
Applying Metagenomic Analysis Using Nanopore Sequencer (MinION) for Precision Medicine in Bacterial Keratoconjunctivitis: Comprehensive Validation of Molecular Biological and Conventional Examinations

Abstract
1. Introduction
2. Results (Table 1)
2.1. Smear Microscopy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Smear | Culture | Dominant Species 6 | Reads 7 | Ave. 8 | Abundance (%) 9 |
|---|---|---|---|---|---|---|---|---|
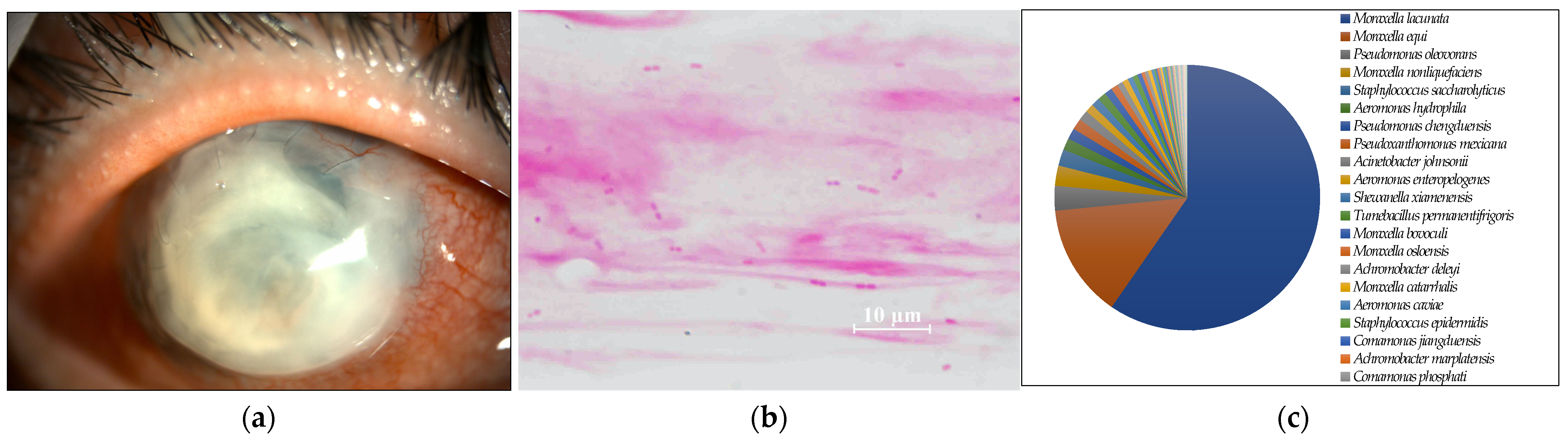
| 1 | 45 | M | GNR 1 | Negative | M. lacunata | 832 | 2000 | 70.5 |
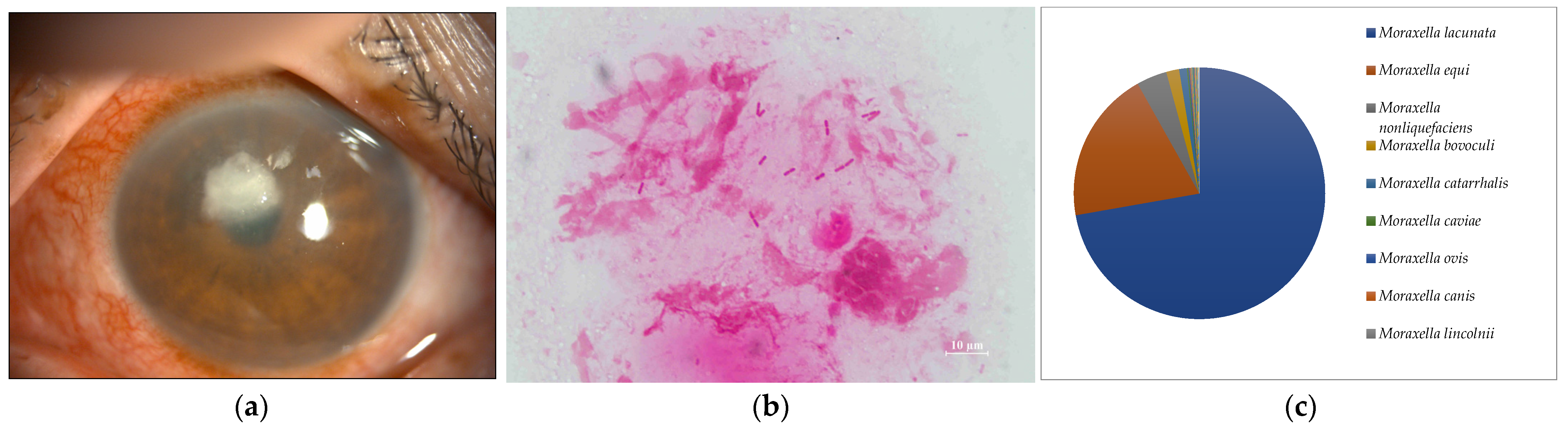
| 2 | 73 | F | GNR | Negative | M. lacunata | 24,969 | 2000 | 72.2 |
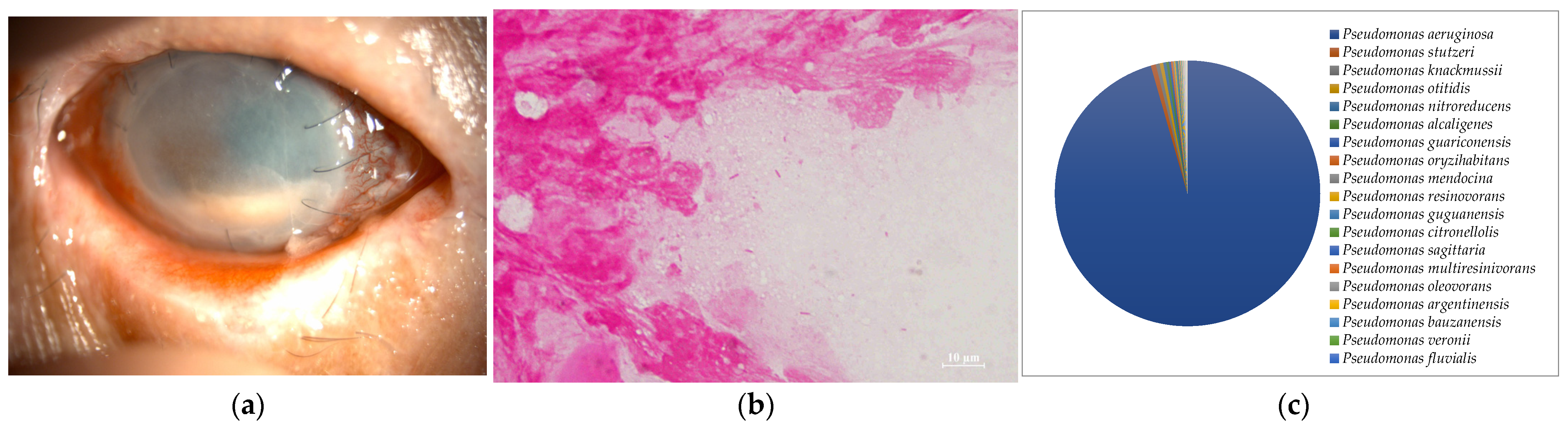
| 3 | 76 | M | GNR | P. aeruginosa | P. aeruginosa | 2357 | 2000 | 95.4 |
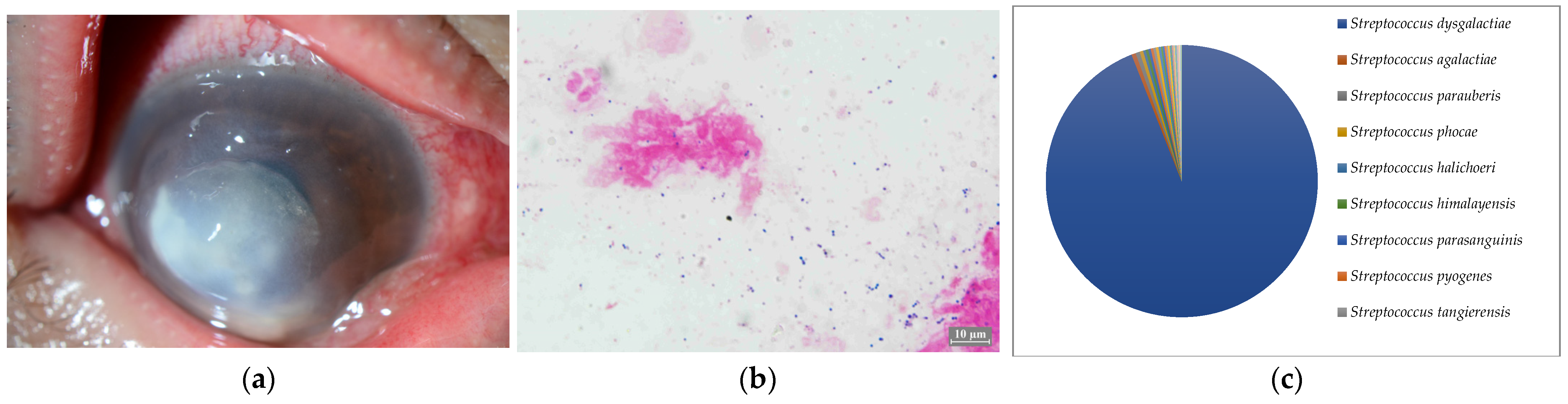
| 4 | 56 | M | GPC 2 | SDSE 5 | SDSE | 982 | 2000 | 94.0 |
| 5 | 83 | M | GPC | Str. pneumoniae | Str. pneumoniae | 25 | 1988 | 64.0 |
| 6 | 79 | F | GPR 3 | Corynebacterium | None | 93 | 1187 | 44.1 |
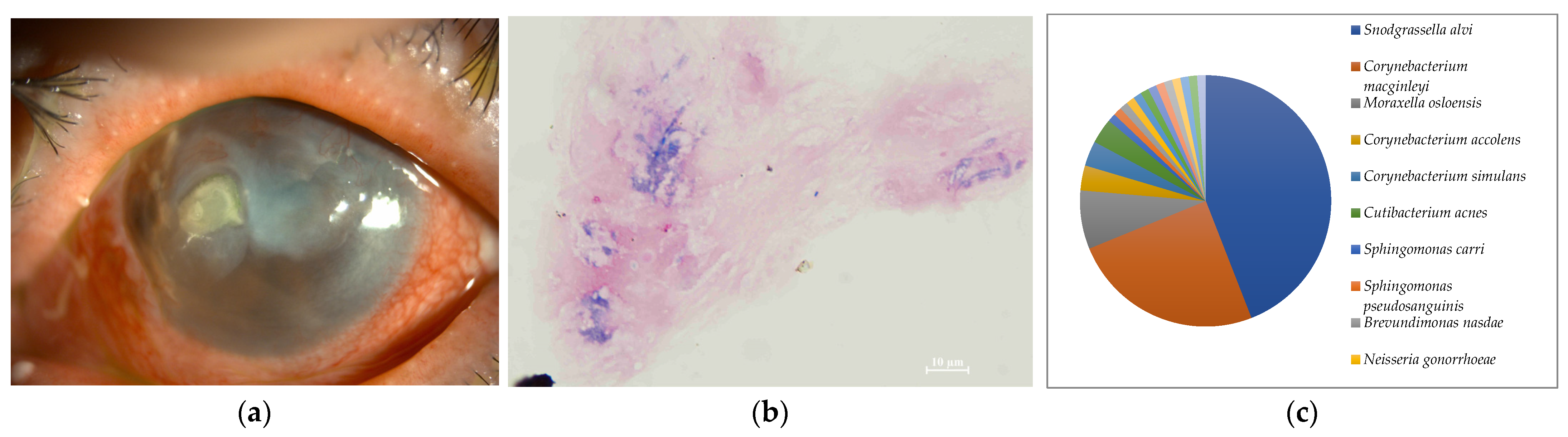
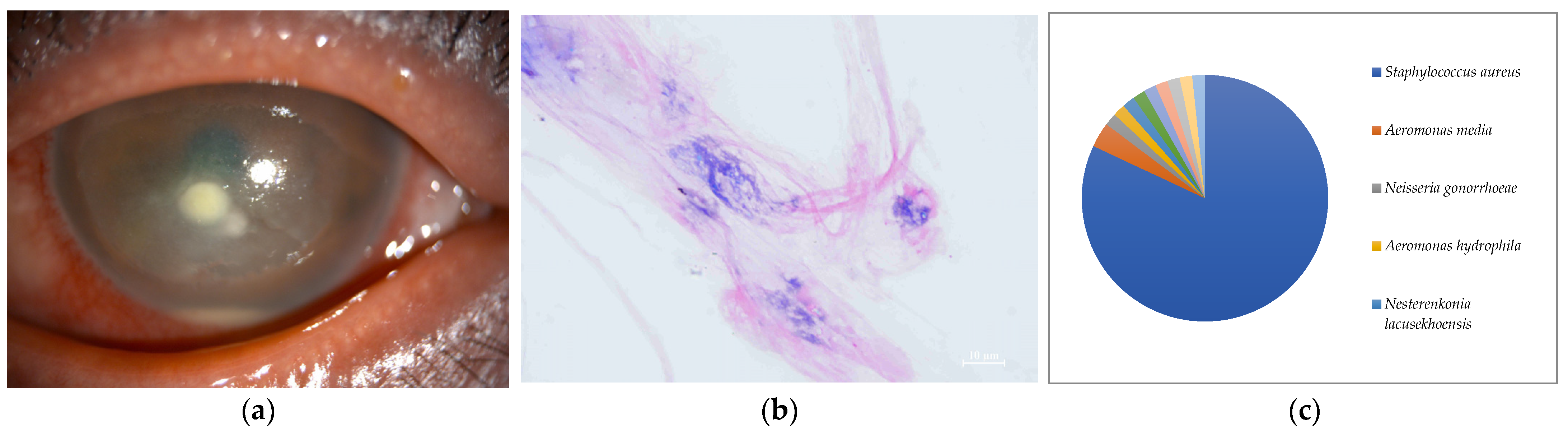
| 7 | 47 | M | Negative | Negative | S. aureus | 61 | 2000 | 81.9 |
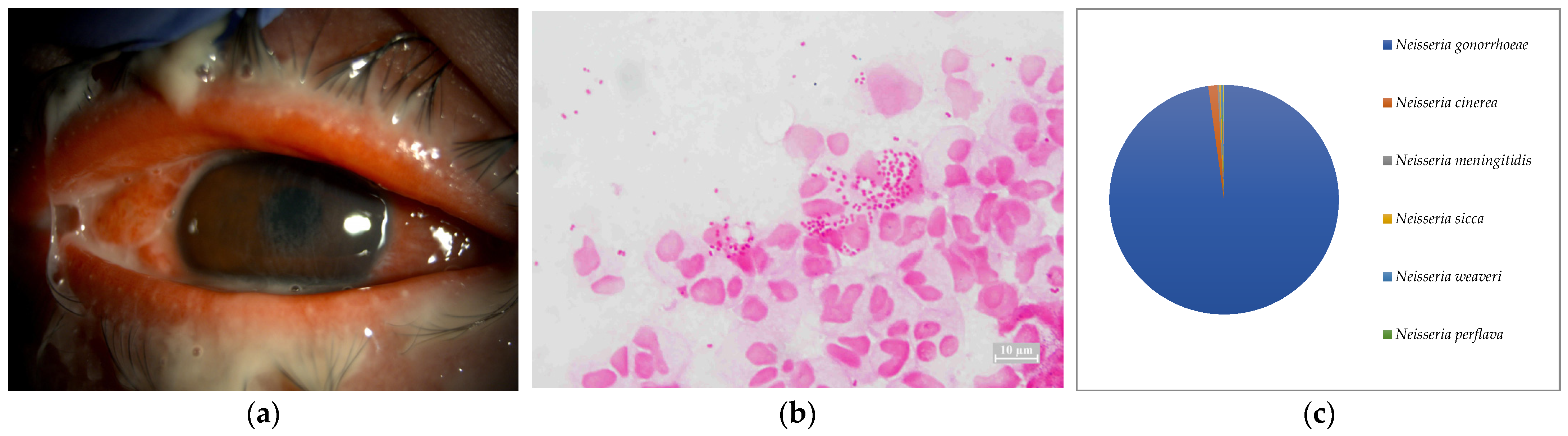
| 8 | 38 | M | GNC 4 | N. gonorrhoeae | N. gonorrhoeae | 5335 | 2000 | 97.8 |








2.2. Culture
2.3. Nanopore Sequencing by the MinION
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ung, L.; Acharya, N.R.; Agarwal, T.; Alfonso, E.C.; Bagga, B.; Bispo, P.J.; Burton, M.J.; Dart, J.K.; Doan, T.; Fleiszig, S.M.; et al. Infectious corneal ulceration: A proposal for neglected tropical disease status. Bull World Health Organ 2019, 97, 854–856. [Google Scholar] [CrossRef]
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef]
- Johnson, D.; Liu, D.; Simel, D. Does this patient with acute infectious conjunctivitis have a bacterial infection? The rational clinical examination systematic review. JAMA 2022, 327, 2231–2237. [Google Scholar] [CrossRef]
- Smith, A.F.; Waycaster, C. Estimate of the direct and indirect annual cost of bacterial conjunctivitis in the United States. BMC Ophthalmol. 2009, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Levey, S.B.; Katz, H.R.; Abrams, D.A.; Hirschbein, M.J.; Marsh, M.J. The role of cultures in the management of ulcerative keratitis. Cornea 1997, 16, 383–386. [Google Scholar] [CrossRef]
- Amann, R.I.; Ludwig, W.; Schleifer, K.H. Phylogenetic identification and in situ detection of individual microbial cells without cultivation. Microbiol. Rev. 1995, 59, 154–196. [Google Scholar] [CrossRef]
- Hoffman, J.J.; Dart, J.G.; De, S.K.; Carnt, N.; Cleary, G.; Hau, S. Comparison of culture, confocal microscopy and PCR in routine hospital use for microbial keratitis diagnosis. Eye 2022, 36, 2172–2178. [Google Scholar] [CrossRef] [PubMed]
- Somerville, T.; Caroline, C.E.; Sueke, H.; Neal, T.; Kaye, S.B. 16S ribosomal RNA PCR versus conventional diagnostic culture in the investigation of suspected bacterial keratitis. Trans. Vis. Sci. Technol. 2020, 9, 2. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, D.; Miyazaki, D.; Ehara, F.; Shimizu, Y.; Uotani, R.; Inata, K.; Sasaki, S.I.; Inoue, Y. Effectiveness of 16S ribosomal DNA real-time PCR and sequencing for diagnosing bacterial keratitis. Graefes. Arch. Clin. Exp. Ophthalmol. 2020, 258, 157–166. [Google Scholar] [CrossRef]
- Knox, C.M.; Cevellos, V.; Dean, D. 16S ribosomal DNA typing for identification of pathogens in patients with bacterial keratitis. J. Clin. Microbiol. 1998, 36, 3492–3496. [Google Scholar] [CrossRef]
- Lecuit, M.; Eloit, M. The diagnosis of infectious diseases by whole genome next generation sequencing: A new era is opening. Front. Cell Infect. Microbiol. 2014, 4, 25. [Google Scholar] [CrossRef]
- Eguchi, H.; Ozkan, J.; Holland, M.J. Editorial: Next-generation sequencing in ophthalmology: The microbiome in ocular health and disease. Front. Cell Infect. Microbiol. 2022, 10, 1711. [Google Scholar] [CrossRef]
- Leggett, R.M.; Alcon-Giner, C.; Heavens, D.; Caim, S.; Brook, T.C.; Magdalena, K.; Martin, S.; Peel, N.; Acford-Palmer, H.; Hoyles, L.; et al. Rapid MinION profiling of preterm microbiota and antimicrobial-resistant pathogens. Nat. Microbiol. 2020, 5, 430–442. [Google Scholar] [CrossRef] [PubMed]
- Pallerla, S.R.; Dong, D.V.; Linh, L.T.K.; Son, T.V.; Quyen, D.T.; Hoan, P.Q.; Trung, N.T.; The, N.T.; Rüter, J.; Boutin, S.; et al. Diagnosis of pathogens causing bacterial meningitis using Nanopore sequencing in a resource-limited setting. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 39. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.; Kim, N.; Kim, T.J.; Jun, J.S.; Lee, H.S.; Shin, H.R.; Lee, S.T.; Jung, K.H.; Park, K.I.; Jung, K.Y.; et al. Rapid diagnosis of bacterial meningitis by nanopore 16S amplicon sequencing: A pilot study. Int. J. Med. Microbiol. 2019, 309, 151338. [Google Scholar] [CrossRef]
- Huang, Q.; Fu, A.; Wang, Y.; Zhang, J.; Zhao, W.; Cheng, Y. Microbiological diagnosis of endophthalmitis using nanopore targeted sequencing. Clin. Exp. Ophthalmol. 2021, 49, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Tarumoto, N.; Amo, K.; Takahashi, M.; Sakamoto, N.; Kosaka, A.; Kato, Y.; Mikita, K.; Sakai, J.; Murakami, T.; et al. Non-invasive diagnosis of cutaneous leishmaniasis by the direct boil loop-mediated isothermal amplification methods and MinIONTM nanopore sequencing. Parasitol. Int. 2018, 67, 34–37. [Google Scholar] [CrossRef]
- Inoue, H.; Suzuki, T.; Inoue, T.; Hattori, T.; Nejima, R.; Todokoro, D.; Hoshi, S.; Eguchi, H.; Miyamoto, H.; Ohashi, Y. Clinical characteristics and bacterialical profile of Moraxella keratitis. Cornea 2015, 34, 1105–1109. [Google Scholar] [CrossRef]
- Buchanan, R.E.; Gibbons, N.E. Manual of Determinative Bacteriology, 8th ed.; Wilkins: Baltimore, MD, USA, 1974; pp. 427–436. [Google Scholar]
- Liu, C.; Zhang, L.; Liu, L.; Wang, Y.; Cui, Y.; Liang, T.; Chen, T.; Jiang, Y.; Liu, G.; Li, L. Case report: First case of endophthalmitis caused by an emerging pathogen: Nocardia huaxiensis. Front. Public Health 2022, 10, 933851. [Google Scholar] [CrossRef]
- Weidinger, S.; Beck, L.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Primers. 2018, 4, 1. [Google Scholar] [CrossRef]
- Martinson, V.G.; Moy, J.; Moran, N.A. Establishment of characteristic but bacteria during development of the honeybee worker. Appl. Environ. Microbiol. 2012, 78, 2830–2840. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eguchi, H.; Hotta, F.; Kusaka, S. Applying Metagenomic Analysis Using Nanopore Sequencer (MinION) for Precision Medicine in Bacterial Keratoconjunctivitis: Comprehensive Validation of Molecular Biological and Conventional Examinations. Int. J. Mol. Sci. 2023, 24, 2611. https://doi.org/10.3390/ijms24032611
Eguchi H, Hotta F, Kusaka S. Applying Metagenomic Analysis Using Nanopore Sequencer (MinION) for Precision Medicine in Bacterial Keratoconjunctivitis: Comprehensive Validation of Molecular Biological and Conventional Examinations. International Journal of Molecular Sciences. 2023; 24(3):2611. https://doi.org/10.3390/ijms24032611
Chicago/Turabian StyleEguchi, Hiroshi, Fumika Hotta, and Shunji Kusaka. 2023. "Applying Metagenomic Analysis Using Nanopore Sequencer (MinION) for Precision Medicine in Bacterial Keratoconjunctivitis: Comprehensive Validation of Molecular Biological and Conventional Examinations" International Journal of Molecular Sciences 24, no. 3: 2611. https://doi.org/10.3390/ijms24032611
APA StyleEguchi, H., Hotta, F., & Kusaka, S. (2023). Applying Metagenomic Analysis Using Nanopore Sequencer (MinION) for Precision Medicine in Bacterial Keratoconjunctivitis: Comprehensive Validation of Molecular Biological and Conventional Examinations. International Journal of Molecular Sciences, 24(3), 2611. https://doi.org/10.3390/ijms24032611