

Nanoparticle-Encapsulated Epirubicin Efficacy in the Inhibition of Growth of Orthotopic Ovarian Patient-Derived Xenograft in Immunocompromised Mice


Abstract
1. Introduction
2. Results
2.1. Ex Vivo Cytotoxicity of POLEPI in Champions TumorGraft® and Certis Oncology Solutions PDX Models
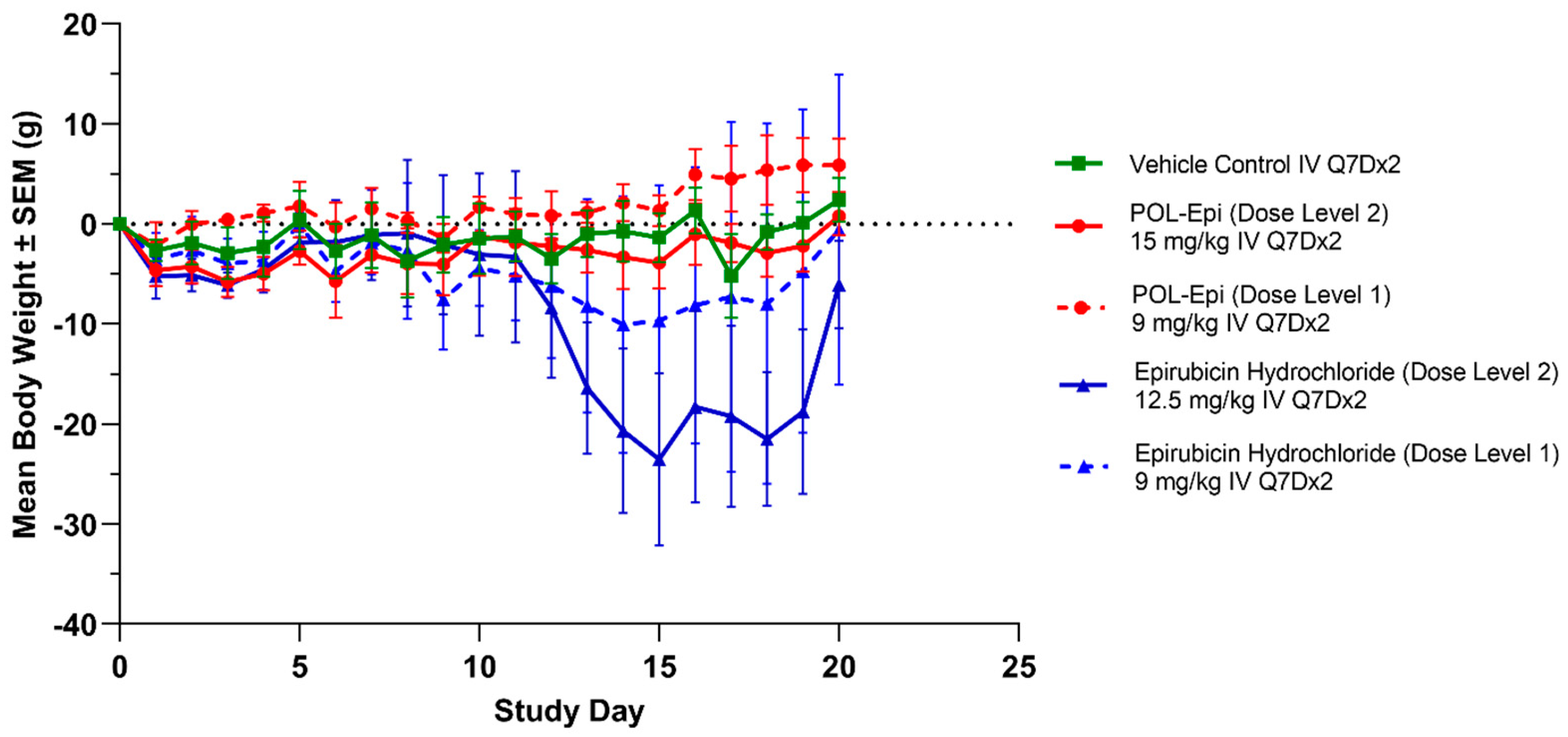
2.2. In Vivo Determination of MTD of POLEPI and EPI in Non-Tumor-Bearing Immunocompromised Mice
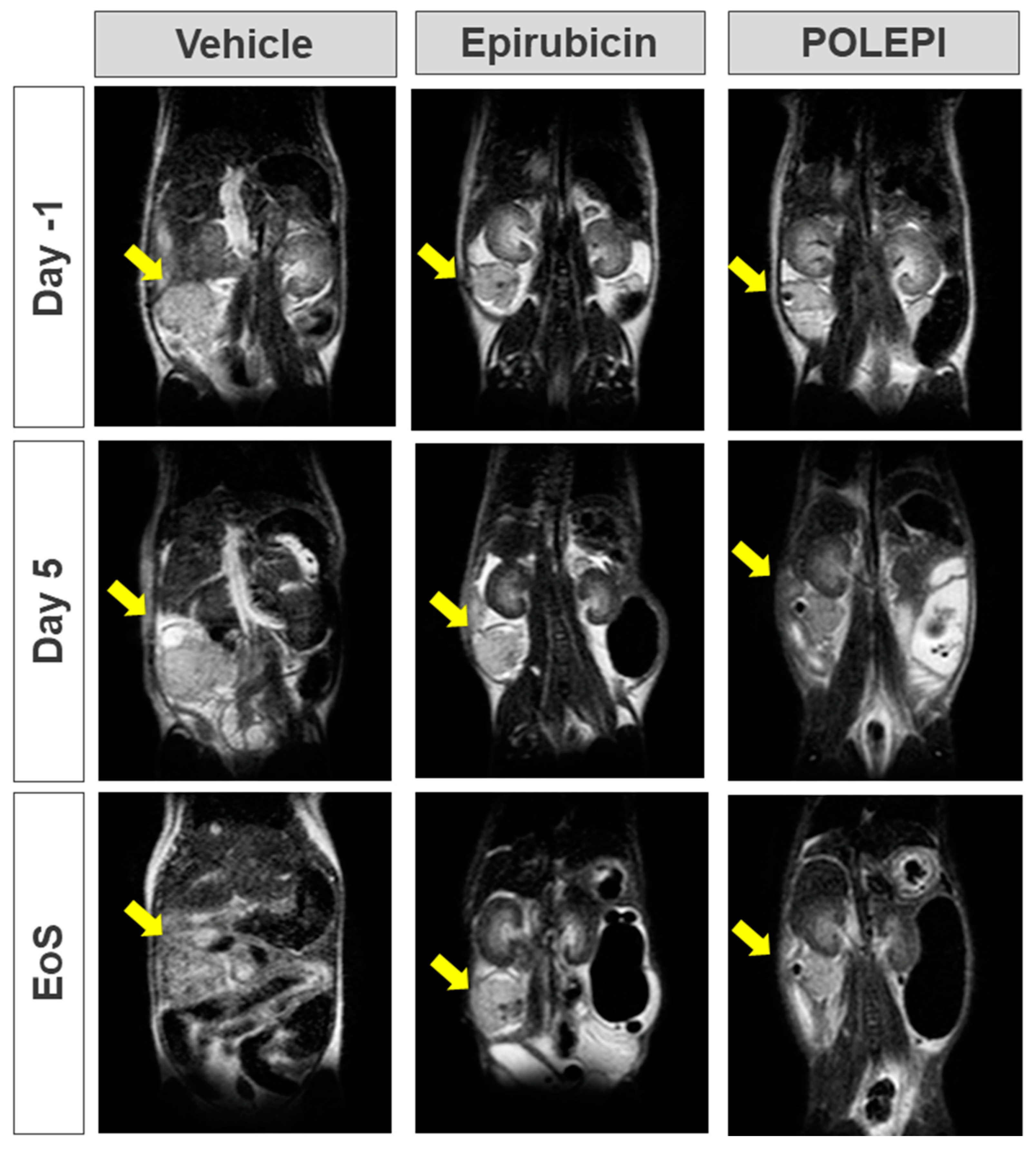
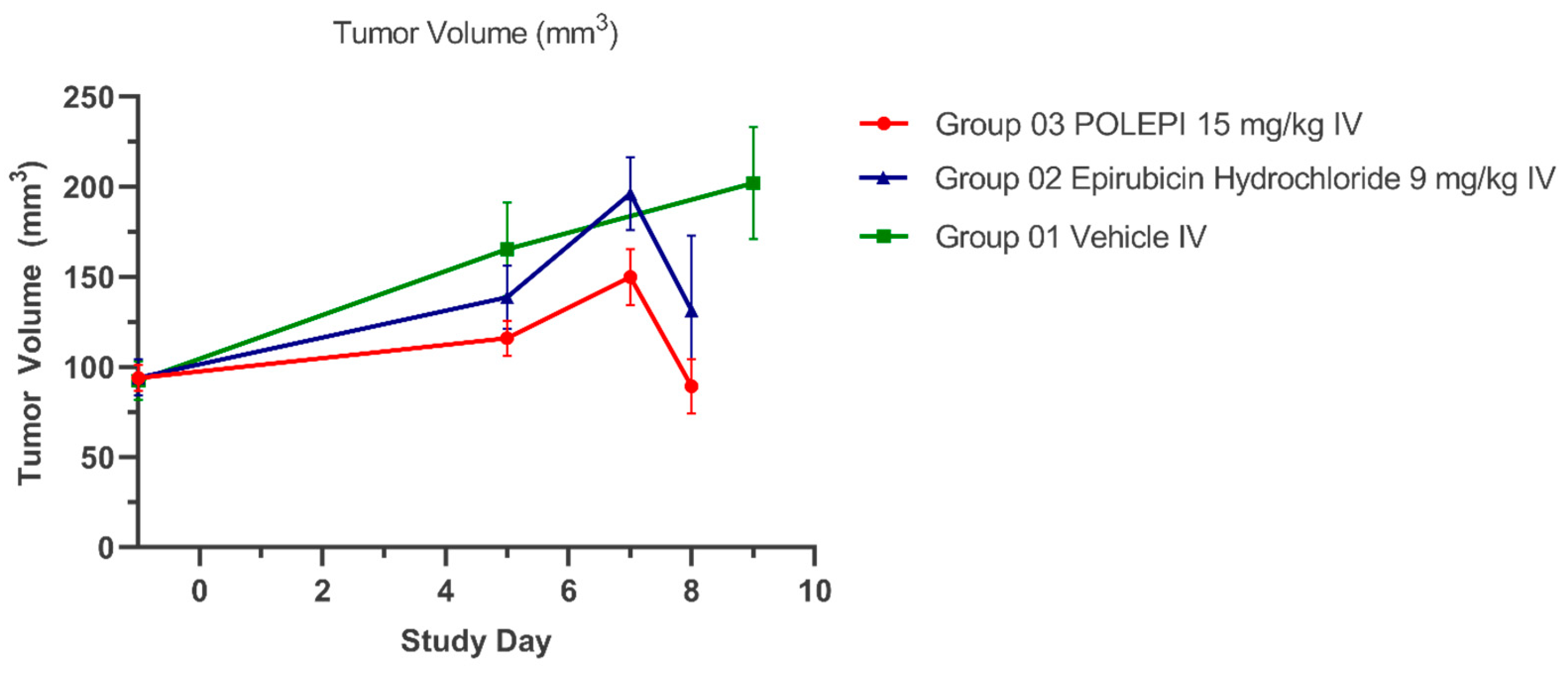
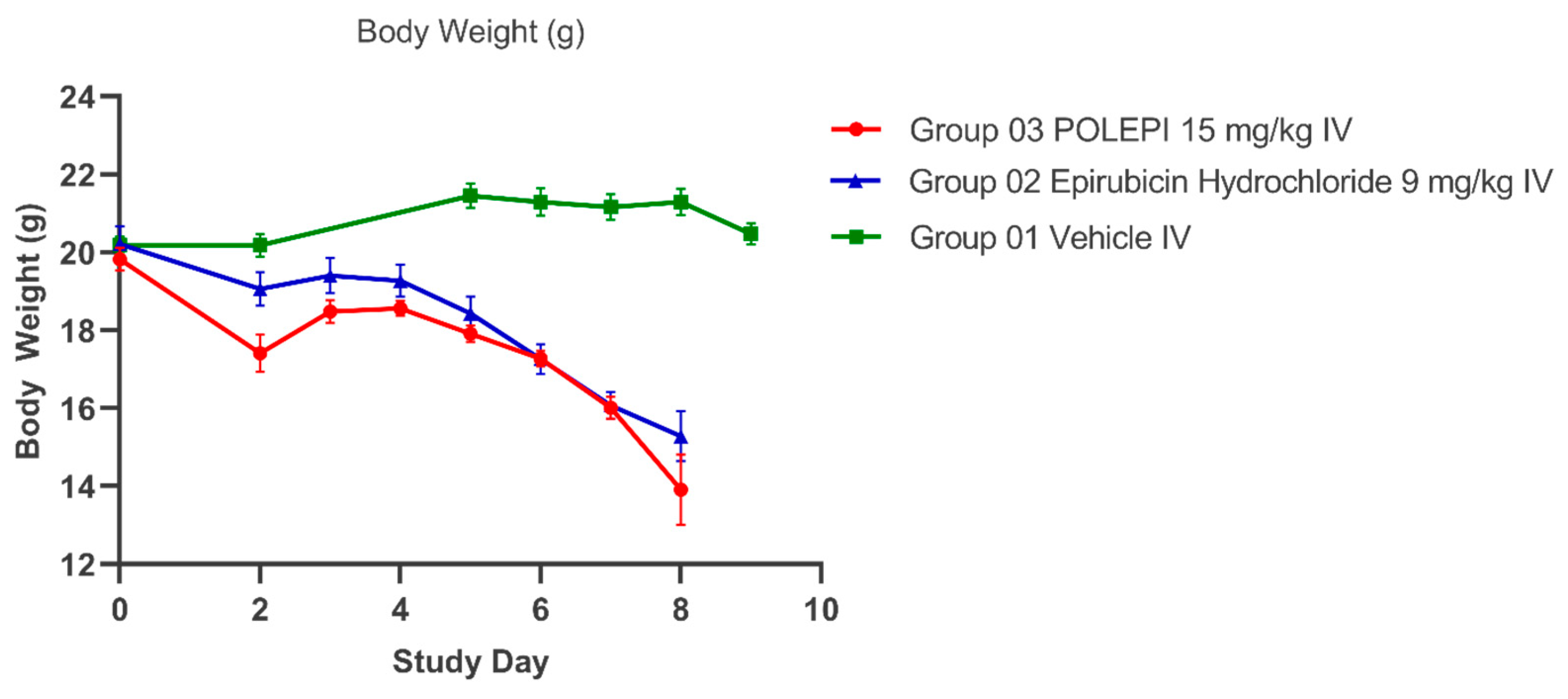
2.3. In Vivo Efficacy of POLEPI in Immunocompromised Mice Bearing Orthotopic Ovarian PDX
3. Discussion
4. Materials and Methods
4.1. Materials
Test Articles Stock and Working Solution Preparation
4.2. Ex Vivo Evaluation of POLEPI and EPI Using Low Passage Champions TumorGraft® Models
4.2.1. Tumor Fragment Assay for the Determination of IC50 Values
4.2.2. Data Analysis and Efficacy Evaluation
4.3. Ex Vivo Evaluation of POLEPI Using Certis Oncology Ovarian PDX for Orthotopic Engrafting
4.4. In Vivo Determination of Maximum Tolerated Dose (MTD) in Non-Tumor-Bearing Immunocompromised Mice
4.5. In Vivo Evaluation of POLEPI in a Certis Oncology Solutions Orthotopic CRT_OV_00367 Model in Immunocompromised Mice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Reid, B.M.; Permuth, J.B.; Sellers, T.A. Epidemiology of ovarian cancer: A review. Cancer Biol. Med. 2017, 14, 9–32. [Google Scholar] [PubMed]
- Momenimovahed, Z.; Tiznobaik, A.; Taheri, S.; Salehiniya, H. Ovarian cancer in the world: Epidemiology and risk factors. Int. J. Womens Health 2019, 11, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef] [PubMed]
- Lheureux, S.; Braunstein, M.; Oza, A.M. Epithelial ovarian cancer: Evolution of management in the era of precision medicine. CA Cancer J. Clin. 2019, 69, 280–304. [Google Scholar] [CrossRef] [PubMed]
- Morand, S.; Devanaboyina, M.; Staats, H.; Stanbery, L.; Nemunaitis, J. Ovarian Cancer Immunotherapy and Personalized Medicine. Int. J. Mol. Sci. 2021, 22, 6532. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Kobierska, A.; Chevallier, B.; Zanaboni, F.; Pawinski, A.; Bolis, G. A phase II study of high-dose epirubicin in ovarian cancer patients previously treated with cisplatin. EORTC Gynecological Cancer Cooperative Group. Ann. Oncol. 2000, 11, 1035–1040. [Google Scholar] [CrossRef]
- Main, C.; Bojke, L.; Griffin, S.; Norman, G.; Barbieri, M.; Mather, L.; Stark, D.; Palmer, S.; Riemsma, R. Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: A systematic review and economic evaluation. Health Technol. Assess. 2006, 10, 1–132. [Google Scholar] [CrossRef]
- Gebbia, V.; Di Marco, P.; Borsellino, N.; Gebbia, N.; Valerio, M.R.; Fallica, G.; Tirrito, M.L.; Valenza, R.; Citarrella, P.; Benedetti Panici, P. Escalating doses of paclitaxel and epirubicin in combination with cisplatin in advanced ovarian epithelial carcinoma: A phase I-II study. Anticancer Drugs 2003, 14, 359–364. [Google Scholar] [CrossRef]
- Johnston, H.; Brown, D.; Kermanizadeh, A.; Gubbins, E.; Stone, V. Investigating the relationship between nanomaterial hazard and physicochemical properties: Informing the exploitation of nanomaterials within therapeutic and diagnostic applications. J. Control. Release 2012, 164, 307–313. [Google Scholar] [CrossRef]
- Dobrovolskaia, M.A.; Aggarwal, P.; Hall, J.B.; McNeil, S.E. Preclinical studies to understand nanoparticle interaction with the immune system and its potential effects on nanoparticle biodistribution. Mol. Pharm. 2008, 5, 487–495. [Google Scholar] [CrossRef]
- Aggarwal, P.; Hall, J.B.; McLeland, C.B.; Dobrovolskaia, M.A.; McNeil, S.E. Nanoparticle interaction with plasma proteins as it relates to particle biodistribution, biocompatibility and therapeutic efficacy. Adv. Drug Deliv. Rev. 2009, 61, 428–437. [Google Scholar] [CrossRef]
- Chen, D.; Ganesh, S.; Wang, W.; Amiji, M. Plasma protein adsorption and biological identity of systemically administered nanoparticles. Nanomedicine 2017, 12, 2113–2135. [Google Scholar] [CrossRef]
- Morales-Cruz, M.; Delgado, Y.; Castillo, B.; Figueroa, C.M.; Molina, A.M.; Torres, A.; Milián, M.; Griebenow, K. Smart Targeting To Improve Cancer Therapeutics. Drug Des. Devel. Ther. 2019, 13, 3753–3772. [Google Scholar] [CrossRef]
- Huang, W.; Yao, F.; Tian, S.; Liu, M.; Liu, G.; Jiang, Y. Recent Advances in Zein-Based Nanocarriers for Precise Cancer Therapy. Pharmaceutics. 2023, 15, 1820. [Google Scholar] [CrossRef]
- Upreti, M.; Jyoti, A.; Sethi, P. Tumor microenvironment and nanotherapeutics. Transl. Cancer Res. 2013, 2, 309–319. [Google Scholar] [PubMed]
- Han, S.; Chi, Y.; Yang, Z.; Ma, J.; Wang, L. Tumor Microenvironment Regulation and Cancer Targeting Therapy Based on Nanoparticles. J. Funct. Biomater. 2023, 14, 136. [Google Scholar] [CrossRef]
- Liberti, M.V.; Locasale, J.W. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem. Sci. 2016, 41, 211–218. [Google Scholar] [CrossRef]
- Yamagishi, J.F.; Hatakeyama, T.S. Microeconomics of Metabolism: The Warburg Effect as Giffen Behaviour. Bull. Math. Biol. 2021, 83, 120. [Google Scholar] [CrossRef]
- Ho, P.C.; Bihuniak, J.D.; Macintyre, A.N.; Staron, M.; Liu, X.; Amezquita, R.; Tsui, Y.C.; Cui, G.; Micevic, G.; Perales, J.C.; et al. Phosphoenolpyruvate Is a Metabolic Checkpoint of Anti-tumor T Cell Responses. Cell 2015, 162, 1217–1228. [Google Scholar] [CrossRef]
- Trzaskowski, M.; Drozd, M.; Ciach, T. Study on Saccharide–Glucose Receptor Interactions with the Use of Surface Plasmon Resonance. Int. J. Mol. Sci. 2023, 24, 16079. [Google Scholar] [CrossRef] [PubMed]
- Feron, O. Pyruvate into lactate and back: From the Warburg effect to symbiotic energy fuel exchange in cancer cells. Radiother. Oncol. 2009, 92, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Danhier, F.; Feron, O.; Préat, V. To exploit the tumor microenvironment: Passive and active tumor targeting of nanocarriers for anti-cancer drug delivery. J. Control. Release 2010, 148, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Wasiak, I.; Kulikowska, A.; Janczewska, M.; Michalak, M.; Cymerman, I.A.; Nagalski, A.; Kallinger, P.; Szymanski, W.W.; Ciach, T. Dextran Nanoparticle Synthesis and Properties. PLoS ONE 2016, 11, e0146237. [Google Scholar] [CrossRef] [PubMed]
- Sagnella, S.M.; Duong, H.; MacMillan, A.; Boyer, C.; Whan, R.; McCarroll, J.A.; Davis, T.P.; Kavallaris, M. Dextran-based doxorubicin nanocarriers with improved tumor penetration. Biomacromolecules 2014, 15, 262–275. [Google Scholar] [CrossRef]
- Chen, F.; Huang, G.; Huang, H. Preparation and application of dextran and its derivatives as carriers. Int. J. Biol. Macromol. 2020, 145, 827–834. [Google Scholar] [CrossRef]
- Petrovici, A.R.; Pinteala, M.; Simionescu, N. Dextran Formulations as Effective Delivery Systems of Therapeutic Agents. Molecules 2023, 28, 1086. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Matulonis, U.A. Current status and evolution of preclinical drug development models of epithelial ovarian cancer. Front. Oncol. 2013, 3, 296. [Google Scholar] [CrossRef]
- Karakashev, S.; Zhang, R.G. Mouse models of epithelial ovarian cancer for preclinical studies. Zool. Res. 2021, 42, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Sambasivan, S. Epithelial ovarian cancer: Review article. Cancer Treat. Res. Commun. 2022, 33, 100629. [Google Scholar] [CrossRef] [PubMed]
- Ferté, C.; Fernandez, M.; Hollebecque, A.; Koscielny, S.; Levy, A.; Massard, C.; Balheda, R.; Bot, B.; Gomez-Roca, C.; Dromain, C.; et al. Tumor Growth Rate (TGR) is an early indicator of anti-tumor drug activity in phase I clinical trials. Clin. Cancer Res. 2014, 20, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.; Stebbing, J.; Shousha, M.; Coombes, R. Tumor Volume Analysis and Tumor Doubling. Cancer Res. 2009, 69 (Suppl. S24), 5030. [Google Scholar] [CrossRef]
- Chida, T.; Miura, Y.; Cabral, H.; Nomoto, T.; Kataoka, K.; Nishiyama, N. Epirubicin-loaded polymeric micelles effectively treat axillary lymph nodes metastasis of breast cancer through selective accumulation and pH-triggered drug release. J. Control. Release 2018, 292, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Yamamoto, Y.; Yasunaga, M.; Koga, Y.; Kuroda, J.; Takigahira, M.; Harada, M.; Saito, H.; Hayashi, T.; Kato, Y.; et al. NC-6300, an epirubicin-incorporating micelle, extends the antitumor effect and reduces the cardiotoxicity of epirubicin. Cancer Sci. 2013, 104, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Harada, M.; Bobe, I.; Saito, H.; Shibata, N.; Tanaka, R.; Hayashi, T.; Kato, Y. Improved anti-tumor activity of stabilized anthracycline polymeric micelle formulation, NC-6300. Cancer Sci. 2011, 102, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Maletzki, C.; Bock, S.; Fruh, P.; Macius, K.; Witt, A.; Prall, F.; Linnebacher, M. NSG mice as hosts for oncological precision medicine. Lab. Invest. 2020, 100, 27–37. [Google Scholar] [CrossRef]
- Harrison, S.D.; Giles, H.D.; Denine, E.P. Antitumor drug toxicity in tumor-free and tumor-bearing mice. Cancer Chemother. Pharmacol. 1980, 4, 199–204. [Google Scholar] [CrossRef]
- Li, F.; Ulrich, M.L.; Shih, V.F.; Cochran, J.H.; Hunter, J.H.; Westendorf, L.; Neale, J.; Benjamin, D.R. Mouse Strains Influence Clearance and Efficacy of Antibody and Antibody–Drug Conjugate Via Fc–FcγR Interaction. Mol. Cancer Ther. 2019, 18, 780–787. [Google Scholar] [CrossRef]
- Ricci, F.; Bizzaro, F.; Cesca, M.; Guffanti, F.; Ganzinelli, M.; Decio, A.; Ghilardi, C.; Perego, P.; Fruscio, R.; Buda, A.; et al. Patient-derived ovarian tumor xenografts recapitulate human clinicopathology and genetic alterations. Cancer Res. 2014, 74, 6980–6990. [Google Scholar] [CrossRef]
- Abdolahi, S.; Ghazvinian, Z.; Muhammadnejad, S.; Saleh, M.; Asadzadeh Aghdaei, H.; Baghaei, K. Patient-derived xenograft (PDX) models, applications and challenges in cancer research. J. Transl. Med. 2022, 20, 206. [Google Scholar] [CrossRef]
- Woo, X.Y.; Giordano, J.; Srivastava, A.; Zhao, Z.M.; Lloyd, M.W.; de Bruijn, R.; Suh, Y.S.; Patidar, R.; Chen, L.; Scherer, S.; et al. Conservation of copy number profiles during engraftment and passaging of patient-derived cancer xenografts. Nat. Genet. 2021, 53, 86–99. [Google Scholar] [CrossRef]
- Hansen, J.M.; Coleman, R.L.; Sood, A.K. Targeting the tumour microenvironment in ovarian cancer. Eur. J. Cancer 2016, 56, 131–143. [Google Scholar] [CrossRef]
- Izumchenko, E.; Paz, K.; Ciznadija, D.; Sloma, I.; Katz, A.; Vasquez-Dunddel, D.; Ben-Zvi, I.; Stebbing, J.; McGuire, W.; Harris, W.; et al. Patient-derived xenografts effectively capture responses to oncology therapy in a heterogeneous cohort of patients with solid tumors. Ann. Oncol. 2017, 28, 2595–2605. [Google Scholar]
- Topp, M.D.; Hartley, L.; Cook, M.; Heong, V.; Boehm, E.; McShane, L.; Pyman, J.; McNally, O.; Ananda, S.; Harrell, M.; et al. Molecular correlates of platinum response in human high-grade serous ovarian cancer patient-derived xenografts. Mol. Oncol. 2014, 8, 656–668. [Google Scholar] [CrossRef]
- Gao, H.; Korn, J.M.; Ferretti, S.; Monahan, J.E.; Wang, Y.; Singh, M.; Zhang, C.; Schnell, C.; Yang, G.; Zhang, Y.; et al. High-throughput screening using patient-derived tumor xenografts to predict clinical trial drug response. Nat. Med. 2015, 21, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Atkins, J.T.; George, G.C.; Hess, K.; Marcelo-Lewis, K.L.; Yuan, Y.; Borthakur, G.; Khozin, S.; LoRusso, P.; Hong, D.S. Pre-clinical animal models are poor predictors of human toxicities in phase 1 oncology clinical trials. Br. J. Cancer 2020, 123, 1496–1501. [Google Scholar] [CrossRef]
- Muangsiri, W.; Kirsch, L.E. The protein-binding and drug release properties of macromolecular conjugates containing daptomycin and dextran. Int. J. Pharm. 2006, 315, 30–43. [Google Scholar] [CrossRef]
- Fuentes, M.; Segura, R.L.; Abian, O.; Betancor, L.; Hidalgo, A.; Mateo, C.; Fernandez-Lafuente, R.; Guisan, J.M. Determination of protein-protein interactions through aldehyde-dextran intermolecular cross-linking. Proteomics 2004, 4, 2602–2607. [Google Scholar] [CrossRef]
- Heindel, N.D.; Zhao, H.R.; Leiby, J.; VanDongen, J.M.; Lacey, C.J.; Lima, D.A.; Shabsoug, B.; Buzby, J.H. Hydrazide pharmaceuticals as conjugates to polyaldehyde dextran: Syntheses, characterization, and stability. Bioconjug. Chem. 1990, 1, 77–82. [Google Scholar] [CrossRef]
- D’Souza, S. A Review of In Vitro Drug Release Test Methods for Nano-Sized Dosage Forms. Adv. Pharm. 2014, 2014, 304757. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
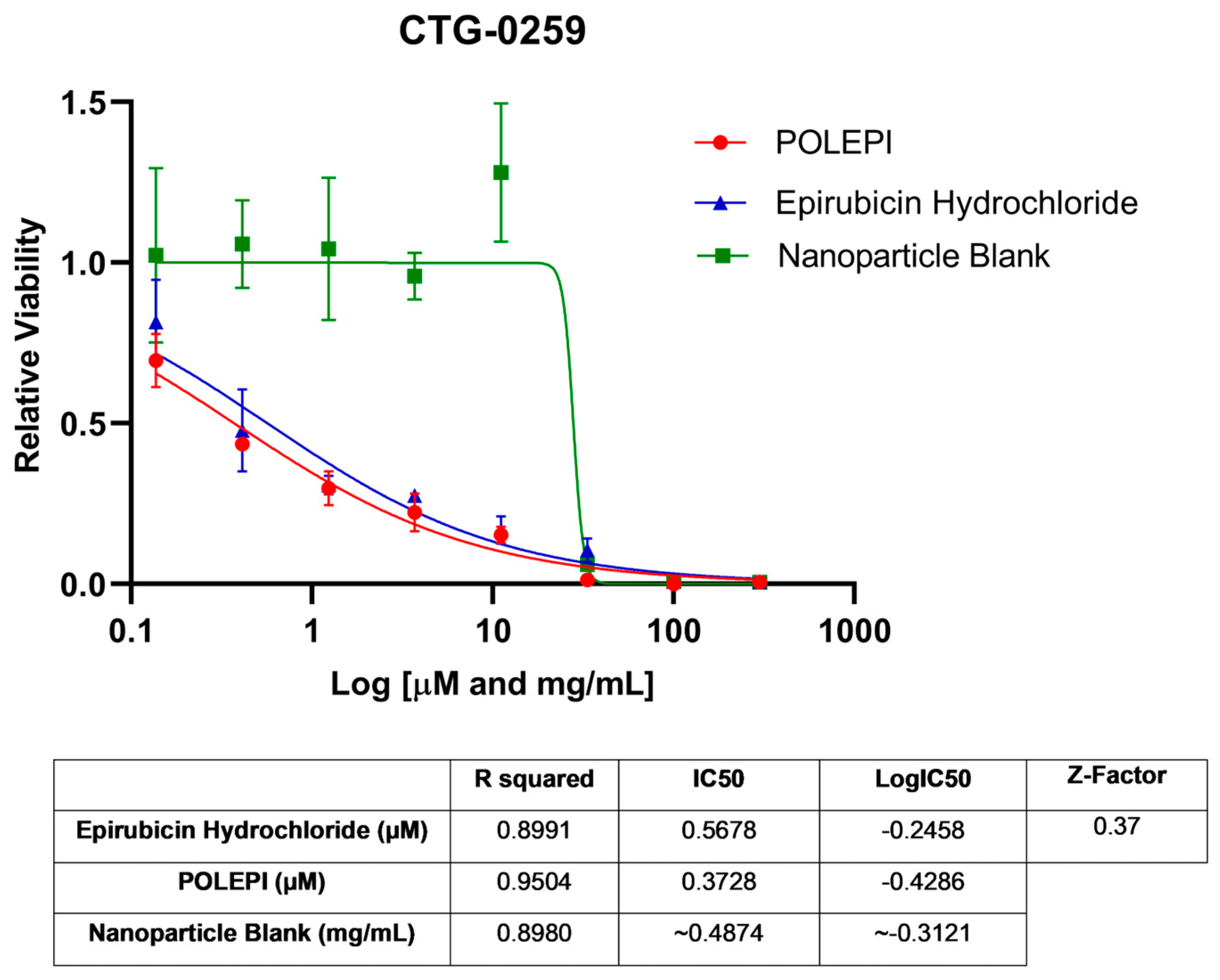
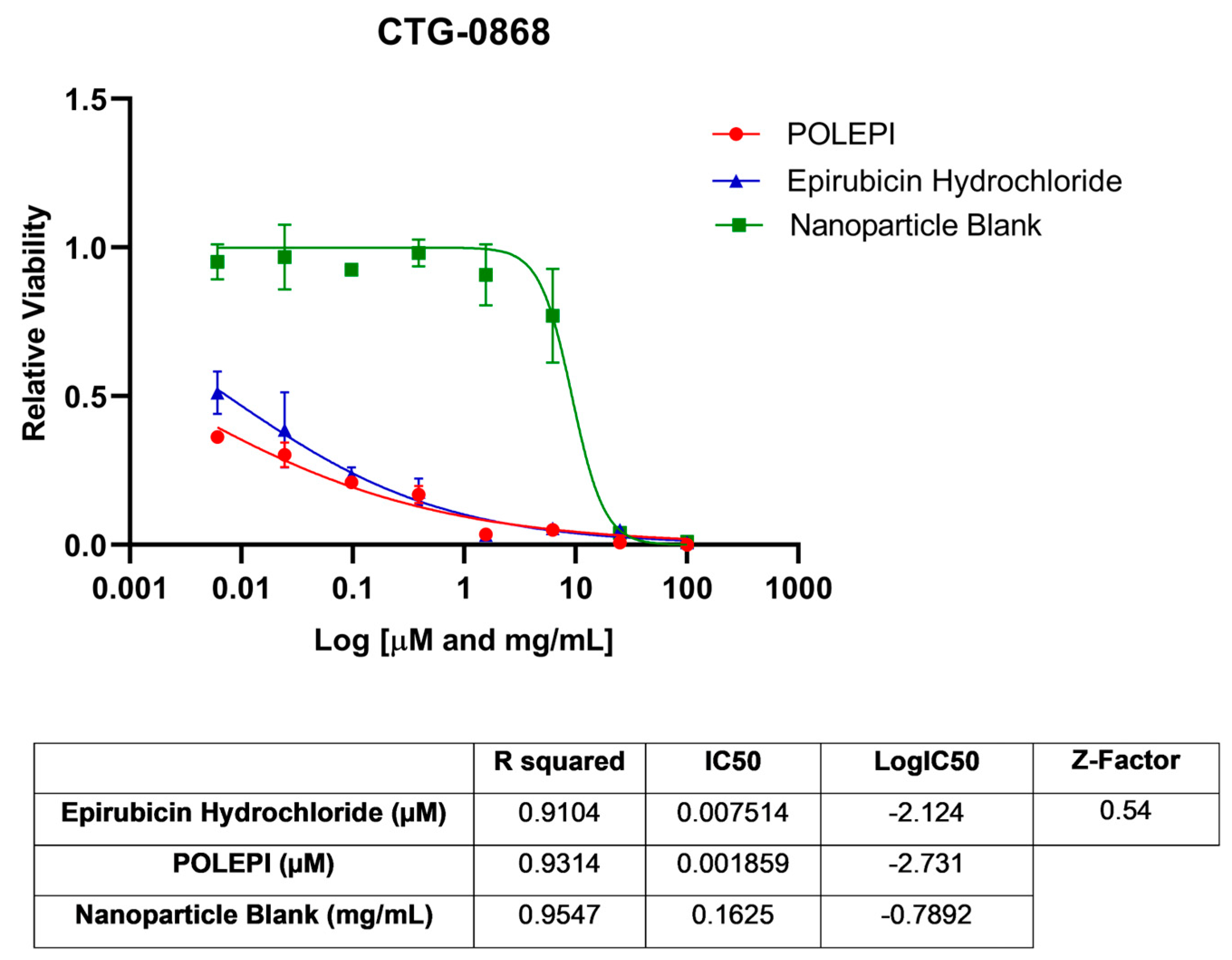
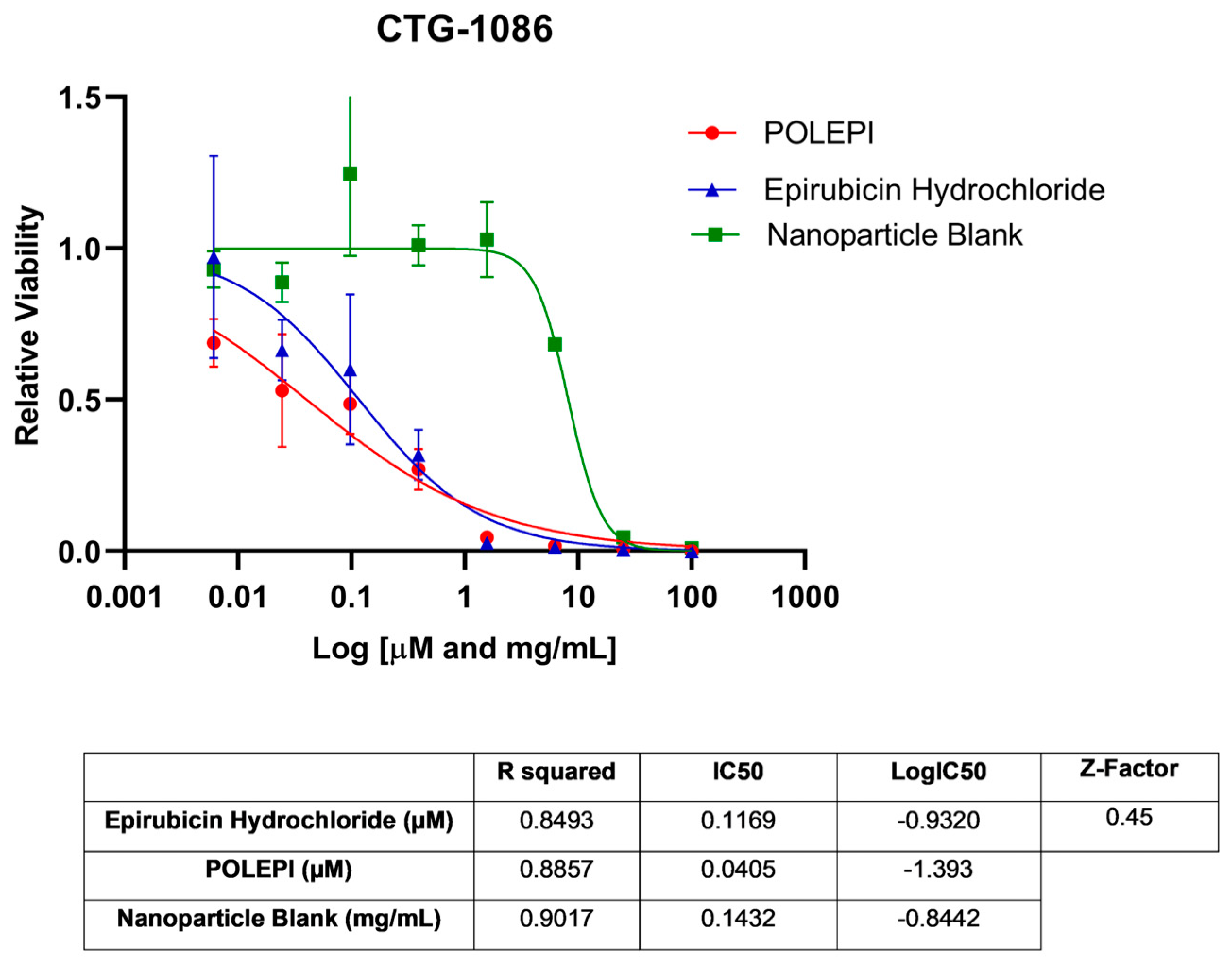
| Model ID | Z-Factor | Test Agent | IC50 | R2 | Log IC50 |
|---|---|---|---|---|---|
| CTG-0259 | 0.37 | Epirubicin Hydrochloride | 0.5678 µM | 0.8991 | −0.2458 |
| POLEPI | 0.3728 µM | 0.9504 | −0.4286 | ||
| Nanoparticle Blank | ~0.4874 mg/mL | 0.8980 | ~−0.3121 | ||
| CTG-0868 | 0.54 | Epirubicin Hydrochloride | 0.007514 µM | 0.9104 | −2.124 |
| POLEPI | 0.001859 µM | 0.9314 | −2.731 | ||
| Nanoparticle Blank | 0.1625 mg/mL | 0.9547 | −0.7892 | ||
| CTG-0964 | 0.33 | Epirubicin Hydrochloride | 0.008680 µM | 0.7393 | −2.061 |
| POLEPI | 0.006624 µM | 0.7399 | −2.179 | ||
| Nanoparticle Blank | 0.1324 mg/mL | 0.8442 | −0.8780 | ||
| CTG-0964 * | −0.45 | Epirubicin Hydrochloride | 35,175,064 µM | 0.03104 | 7.546 |
| POLEPI | 2.806 × 1017 µM | 0.001213 | 17.45 | ||
| Nanoparticle Blank | ~0.3647 mg/mL | 0.4510 | ~−0.4381 | ||
| CTG-1086 | 0.45 | Epirubicin Hydrochloride | 0.1169 µM | 0.8493 | −0.9320 |
| POLEPI | 0.04049 µM | 0.8857 | −1.393 | ||
| Nanoparticle Blank | 0.1432 mg/mL | 0.9017 | −0.8442 |
| Group | Animal ID | Absolute MRI Tumor Volume (mm³) | TGI% | TDT | |||||
|---|---|---|---|---|---|---|---|---|---|
| Study Days | |||||||||
| −1 (0) | 5 | 7 | 8 | 9 | Day 5–Day 0 | ||||
| Group 1: NP Blank | 001 | 127.32 | 296.41 | 340.08 | 169.09 | ||||
| Group 1: NP Blank | 002 | 128.30 | 254.47 | 340.25 | 126.17 | ||||
| Group 1: NP Blank | 008 | 108.23 | 201.34 | 256.85 | 93.11 | ||||
| Group 1: NP Blank | 009 | 58.64 | 91.05 | 93.84 | 32.41 | ||||
| Group 1: NP Blank | 014 | 54.03 | 76.73 | 76.82 | 22.70 | ||||
| Group 1: NP Blank | 015 | 89.65 | 153.55 | 183.41 | 63.90 | ||||
| Group 1: NP Blank | 034 | 57.00 | 74.51 | 132.83 | 17.51 | ||||
| Group 1: NP Blank | 037 | 100.67 | 186.78 | 209.81 | 86.11 | ||||
| Group 1: NP Blank | 039 | 143.44 | 235.30 | 273.96 | 91.86 | ||||
| Group 1: NP Blank | 040 | 57.16 | 83.97 | 112.02 | 26.81 | ||||
| Average | 92.44 | 165.41 | 201.99 | 72.97 | 5.96 | ||||
| Group 2: EPI | 004 | 161.61 | 147.71 | 159.14 | −13.90 | ||||
| Group 2: EPI | 005 | 67.52 | 105.44 | 37.92 | |||||
| Group 2: EPI | 007 | 103.96 | 140.56 | 163.01 | 36.60 | ||||
| Group 2: EPI | 017 | 90.06 | 144.50 | 172.88 | 54.44 | ||||
| Group 2: EPI | 022 | 61.85 | 87.43 | 89.73 | 25.58 | ||||
| Group 2: EPI | 028 | 69.25 | 66.78 | −2.47 | |||||
| Group 2: EPI | 036 | 91.62 | 179.38 | 87.76 | |||||
| Group 2: EPI | 038 | 133.24 | 241.22 | 233.00 | 107.98 | ||||
| Group 2: EPI | 043 | 88.17 | 197.96 | 229.05 | 109.79 | ||||
| Group 2: EPI | 045 | 73.86 | 75.91 | 2.05 | |||||
| Average | 94.11 | 138.69 | 196.05 | 131.31 | 44.58 | 38.91 | 8.94 | ||
| Group 3: POLEPI | 006 | 105.52 | 121.64 | 16.12 | |||||
| Group 3: POLEPI | 011 | 54.12 | 74.02 | 58.56 | 19.90 | ||||
| Group 3: POLEPI | 018 | 97.21 | 159.39 | 62.18 | |||||
| Group 3: POLEPI | 026 | 72.79 | |||||||
| Group 3: POLEPI | 029 | 104.20 | |||||||
| Group 3: POLEPI | 032 | 77.39 | 108.97 | 102.72 | 31.58 | ||||
| Group 3: POLEPI | 033 | 90.06 | 102.23 | 106.26 | 12.17 | ||||
| Group 3: POLEPI | 035 | 93.76 | 141.13 | 156.84 | 47.37 | ||||
| Group 3: POLEPI | 041 | 141.54 | 124.93 | 172.55 | −16.61 | ||||
| Group 3: POLEPI | 044 | 101.49 | 95.08 | 120.49 | −6.41 | ||||
| Average | 93.81 | 115.92 | 149.96 | 89.18 | 22.12 | 69.69 | 16.37 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kośnik, W.; Sikorska, H.; Kiciak, A.; Ciach, T. Nanoparticle-Encapsulated Epirubicin Efficacy in the Inhibition of Growth of Orthotopic Ovarian Patient-Derived Xenograft in Immunocompromised Mice. Int. J. Mol. Sci. 2024, 25, 645. https://doi.org/10.3390/ijms25010645
Kośnik W, Sikorska H, Kiciak A, Ciach T. Nanoparticle-Encapsulated Epirubicin Efficacy in the Inhibition of Growth of Orthotopic Ovarian Patient-Derived Xenograft in Immunocompromised Mice. International Journal of Molecular Sciences. 2024; 25(1):645. https://doi.org/10.3390/ijms25010645
Chicago/Turabian StyleKośnik, Wioletta, Hanna Sikorska, Adam Kiciak, and Tomasz Ciach. 2024. "Nanoparticle-Encapsulated Epirubicin Efficacy in the Inhibition of Growth of Orthotopic Ovarian Patient-Derived Xenograft in Immunocompromised Mice" International Journal of Molecular Sciences 25, no. 1: 645. https://doi.org/10.3390/ijms25010645
APA StyleKośnik, W., Sikorska, H., Kiciak, A., & Ciach, T. (2024). Nanoparticle-Encapsulated Epirubicin Efficacy in the Inhibition of Growth of Orthotopic Ovarian Patient-Derived Xenograft in Immunocompromised Mice. International Journal of Molecular Sciences, 25(1), 645. https://doi.org/10.3390/ijms25010645