
Sex-Specific Models to Predict Insulin Secretion and Sensitivity in Subjects with Overweight and Obesity
 ,
,
Abstract
1. Introduction
2. Results
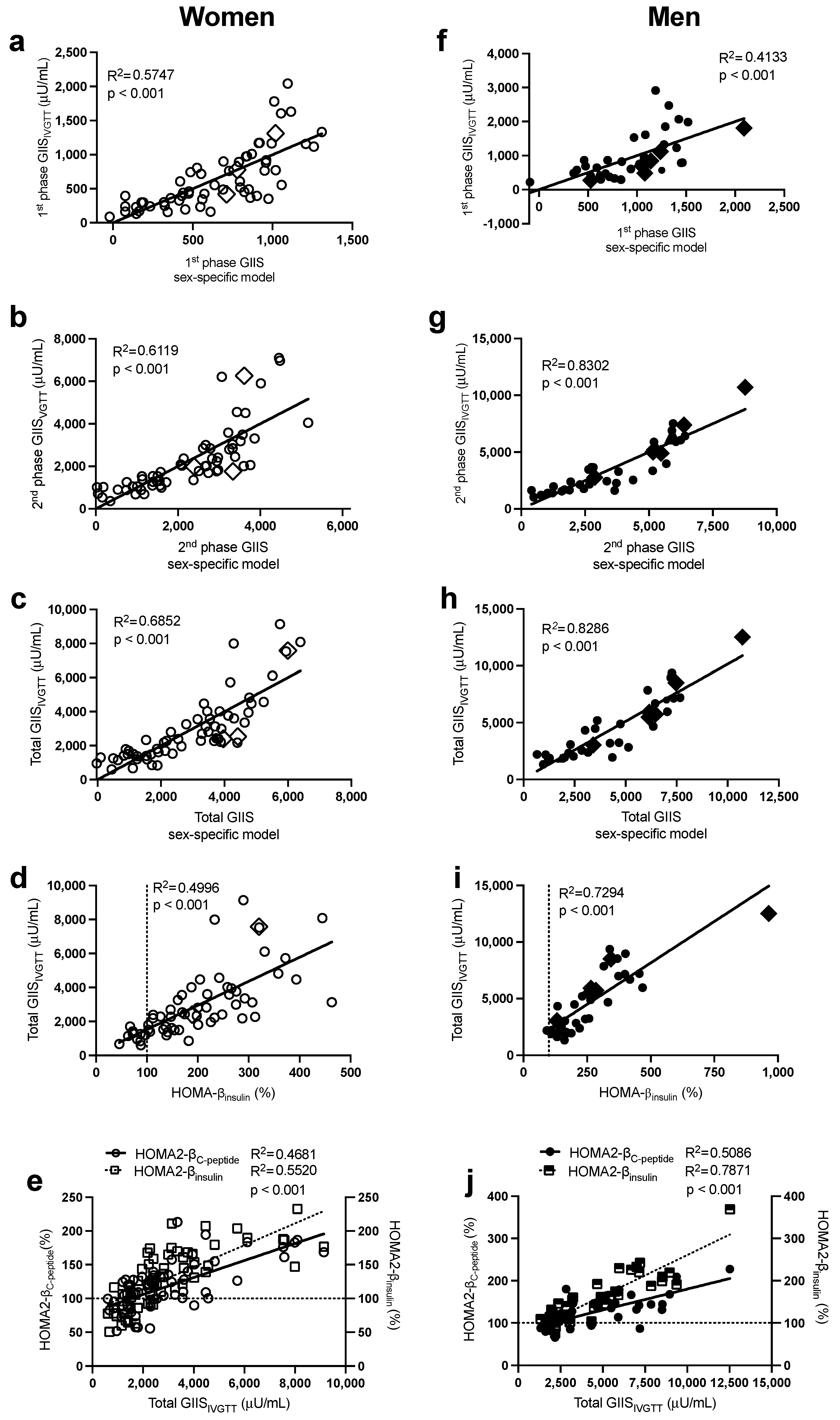
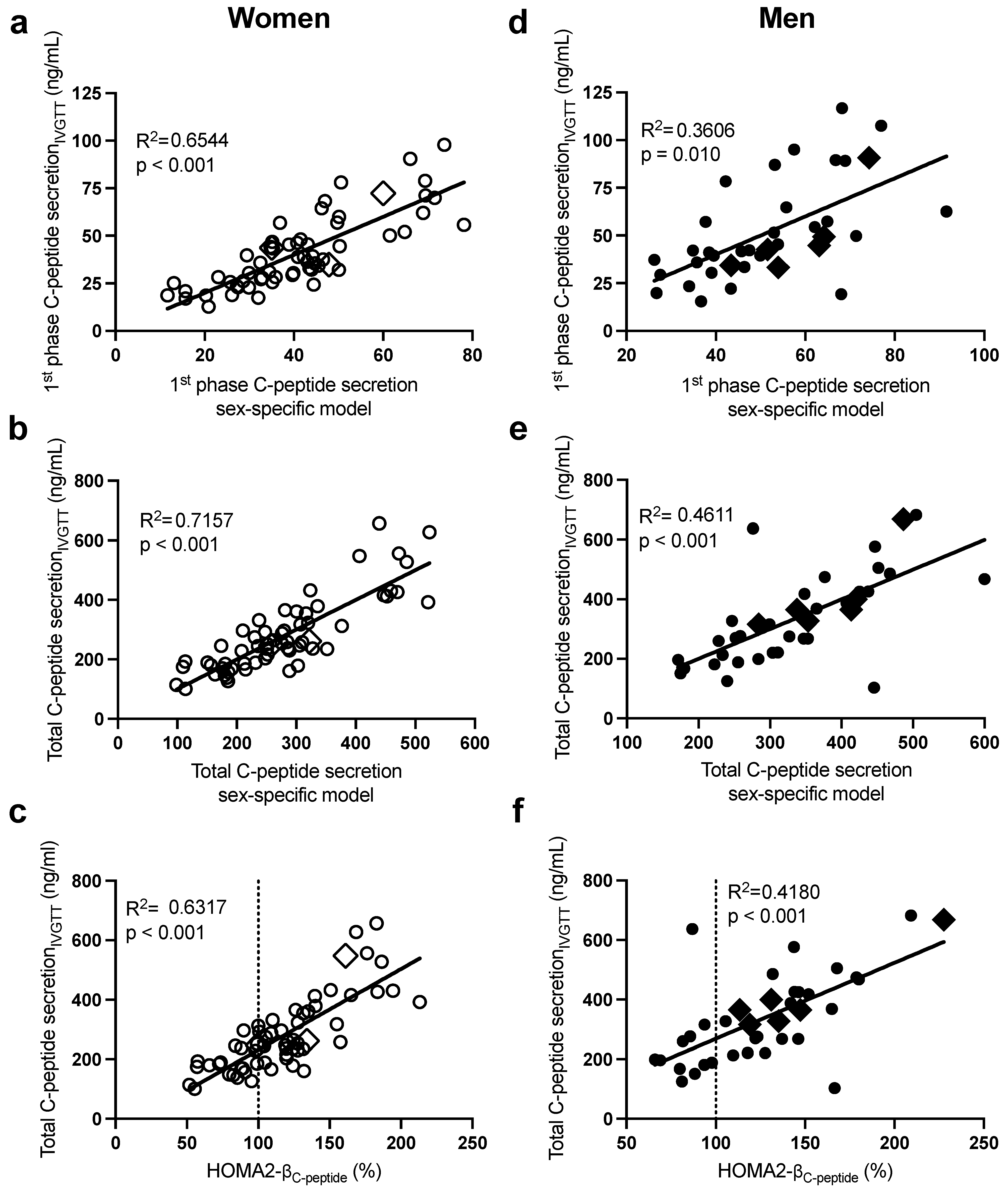
2.1. Sex-Specific Models to Predict Glucose-Induced Insulin Secretion (GIIS) Measured by the IVGTT
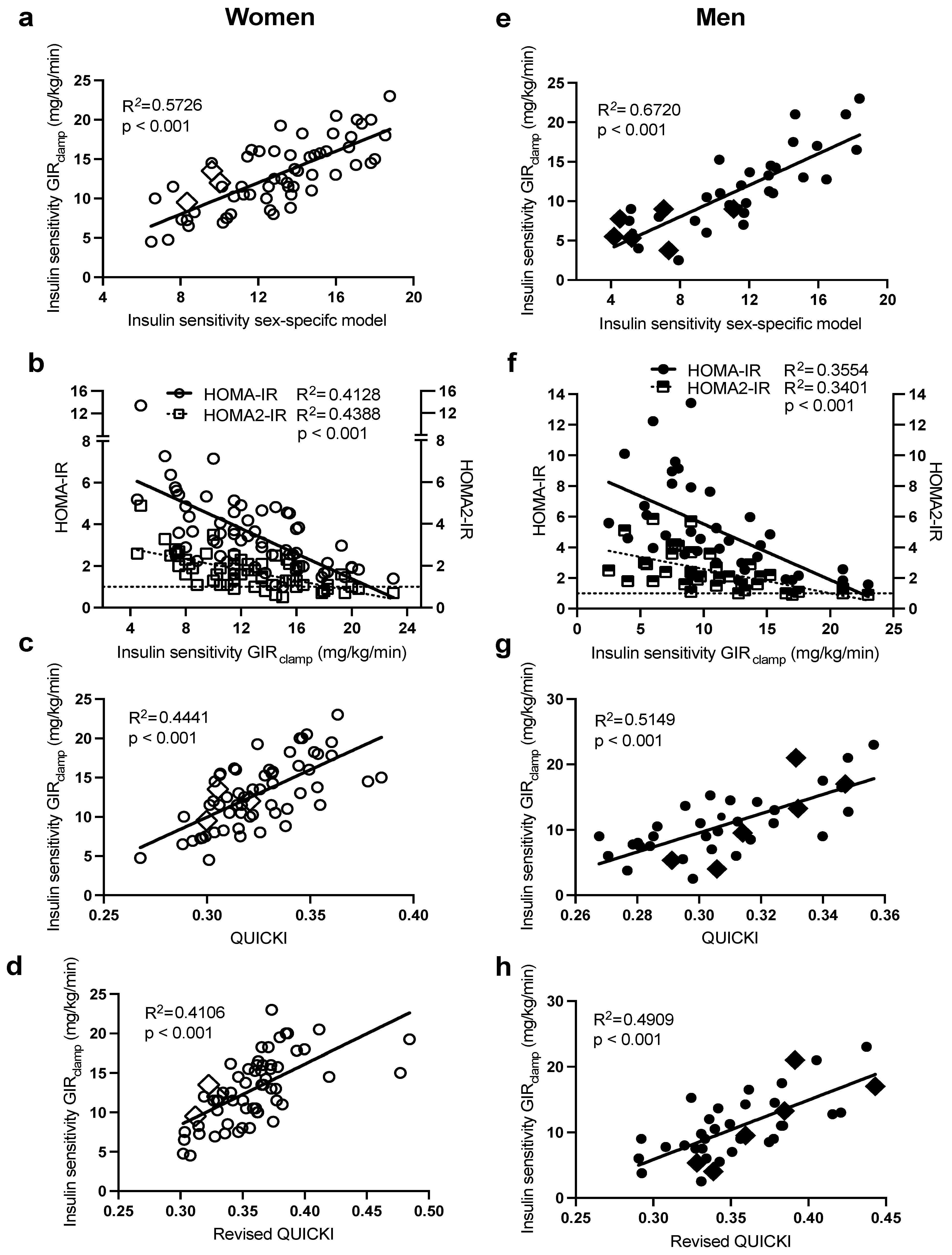
2.2. Sex-Specific Models to Predict Insulin Sensitivity (IS) Measured by the HIEG Clamp
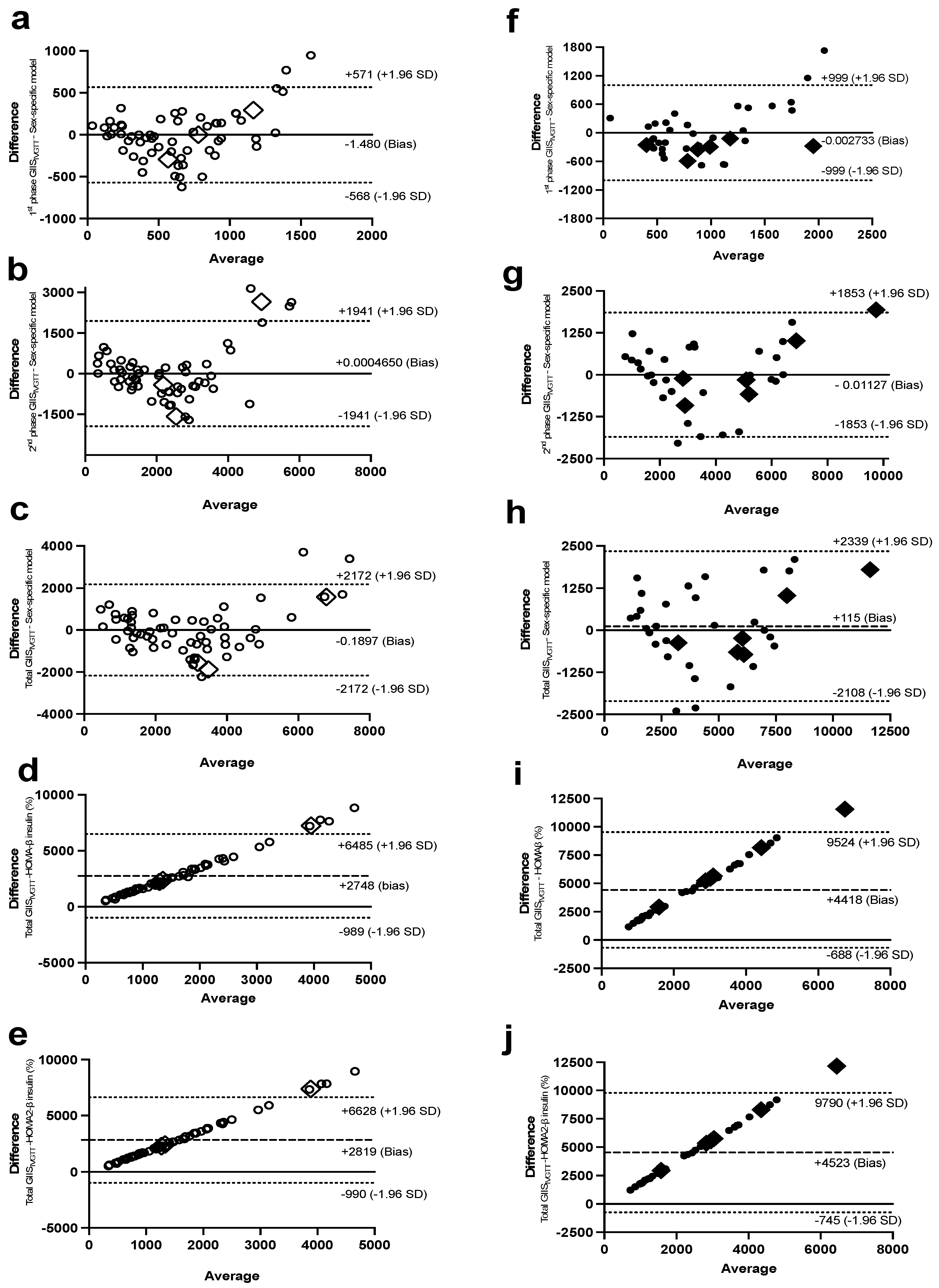
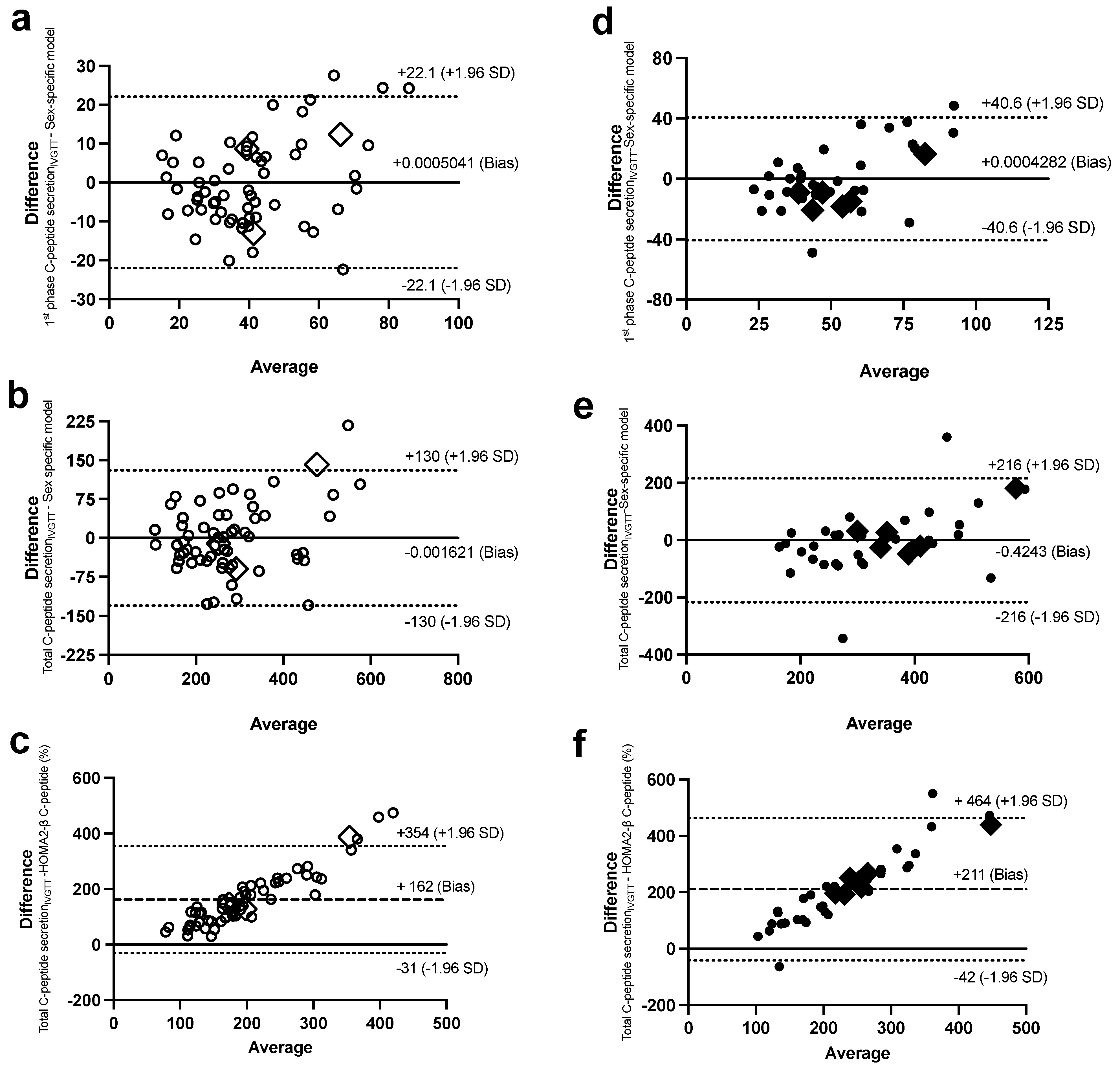
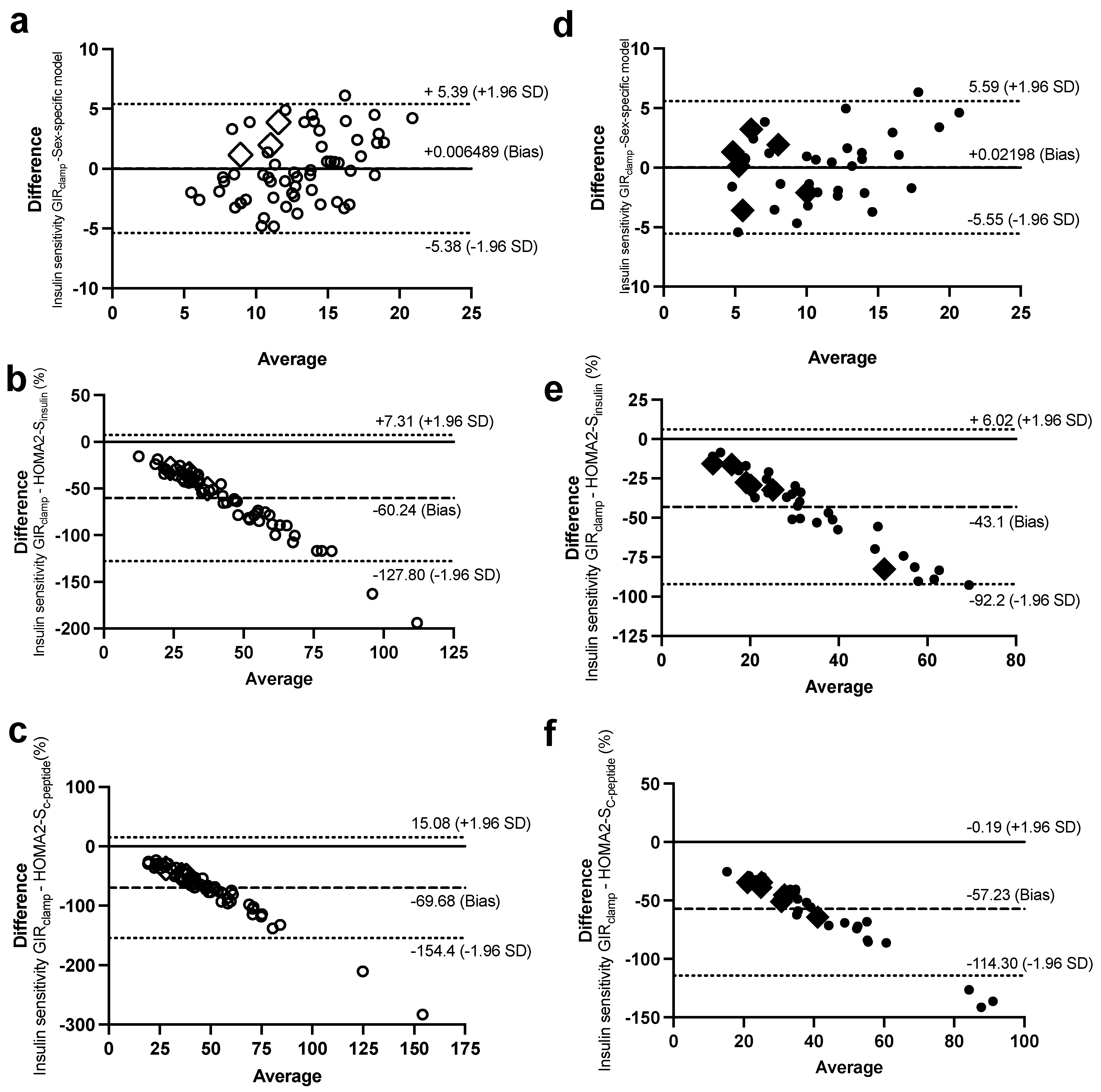
2.3. Bland–Altman Plots to Assess the Agreement with the Botnia-Clamp Data
3. Discussion
4. Methods
4.1. Study Population
4.2. Anthropometric and Biochemical Parameters
4.3. Insulin Secretion and Sensitivity
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kahn, S.E.; Cooper, M.E.; Del Prato, S. Pathophysiology and treatment of type 2 diabetes: Perspectives on the past, present, and future. Lancet 2014, 383, 1068–1083. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, C.; Wagenknecht, L.E.; Rewers, M.J.; Karter, A.J.; Bergman, R.N.; Hanley, A.J.; Haffner, S.M. Disposition Index, Glucose Effectiveness, and Conversion to Type 2 Diabetes: The Insulin Resistance Atherosclerosis Study (IRAS). Diabetes Care 2010, 33, 2098–2103. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef]
- Tripathy, D.; Wessman, Y.; Gullstrom, M.; Tuomi, T.; Groop, L. Importance of Obtaining Independent Measures of Insulin Secretion and Insulin Sensitivity During the Same Test: Results with the Botnia clamp. Diabetes Care 2003, 26, 1395–1401. [Google Scholar] [CrossRef]
- Levy, J.C.; Matthews, D.R.; Hermans, M.P. Correct homeostasis model assessment (HOMA) evaluation uses the computer program. Diabetes Care 1998, 21, 2191. [Google Scholar] [CrossRef]
- Katz, A.; Nambi, S.S.; Mather, K.; Baron, A.D.; Follmann, D.A.; Sullivan, G.; Quon, M.J. Quantitative insulin sensitivity check index: A simple, accurate method for assessing insulin sensitivity in humans. J. Clin. Endocrinol. Metab. 2000, 85, 2402–2410. [Google Scholar] [CrossRef]
- Perseghin, G.; Caumo, A.; Caloni, M.; Testolin, G.; Luzi, L. Incorporation of the fasting plasma FFA concentration into QUICKI improves its association with insulin sensitivity in nonobese individuals. J. Clin. Endocrinol. Metab. 2001, 86, 4776–4781. [Google Scholar] [CrossRef]
- Rabasa-Lhoret, R.; Bastard, J.P.; Jan, V.; Ducluzeau, P.H.; Andreelli, F.; Guebre, F.; Bruzeau, J.; Louche-Pellissier, C.; Maîtrepierre, C.; Peyrat, J.; et al. Modified Quantitative Insulin Sensitivity Check Index Is Better Correlated to Hyperinsulinemic Glucose Clamp than Other Fasting-Based Index of Insulin Sensitivity in Different Insulin-Resistant States. J. Clin. Endocrinol. Metab. 2003, 88, 4917–4923. [Google Scholar] [CrossRef]
- Muniyappa, R.; Lee, S.; Chen, H.; Quon, M.J. Current approaches for assessing insulin sensitivity and resistance in vivo: Advantages, limitations, and appropriate usage. Am. J. Physiol.-Endocrinol. Metab. 2008, 294, E15–E26. [Google Scholar] [CrossRef]
- Tramunt, B.; Smati, S.; Grandgeorge, N.; Lenfant, F.; Arnal, J.F.; Montagner, A.; Gourdy, P. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia 2020, 63, 453–461. [Google Scholar] [CrossRef]
- Bissonnette, S.; Saint-Pierre, N.; Lamantia, V.; Cyr, Y.; Wassef, H.; Faraj, M. Plasma IL-1Ra: Linking hyperapoB to risk factors for type 2 diabetes independent of obesity in humans. Nutr. Diabetes 2015, 5, e180. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Bissonnette, S.; Saint-Pierre, N.; Lamantia, V.; Leroux, C.; Provost, V.; Cyr, Y.; Rabasa-Lhoret, R.; Faraj, M. High plasma apolipoprotein B identifies obese subjects who best ameliorate white adipose tissue dysfunction and glucose-induced hyperinsulinemia after a hypocaloric diet. Am. J. Clin. Nutr. 2018, 108, 62–76. [Google Scholar] [CrossRef]
- Cerasi, E.; Luft, R. Plasma-insulin response to sustained hyperglycemia induced by glucose infusion in human subjects. Lancet 1963, 2, 1359–1361. [Google Scholar] [CrossRef]
- Barg, S.; Eliasson, L.; Renström, E.; Rorsman, P. A subset of 50 secretory granules in close contact with L-type Ca2+ channels accounts for first-phase insulin secretion in mouse beta-cells. Diabetes 2002, 51 (Suppl. 1), S74–S82. [Google Scholar] [CrossRef]
- Seino, S.; Shibasaki, T.; Minami, K. Dynamics of insulin secretion and the clinical implications for obesity and diabetes. J. Clin. Investig. 2011, 121, 2118–2125. [Google Scholar] [CrossRef]
- Cerasi, E.; Ktorza, A. Anatomical and functional plasticity of pancreatic beta-cells and type 2 diabetes. Med. Sci. 2007, 23, 885–894. [Google Scholar]
- Del Prato, S.; Tiengo, A. The importance of first-phase insulin secretion: Implications for the therapy of type 2 diabetes mellitus. Diabetes Metab. Res. Rev. 2001, 17, 164–174. [Google Scholar] [CrossRef]
- Del Prato, S. Loss of early insulin secretion leads to postprandial hyperglycaemia. Diabetologia 2003, 46 (Suppl. 1), M2–M8. [Google Scholar] [CrossRef]
- Jones, A.G.; Hattersley, A.T. The clinical utility of C-peptide measurement in the care of patients with diabetes. Diabetes Med. 2013, 30, 803–817. [Google Scholar] [CrossRef]
- Perego, C.; Da Dalt, L.; Pirillo, A.; Galli, A.; Catapano, A.L.; Norata, G.D. Cholesterol metabolism, pancreatic β-cell function and diabetes. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2019, 1865, 2149–2156. [Google Scholar] [CrossRef]
- Yazıcı, D.; Sezer, H. Insulin Resistance, Obesity and Lipotoxicity. Adv. Exp. Med. Biol. 2017, 960, 277–304. [Google Scholar]
- Faraj, M. LDL, LDL receptors, and PCSK9 as modulators of the risk for type 2 diabetes: A focus on white adipose tissue. J. Biomed. Res. 2020, 34, 251–259. [Google Scholar] [CrossRef]
- Faraj, M. Au-delà du risque cardiovasculaire: Le rôle des lipoprotéines contenant l’apoB athérogènes dans l’étiologie du diabète de type 2. Médecine des Maladies Métaboliques 2019, 13, 129–139. [Google Scholar] [CrossRef]
- Li, N.; Fu, J.; Koonen, D.P.; Kuivenhoven, J.A.; Snieder, H.; Hofker, M.H. Are hypertriglyceridemia and low HDL causal factors in the development of insulin resistance? Atherosclerosis 2014, 233, 130–138. [Google Scholar] [CrossRef]
- Bastard, J.P.; Vandernotte, J.M.; Faraj, M.; Karelis, A.D.; Messier, L.; Malita, F.M.; Garrel, D.; Prud’homme, D.; Rabasa-Lhoret, R. Relationship between the hyperinsulinemic-euglycaemic clamp and a new simple index assessing insulin sensitivity in overweight and obese postmenopausal women. Diabetes Metab. 2007, 33, 261–268. [Google Scholar] [CrossRef]
- Tura, A.; Chemello, G.; Szendroedi, J.; Göbl, C.; Færch, K.; Vrbíková, J.; Pacini, G.; Ferrannini, E.; Roden, M. Prediction of clamp-derived insulin sensitivity from the oral glucose insulin sensitivity index. Diabetologia 2018, 61, 1135–1141. [Google Scholar] [CrossRef]
- Prystupa, K.; Renklint, R.; Chninou, Y.; Otten, J.; Fritsche, L.; Hoerber, S.; Peter, A.; Birkenfeld, A.L.; Fritsche, A.; Heni, M.; et al. Comprehensive validation of fasting-based and oral glucose tolerance test-based indices of insulin secretion against gold standard measures. BMJ Open Diabetes Res. Care 2022, 10, e002909. [Google Scholar] [CrossRef]
- Knopp, J.L.; Holder-Pearson, L.; Chase, J.G. Insulin Units and Conversion Factors: A Story of Truth, Boots, and Faster Half-Truths. J. Diabetes Sci. Technol. 2019, 13, 597–600. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Women (N = 61) | Men (N = 37) | p Value |
|---|---|---|---|
| Age (years) | 58.4 ± 5.84 | 56.4 ± 7.16 | 0.147 |
| Systolic blood pressure (mmHg) 1 | 121 ± 16 | 129 ± 11 | 0.002 |
| Diastolic blood pressure (mmHg) 1 | 76 ± 9 | 81 ± 8 | 0.001 |
| Anthropometric measurements Weight (kg) | 81.8 ± 12.7 | 101 ± 19.4 | <0.001 |
| BMI (kg/m2) | 32.0 ± 4.38 | 33.3 ± 5.09 | 0.212 |
| Total fat mass (kg) | 37.2 ± 8.62 | 36.5 ± 13.3 | 0.778 |
| Lean body mass (kg) | 41.6 ± 4.73 | 61.3 ± 7.8 | <0.001 |
| Android fat mass (kg) | 3.49 ± 1.0 | 4.27 ± 1.71 | 0.015 |
| Gynoid fat mass (kg) | 6.27 ± 1.40 | 5.04 ± 2.09 | 0.002 |
| Android/gynoid (kg/kg) | 0.56 ± 0.11 | 0.87 ± 0.19 | <0.001 |
| Waist circumference (cm) | 101 ± 11.5 | 114 ± 14.0 | <0.001 |
| Hip circumference (cm) 2 | 113 ± 12.1 | 112 ± 12.7 | 0.773 |
| Waist/hip ratio | 0.90 ± 0.07 | 1.02 ± 0.06 | <0.001 |
| Fasting blood parameters Plasma glucose (mmol/L) | 5.13 ± 0.57 | 5.22 ± 0.47 | 0.424 |
| Plasma insulin (μU/mL) | 15.3 ± 7.28 | 22.1 ± 12.2 | 0.003 |
| Plasma C-peptide (ng/mL) | 2.01 ± 0.84 | 2.36 ± 0.91 | 0.062 |
| HbA1C (%) 3 | 5.65 ± 0.35 | 5.49 ± 0.50 | 0.103 |
| Plasma total cholesterol (mmol/L) | 5.54 ± 0.94 | 5.04 ± 0.95 | 0.013 |
| Plasma non-HDL cholesterol (mmol/L) | 4.03 ± 1.01 | 3.99 ± 1.00 | 0.831 |
| Plasma LDL cholesterol (mmol/L) | 3.36 ± 0.80 | 2.95 ± 0.71 | 0.010 |
| Plasma HDL cholesterol (mmol/L) | 1.51 ± 0.35 | 1.05 ± 0.20 | <0.001 |
| Plasma TG (mmol/L) | 1.48 ± 0.87 | 2.26 ± 1.61 | 0.009 |
| Plasma NEFA (mmol/L) | 0.56 ± 0.19 | 0.41 ± 0.13 | <0.001 |
| Plasma apoB (g/L) | 0.99 ± 0.26 | 1.04 ± 0.25 | 0.381 |
| Fasting indices of insulin secretion and sensitivity | |||
| HOMA-IR | 3.65 ± 1.98 | 5.19 ± 3.03 | 0.004 |
| HOMA-βinsulin (%) | 200 ± 98.5 | 260 ± 161 | 0.049 |
| HOMA2-IR | 1.70 ± 0.81 | 2.35 ± 1.24 | 0.006 |
| HOMA2-S (%) | 73.1 ± 36.8 | 54.9 ± 28.1 | 0.007 |
| HOMA2-β insulin (%) | 129 ± 42.9 | 155 ± 59.0 | 0.023 |
| HOMA2-βC-peptide (%) | 117 ± 36.4 | 127 ± 38.7 | 0.235 |
| QUICKI | 0.32 ± 0.02 | 0.31 ± 0.02 | 0.004 |
| Revised QUICKI | 0.36 ± 0.04 | 0.36 ± 0.04 | 0.781 |
| Botnia-clamp measures of insulin secretion and sensitivity | |||
| 1st-phase GIISIVGTT (μU/mL/10 min) | 654 ± 446 | 942 ± 666 | 0.024 |
| 2nd-phase GIISIVGTT (μU/mL/50 min) | 2290 ± 1589 | 3739 ± 2293 | 0.001 |
| Total GIISIVGTT (μU/mL/60 min) | 2948 ± 1975 | 4680 ± 2740 | 0.001 |
| AUCIVGTT glucose (mmol/L) | 654 ± 86.2 | 663 ± 82.8 | 0.609 |
| 1st-phase C-peptide secretionIVGTT (ng/mL/10 min) | 41.2 ± 19.1 | 51.7 ± 25.9 | 0.037 |
| Total C-peptide secretionIVGTT (ng/mL/60 min) | 279 ± 125 | 338 ± 150 | 0.049 |
| Plasma insulin at steady stateclamp (μU/mL) | 234 ± 72.5 | 261 ± 84.4 | 0.110 |
| GIRclamp (mg/kg/min) | 12.9 ± 4.21 | 10.9 ± 4.96 | 0.047 |
| Models | Steps | Independent Variables | Constant | Coefficient | R2 | p Value |
|---|---|---|---|---|---|---|
| Women 1st-phase GIISIVGTT | 178 | |||||
| 1 | Log10 Insulin | 1409 | 0.359 | <0.001 | ||
| 2 | Glucose | −303 | 0.511 | <0.001 | ||
| 3 | ApoB | 438 | 0.575 | 0.005 | ||
| 2nd-phase GIISIVGTT | −5458 | |||||
| 1 | Log10 Insulin | 5683 | 0.567 | <0.001 | ||
| 2 | ApoB | 1298 | 0.612 | 0.013 | ||
| Total GIISIVGTT | −6240 | |||||
| 1 | Log10 Insulin | 7283 | 0.548 | <0.001 | ||
| 2 | ApoB | 2632 | 0.600 | <0.001 | ||
| 3 | Glucose | −894 | 0.632 | 0.002 | ||
| 4 | Waist circumference | 31 | 0.662 | 0.036 | ||
| 5 | Log10 Triglycerides | −1963 | 0.685 | 0.049 | ||
| 1st-phase glucose-induced C-peptide secretionIVGTT | 76.0 | |||||
| 1 | C−peptide | 18.3 | 0.493 | <0.001 | ||
| 2 | Glucose | −13.9 | 0.654 | <0.001 | ||
| Total glucose-induced C-peptide secretionIVGTT | 319 | |||||
| 1 | C-peptide | 129 | 0.650 | <0.001 | ||
| 2 | Glucose | −58.1 | 0.716 | <0.001 | ||
| Insulin sensitivity (GIRclamp) | 30.9 | |||||
| 1 | Log10 Insulin | −8.37 | 0.432 | <0.001 | ||
| 2 | Waist circumference | −0.130 | 0.524 | <0.001 | ||
| 3 | HDL-C | 3.03 | 0.573 | 0.013 | ||
| Men 1st-phase GIISIVGTT | 1369 | |||||
| 1 | Log10 Insulin | 1863 | 0.285 | <0.001 | ||
| 2 | Glucose | −539 | 0.413 | 0.010 | ||
| 2nd-phase GIISIVGTT | −5934 | |||||
| 1 | Log10 Insulin | 7850 | 0.720 | <0.001 | ||
| 2 | Glucose | −1137 | 0.767 | 0.005 | ||
| 3 | BMI | 104 | 0.802 | 0.007 | ||
| 4 | Total cholesterol | 413 | 0.830 | 0.028 | ||
| Total GIISIVGTT | −4859 | |||||
| 1 | Log10 Insulin | 9652 | 0.706 | <0.001 | ||
| 2 | Glucose | −1680 | 0.778 | <0.001 | ||
| 3 | BMI | 108 | 0.804 | 0.018 | ||
| 4 | Total cholesterol | 466 | 0.829 | 0.038 | ||
| 1st-phase glucose-induced C-peptide secretionIVGTT | 11.6 | |||||
| 1 | C-peptide | 17.0 | 0.361 | <0.001 | ||
| Total glucose-induced C-peptide secretionIVGTT | 75.6 | |||||
| 1 | C-peptide | 111 | 0.461 | <0.001 | ||
| Insulin sensitivity (GIRclamp) | 55.9 | |||||
| 1 | Log10 Insulin | −8.43 | 0.434 | 0.001 | ||
| 2 | Waist circumference | −0.134 | 0.567 | 0.001 | ||
| 3 | Glucose | −3.63 | 0.672 | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beaudry, M.; Bissonnette, S.; Lamantia, V.; Devaux, M.; Faraj, M. Sex-Specific Models to Predict Insulin Secretion and Sensitivity in Subjects with Overweight and Obesity. Int. J. Mol. Sci. 2023, 24, 6130. https://doi.org/10.3390/ijms24076130
Beaudry M, Bissonnette S, Lamantia V, Devaux M, Faraj M. Sex-Specific Models to Predict Insulin Secretion and Sensitivity in Subjects with Overweight and Obesity. International Journal of Molecular Sciences. 2023; 24(7):6130. https://doi.org/10.3390/ijms24076130
Chicago/Turabian StyleBeaudry, Myriam, Simon Bissonnette, Valérie Lamantia, Marie Devaux, and May Faraj. 2023. "Sex-Specific Models to Predict Insulin Secretion and Sensitivity in Subjects with Overweight and Obesity" International Journal of Molecular Sciences 24, no. 7: 6130. https://doi.org/10.3390/ijms24076130
APA StyleBeaudry, M., Bissonnette, S., Lamantia, V., Devaux, M., & Faraj, M. (2023). Sex-Specific Models to Predict Insulin Secretion and Sensitivity in Subjects with Overweight and Obesity. International Journal of Molecular Sciences, 24(7), 6130. https://doi.org/10.3390/ijms24076130