

An Adjuvant Stem Cell Patch with Coronary Artery Bypass Graft Surgery Improves Diastolic Recovery in Porcine Hibernating Myocardium

 , ,
, , 
Abstract
1. Introduction
2. Results
2.1. Physiologic Analysis
2.2. Histologic Analysis
2.3. Inflammatory Signals
3. Discussion
Limitations
4. Materials and Methods
4.1. Animal Use
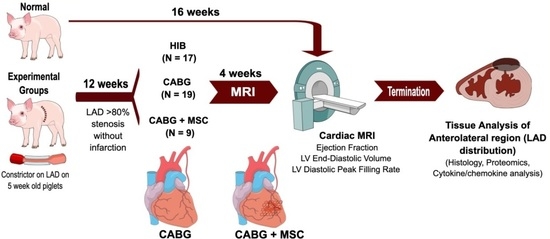
4.2. Study Design
4.3. Off-Pump CABG + Mesenchymal Stem Cell (MSC) Patch Placement
4.4. Cardiac MRI
4.5. Terminal Procedure
4.6. Isolation of Bone Marrow-Derived Mesenchymal Stem Cells (MSCs)
4.7. Creation of an Allogeneic MSC Patch
4.8. Histology
4.9. Histologic Fibrosis and Inflammation Scoring
4.10. Tissue and Protein Preparation
4.11. Western Blot
4.12. Cytokine and Chemokine Analysis
4.13. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Velazquez, E.J.; Lee, K.L.; Deja, M.A.; Jain, A.; Sopko, G.; Marchenko, A.; Ali, I.S.; Pohost, G.; Gradinac, S.; Abraham, W.T.; et al. Coronary-Artery Bypass Surgery in Patients with Left Ventricular Dysfunction. N. Engl. J. Med. 2011, 364, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Velazquez, E.J.; Lee, K.L.; Jones, R.H.; Al-Khalidi, H.R.; Hill, J.A.; Panza, J.A.; Michler, R.E.; Bonow, R.O.; Doenst, T.; Petrie, M.C.; et al. Coronary-Artery Bypass Surgery in Patients with Ischemic Cardiomyopathy. N. Engl. J. Med. 2016, 374, 1511–1520. [Google Scholar] [CrossRef] [PubMed]
- Rahimtoola, S.H. The hibernating myocardium. Am. Hear. J. 1989, 117, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Canty, J.M.; Fallavollita, J.A. Hibernating myocardium. J. Nucl. Cardiol. 2005, 12, 104–119. [Google Scholar] [CrossRef] [PubMed]
- Page, B.J.; Banas, M.D.; Suzuki, G.; Weil, B.R.; Young, R.F.; Fallavollita, J.A.; Palka, B.A.; Canty, J.M. Revascularization of Chronic Hibernating Myocardium Stimulates Myocyte Proliferation and Partially Reverses Chronic Adaptations to Ischemia. J. Am. Coll. Cardiol. 2015, 65, 684–697. [Google Scholar] [CrossRef]
- Olsen, F.J.; Lindberg, S.; Fritz-Hansen, T.; Modin, D.; Pedersen, S.; Iversen, A.; Galatius, S.; Gislason, G.; Møgelvang, R.; Biering-Sørensen, T. Prognostic Value and Interplay Between Myocardial Tissue Velocities in Patients Undergoing Coronary Artery Bypass Grafting. Am. J. Cardiol. 2020, 144, 37–45. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Hocum Stone, L.H.; Wright, C.; Chappuis, E.; Messer, M.; Ward, H.B.; McFalls, E.O.; Kelly, R.F. Surgical Swine Model of Chronic Cardiac Ischemia Treated by Off-Pump Coronary Artery Bypass Graft Surgery. J. Vis. Exp. 2018, 133, 57229. [Google Scholar] [CrossRef]
- Aggarwal, R.; Qi, S.S.; So, S.W.; Swingen, C.; Reyes, C.P.; Rose, R.; Wright, C.; Stone, L.L.H.; Nixon, J.P.; McFalls, E.O.; et al. Persistent Diastolic Dysfunction in Chronically Ischemic Hearts following Coronary Artery Bypass Graft. J. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef]
- Page, B.; Young, R.; Iyer, V.; Suzuki, G.; Lis, M.; Korotchkina, L.; Patel, M.S.; Blumenthal, K.M.; Fallavollita, J.A.; Canty, J.J.M. Persistent Regional Downregulation in Mitochondrial Enzymes and Upregulation of Stress Proteins in Swine with Chronic Hibernating Myocardium. Circ. Res. 2008, 102, 103–112. [Google Scholar] [CrossRef]
- Qu, J.; Young, R.; Page, B.J.; Shen, X.; Tata, N.; Li, J.; Duan, X.; Fallavollita, J.A.; Canty, J.J.M. Reproducible Ion-Current-Based Approach for 24-Plex Comparison of the Tissue Proteomes of Hibernating versus Normal Myocardium in Swine Models. J. Proteome Res. 2014, 13, 2571–2584. [Google Scholar] [CrossRef]
- Kelly, R.F.; Cabrera, J.A.; Ziemba, E.A.; Crampton, M.; Anderson, L.B.; McFalls, E.O.; Ward, H.B. Continued depression of maximal oxygen consumption and mitochondrial proteomic expression despite successful coronary artery bypass grafting in a swine model of hibernation. J. Thorac. Cardiovasc. Surg. 2011, 141, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Hocum Stone, L.L.H.; Swingen, C.; Holley, C.; Wright, C.; Chappuis, E.; Ward, H.B.; McFalls, E.O.; Kelly, R.F. Magnetic resonance imaging assessment of cardiac function in a swine model of hibernating myocardium 3 months following bypass surgery. J. Thorac. Cardiovasc. Surg. 2017, 153, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Baldelli, S.; Aquilano, K.; Ciriolo, M.R. PGC-1alpha buffers ROS-mediated removal of mitochondria during myogenesis. Cell Death Dis. 2014, 5, e1515. [Google Scholar] [CrossRef] [PubMed]
- Eisele, P.S.; Salatino, S.; Sobek, J.; Hottiger, M.; Handschin, C. The peroxisome proliferator-activated receptor gamma coactivator 1alpha/beta (PGC-1) coactivators repress the transcriptional activity of NF-kappaB in skeletal muscle cells. J. Biol. Chem. 2013, 288, 2246–2260. [Google Scholar] [CrossRef] [PubMed]
- Hocum Stone, L.L.H.; Swingen, C.; Wright, C.; Qi, S.S.; Rassette, M.; McFalls, E.O.; Kelly, R.F. Recovery of hibernating myocardium using stem cell patch with coronary bypass surgery. J. Thorac. Cardiovasc. Surg. 2020, 162, e3–e16. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Zhang, C. Ex vivo expansion of hematopoietic stem cells. Sci. China Life Sci. 2015, 58, 839–853. [Google Scholar] [CrossRef]
- Tajer, P.; Pike-Overzet, K.; Arias, S.; Havenga, M.; Staal, F.J. Ex Vivo Expansion of Hematopoietic Stem Cells for Therapeutic Purposes: Lessons from Development and the Niche. Cells 2019, 8, 169. [Google Scholar] [CrossRef]
- Perico, L.; Morigi, M.; Rota, C.; Breno, M.; Mele, C.; Noris, M.; Introna, M.; Capelli, C.; Longaretti, L.; Rottoli, D.; et al. Human mesenchymal stromal cells transplanted into mice stimulate renal tubular cells and enhance mitochondrial function. Nat. Commun. 2017, 8, 983. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. The Extracellular Matrix in Ischemic and Nonischemic Heart Failure. Circ. Res. 2019, 125, 117–146. [Google Scholar] [CrossRef]
- Tarbit, E.; Singh, I.; Peart, J.N.; Rose’Meyer, R.B. Biomarkers for the identification of cardiac fibroblast and myofibroblast cells. Hear. Fail. Rev. 2018, 24, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Huss, J.M.; Kelly, D.P. Mitochondrial energy metabolism in heart failure: A question of balance. J. Clin. Investig. 2005, 115, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.Q.; Jiao, Y.; Liu, Y.N.; Fu, J.Y.; Sun, L.K.; Su, J. PGC-1α protects from myocardial ischaemia-reperfusion injury by regulating mitonuclear communication. J. Cell. Mol. Med. 2021, 26, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Depre, C.; Kim, S.-J.; John, A.S.; Huang, Y.; Rimoldi, O.E.; Pepper, J.R.; Dreyfus, G.D.; Gaussin, V.; Pennell, D.J.; Vatner, D.E.; et al. Program of Cell Survival Underlying Human and Experimental Hibernating Myocardium. Circ. Res. 2004, 95, 433–440. [Google Scholar] [CrossRef]
- Finck, B.N.; Kelly, D.P. Peroxisome Proliferator–Activated Receptor γ Coactivator-1 (PGC-1) Regulatory Cascade in Cardiac Physiology and Disease. Circulation 2007, 115, 2540–2548. [Google Scholar] [CrossRef]
- Fiordelisi, A.; Iaccarino, G.; Morisco, C.; Coscioni, E.; Sorriento, D. NFkappaB is a Key Player in the Crosstalk between Inflammation and Cardiovascular Diseases. Int. J. Mol. Sci. 2019, 20, 1599. [Google Scholar] [CrossRef]
- Shake, J.G.; Gruber, P.J.; Baumgartner, W.A.; Senechal, G.; Meyers, J.; Redmond, J.; Pittenger, M.F.; Martin, B.J. Mesenchymal stem cell implantation in a swine myocardial infarct model: Engraftment and functional effects. Ann. Thorac. Surg. 2002, 73, 1919–1926. [Google Scholar] [CrossRef]
- Discher, D.E.; Mooney, D.J.; Zandstra, P.W. Growth Factors, Matrices, and Forces Combine and Control Stem Cells. Science 2009, 324, 1673–1677. [Google Scholar] [CrossRef]
- Keating, A. Mesenchymal Stromal Cells: New Directions. Cell Stem Cell. 2012, 10, 709–716. [Google Scholar] [CrossRef]
- Aggarwal, S.; Pittenger, M.F. Human mesenchymal stem cells modulate allogeneic immune cell responses. Blood 2005, 105, 1815–1822. [Google Scholar] [CrossRef]
- Hare, J.M.; Fishman, J.E.; Gerstenblith, G.; Velazquez, D.L.D.; Zambrano, J.P.; Suncion, V.Y.; Tracy, M.; Ghersin, E.; Johnston, P.V.; Brinker, J.A.; et al. Comparison of Allogeneic vs Autologous Bone Marrow–Derived Mesenchymal Stem Cells Delivered by Transendocardial Injection in Patients with Ischemic Cardiomyopathy. JAMA 2012, 308, 2369–2379. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Wollert, K.C.; Meyer, G.P.; Menke, A.; Arseniev, L.; Hertenstein, B.; Ganser, A.; Knapp, W.H.; Drexler, H. Monitoring of Bone Marrow Cell Homing Into the Infarcted Human Myocardium. Circulation 2005, 111, 2198–2202. [Google Scholar] [CrossRef]
- Zimmermann, W.-H.; Eschenhagen, T. Cardiac tissue engineering for replacement therapy. Heart Fail. Rev. 2003, 8, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Lim, K.S.; Oh, J.-E.; Yoon, A.-R.; Joo, W.S.; Kim, H.S.; Yun, C.-O.; Kim, S.W. Development of porous PLGA/PEI1.8k biodegradable microspheres for the delivery of mesenchymal stem cells (MSCs). J. Control. Release 2015, 205, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Stone, L.H.; Chappuis, E.; Wright, C.; Kelly, R.F.; McFalls, E.O. CoQ10 enhances PGC1α and increases expression of mitochondrial antioxidant proteins in chronically ischemic swine myocardium. Nutr. Metab. 2019, 16, 92. [Google Scholar] [CrossRef] [PubMed]
- Hughey, C.C.; James, F.D.; Ma, L.; Bracy, D.P.; Wang, Z.; Wasserman, D.H.; Rottman, J.N.; Shearer, J. Diminishing impairments in glucose uptake, mitochondrial content, and ADP-stimulated oxygen flux by mesenchymal stem cell therapy in the infarcted heart. Am. J. Physiol. Physiol. 2014, 306, C19–C27. [Google Scholar] [CrossRef]
- Deng, Y.; Xie, M.; Li, Q.; Xu, X.; Ou, W.; Zhang, Y.; Xiao, H.; Yu, H.; Zheng, Y.; Liang, Y.; et al. Targeting Mitochondria-Inflammation Circuit by β-Hydroxybutyrate Mitigates HFpEF. Circ. Res. 2021, 128, 232–245. [Google Scholar] [CrossRef]
- Holley, C.T.; Long, E.K.; Butterick, T.A.; Duffy, C.M.; Lindsey, M.E.; Stone, L.H.; McFalls, E.O.; Kelly, R.F. Mitochondrial fusion proteins in revascularized hibernating hearts. J. Surg. Res. 2015, 195, 29–36. [Google Scholar] [CrossRef]
- Tornatore, L.; Thotakura, A.K.; Bennett, J.; Moretti, M.; Franzoso, G. The nuclear factor kappa B signaling pathway: Integrating metabolism with inflammation. Trends Cell Biol. 2012, 22, 557–566. [Google Scholar] [CrossRef]
- McFalls, E.O.; Kelly, R.F.; Hu, Q.; Mansoor, A.; Lee, J.; Kuskowski, M.; Sikora, J.; Ward, H.B.; Zhang, J. The energetic state within hibernating myocardium is normal during dobutamine despite inhibition of ATP-dependent potassium channel opening with glibenclamide. Am. J. Physiol. Circ. Physiol. 2007, 293, H2945–H2951. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grades of Fibrosis | Interstitial Fibrosis | Scoring of Inflammation | Severity of Inflammation |
|---|---|---|---|
| 1 | Limited in perimysium | A | No cells |
| 2 | Focally extending into endomysium | B | 1–5 cells/HPF |
| 3 | Multiple extension into endomysium | C | 5–10 cells/HPF |
| 4 | Diffusely extending into endomysium | D | 11–20 cells/HPF |
| 5 | Replacement fibrosis | E | >20 cells/HPF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aggarwal, R.; Potel, K.N.; Shao, A.; So, S.W.; Swingen, C.; Reyes, C.P.; Rose, R.; Wright, C.; Hocum Stone, L.L.; McFalls, E.O.; et al. An Adjuvant Stem Cell Patch with Coronary Artery Bypass Graft Surgery Improves Diastolic Recovery in Porcine Hibernating Myocardium. Int. J. Mol. Sci. 2023, 24, 5475. https://doi.org/10.3390/ijms24065475
Aggarwal R, Potel KN, Shao A, So SW, Swingen C, Reyes CP, Rose R, Wright C, Hocum Stone LL, McFalls EO, et al. An Adjuvant Stem Cell Patch with Coronary Artery Bypass Graft Surgery Improves Diastolic Recovery in Porcine Hibernating Myocardium. International Journal of Molecular Sciences. 2023; 24(6):5475. https://doi.org/10.3390/ijms24065475
Chicago/Turabian StyleAggarwal, Rishav, Koray N. Potel, Annie Shao, Simon W. So, Cory Swingen, Christina P. Reyes, Rebecca Rose, Christin Wright, Laura L. Hocum Stone, Edward O. McFalls, and et al. 2023. "An Adjuvant Stem Cell Patch with Coronary Artery Bypass Graft Surgery Improves Diastolic Recovery in Porcine Hibernating Myocardium" International Journal of Molecular Sciences 24, no. 6: 5475. https://doi.org/10.3390/ijms24065475
APA StyleAggarwal, R., Potel, K. N., Shao, A., So, S. W., Swingen, C., Reyes, C. P., Rose, R., Wright, C., Hocum Stone, L. L., McFalls, E. O., Butterick, T. A., & Kelly, R. F. (2023). An Adjuvant Stem Cell Patch with Coronary Artery Bypass Graft Surgery Improves Diastolic Recovery in Porcine Hibernating Myocardium. International Journal of Molecular Sciences, 24(6), 5475. https://doi.org/10.3390/ijms24065475