
Assessing the Relationship between Systemic Immune-Inflammation Index and Metabolic Syndrome in Children with Obesity
 ,
,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. CBC-Derived Inflammatory Parameters
2.3. Association between SII Index and MetS
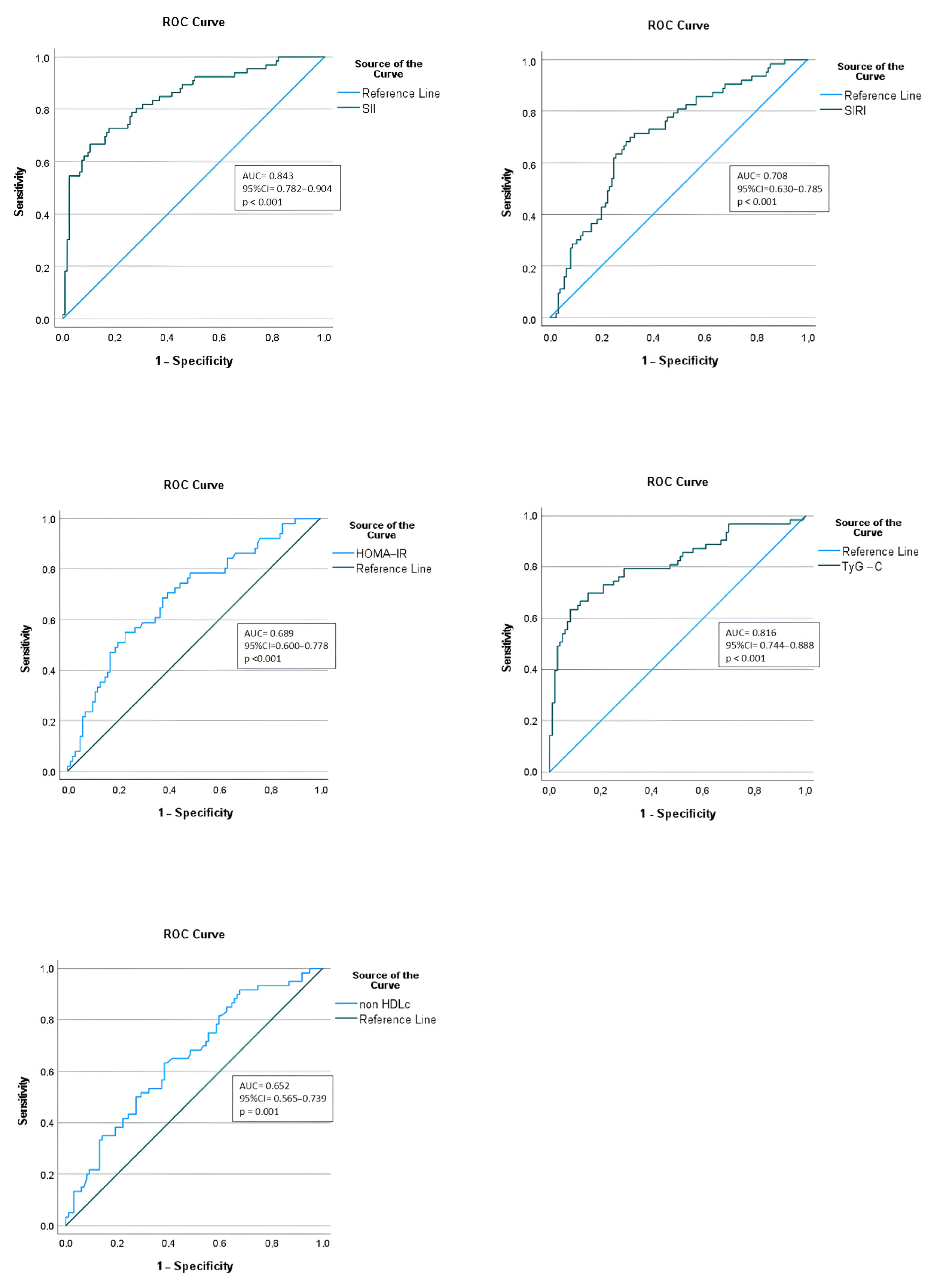
2.4. ROC Curves of Inflammation and Cardiometabolic Markers
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Selection
4.2. Clinical and Laboratory Assessments
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- González-Gil, E.M.; Anguita-Ruiz, A.; Kalén, A.; De Las Lamas Perez, C.; Rupérez, A.I.; Vázquez-Cobela, R.; Flores, K.; Gil, A.; Gil-Campos, M.; Bueno, G.; et al. Longitudinal associations between cardiovascular biomarkers and metabolic syndrome during puberty: The PUBMEP study. Eur. J. Pediatr. 2023, 182, 419–429. [Google Scholar] [CrossRef] [PubMed]
- The GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Polak-Szczybyło, E. Low-Grade Inflammation and Role of Anti-Inflammatory Diet in Childhood Obesity. Int. J. Environ. Res. Public Health 2023, 20, 1682. [Google Scholar] [CrossRef] [PubMed]
- Versini, M.; Jeandel, P.-Y.; Rosenthal, E.; Shoenfeld, Y. Obesity in autoimmune diseases: Not a passive bystander. Autoimmun. Rev. 2014, 13, 981–1000. [Google Scholar] [CrossRef]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M. Overweight, Obesity, and Mortality from Cancer in a Prospectively Studied Cohort of U.S. Adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef]
- Chirita-Emandi, A.; Barbu, C.G.; Cinteza, E.E.; Chesaru, B.I.; Gafencu, M.; Mocanu, V.; Pascanu, I.M.; Tatar, S.A.; Balgradean, M.; Dobre, M.; et al. Overweight and Underweight Prevalence Trends in Children from Romania—Pooled Analysis of Cross-Sectional Studies between 2006 and 2015. Obes. Facts 2016, 9, 206–220. [Google Scholar] [CrossRef]
- Guzmán-Guzmán, I.P.; Salgado-Bernabé, A.B.; Valle, J.F.M.; Vences-Velázquez, A.; Parra-Rojas, I. Prevalence of metabolic syndrome in children with and without obesity. Med. Clín. 2015, 144, 198–203. (In Spanish) [Google Scholar] [CrossRef]
- Hedley, A.A.; Ogden, C.L.; Johnson, C.L.; Carroll, M.D.; Curtin, L.R.; Flegal, K.M. Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999–2002. JAMA 2004, 291, 2847–2850. [Google Scholar] [CrossRef]
- World Health Organization. Population-Based Prevention Strategies for Childhood Obesity: Report of a WHO Forum and Technical Meeting; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Brady, T.M. The Role of Obesity in the Development of Left Ventricular Hypertrophy Among Children and Adolescents. Curr. Hypertens. Rep. 2016, 18, 3. [Google Scholar] [CrossRef]
- Giannini, C.; de Giorgis, T.; Scarinci, A.; Cataldo, I.; Marcovecchio, M.L.; Chiarelli, F.; Mohn, A. Increased carotid intima-media thickness in pre-pubertal children with constitutional leanness and severe obesity: The speculative role of insulin sensitivity, oxidant status, and chronic inflammation. Eur. J. Endocrinol. 2009, 161, 73–80. [Google Scholar] [CrossRef]
- Yazarlı, E.; Ünsal Saç, R.; Şimşek, B.; Engiz, Ö.; Dallar Bilge, Y.; Alioğlu, B. The relation between increased carotid intima-media thickness with fibrin monomers in obese children. Int. J. Clin. Pract. 2021, 75, e14199. [Google Scholar] [CrossRef] [PubMed]
- Magge, S.N.; Goodman, E.; Armstrong, S.C.; Daniels, S.; Corkins, M.; de Ferranti, S.; Golden, N.H.; Kim, J.H.; Schwarzenberg, S.J.; Sills, I.N.; et al. The Metabolic Syndrome in Children and Adolescents: Shifting the Focus to Cardiometabolic Risk Factor Clustering. Pediatrics 2017, 140, e20171603. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Weitzman, M.; Auinger, P.; Nguyen, M.; Dietz, W.H. Prevalence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Arch. Pediatr. Adolesc. Med. 2003, 157, 821–827. [Google Scholar] [CrossRef]
- Reinehr, T. Metabolic Syndrome in Children and Adolescents: A Critical Approach Considering the Interaction between Pubertal Stage and Insulin Resistance. Curr. Diabetes Rep. 2016, 16, 8. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C. Defining the metabolic syndrome in children and adolescents: Will the real definition please stand up? J. Pediatr. 2008, 152, 160–164. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Andreeva, V.A.; Kesse-Guyot, E.; Hercberg, S. Dietary patterns, inflammation and the metabolic syndrome. Diabetes Metab. 2013, 39, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Segal, T.Y.; Lichtarowicz-Krynska, E.; Hindmarsh, P. Prevalence of the insulin resistance syndrome in obesity. Arch. Dis. Child. 2005, 90, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the Metabolic Syndrome in Children and Adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef]
- Zimmet, P.; Alberti, K.G.M.; Kaufman, F.; Tajima, N.; Silink, M.; Arslanian, S.; Wong, G.; Bennett, P.; Shaw, J.; Caprio, S.; et al. The metabolic syndrome in children and adolescents ? An IDF consensus report. Pediatr. Diabetes 2007, 8, 299–306. [Google Scholar] [CrossRef]
- Bitew, Z.W.; Alemu, A.; Ayele, E.G.; Tenaw, Z.; Alebel, A.; Worku, T. Metabolic syndrome among children and adolescents in low and middle income countries: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2020, 12, 93. [Google Scholar] [CrossRef] [PubMed]
- Wittcopp, C.; Conroy, R. Metabolic Syndrome in Children and Adolescents. Pediatr. Rev. 2016, 37, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Serbis, A.; Giapros, V.; Galli-Tsinopoulou, A.; Siomou, E. Metabolic Syndrome in Children and Adolescents: Is There a Universally Accepted Definition? Does it Matter? Metab. Syndr. Relat. Disord. 2020, 18, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Tobisch, B.; Blatniczky, L.; Barkai, L. Cardiometabolic risk factors and insulin resistance in obese children and adolescents: Relation to puberty. Pediatr. Obes. 2015, 10, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Di Pino, A.; Alagona, C.; Piro, S.; Calanna, S.; Spadaro, L.; Palermo, F.; Urbano, F.; Purrello, F.; Rabuazzo, A. Separate impact of metabolic syndrome and altered glucose tolerance on early markers of vascular injuries. Atherosclerosis 2012, 223, 458–462. [Google Scholar] [CrossRef]
- Walsh, S.; Cook, E.; Goulder, F.; Justin, T.; Keeling, N. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef]
- Vallance, S. Platelets, leucocytes and buffy layer vitamin C after surgery. Hum. Nutr. Clin. Nutr. 1986, 40, 35–41. [Google Scholar]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic Immune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Niculescu, R.; Russu, E.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Melinte, R.M.; Coșarcă, C.M.; Cocuz, I.G.; Sabău, A.H.; Tinca, A.C.; et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. Int. J. Environ. Res. Public Health 2022, 19, 13934. [Google Scholar] [CrossRef]
- Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; Voidăzan, S.; Arbănași, E.M.; Horváth, E.; Suciu, B.A.; Hosu, I.; Halmaciu, I.; Brinzaniuc, K.; et al. The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure. Life 2022, 12, 1447. [Google Scholar] [CrossRef]
- Melinte, R.M.; Arbănași, E.M.; Blesneac, A.; Zolog, D.N.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Melinte, I.M.; Niculescu, R.; Russu, E. Inflammatory Biomarkers as Prognostic Factors of Acute Deep Vein Thrombosis Following the Total Knee Arthroplasty. Medicina 2022, 58, 1502. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Zhuang, L.; Shen, Y.; Geng, Y.; Yu, S.; Chen, H.; Liu, L.; Meng, Z.; Wang, P.; Chen, Z. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer 2016, 122, 2158–2167. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Srinivasan, S.R.; Elkasabany, A.; Berenson, G.S. Cardiovascular risk factors clustering features of insulin resistance syndrome (Syndrome X) in a biracial (Black-White) population of children, adolescents, and young adults: The Bogalusa Heart Study. Am. J. Epidemiol. 1999, 150, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Lissau, I.; Flodmark, C.-E.; Moreno, L.A.; Widhalm, K.; Wabitsch, M.; Pietrobelli, A. Metabolic risk-factor clustering estimation in children: To draw a line across pediatric metabolic syndrome. Int. J. Obes. 2007, 31, 591–600. [Google Scholar] [CrossRef]
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [CrossRef]
- Friend, A.; Craig, L.; Turner, S. The Prevalence of Metabolic Syndrome in Children: A Systematic Review of the Literature. Metab. Syndr. Relat. Disord. 2013, 11, 71–80. [Google Scholar] [CrossRef]
- De Ferranti, S.D.; Gauvreau, K.; Ludwig, D.S.; Newburger, J.W.; Rifai, N. Inflammation and Changes in Metabolic Syndrome Abnormalities in US Adolescents: Findings from the 1988–1994 and 1999–2000 National Health and Nutrition Examination Surveys. Clin. Chem. 2006, 52, 1325–1330. [Google Scholar] [CrossRef]
- Reisinger, C.; Nkeh-Chungag, B.N.; Fredriksen, P.M.; Goswami, N. The prevalence of pediatric metabolic syndrome—A critical look on the discrepancies between definitions and its clinical importance. Int. J. Obes. 2021, 45, 12–24. [Google Scholar] [CrossRef]
- I’Allemand, D.; Wiegand, S.; Reinehr, T.; Müller, J.; Wabitsch, M.; Widhalm, K.; Holl, R.; APV-Study Group. Cardiovascular Risk in 26,008 European Overweight Children as Established by a Multicenter Database. Obesity 2008, 16, 1672–1679. [Google Scholar] [CrossRef]
- Kuschnir, M.C.C.; Bloch, K.V.; Szklo, M.; Klein, C.H.; Barufaldi, L.A.; Abreu, G.D.A.; Schaan, B.; Da Veiga, G.V.; Da Silva, T.L.N.; De Vasconcellos, M.T.L. ERICA: Prevalence of metabolic syndrome in Brazilian adolescents [correction]. Rev. Saude Publica 2016, 50 (Suppl. S1), 11s. [Google Scholar] [CrossRef]
- Li, P.; Jiang, R.; Li, L.; Liu, C.; Yang, F.; Qiu, Y. Prevalence and risk factors of metabolic syndrome in school adolescents of northeast China. J. Pediatr. Endocrinol. Metab. 2014, 27, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Fadzlina, A.; Harun, F.; Haniza, M.N.; Al Sadat, N.; Murray, L.; Cantwell, M.M.; Su, T.T.; Majid, H.A.; Jalaludin, M.Y. Metabolic syndrome among 13 year old adolescents: Prevalence and risk factors. BMC Public Health 2014, 14 (Suppl. S3), S7. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Anzola, A.; Martinez-Torres, J.; Vivas, A.; Tordecilla-Sanders, A.; Prieto-Benavides, D.H.; Izquierdo, M.; Correa-Bautista, J.E.; Garcia-Hermoso, A. Metabolic Syndrome and Associated Factors in a Population-Based Sample of Schoolchildren in Colombia: The FUPRECOL Study. Metab. Syndr. Relat. Disord. 2016, 14, 455–462. [Google Scholar] [CrossRef]
- Agudelo, G.M.; Bedoya, G.; Estrada, A.; Patiño, F.A.; Muñoz, A.M.; Velásquez, C.M. Variations in the prevalence of metabolic syndrome in adolescents according to different criteria used for diagnosis: Which definition should be chosen for this age group? Metab. Syndr. Relat. Disord. 2014, 12, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; So, W.-Y. Prevalence of Metabolic Syndrome among Korean Adolescents According to the National Cholesterol Education Program, Adult Treatment Panel III and International Diabetes Federation. Nutrients 2016, 8, 588. [Google Scholar] [CrossRef] [PubMed]
- Reyes, M.; Mederico, M.; Paoli, M.; Briceño, Y.; Miliani, Y.; GómezPérez, R.; Camacho, N.; Martínez, J.L.; Valeri, L.; Arata-Bellabarba, G.; et al. Metabolic syndrome in children and adolescents from Mérida city, Venezuela: Comparison of results using local and international reference values (CREDEFAR study). Endocrinol. Nutr. 2014, 61, 474–485. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, C.G.; Fraser, B.J.; Raitakari, O.T. Pediatric Metabolic Syndrome: Long-Term Risks for Type 2 Diabetes and Cardiovascular Disease. In Pediatric Obesity: Contemporary Endocrinology; Freemark, M., Ed.; Humana Press: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Gidding, S.S.; Bao, W.; Srinivasan, S.R.; Berenson, G.S. Effects of secular trends in obesity on coronary risk factors in children: The Bogalusa Heart Study. J. Pediatr. 1995, 127, 868–874. [Google Scholar] [CrossRef]
- Morrison, J.A.; Friedman, L.A.; Gray-McGuire, C. Metabolic Syndrome in Childhood Predicts Adult Cardiovascular Disease 25 Years Later: The Princeton Lipid Research Clinics Follow-up Study. Pediatrics 2007, 120, 340–345. [Google Scholar] [CrossRef]
- Chinali, M.; de Simone, G.; Roman, M.J.; Best, L.G.; Lee, E.T.; Russell, M.; Howard, B.V.; Devereux, R.B. Cardiac Markers of Pre-Clinical Disease in Adolescents With the Metabolic Syndrome: The Strong Heart Study. J. Am. Coll. Cardiol. 2008, 52, 932–938. [Google Scholar] [CrossRef]
- Battista, M.; Murray, R.D.; Daniels, S.R. Use of the metabolic syndrome in pediatrics: A blessing and a curse. Semin. Pediatr. Surg. 2009, 18, 136–143. [Google Scholar] [CrossRef]
- Gisterå, A.; Hansson, G.K. The immunology of atherosclerosis. Nat. Rev. Nephrol. 2017, 13, 368–380. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Henao-Mejia, J.; Flavell, R.A. Innate Immune Receptors: Key Regulators of Metabolic Disease Progression. Cell Metab. 2013, 17, 873–882. [Google Scholar] [CrossRef]
- Furman, D.; Chang, J.; Lartigue, L.; Bolen, C.R.; Haddad, F.; Gaudilliere, B.; Ganio, E.A.; Fragiadakis, G.K.; Spitzer, M.; Douchet, I.; et al. Expression of specific inflammasome gene modules stratifies older individuals into two extreme clinical and immunological states. Nat. Med. 2017, 23, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Karin, M. NF-κB, inflammation, immunity and cancer: Coming of age. Nat. Rev. Immunol. 2018, 18, 309–324. [Google Scholar] [CrossRef] [PubMed]
- Straub, R.H.; Cutolo, M.; Pacifici, R. Evolutionary medicine and bone loss in chronic inflammatory diseases—A theory of inflammation-related osteopenia. Semin. Arthritis Rheum. 2015, 45, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Örgül, G.; Haklı, D.A.; Özten, G.; Fadiloğlu, E.; Tanacan, A.; Beksaç, M. First trimester complete blood cell indices in early and late onset preeclampsia. Turk. J. Obstet. Gynecol. 2019, 16, 112. [Google Scholar] [CrossRef]
- Velioglu, Y.; Yuksel, A. Complete blood count parameters in peripheral arterial disease. Aging Male 2019, 22, 187–191. [Google Scholar] [CrossRef]
- Slamoğlu, Z.G.K.; Demirbaş, A. Evaluation of complete blood cell and in flammatory parameters in patients with alopecia areata: Their association with disease severity. J. Cosmet. Dermatol. 2020, 19, 1239–1245. [Google Scholar] [CrossRef]
- Haybar, H.; Pezeshki, S.M.S.; Saki, N. Evaluation of complete blood count parameters in cardiovascular diseases: An early indicator of prognosis? Exp. Mol. Pathol. 2019, 110, 104267. [Google Scholar] [CrossRef]
- Xia, Y.; Xia, C.; Wu, L.; Li, Z.; Li, H.; Zhang, J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: A 20-Year Follow-Up Cohort Study of 42,875 US Adults. J. Clin. Med. 2023, 12, 1128. [Google Scholar] [CrossRef]
- Taha, S.I.; Samaan, S.F.; Ibrahim, R.A.; Moustafa, N.M.; El-Sehsah, E.M.; Youssef, M.K. Can Complete Blood Count Picture Tell Us More About the Activity of Rheumatological Diseases? Clin. Med. Insights Arthritis Musculoskelet. Disord. 2022, 15, 11795441221089182. [Google Scholar] [CrossRef] [PubMed]
- Mercan, R.; Bitik, B.; Tufan, A.; Bozbulut, U.B.; Atas, N.; Ozturk, M.A.; Haznedaroglu, S.; Goker, B. The Association Between Neutrophil/Lymphocyte Ratio and Disease Activity in Rheumatoid Arthritis and Ankylosing Spondylitis. J. Clin. Lab. Anal. 2016, 30, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Chen, D.-Y.; Xu, X.-Z.; Liu, Y.-Y.; Yin, T.-T.; Li, D. Platelet/Lymphocyte, Lymphocyte/Monocyte, and Neutrophil/Lymphocyte Ratios as Biomarkers in Patients with Rheumatoid Arthritis and Rheumatoid Arthritis-Associated Interstitial Lung Disease. Med. Sci. Monit. 2019, 25, 6474–6481. [Google Scholar] [CrossRef] [PubMed]
- Mǎrginean, C.O.; Meliţ, L.E.; Ghiga, D.V.; Mǎrginean, M.O. Early inflammatory status related to pediatric obesity. Front. Pediatr. 2019, 7, 241. [Google Scholar] [CrossRef] [PubMed]
- Gok, M.; Kurtul, A. A novel marker for predicting severity of acute pulmonary embolism: Systemic immune-inflammation index. Scand. Cardiovasc. J. 2021, 55, 91–96. [Google Scholar] [CrossRef]
- He, L.; Xie, X.; Xue, J.; Xie, H.; Zhang, Y. Association of the systemic immune-inflammation index with all-cause mortality in patients with arteriosclerotic cardiovascular disease. Front. Cardiovasc. Med. 2022, 9, 952953. [Google Scholar] [CrossRef]
- Trifan, G.; Testai, F.D. Systemic Immune-Inflammation (SII) index predicts poor outcome after spontaneous supratentorial intracerebral hemorrhage. J. Stroke Cerebrovasc. Dis. 2020, 29, 105057. [Google Scholar] [CrossRef]
- Dincer, A.K.; Sezer, S. Systemic Immune Inflammation Index as a Reliable Disease Activity Marker in Psoriatic Arthritis. J. Coll. Physicians Surg. Pak. 2022, 32, 773–778. [Google Scholar] [CrossRef]
- Rota, D.D.; Tanacan, E. The utility of systemic-immune inflammation index for predicting the disease activation in patients with psoriasis. Int. J. Clin. Pract. 2021, 75, e14101. [Google Scholar] [CrossRef]
- Qin, Z.; Li, H.; Wang, L.; Geng, J.; Yang, Q.; Su, B.; Liao, R. Systemic Immune-Inflammation Index Is Associated With Increased Urinary Albumin Excretion: A Population-Based Study. Front. Immunol. 2022, 13, 863640. [Google Scholar] [CrossRef]
- Chen, J.-H.; Zhai, E.-T.; Yuan, Y.; Wu, K.-M.; Xu, J.-B.; Peng, J.-J.; Chen, C.-Q.; He, Y.-L.; Cai, S.-R. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Zheng, J.; Cai, J.; Zeng, K.; Yao, J.; Chen, L.; Li, H.; Zhang, J.; Zhang, Y.; Zhao, H.; et al. Systemic Immune-Inflammation Index (SII) is Useful to Predict Survival Outcomes in Patients After Liver Transplantation for Hepatocellular Carcinoma within Hangzhou Criteria. Cell. Physiol. Biochem. 2018, 47, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic value of Systemic immune-inflammation index in cancer: A meta-analysis. J. Cancer 2018, 9, 3295–3302. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.-H.; Huang, D.-H.; Chen, Z.-Y. Prognostic role of systemic immune-inflammation index in solid tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 75381–75388. [Google Scholar] [CrossRef]
- Xie, Y.; Zhuang, T.; Ping, Y.; Zhang, Y.; Wang, X.; Yu, P.; Duan, X. Elevated systemic immune inflammation index level is associated with disease activity in ulcerative colitis patients. Clin. Chim. Acta 2021, 517, 122–126. [Google Scholar] [CrossRef]
- Yang, Y.-L.; Wu, C.-H.; Hsu, P.-F.; Chen, S.-C.; Huang, S.-S.; Chan, W.L.; Lin, S.-J.; Chou, C.-Y.; Chen, J.-W.; Pan, J.-P.; et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur. J. Clin. Investig. 2020, 50, e13230. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, Q.; Wang, R.; Ji, H.; Chen, Y.; Quan, X.-Q.; Zhang, C. Systemic Immune-Inflammatory Index Predicts Clinical Outcomes for Elderly Patients with Acute Myocardial Infarction Receiving Percutaneous Coronary Intervention. Med. Sci. Monit. 2019, 25, 9690–9701. [Google Scholar] [CrossRef]
- Çırakoğlu, F.; Yılmaz, A.S. Systemic immune-inflammation index is associated with increased carotid intima-media thickness in hypertensive patients. Clin. Exp. Hypertens. 2021, 43, 565–571. [Google Scholar] [CrossRef]
- Li, L.-H.; Chen, C.-T.; Chang, Y.-C.; Chen, Y.-J.; Lee, I.-H.; How, C.-K. Prognostic role of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and systemic immune inflammation index in acute ischemic stroke: A STROBE-compliant retrospective study. Medicine 2021, 100, e26354. [Google Scholar] [CrossRef]
- Seo, M.; Yamada, T.; Morita, T.; Furukawa, Y.; Tamaki, S.; Iwasaki, Y.; Kawasaki, M.; Kikuchi, A.; Kawai, T.; Ikeda, I.; et al. P589Prognostic value of systemic immune-inflammation index in patients with chronic heart failure. Eur. Heart J. 2018, 39, 589. [Google Scholar] [CrossRef]
- Tanacan, E.; Dincer, D.; Erdogan, F.G.; Gurler, A. A cutoff value for the Systemic Immune-Inflammation Index in determining activity of Behçet disease. Clin. Exp. Dermatol. 2021, 46, 286–291. [Google Scholar] [CrossRef]
- Wang, P.; Guo, X.; Zhou, Y.; Li, Z.; Yu, S.; Sun, Y.; Hua, Y. Monocyte-to-high-density lipoprotein ratio and systemic inflammation response index are associated with the risk of metabolic disorders and cardiovascular diseases in general rural population. Front. Endocrinol. 2022, 13, 944991. [Google Scholar] [CrossRef]
- Țaranu, I.; Lazea, C.; Creț, V.; Răcătăianu, N.; Iancu, M.; Bolboacă, S.D. Inflammation-Related Markers and Thyroid Function Measures in Pediatric Patients: Is the Grade of Obesity Relevant? Diagnostics 2021, 11, 485. [Google Scholar] [CrossRef]
- Bastard, J.-P.; Maachi, M.; Lagathu, C.; Kim, M.J.; Caron, M.; Vidal, H.; Capeau, J.; Feve, B. Recent advances in the relationship between obesity, inflammation, and insulin resistance. Eur. Cytokine Netw. 2006, 17, 4–12. [Google Scholar] [PubMed]
- Magnussen, C.G.; Koskinen, J.; Chen, W.; Thomson, R.; Schmidt, M.D.; Srinivasan, S.R.; Kivimäki, M.; Mattsson, N.; Kähönen, M.; Laitinen, T.; et al. Pediatric metabolic syndrome predicts adulthood metabolic syndrome, subclinical atherosclerosis, and type 2 diabetes mellitus but is no better than body mass index alone: The Bogalusa Heart Study and the Cardiovascular Risk in Young Finns Study. Circulation 2010, 122, 1604–1611. [Google Scholar] [CrossRef]
- Liu, C.-C.; Ko, H.-J.; Liu, W.-S.; Hung, C.-L.; Hu, K.-C.; Yu, L.-Y.; Shih, S.-C. Neutrophil-to-lymphocyte ratio as a predictive marker of metabolic syndrome. Medicine 2019, 98, e17537. [Google Scholar] [CrossRef] [PubMed]
- Buyukkaya, E.; Karakaş, M.F.; Karakaş, E.; Akçay, A.B.; Tanboga, I.H.; Kurt, M.; Sen, N. Correlation of Neutrophil to Lymphocyte Ratio With the Presence and Severity of Metabolic Syndrome. Clin. Appl. Thromb./Hemost. 2014, 20, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Balta, S.; Cakar, M.; Demirkol, S.; Arslan, Z.; Akhan, M. Higher Neutrophil to Lymhocyte Ratio in Patients With Metabolic Syndrome. Clin. Appl. Thromb./Hemost. 2013, 19, 579. [Google Scholar] [CrossRef] [PubMed]
- Akboga, M.K.; Canpolat, U.; Yuksel, M.; Yayla, C.; Yilmaz, S.; Turak, O.; Ozeke, O.; Topaloglu, S.; Aras, D. Platelet to lymphocyte ratio as a novel indicator of inflammation is correlated with the severity of metabolic syndrome: A single center large-scale study. Platelets 2016, 27, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, H.; Özen, B.; Çatlı, G.; Dündar, B.N. Macular Variability in Children and Adolescents with Metabolic Syndrome: A Cross-sectional Study Examining the Associations with Anthropometric Measurements, Metabolic Parameters and Inflammatory Markers. J. Clin. Res. Pediatr. Endocrinol. 2020, 12, 63–70. [Google Scholar] [CrossRef]
- Iwani, N.A.K.Z.; Jalaludin, M.Y.; Zin, R.M.W.M.; Fuziah, Z.; Hong, J.Y.H.; Abqariyah, Y.; Mokhtar, A.H.; Wan Nazaimoon, W.M. Triglyceride to HDL-C Ratio is Associated with Insulin Resistance in Overweight and Obese Children. Sci. Rep. 2017, 7, 40055. [Google Scholar] [CrossRef] [PubMed]
- Von Bibra, H.; Saha, S.; Hapfelmeier, A.; Müller, G.; Schwarz, P.E.H. Impact of the Triglyceride/High-Density Lipoprotein Cholesterol Ratio and the Hypertriglyceremic-Waist Phenotype to Predict the Metabolic Syndrome and Insulin Resistance. Horm. Metab. Res. 2017, 49, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk, M.; Rumińska, M.; Sędek, E.W.; Majcher, A.; Pyrżak, B. Usefulness of the Triglycerides to High-Density Lipoprotein Cholesterol ratio (TG/HDL-C) in prediction of metabolic syndrome in Polish obese children and adolescents. Acta Biochim. Pol. 2018, 65, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Saito, E.; Okada, T.; Abe, Y.; Kazama, M.; Yonezawa, R.; Kuromori, Y.; Iwata, F.; Hara, M. Non-high-density Lipoprotein Cholesterol Levels in Japanese Obese Boys with Metabolic Syndrome. J. Atheroscler. Thromb. 2016, 23, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Angoorani, P.; Khademian, M.; Ejtahed, H.-S.; Heshmat, R.; Motlagh, M.E.; Vafaeenia, M.; Shafiee, G.; Mahdivi-Gorabi, A.; Qorbani, M.; Kelishadi, R. Are non-high–density lipoprotein fractions associated with pediatric metabolic syndrome? The CASPIAN-V study. Lipids Health Dis. 2018, 17, 257. [Google Scholar] [CrossRef] [PubMed]
- Iwani, A.K.N.Z.; Jalaludin, M.Y.; Zin, R.M.W.M.; Fuziah, Z.; Hong, J.Y.H.; Abqariyah, Y.; Mokhtar, A.H.; Mohamud, W.N.W. TG: HDL-C Ratio Is a Good Marker to Identify Children Affected by Obesity with Increased Cardiometabolic Risk and Insulin Resistance. Int. J. Endocrinol. 2019, 2019, 8586167. [Google Scholar] [CrossRef]
- Al-Hamad, D.; Raman, V. Metabolic syndrome in children and adolescents. Transl. Pediatr. 2017, 6, 397–407. [Google Scholar] [CrossRef]
- Burns, S.F.; Lee, S.J.; Arslanian, S.A. Surrogate Lipid Markers for Small Dense Low-Density Lipoprotein Particles in Overweight Youth. J. Pediatr. 2012, 161, 991–996. [Google Scholar] [CrossRef]
- Jin, Z.; Wu, Q.; Chen, S.; Gao, J.; Li, X.; Zhang, X.; Zhou, Y.; He, D.; Cheng, Z.; Zhu, Y.; et al. The Associations of Two Novel Inflammation Indexes, SII and SIRI with the Risks for Cardiovascular Diseases and All-Cause Mortality: A Ten-Year Follow-Up Study in 85,154 Individuals. J. Inflamm. Res. 2021, 14, 131–140. [Google Scholar] [CrossRef]
- Ye, Z.; Hu, T.; Wang, J.; Xiao, R.; Liao, X.; Liu, M.; Sun, Z. Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 933913. [Google Scholar] [CrossRef]
- Li, J.; He, D.; Yu, J.; Chen, S.; Wu, Q.; Cheng, Z.; Wei, Q.; Xu, Y.; Zhu, Y.; Wu, S. Dynamic Status of SII and SIRI Alters the Risk of Cardiovascular Diseases: Evidence from Kailuan Cohort Study. J. Inflamm. Res. 2022, 15, 5945–5957. [Google Scholar] [CrossRef] [PubMed]
- Uzun, F.; Güner, A.; Pusuroglu, H.; Demir, A.R.; Gündüz, S.; Gürbak, I.; Aslan, S.; Demirci, G.; Güner, E.G.; Arslan, E.; et al. Association of red blood cell distribution width, systemic-immune-inflammation index and poor cardiovascular outcomes in patients with newly diagnosed hypertension. Clin. Exp. Hypertens. 2022, 44, 530–538. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Polonsky, S.M.; Bellet, P.S.; Sprecher, D.L. Primary hyperlipidemia in a pediatric population: Classification and effect of dietary treatment. Pediatrics 1993, 91, 92–96. [Google Scholar] [CrossRef]
- Masarei, J.; Pyke, J.; Pyke, F. Physical fitness and plasma HDL cholesterol concentrations in male business executives. Atherosclerosis 1982, 42, 77–83. [Google Scholar] [CrossRef]

 , case number;
, case number;  , regression.
, case number; , regression.
, regression.
, case number; , regression.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Non-MetS (n = 125) | MetS (n = 66) | p-Value |
|---|---|---|---|
| Age (years) | 12 (11–15) | 13 (11–15) | 0.104 U |
| % Males (n) | 58.4 (73) | 57.6 (38) | 0.913 χ2 |
| BMI (kg/m2) | 29.9 (27.9, 32.2) | 32.9 (29.3, 37.9) | <0.001 U |
| WC (cm) | 93.7 ± 13.7 | 104.1 ± 18.9 | <0.001 t |
| SBP (mmHg) | 115 (103, 123) | 125 (111, 140) | <0.001 U |
| DBP (mmHg) | 69.8 ± 11 | 78.3 ± 12.9 | <0.001 t |
| WBCs (×103/mm3) | 7.23 (6.07, 8.38) | 9.42 (7.90, 10.46) | <0.001 t |
| Neutrophils (×103/mm3) | 3.56 (2.90, 4.53) | 5.47 (4.18, 6.65) | <0.001 t |
| Lymphocytes (×103/mm3) | 2.56 ± 0.83 | 2.66 ± 0.81 | 0.789 t |
| Thrombocytes (×103/mm3) | 296 ± 63.94 | 340.1 ± 83.3 | <0.001 t |
| Monocytes (×103/mm3) | 0.64 (0.53–0.79) | 0.71 (0.58–0.82) | 0.103 U |
| Glycemia (mg/dL) | 89.82 (84.87–94.05) | 91.89 (86.22–100.93) | 0.034 U |
| Insulinemia (uIU/mL) | 16.43 (12.83–25.37) | 25.36 (15.61–42.72) | <0.001 U |
| TG (mg/dL) | 82.37 (56.90–106.28) | 152.78 (102.29–185.33) | <0.001 U |
| Cholesterol (mg/dL) | 154.33 ± 33.27 | 162.21 ± 38 | 0.148 t |
| HDL-C (mg/dL) | 46.65 ± 10.30 | 36.47 ± 8.64 | <0.001 t |
| LDL-C (mg/dL) | 88.28 ± 31.38 | 93.37 ± 33.03 | 0.431 t |
| HOMA-IR | 3.52 (2.68–5.89) | 6.40 (3.66–9.10) | <0.001 U |
| TG:HDL-C | 1.77 (1.05–2.74) | 4.13 (2.71–5.55) | <0.001 U |
| Non-HDL-C | 106 (78.5–125.3) | 121.4 (99.1–144.4) | <0.001 U |
| Parameter | Non-MetS (n = 123) | MetS (n = 68) | p-Value |
|---|---|---|---|
| NLR | 1.36 (1.12–1.77) | 1.90 (1.58–2.67) | <0.001 t |
| PLR | 117.24 (93.75–140.20) | 128.25 (108.10–169.02) | <0.001 t |
| SII | 363.4 (277.9–477.01) | 715.87 (472.98–909.15) | <0.001 t |
| SIRI | 0.890 (0.633–1.312) | 1.380 (0.929–2.030) | <0.001 t |
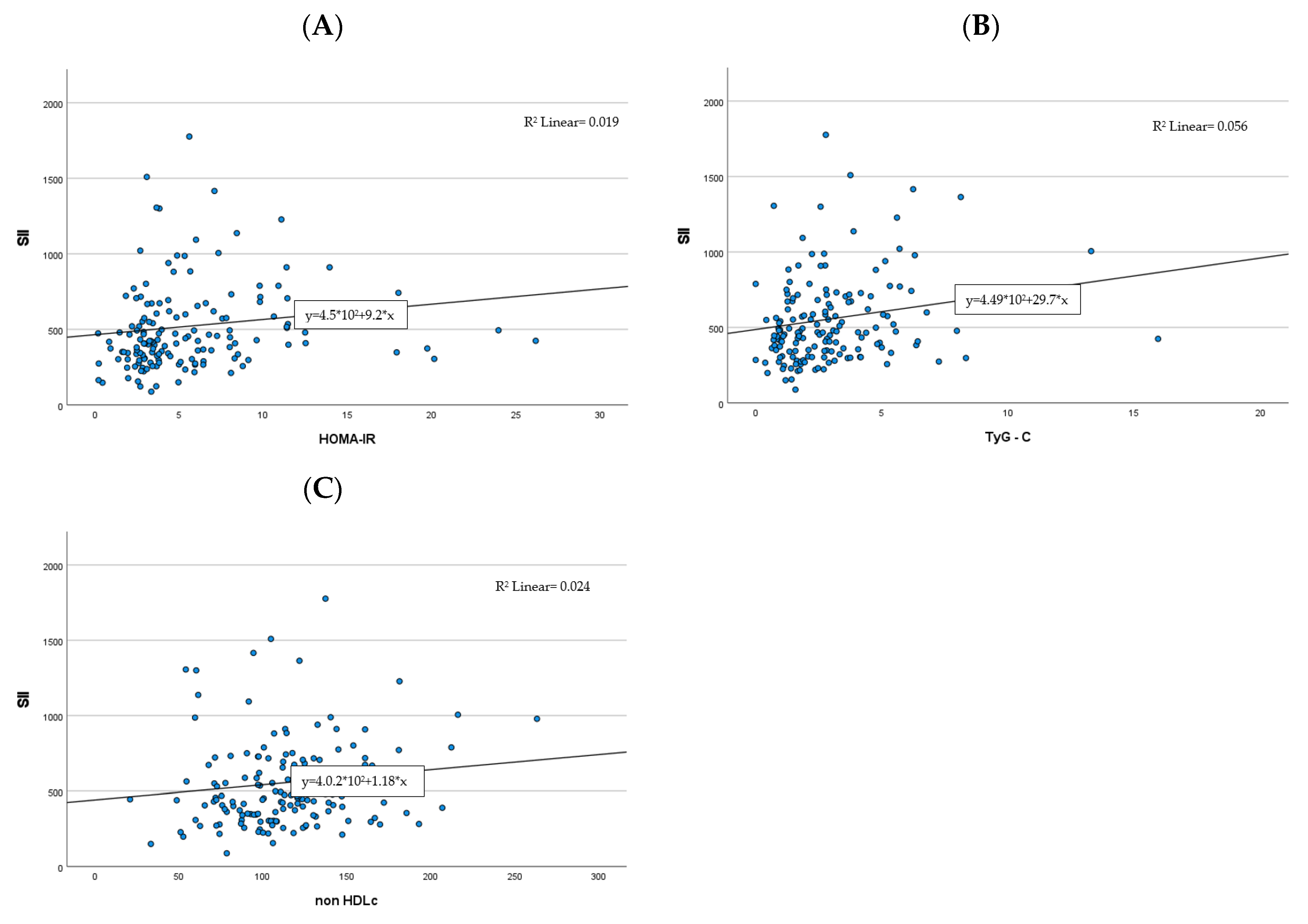
| HOMA-IR | TG:HDL-C | Non-HDL-C | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Item | rS | p | 95% CI | rS | p | 95% CI | rS | p | 95% CI |
| SII | 0.274 | <0.001 | 0.115–0.419 | 0.239 | 0.002 | 0.083–0.383 | 0.18 | 0.021 | 0.024–0.334 |
| Bivariate Analysis | ||
|---|---|---|
| Variable | OR (95% CI) | p-Value |
| SII | 1.005 (1.003–1.008) | <0.001 |
| SIRI | 1.071 (0.938–1.224) | 0.311 |
| HOMA-IR | 0.962 (0.731–1.267) | 0.783 |
| Non-HDL-C | 0.993 (0.976–1.010) | 0.423 |
| TG:HDL-C | 2.884 (1.825–4.555) | <0.001 |
| Variable | ß (95% CI) | p-Value |
|---|---|---|
| WC (cm) | 1.578 (0.281–6.552) | 0.033 |
| SBP (mmHg) | 2.076 (−3.337–4.9130) | 0.705 |
| DBP (mmHg) | 2.789 (−2.931–8.155) | 0.352 |
| Glycemia (mg/dL) | 1.593 (−5.674–0.656) | 0.119 |
| HDL-C (mg/dL) | 2.398 (−8.355–1.176) | 0.138 |
| TG (mg/dL) | 0.399 (−0.799–0.786) | 0.987 |
| AUC | SE | 95% CI | Sensitivity | Specificity | Cut-Off | p-Value | |
|---|---|---|---|---|---|---|---|
| SII | 0.843 | 0.031 | 0.782–0.904 | 0.83 | 0.63 | 426.8 | <0.001 |
| SIRI | 0.708 | 0.039 | 0.630–0.785 | 0.69 | 0.67 | 1.123 | <0.001 |
| HOMA-IR | 0.689 | 0.046 | 0.600–0.778 | 0.66 | 0.62 | 4.24 | <0.001 |
| Non-HDL-C | 0.652 | 0.044 | 0.565–0.739 | 0.63 | 0.61 | 107.7 | 0.001 |
| TG:HDL-C | 0.816 | 0.037 | 0.744–0.888 | 0.81 | 0.50 | 1.786 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicoară, D.-M.; Munteanu, A.-I.; Scutca, A.-C.; Mang, N.; Juganaru, I.; Brad, G.-F.; Mărginean, O. Assessing the Relationship between Systemic Immune-Inflammation Index and Metabolic Syndrome in Children with Obesity. Int. J. Mol. Sci. 2023, 24, 8414. https://doi.org/10.3390/ijms24098414
Nicoară D-M, Munteanu A-I, Scutca A-C, Mang N, Juganaru I, Brad G-F, Mărginean O. Assessing the Relationship between Systemic Immune-Inflammation Index and Metabolic Syndrome in Children with Obesity. International Journal of Molecular Sciences. 2023; 24(9):8414. https://doi.org/10.3390/ijms24098414
Chicago/Turabian StyleNicoară, Delia-Maria, Andrei-Ioan Munteanu, Alexandra-Cristina Scutca, Niculina Mang, Iulius Juganaru, Giorgiana-Flavia Brad, and Otilia Mărginean. 2023. "Assessing the Relationship between Systemic Immune-Inflammation Index and Metabolic Syndrome in Children with Obesity" International Journal of Molecular Sciences 24, no. 9: 8414. https://doi.org/10.3390/ijms24098414
APA StyleNicoară, D.-M., Munteanu, A.-I., Scutca, A.-C., Mang, N., Juganaru, I., Brad, G.-F., & Mărginean, O. (2023). Assessing the Relationship between Systemic Immune-Inflammation Index and Metabolic Syndrome in Children with Obesity. International Journal of Molecular Sciences, 24(9), 8414. https://doi.org/10.3390/ijms24098414