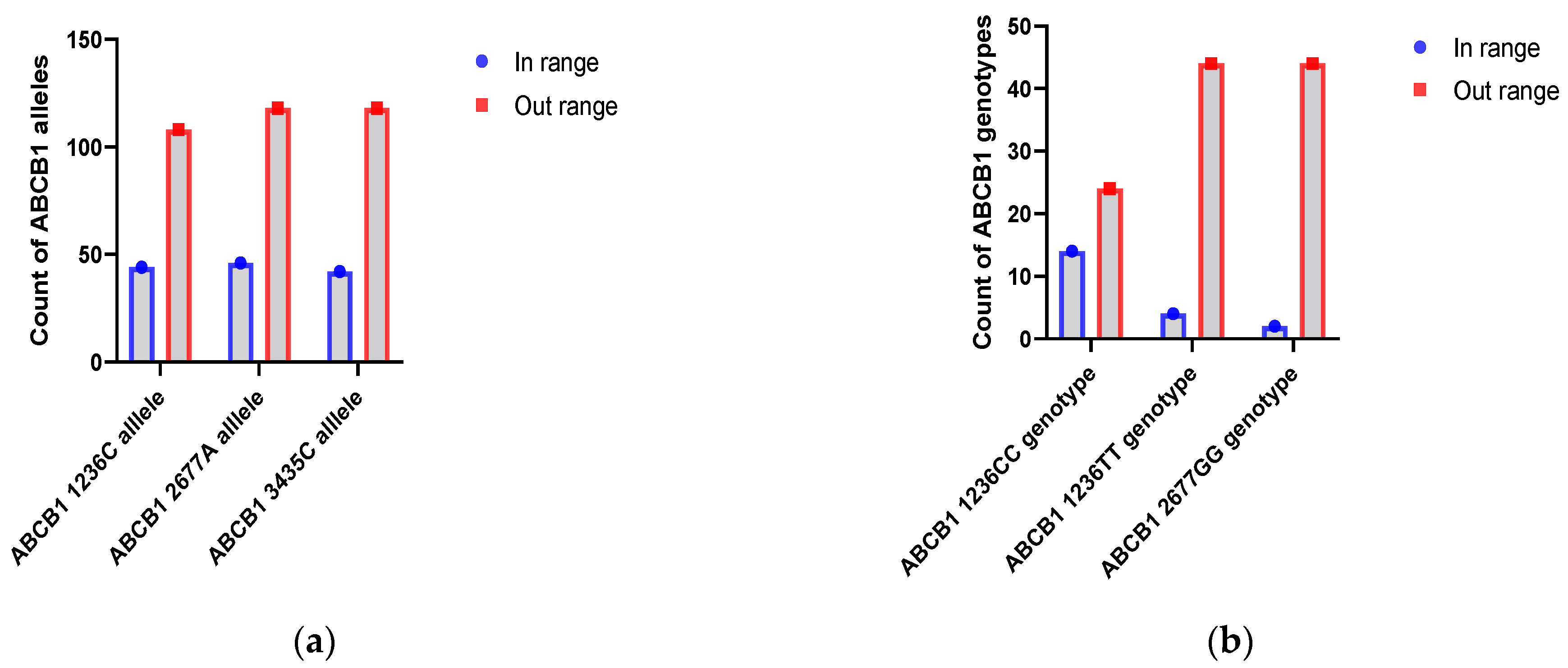
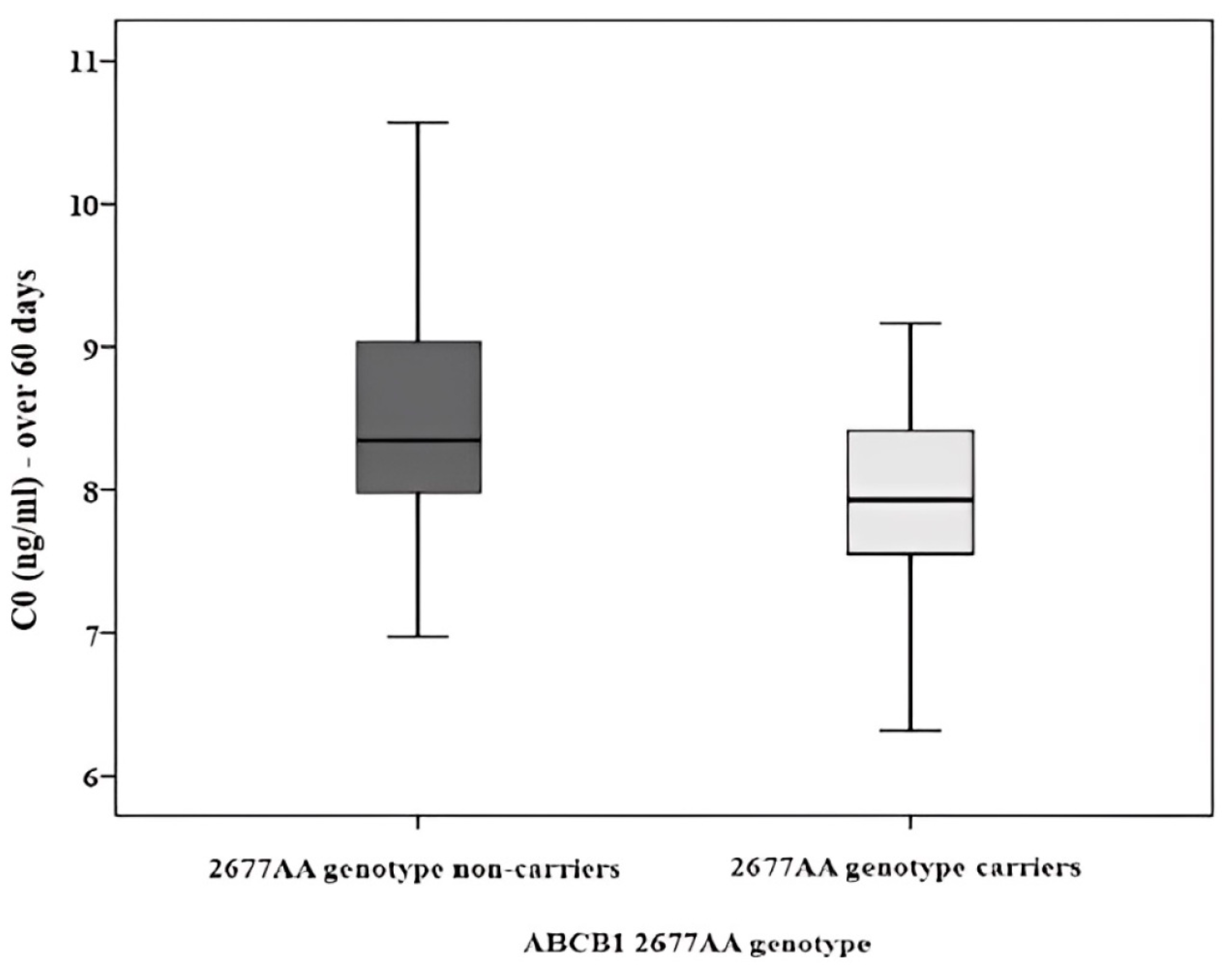
2.2. ABCB1 SNP Alleles and Genotypes Analysis
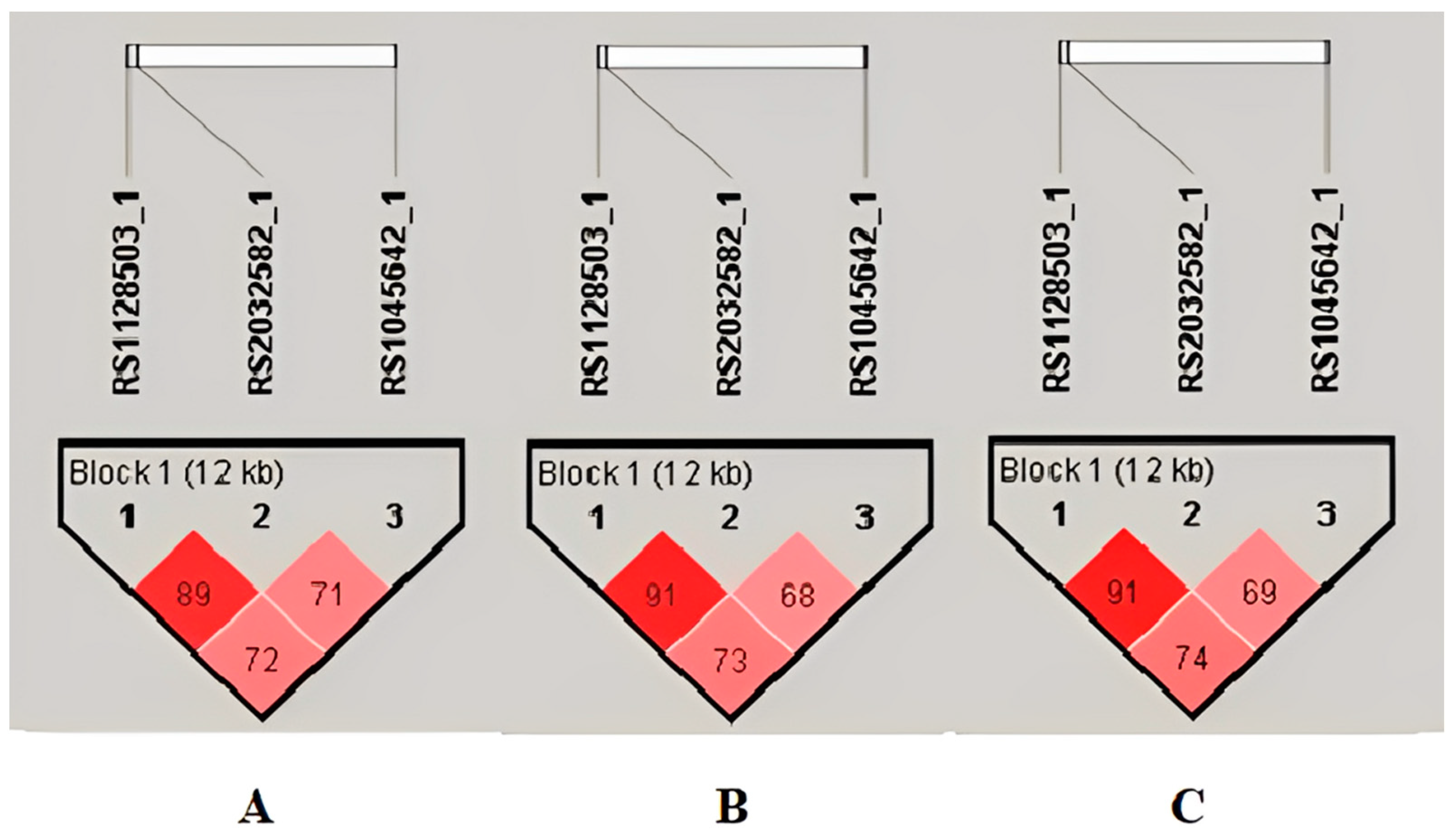
2.3. ABCB1 Haplotypes and Diplotypes Analysis
2.4. Analysis of Tc Variability (C0/Dose Ratio) over Time through Different Mixed-Effects Models
3. Discussion
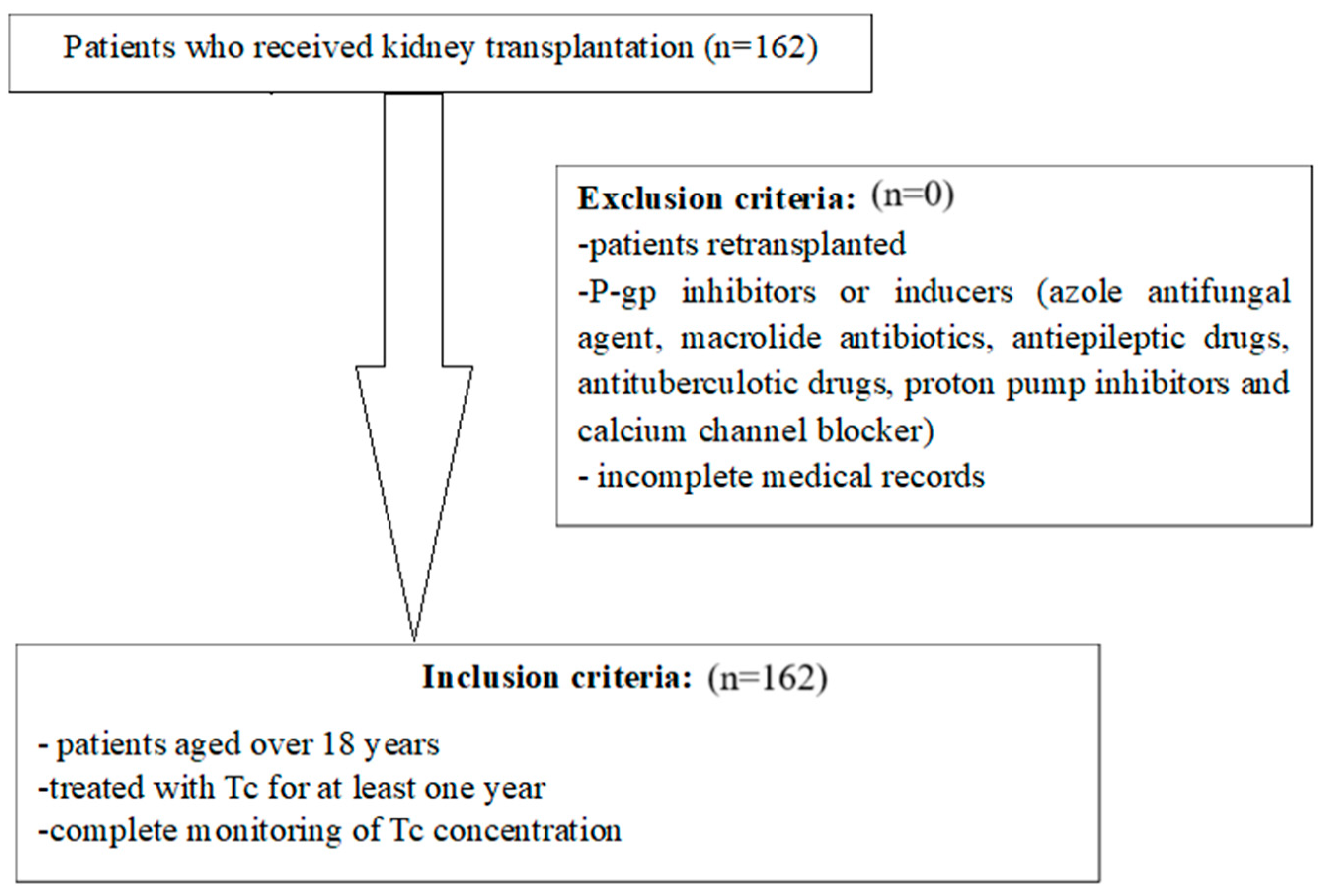
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jager, K.J.; Kovesdy, C.; Langham, R.; Rosenberg, M.; Jha, V.; Zoccali, C. A Single Number for Advocacy and Communication-Worldwide More than 850 Million Individuals Have Kidney Diseases. Kidney Int. 2019, 96, 1048–1050. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Kramer, A.; Jager, K.J. Chronic Kidney Disease and End-Stage Renal Disease-a Review Produced to Contribute to the Report “the Status of Health in the European Union: Towards a Healthier Europe. ” NDT Plus 2010, 3, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, M.F.; Benjamin, O.; Lappin, S.L. End-Stage Renal Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Stevens, L.A.; Li, S.; Wang, C.; Huang, C.; Becker, B.N.; Bomback, A.S.; Brown, W.W.; Burrows, N.R.; Jurkovitz, C.T.; McFarlane, S.I.; et al. Prevalence of CKD and Comorbid Illness in Elderly Patients in the United States: Results from the Kidney Early Evaluation Program (KEEP). Am. J. Kidney Dis. 2010, 55, S23–S33. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Zeier, M.G.; Chapman, J.R.; Craig, J.C.; Ekberg, H.; Garvey, C.A.; Green, M.D.; Jha, V.; Josephson, M.A.; Kiberd, B.A.; et al. KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients: A Summary. Kidney Int. 2010, 77, 299–311. [Google Scholar] [CrossRef]
- Tuteja, S.; Alloway, R.R.; Johnson, J.A.; Gaber, A.O. The Effect of Gut Metabolism on Tacrolimus Bioavailability in Renal Transplant Recipients. Transplantation 2001, 71, 1303–1307. [Google Scholar] [CrossRef]
- Gruber, S.A.; Hewitt, J.M.; Sorenson, A.L.; Barber, D.L.; Bowers, L.; Rynders, G.; Arrazola, L.; Matas, A.J.; Rosenberg, M.E.; Canafax, D.M. Pharmacokinetics of FK506 after Intravenous and Oral Administration in Patients Awaiting Renal Transplantation. J. Clin. Pharmacol. 1994, 34, 859–864. [Google Scholar] [CrossRef]
- Masuda, S.; Goto, M.; Fukatsu, S.; Uesugi, M.; Ogura, Y.; Oike, F.; Kiuchi, T.; Takada, Y.; Tanaka, K.; Inui, K.-I. Intestinal MDR1/ABCB1 Level at Surgery as a Risk Factor of Acute Cellular Rejection in Living-Donor Liver Transplant Patients. Clin. Pharmacol. Ther. 2006, 79, 90–102. [Google Scholar] [CrossRef]
- Ueda, K.; Clark, D.P.; Chen, C.J.; Roninson, I.B.; Gottesman, M.M.; Pastan, I. The Human Multidrug Resistance (MDR1) Gene. cDNA Cloning and Transcription Initiation. J. Biol. Chem. 1987, 262, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Choudhuri, S.; Klaassen, C.D. Structure, Function, Expression, Genomic Organization, and Single Nucleotide Polymorphisms of Human ABCB1 (MDR1), ABCC (MRP), and ABCG2 (BCRP) Efflux Transporters. Int. J. Toxicol. 2006, 25, 231–259. [Google Scholar] [CrossRef]
- Thiebaut, F.; Tsuruo, T.; Hamada, H.; Gottesman, M.M.; Pastan, I.; Willingham, M.C. Cellular Localization of the Multidrug-Resistance Gene Product P-Glycoprotein in Normal Human Tissues. Proc. Natl. Acad. Sci. USA 1987, 84, 7735–7738. [Google Scholar] [CrossRef]
- Tatsuta, T.; Naito, M.; Oh-hara, T.; Sugawara, I.; Tsuruo, T. Functional Involvement of P-Glycoprotein in Blood-Brain Barrier. J. Biol. Chem. 1992, 267, 20383–20391. [Google Scholar] [CrossRef] [PubMed]
- Cordon-Cardo, C.; O’Brien, J.P.; Casals, D.; Rittman-Grauer, L.; Biedler, J.L.; Melamed, M.R.; Bertino, J.R. Multidrug-Resistance Gene (P-Glycoprotein) Is Expressed by Endothelial Cells at Blood-Brain Barrier Sites. Proc. Natl. Acad. Sci. USA 1989, 86, 695–698. [Google Scholar] [CrossRef]
- Andersen, V.; Vogel, U.; Godiksen, S.; Frenzel, F.B.; Sæbø, M.; Hamfjord, J.; Kure, E.; Vogel, L.K. Low ABCB1 Gene Expression Is an Early Event in Colorectal Carcinogenesis. PLoS ONE 2013, 8, e72119. [Google Scholar] [CrossRef]
- He, T.; Mo, A.; Zhang, K.; Liu, L. ABCB1/MDR1 Gene Polymorphism and Colorectal Cancer Risk: A Meta-Analysis of Case-Control Studies. Color. Dis. 2013, 15, 12–18. [Google Scholar] [CrossRef]
- Lee, J.; Huang, H.; Chen, Y.; Lu, X. ABCB1 Haplotype Influences the Sirolimus Dose Requirements in Chinese Renal Transplant Recipients. Biopharm. Drug Dispos. 2014, 35, 164–172. [Google Scholar] [CrossRef]
- Zuo, L.; Wang, K.; Luo, X. Use of Diplotypes—Matched Haplotype Pairs from Homologous Chromosomes—In Gene-Disease Association Studies. Shanghai Arch Psychiatry 2014, 26, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Gümüş-Akay, G.; Rüstemoğlu, A.; Karadağ, A.; Sunguroğlu, A. Haplotype-Based Analysis of MDR1/ABCB1 Gene Polymorphisms in a Turkish Population. DNA Cell Biol. 2010, 29, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Home—SNP—NCBI. Available online: https://www.ncbi.nlm.nih.gov/snp/ (accessed on 24 July 2024).
- Schwab, M.; Eichelbaum, M.; Fromm, M.F. Genetic Polymorphisms of the Human MDR1 Drug Transporter. Annu. Rev. Pharmacol. Toxicol. 2003, 43, 285–307. [Google Scholar] [CrossRef]
- Dey, S. Single Nucleotide Polymorphisms in Human P-Glycoprotein: Its Impact on Drug Delivery and Disposition. Expert Opin. Drug Deliv. 2006, 3, 23–35. [Google Scholar] [CrossRef]
- Sakaeda, T.; Nakamura, T.; Okumura, K. Pharmacogenetics of MDR1 and Its Impact on the Pharmacokinetics and Pharmacodynamics of Drugs. Pharmacogenomics 2003, 4, 397–410. [Google Scholar] [CrossRef]
- Kim, I.-W.; Moon, Y.J.; Ji, E.; Kim, K.I.; Han, N.; Kim, S.J.; Shin, W.G.; Ha, J.; Yoon, J.-H.; Lee, H.S.; et al. Clinical and Genetic Factors Affecting Tacrolimus Trough Levels and Drug-Related Outcomes in Korean Kidney Transplant Recipients. Eur. J. Clin. Pharmacol. 2012, 68, 657–669. [Google Scholar] [CrossRef]
- Fredericks, S.; Moreton, M.; Reboux, S.; Carter, N.D.; Goldberg, L.; Holt, D.W.; MacPhee, I.A.M. Multidrug Resistance Gene-1 (MDR-1) Haplotypes Have a Minor Influence on Tacrolimus Dose Requirements. Transplantation 2006, 82, 705–708. [Google Scholar] [CrossRef]
- Akbas, S.H.; Bilgen, T.; Keser, I.; Tuncer, M.; Yucetin, L.; Tosun, O.; Gultekin, M.; Luleci, G. The Effect of MDR1 (ABCB1) Polymorphism on the Pharmacokinetic of Tacrolimus in Turkish Renal Transplant Recipients. Transplant. Proc. 2006, 38, 1290–1292. [Google Scholar] [CrossRef] [PubMed]
- Provenzani, A.; Notarbartolo, M.; Labbozzetta, M.; Poma, P.; Vizzini, G.; Salis, P.; Caccamo, C.; Bertani, T.; Palazzo, U.; Polidori, P.; et al. Influence of CYP3A5 and ABCB1 Gene Polymorphisms and Other Factors on Tacrolimus Dosing in Caucasian Liver and Kidney Transplant Patients. Int. J. Mol. Med. 2011, 28, 1093–1102. [Google Scholar] [CrossRef]
- Hamzah, S.; Teh, L.K.; Siew, J.S.K.; Ahmad, G.; Wong, H.S.; Zakaria, Z.A.; Salleh, M.Z. Pharmacogenotyping of CYP3A5 in Predicting Dose-Adjusted Trough Levels of Tacrolimus among Malaysian Kidney-Transplant Patients. Can. J. Physiol. Pharmacol. 2014, 92, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.-H.; Yoon, Y.-D.; Park, J.-Y.; Song, E.-J.; Choi, J.-Y.; Yoon, S.-H.; Park, S.-H.; Kim, Y.-L.; Kim, C.-D. Impact of Cytochrome P450 3A and ATP-Binding Cassette Subfamily B Member 1 Polymorphisms on Tacrolimus Dose-Adjusted Trough Concentrations among Korean Renal Transplant Recipients. Transplant. Proc. 2012, 44, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Wallemacq, P.; Goffinet, J.-S.; O’Morchoe, S.; Rosiere, T.; Maine, G.T.; Labalette, M.; Aimo, G.; Dickson, D.; Schmidt, E.; Schwinzer, R.; et al. Multi-Site Analytical Evaluation of the Abbott ARCHITECT Tacrolimus Assay. Ther. Drug Monit. 2009, 31, 198–204. [Google Scholar] [CrossRef]
- Glickman, M.E.; Rao, S.R.; Schultz, M.R. False Discovery Rate Control Is a Recommended Alternative to Bonferroni-Type Adjustments in Health Studies. J. Clin. Epidemiol. 2014, 67, 850–857. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients (n) | 162 | |||
| Age (mean ± standard deviation) | 40.68 ± 11.26 | |||
| Gender (n) | ||||
| Male | 106 (65.4%) | |||
| Female | 56 (34.6%) | |||
| Bodyweight (kg) (mean ± standard deviation) | 69.69 ± 14.85 | |||
| Blood groups (n) | ||||
| A | 74 (45.7%) | |||
| B | 32 (19.7%) | |||
| AB | 18 (11.1%) | |||
| O | 38 (23.5%) | |||
| Type of donor (n) | ||||
| Living donor | 121 (74.7%) | |||
| Cadaveric donor | 41 (25.3%) | |||
| Kidney disease causes (n) | ||||
| Unknown etiology | 67 (41.4%) | |||
| IgA nephropathy | 29 (17.9%) | |||
| Autosomal dominant polycystic kidney | 14 (8.6%) | |||
| Glomerulonephritis | 12 (7.4%) | |||
| Tubulointerstitial disease | 11 (6.8%) | |||
| Alport syndrome | 10 (6.2%) | |||
| Diabetic nephropathy | 8 (4.9%) | |||
| Hypertensive nephropathy | 3 (1.9%) | |||
| Others (LES, ANCA positive vasculitis, Fabry disease, Goodpasture syndrome) | 8 (4.9%) | |||
| Induction therapy (n) | ||||
| Anti-thymocyte globuline | 2 (1.2%) | |||
| Basiliximab | 160 (98.8%) | |||
| Characteristics over time (mean ± standard deviation) | 1–14 days | 15–30 days | 31–60 days | over 60 days |
| Tc C0 (ng/mL) | 12.18 ± 5.42 | 13.55 ± 4.42 | 11.53 ± 3.65 | 8.15 ± 2.91 |
| Tc dose (mg per day) | 12.92 ± 4.19 | 12.43 ± 4.89 | 8.89 ± 4.38 | 4.99 ± 2.56 |
| Tc C0/dose (ng/mL/mg per day) | 1.11 ± 1.20 | 1.29 ± 0.83 | 1.59 ± 0.87 | 1.98 ± 1.12 |
| Tc C0/dose/Bodyweight (ng/mL/mg/kg per day) | 0.016 ± 0.155 | 0.019 ± 0.151 | 0.024 ± 0.015 | 0.029 ± 0.016 |
| eGFR (mL/min/1.73 m2) | 37.87 ± 22.23 | 37.53 ± 21.49 | 43.98 ± 14.76 | 47.29 ± 15.81 |
| Genotype | Total (n = 162) | Allele | Total (n = 324) |
|---|---|---|---|
| ABCB1 3435C>T (rs1045642) CC CT TT | 38 (23.4%) 84 (51.9%) 40 (24.7%) | C T | 244 (75.3%) 80 (24.7%) |
| ABCB1 1236C>T (rs1128503) CC CT TT | 38 (23.5%) 76 (46.9%) 48 (29.6%) | C T | 228 (70.4%) 96 (29.6%) |
| ABCB1 2677G>T/A (rs2032582) GG GA AA GT/TA/TT | 46 (28.5%) 68 (41.9%) 48 (29.6%) 0 (0%) | G A T | 228 (70.4%) 96 (29.6%) 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rotarescu, C.A.; Maruntelu, I.; Rotarescu, I.; Constantinescu, A.-E.; Constantinescu, I. Analysis of ABCB1 Gene Polymorphisms and Their Impact on Tacrolimus Blood Levels in Kidney Transplant Recipients. Int. J. Mol. Sci. 2024, 25, 10999. https://doi.org/10.3390/ijms252010999
Rotarescu CA, Maruntelu I, Rotarescu I, Constantinescu A-E, Constantinescu I. Analysis of ABCB1 Gene Polymorphisms and Their Impact on Tacrolimus Blood Levels in Kidney Transplant Recipients. International Journal of Molecular Sciences. 2024; 25(20):10999. https://doi.org/10.3390/ijms252010999
Chicago/Turabian StyleRotarescu, Corina Andreea, Ion Maruntelu, Ion Rotarescu, Alexandra-Elena Constantinescu, and Ileana Constantinescu. 2024. "Analysis of ABCB1 Gene Polymorphisms and Their Impact on Tacrolimus Blood Levels in Kidney Transplant Recipients" International Journal of Molecular Sciences 25, no. 20: 10999. https://doi.org/10.3390/ijms252010999
APA StyleRotarescu, C. A., Maruntelu, I., Rotarescu, I., Constantinescu, A.-E., & Constantinescu, I. (2024). Analysis of ABCB1 Gene Polymorphisms and Their Impact on Tacrolimus Blood Levels in Kidney Transplant Recipients. International Journal of Molecular Sciences, 25(20), 10999. https://doi.org/10.3390/ijms252010999