Neutrophil-to-Lymphocyte Ratio Is an Independent Risk Factor for Coronary Artery Disease in Central Obesity

 , ,
, ,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics by Dichotomized CACS
2.2. Baseline Characteristics by VAI Tertiles
2.3. Association of Neutrophil-to-Lymphocyte Ratio and Coronary Calcium Score across VAI Tertiles
2.4. Independent Determinants of Increased Coronary Artery Calcium Score
3. Discussion
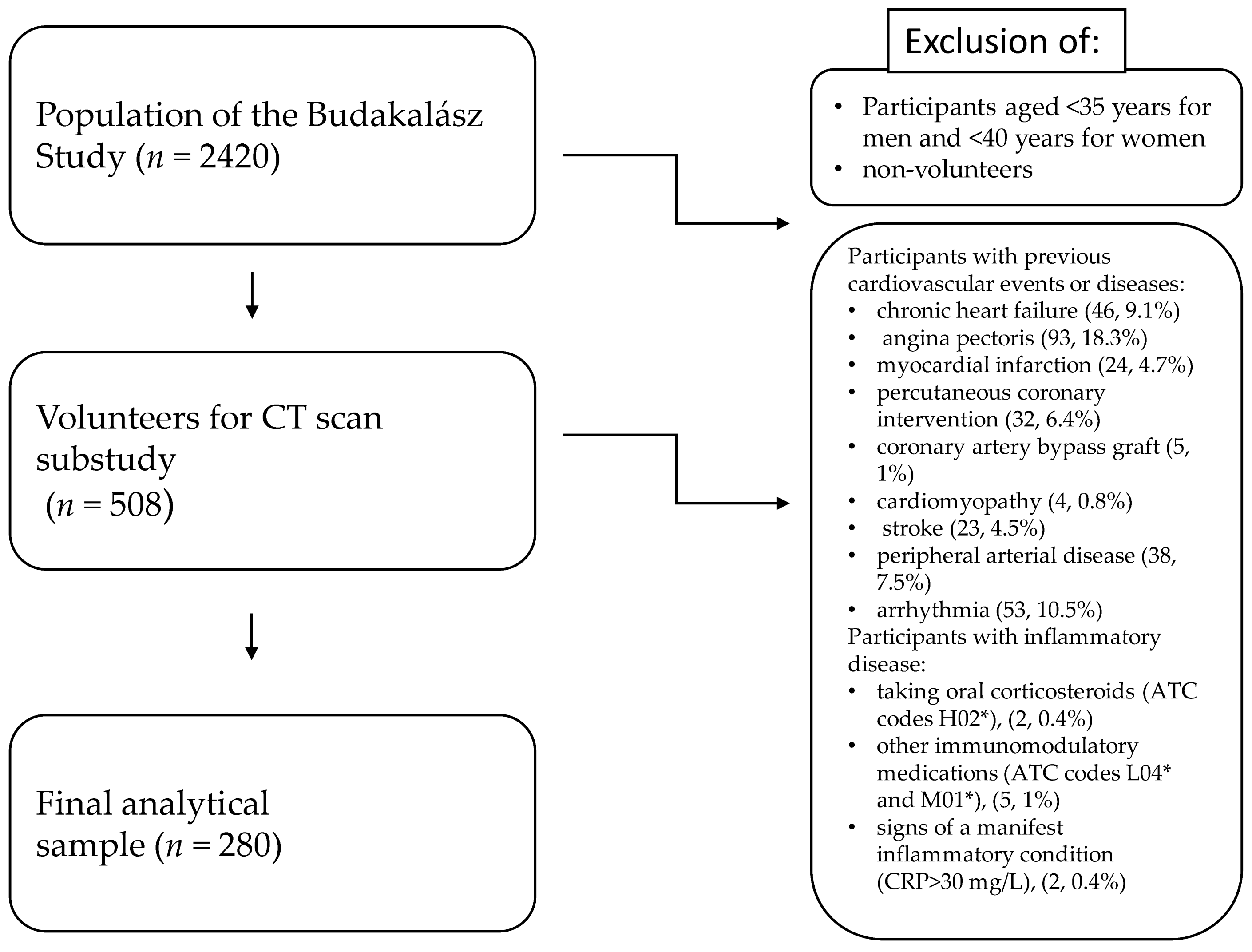
4. Materials and Methods
- Males: VAI = [WC/{39.68 + (1.88 × BMI)}] × (TG/1.03) × (1.31/HDL-C)
- Females: VAI = [WC/{36.58 + (1.89 × BMI)}] × (TG/0.81) × (1.52/HDL-C)
Statistical Methods
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Townsend, N.; Nichols, M.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe—Epidemiological update 2015. Eur. Heart J. 2015, 36, 2696–2705. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.D.; Paisley, R.; Moon, P.; Novak, E.; Villines, T.C. Coronary Artery Calcium and Long-Term Risk of Death, Myocardial Infarction, and Stroke: The Walter Reed Cohort Study. JACC Cardiovasc. Imaging 2018, 11, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Rijlaarsdam-Hermsen, D.; Lo-Kioeng-Shioe, M.S.; Kuijpers, D.; van Domburg, R.T.; Deckers, J.W.; van Dijkman, P.R.M. Prognostic value of the coronary artery calcium score in suspected coronary artery disease: Amstudy of 644 symptomatic patients. Neth. Heart J. Mon. J. Neth. Soc. Cardiol. Neth. Heart Found. 2020, 28, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef]
- Iliodromiti, S.; Celis-Morales, C.A.; Lyall, D.M.; Anderson, J.; Gray, S.R.; Mackay, D.F.; Nelson, S.M.; Welsh, P.; Pell, J.P.; Gill, J.M.R.; et al. The impact of confounding on the associations of different adiposity measures with the incidence of cardiovascular disease: A cohort study of 296 535 adults of white European descent. Eur. Heart J. 2018, 39, 1514–1520. [Google Scholar] [CrossRef]
- Qiao, T.; Luo, T.; Pei, H.; Yimingniyazi, B.; Aili, D.; Aimudula, A.; Zhao, H.; Zhang, H.; Dai, J.; Wang, D. Association between abdominal obesity indices and risk of cardiovascular events in Chinese populations with type 2 diabetes: A prospective cohort study. Cardiovasc. Diabetol. 2022, 21, 225. [Google Scholar] [CrossRef]
- Kouli, G.M.; Panagiotakos, D.B.; Kyrou, I.; Georgousopoulou, E.N.; Chrysohoou, C.; Tsigos, C.; Tousoulis, D.; Pitsavos, C. Visceral adiposity index and 10-year cardiovascular disease incidence: The ATTICA study. Nutr. Metab. Cardiovasc. Dis. NMCD 2017, 27, 881–889. [Google Scholar] [CrossRef]
- Bagyura, Z.; Kiss, L.; Lux, Á.; Csobay-Novák, C.; Jermendy, Á.L.; Polgár, L.; Szelid, Z.; Soós, P.; Merkely, B. Association between coronary atherosclerosis and visceral adiposity index. Nutr. Metab. Cardiovasc. Dis. NMCD 2020, 30, 796–803. [Google Scholar] [CrossRef]
- Maréchal, P.; Tridetti, J.; Nguyen, M.L.; Wéra, O.; Jiang, Z.; Gustin, M.; Donneau, A.F.; Oury, C.; Lancellotti, P. Neutrophil Phenotypes in Coronary Artery Disease. J. Clin. Med. 2020, 9, 1602. [Google Scholar] [CrossRef]
- Cooper, H.A.; Exner, D.V.; Waclawiw, M.A.; Domanski, M.J. White blood cell count and mortality in patients with ischemic and nonischemic left ventricular systolic dysfunction (an analysis of the Studies Of Left Ventricular Dysfunction [SOLVD]). Am. J. Cardiol. 1999, 84, 252–257. [Google Scholar] [CrossRef]
- Warny, M.; Helby, J.; Nordestgaard, B.G.; Birgens, H.; Bojesen, S.E. Incidental lymphopenia and mortality: A prospective cohort study. CMAJ Can. Med. Assoc. J. = J. De L’association Med. Can. 2020, 192, E25–E33. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, E.; López-Sobaler, A.M.; Ortega, R.M.; Delgado-Losada, M.L.; López-Parra, A.M.; Aparicio, A. Association between Neutrophil-to-Lymphocyte Ratio with Abdominal Obesity and Healthy Eating Index in a Representative Older Spanish Population. Nutrients 2020, 12, 855. [Google Scholar] [CrossRef]
- Karakaya, S.; Altay, M.; Kaplan Efe, F.; Karadağ, İ.; Ünsal, O.; Bulur, O.; Eser, M.; Taner Ertuğrul, D. The neutrophil-lymphocyte ratio and its relationship with insulin resistance in obesity. Turk. J. Med. Sci. 2019, 49, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Angkananard, T.; Anothaisintawee, T.; McEvoy, M.; Attia, J.; Thakkinstian, A. Neutrophil Lymphocyte Ratio and Cardiovascular Disease Risk: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2018, 2018, 2703518. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Hou, M.; Ding, Z.; Liu, X.; Shao, Y.; Li, X. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 686983. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Cao, D.; Han, L. Correlation of neutrophil-to-lymphocyte ratio with the prognosis of non-ST-segment elevation in patients with acute coronary syndrome undergoing selective percutaneous coronary intervention. J. Int. Med. Res. 2020, 48, 300060520959510. [Google Scholar] [CrossRef]
- Dentali, F.; Nigro, O.; Squizzato, A.; Gianni, M.; Zuretti, F.; Grandi, A.M.; Guasti, L. Impact of neutrophils to lymphocytes ratio on major clinical outcomes in patients with acute coronary syndromes: A systematic review and meta-analysis of the literature. Int. J. Cardiol. 2018, 266, 31–37. [Google Scholar] [CrossRef]
- Del Turco, S.; Bastiani, L.; Minichilli, F.; Landi, P.; Basta, G.; Pingitore, A.; Vassalle, C. Interaction of Uric Acid and Neutrophil-to-Lymphocyte Ratio for Cardiometabolic Risk Stratification and Prognosis in Coronary Artery Disease Patients. Antioxidants 2022, 11, 2163. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Gąsior, J.S.; Tuzimek, A.; Dąbrowski, M.; Jankowski, P. Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome. Biology 2022, 11, 1001. [Google Scholar] [CrossRef]
- Taurino, M.; Aloisi, F.; Del Porto, F.; Nespola, M.; Dezi, T.; Pranteda, C.; Rizzo, L.; Sirignano, P. Neutrophil-to-Lymphocyte Ratio Could Predict Outcome in Patients Presenting with Acute Limb Ischemia. J. Clin. Med. 2021, 10, 4343. [Google Scholar] [CrossRef]
- Spark, J.I.; Sarveswaran, J.; Blest, N.; Charalabidis, P.; Asthana, S. An elevated neutrophil-lymphocyte ratio independently predicts mortality in chronic critical limb ischemia. J. Vasc. Surg. 2010, 52, 632–636. [Google Scholar] [CrossRef]
- Pasqui, E.; de Donato, G.; Lazzeri, E.; Molino, C.; Galzerano, G.; Giubbolini, M.; Palasciano, G. High Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios Are Associated with a Higher Risk of Hemodialysis Vascular Access Failure. Biomedicines 2022, 10, 2218. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Cuenca, J.A.; Ruíz-Hernández, A.S.; Mendoza-Castañeda, A.A.; Domínguez-Pérez, G.A.; Hernández-Patricio, A.; Vera-Gómez, E.; De la Peña-Sosa, G.; Banderas-Lares, D.Z.; Montoya-Ramírez, J.; Blas-Azotla, R.; et al. Neutrophil-to-lymphocyte ratio and its relation with pro-inflammatory mediators, visceral adiposity and carotid intima-media thickness in population with obesity. Eur. J. Clin. Investig. 2019, 49, e13085. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Lai, X.; Yan, C.; Jia, X.; Li, Y. The associations between neutrophil-to-lymphocyte ratio and the Chinese Visceral Adiposity Index, and carotid atherosclerosis and atherosclerotic cardiovascular disease risk. Exp. Gerontol. 2020, 139, 111019. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Gu, C.; Wang, F.; Lv, B.; Zhang, C.; Peng, R.; Cong, X.; Chen, X. Association of Neutrophil-Lymphocyte Ratio and the Presence of Noncalcified or Mixed Coronary Atherosclerotic Plaques. Angiology 2018, 69, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.H.; Kang, S.G.; Song, S.W. The Neutrophil-Lymphocyte Ratio Is Associated with Coronary Artery Calcification in Asymptomatic Korean Males: A Cross-Sectional Study. BioMed Res. Int. 2017, 2017, 1989417. [Google Scholar] [CrossRef] [PubMed]
- Serrano, C.V., Jr.; de Mattos, F.R.; Pitta, F.G.; Nomura, C.H.; de Lemos, J.; Ramires, J.A.F.; Kalil-Filho, R. Association between Neutrophil-Lymphocyte and Platelet-Lymphocyte Ratios and Coronary Artery Calcification Score among Asymptomatic Patients: Data from a Cross-Sectional Study. Mediat. Inflamm. 2019, 2019, 6513847. [Google Scholar] [CrossRef]
- Nicoll, R.; Wiklund, U.; Zhao, Y.; Diederichsen, A.; Mickley, H.; Ovrehus, K.; Zamorano, J.; Gueret, P.; Schmermund, A.; Maffei, E.; et al. Gender and age effects on risk factor-based prediction of coronary artery calcium in symptomatic patients: A Euro-CCAD study. Atherosclerosis 2016, 252, 32–39. [Google Scholar] [CrossRef]
- Kiss, L.Z.; Bagyura, Z.; Csobay-Novák, C.; Lux, Á.; Polgár, L.; Jermendy, Á.; Soós, P.; Szelid, Z.; Maurovich-Horvat, P.; Becker, D.; et al. Serum Uric Acid Is Independently Associated with Coronary Calcification in an Asymptomatic Population. J. Cardiovasc. Transl. Res. 2019, 12, 204–210. [Google Scholar] [CrossRef]
- Rohm, T.V.; Meier, D.T.; Olefsky, J.M.; Donath, M.Y. Inflammation in obesity, diabetes, and related disorders. Immunity 2022, 55, 31–55. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, G.; Laukkanen, J.A.; Song, X.; Zhang, J.; Wei, L.; Chen, X.; Li, Y.; Liu, C. Higher neutrophil to lymphocyte ratio is associated with renal dysfunction and cardiac adverse remodeling in elderly with metabolic syndrome. Front. Cardiovasc. Med. 2022, 9, 921204. [Google Scholar] [CrossRef] [PubMed]
- Hashemi Moghanjoughi, P.; Neshat, S.; Rezaei, A.; Heshmat-Ghahdarijani, K. Is the Neutrophil-to-Lymphocyte Ratio an Exceptional Indicator for Metabolic Syndrome Disease and Outcomes? Endocr. Pract. 2022, 28, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Osaka, M.; Deushi, M.; Aoyama, J.; Funakoshi, T.; Ishigami, A.; Yoshida, M. High-Fat Diet Enhances Neutrophil Adhesion in LDLR-Null Mice Via Hypercitrullination of Histone H3. JACC Basic Transl. Sci. 2021, 6, 507–523. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.S.; Brownlee, M. Molecular and Cellular Mechanisms of Cardiovascular Disorders in Diabetes. Circ. Res. 2016, 118, 1808–1829. [Google Scholar] [CrossRef]
- Flynn, M.C.; Kraakman, M.J.; Tikellis, C.; Lee, M.K.S.; Hanssen, N.M.J.; Kammoun, H.L.; Pickering, R.J.; Dragoljevic, D.; Al-Sharea, A.; Barrett, T.J.; et al. Transient Intermittent Hyperglycemia Accelerates Atherosclerosis by Promoting Myelopoiesis. Circ. Res. 2020, 127, 877–892. [Google Scholar] [CrossRef]
- Vallejo, J.; Cochain, C.; Zernecke, A.; Ley, K. Heterogeneity of immune cells in human atherosclerosis revealed by scRNA-Seq. Cardiovasc. Res. 2021, 117, 2537–2543. [Google Scholar] [CrossRef]
- Mauersberger, C.; Hinterdobler, J.; Schunkert, H.; Kessler, T.; Sager, H.B. Where the Action Is-Leukocyte Recruitment in Atherosclerosis. Front. Cardiovasc. Med. 2021, 8, 813984. [Google Scholar] [CrossRef]
- Silvestre-Roig, C.; Braster, Q.; Ortega-Gomez, A.; Soehnlein, O. Neutrophils as regulators of cardiovascular inflammation. Nat. Rev. Cardiol. 2020, 17, 327–340. [Google Scholar] [CrossRef]
- Akers, E.J.; Nicholls, S.J.; Bartolo, B.A.D. Plaque Calcification. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 1902–1910. [Google Scholar] [CrossRef]
- Jinnouchi, H.; Sato, Y.; Sakamoto, A.; Cornelissen, A.; Mori, M.; Kawakami, R.; Gadhoke, N.V.; Kolodgie, F.D.; Virmani, R.; Finn, A.V. Calcium deposition within coronary atherosclerotic lesion: Implications for plaque stability. Atherosclerosis 2020, 306, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Balmos, I.A.; Horváth, E.; Brinzaniuc, K.; Muresan, A.V.; Olah, P.; Molnár, G.B.; Nagy, E.E. Inflammation, Microcalcification, and Increased Expression of Osteopontin Are Histological Hallmarks of Plaque Vulnerability in Patients with Advanced Carotid Artery Stenosis. Biomedicines 2023, 11, 881. [Google Scholar] [CrossRef] [PubMed]
- Bagyura, Z.; Kiss, L.; Edes, E.; Lux, A.; Polgár, L.; Soós, P.; Szenczi, O.; Szelid, Z.; Vadas, R.; Józan, P.; et al. Cardiovascular screening programme in the Central Hungarian region. The Budakalász Study. Orv. Hetil. 2014, 155, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef] [PubMed]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [Google Scholar] [CrossRef]


{kind=link}
| Demographics and Risk Factors (n (%)/Mean (SD)) | CACS ≤ 100 (201) | CACS > 100 (79) | p |
|---|---|---|---|
| BMI, mean (SD) | 27.6 (4.8) | 29.2 (5.29) | 0.02 |
| hsCRP, mean (SD) | 2.63 (3.05) | 2.89 (3.68) | NS |
| HbA1c, mean (SD) | 5.75 (0.55) | 6.17 (1.1) | 0.01 |
| age, mean (SD) | 57.4 (10.6) | 67 (7.6) | <0.001 |
| NLR, mean (SD) | 1.88 (0.71) | 2.19 (0.88) | 0.008 |
| smoking, n (%) | 24 (11.9) | 10 (12.7) | NS |
| HT, n (%) | 86 (42.8) | 64 (81.0) | <0.001 |
| HLP, n % | 74 (36.8) | 38 (48.1) | NS |
| DM, n % | 11 (5.5) | 22 (27.8) | <0.001 |
| Sex, n % | 77 (38.3) | 45 (57.0) | 0.005 |
| Demographics and Risk Factors (n (%)/Mean (SD) | Total Population | VAI 1st Tertile | VAI 2nd Tertile | VAI 3rd Tertile | p |
|---|---|---|---|---|---|
| n (%) | 280 (100) | 93 | 94 | 93 | NS |
| Male, n (%) | 122 (43.6) | 41 (42.7) | 42 (43.3) | 41 (42.7) | NS |
| VAI mean (SD) | 1.73 (0.32) | 1.72 (0.3) | 1.87 (0.3) | 1.9 (0.35) | <0.001 |
| HLP, n (%) | 112 (40.8) | 33 (35.5) | 39 (41.5) | 40 (43.0) | NS |
| HT, n (%) | 150 (53.6) | 41 (44.1) | 54 (57.4) | 55 (59.1) | NS |
| DM, n (%) | 33 (11.8) | 6 (6.5) | 7 (7.4) | 20 (21.5) | 0.002 |
| Smoking, n (%) | 34 (12.1) | 17 (18.3) | 7 (7.4) | 10 (10.8) | NS |
| Age, years, mean (SD) | 60.3 (10.7) | 56.8 (11.0) | 61.6 (10.5) | 62.1 (10.1) | 0.001 |
| BMI, (kg/m2), mean (SD) | 28.1 (5.0) | 27.5 (5.3) | 29.0 (4.3) | 27.7 (5.2) | NS |
| NLR, mean (SD) | 1.97 (0.77) | 1.88 (0.66) | 1.9 (0.71) | 2.14 (0.91) | 0.042 |
| HbA1c, %, mean (SD) | 5.87 (0.78) | 5.72 (0.58) | 5.84 (0.65) | 6.04 (1.01) | 0.02 |
| hsCRP, mmol/L, mean (SD) | 2.71 (3.24) | 2.43 (3.26) | 2.65 (2.8) | 3.05 (3.6) | NS |
| CACS > 100, n (%) | 79 (28.2) | 17 (18.3) | 26 (27.7) | 36 (38.7) | 0.008 |
| CACS, mean (SD) | 174 (448) | 98.5 (221) | 188.1 (469) | 236 (572) | NS |
| NLR-Mean | Low Risk (CACS ≤ 100) | Moderate to High Risk (CACS > 100) | p |
|---|---|---|---|
| VAI 1st tertile | 1.86 (0.67) | 1.94 (0.59) | NS |
| VAI 2nd tertile | 1.89 (0.73) | 1.94 (0.66) | NS |
| VAI 3rd tertile | 1.89 (0.74) | 2.48 (1.1) | 0.008 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Male | 2.70 | 1.48–4.93 | 0.00 | 2.61 | 1.4–4.85 | 0.00 | 2.42 | 1.29–4.53 | 0.01 | 2.08 | 1.06–4.07 | 0.03 | 2.05 | 1.03–4.08 | 0.04 |
| Age | 1.13 | 1.08–5.03 | <0.001 | 1.12 | 1.08–1.16 | <0.001 | 1.13 | 1.08–1.17 | <0.001 | 1.11 | 1.06–1.17 | <0.001 | 1.11 | 1.06–1.16 | <0.001 |
| VAI tertile 1 by NLR | 0.99 | 0.60–1.59 | NS | 1.06 | 0.65–1.72 | 0.03 | 1.09 | 0.67–1.72 | NS | 1.16 | 0.7–1.92 | NS | |||
| VAI tertile 2 by NLR | 1.09 | 0.687–1.75 | NS | 1.13 | 0.71–1.82 | NS | 1.13 | 0.69–1.86 | NS | 1.21 | 0.73–1.99 | NS | |||
| VAI tertile 3 by NLR | 1.45 | 0.97–2.18 | 0.07 | 1.56 | 1.02–2.4 | 0.04 | 1.52 | 1–2.34 | 0.05 | 1.67 | 1.06–2.62 | 0.03 | |||
| Current smoking | 2.18 | 0.82–5.7 | NS | 3.20 | 1.2–10.45 | 0.02 | 3.97 | 1.34–11.7 | 0.02 | ||||||
| BMI (kg/m2) | 1.08 | 1–1.15 | 0.02 | 1.04 | 0.97–1.1 | NS | 1.05 | 0.97–1.14 | NS | ||||||
| HLP | 1.62 | 0.83–3.15 | NS | 1.50 | 0.79–3.3 | NS | |||||||||
| HT | 3.14 | 1.4–6.87 | 0.01 | 3.14 | 1.43–6.91 | <0.01 | |||||||||
| DM | 2.25 | 0.85–5.95 | NS | 1.69 | 1.73–4.93 | NS | |||||||||
| HbA1c (%) | 1.28 | 0.81–2.04 | NS | ||||||||||||
| hsCRP (mg/L) | 0.93 | 0.82–1.05 | NS | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagyura, Z.; Kiss, L.; Lux, Á.; Csobay-Novák, C.; Jermendy, Á.L.; Polgár, L.; Tabák, Á.G.; Soós, P.; Szelid, Z.; Merkely, B.; et al. Neutrophil-to-Lymphocyte Ratio Is an Independent Risk Factor for Coronary Artery Disease in Central Obesity. Int. J. Mol. Sci. 2023, 24, 7397. https://doi.org/10.3390/ijms24087397
Bagyura Z, Kiss L, Lux Á, Csobay-Novák C, Jermendy ÁL, Polgár L, Tabák ÁG, Soós P, Szelid Z, Merkely B, et al. Neutrophil-to-Lymphocyte Ratio Is an Independent Risk Factor for Coronary Artery Disease in Central Obesity. International Journal of Molecular Sciences. 2023; 24(8):7397. https://doi.org/10.3390/ijms24087397
Chicago/Turabian StyleBagyura, Zsolt, Loretta Kiss, Árpád Lux, Csaba Csobay-Novák, Ádám L. Jermendy, Lívia Polgár, Ádám G. Tabák, Pál Soós, Zsolt Szelid, Béla Merkely, and et al. 2023. "Neutrophil-to-Lymphocyte Ratio Is an Independent Risk Factor for Coronary Artery Disease in Central Obesity" International Journal of Molecular Sciences 24, no. 8: 7397. https://doi.org/10.3390/ijms24087397
APA StyleBagyura, Z., Kiss, L., Lux, Á., Csobay-Novák, C., Jermendy, Á. L., Polgár, L., Tabák, Á. G., Soós, P., Szelid, Z., Merkely, B., Kőhidai, L., & Pállinger, É. (2023). Neutrophil-to-Lymphocyte Ratio Is an Independent Risk Factor for Coronary Artery Disease in Central Obesity. International Journal of Molecular Sciences, 24(8), 7397. https://doi.org/10.3390/ijms24087397