
Alterations in Intratumoral Immune Response before and during Early-On Nivolumab Treatment for Unresectable Advanced or Recurrent Gastric Cancer
 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Results
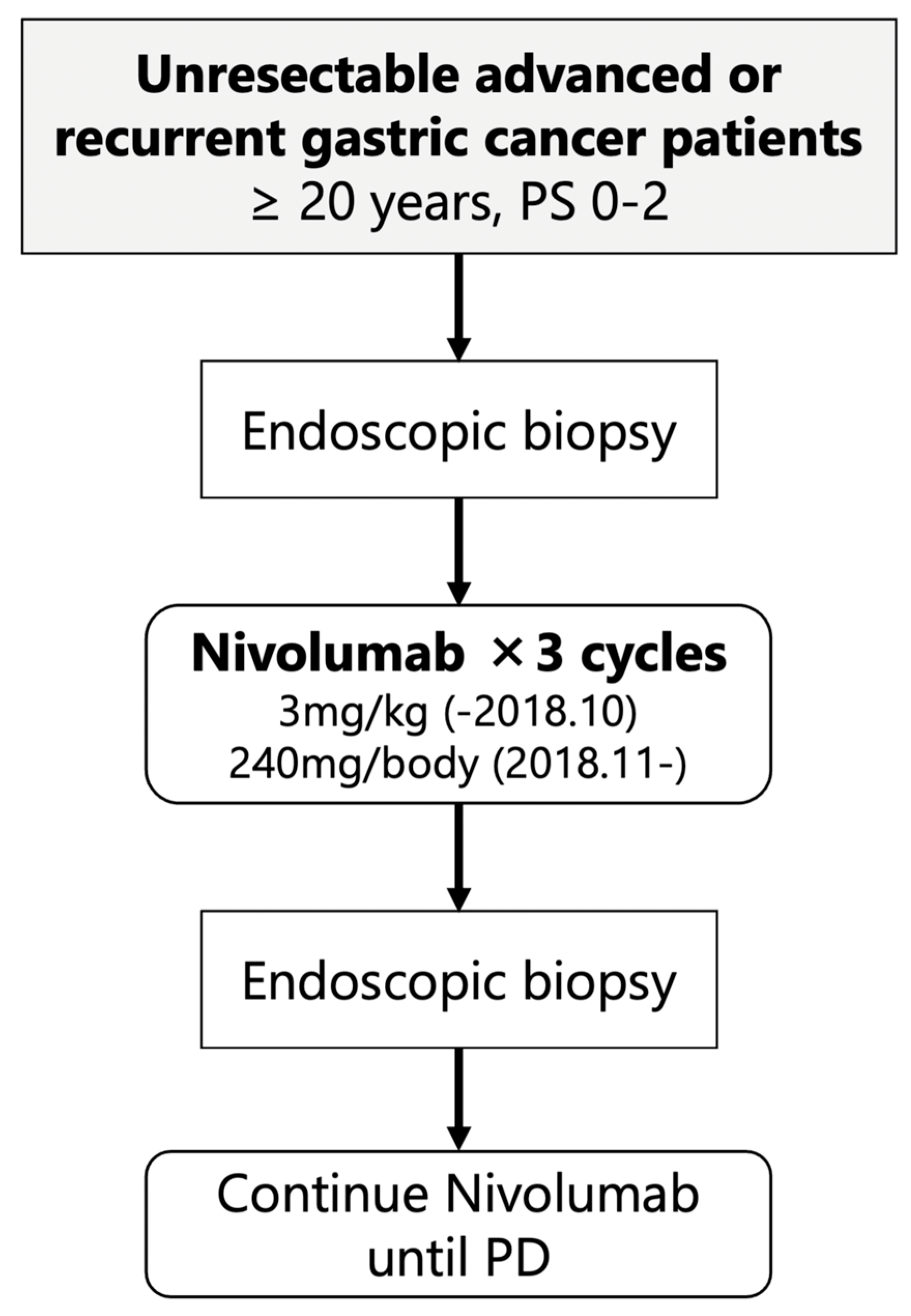
2.1. Study Design and Baseline Characteristic
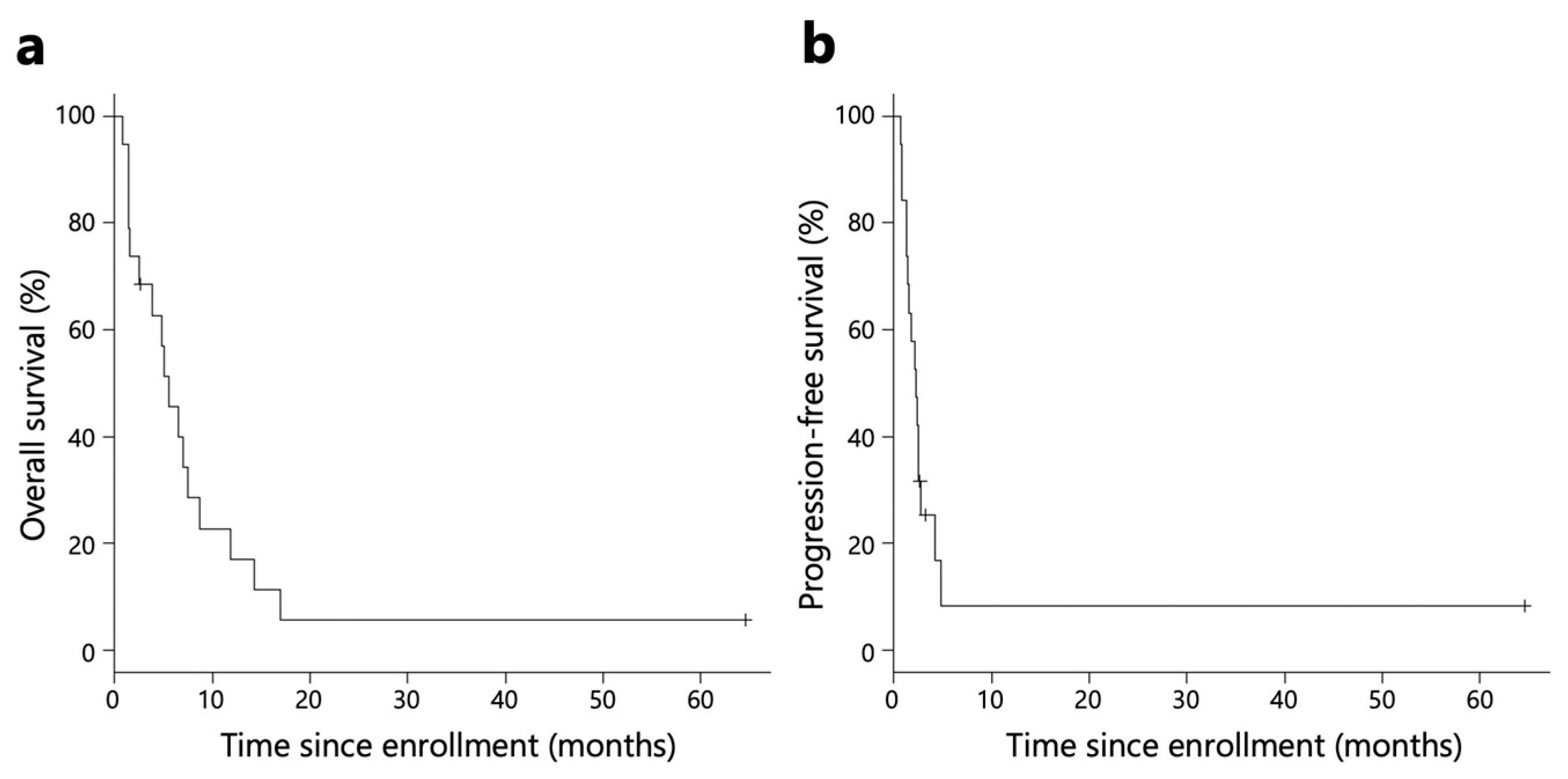
2.2. Efficacy of Nivolumab Monotherapy
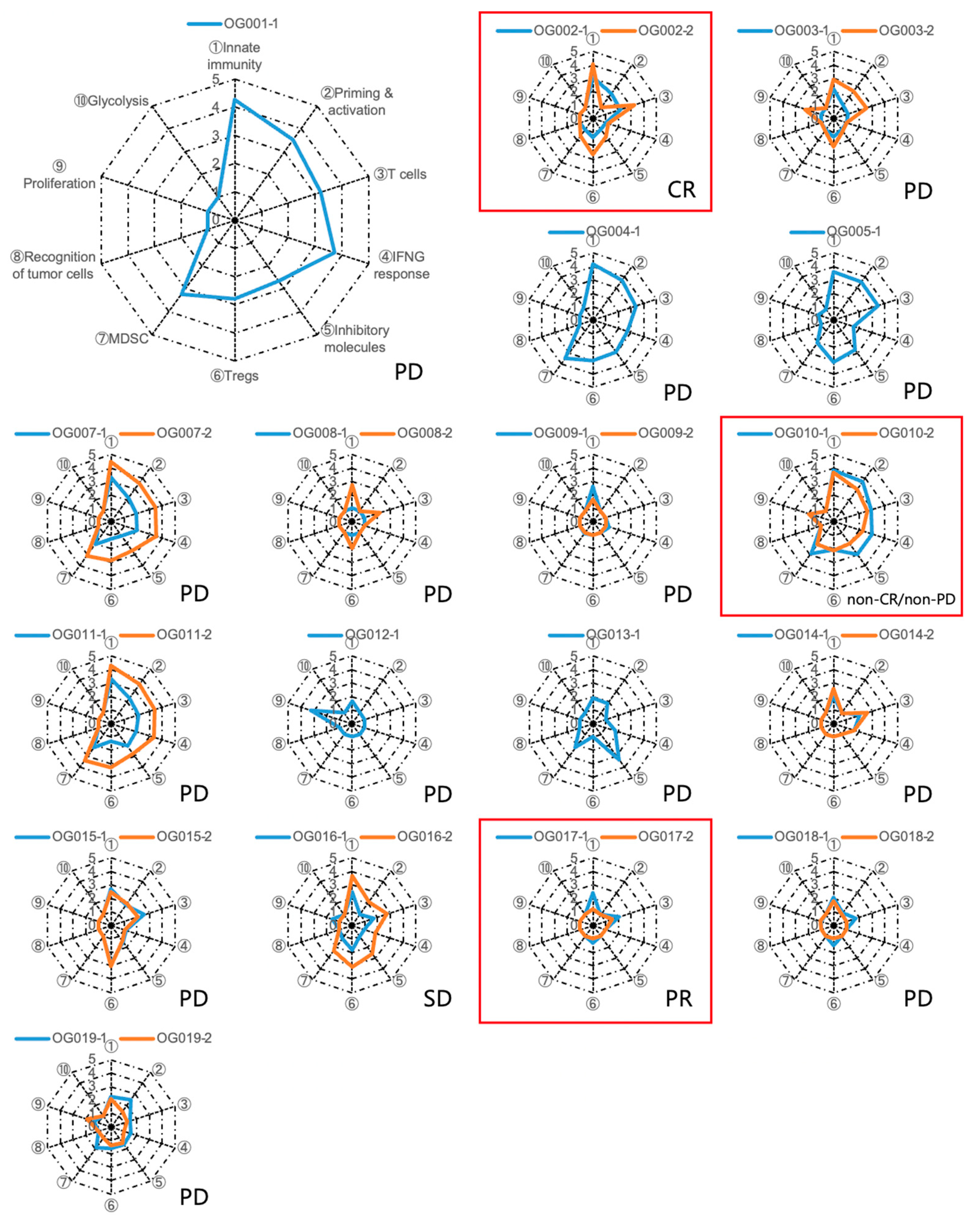
2.3. Immunogram Analysis
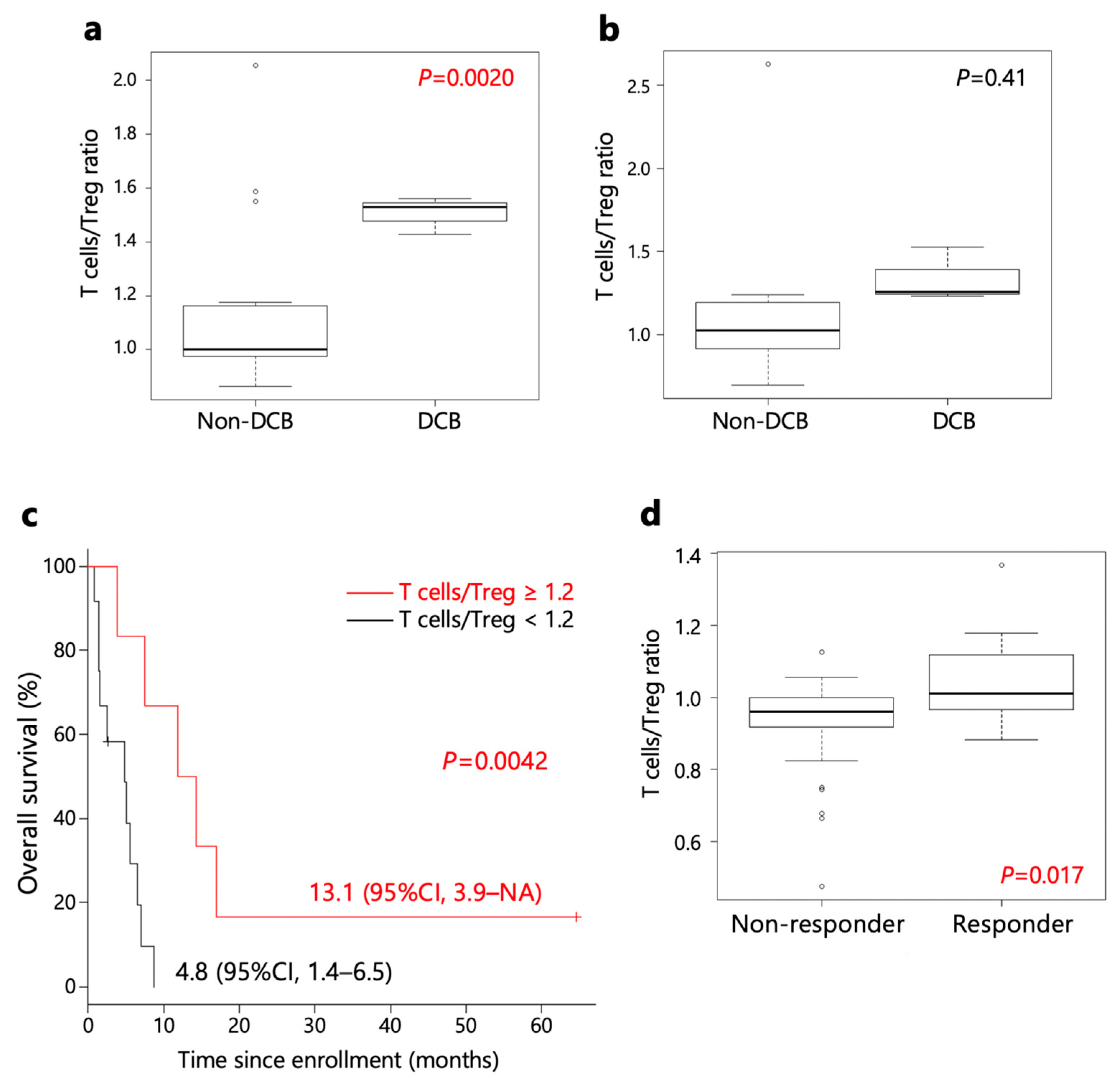
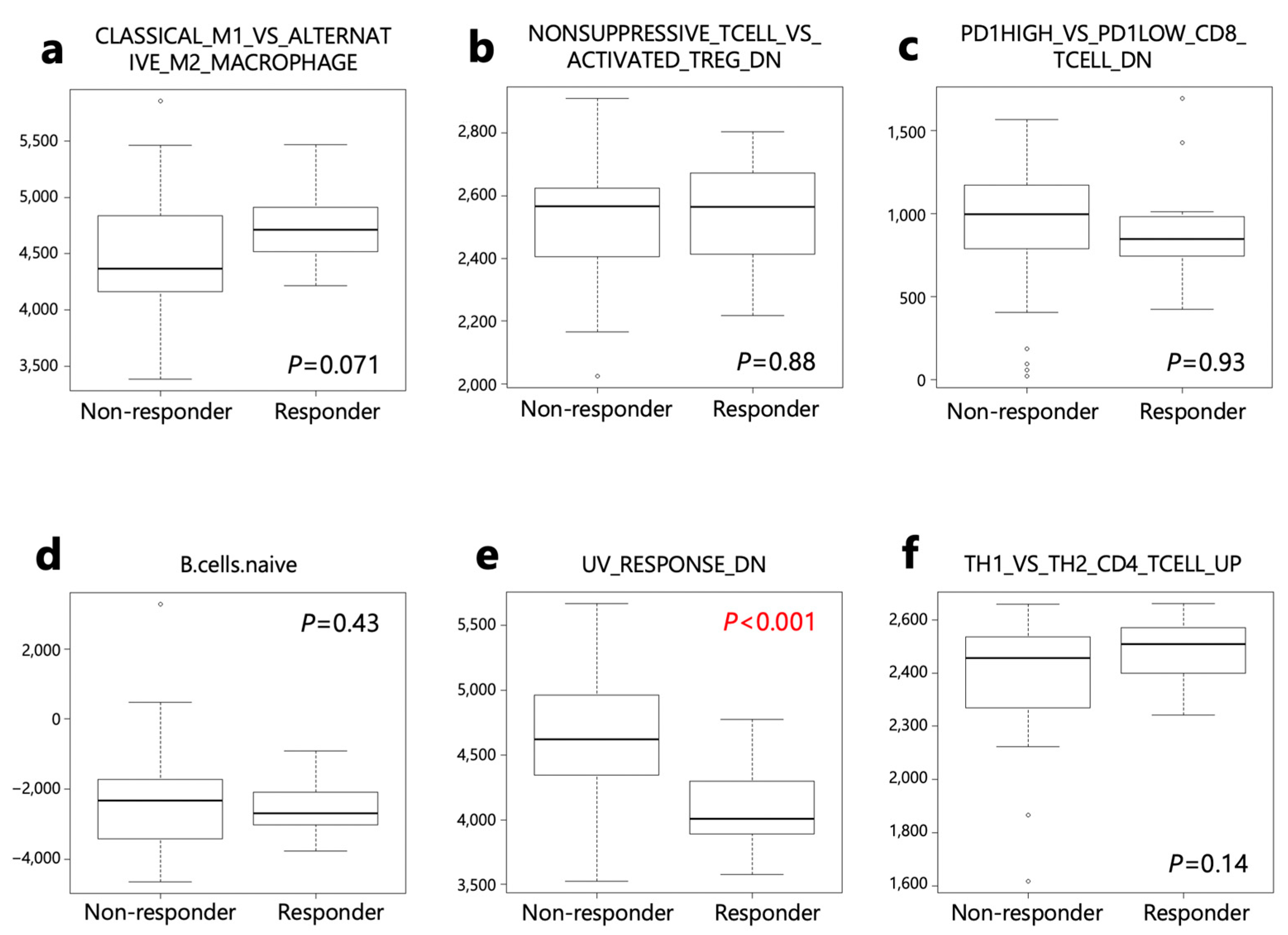
2.4. Biomarker for Anti-PD-1 Monotherapy
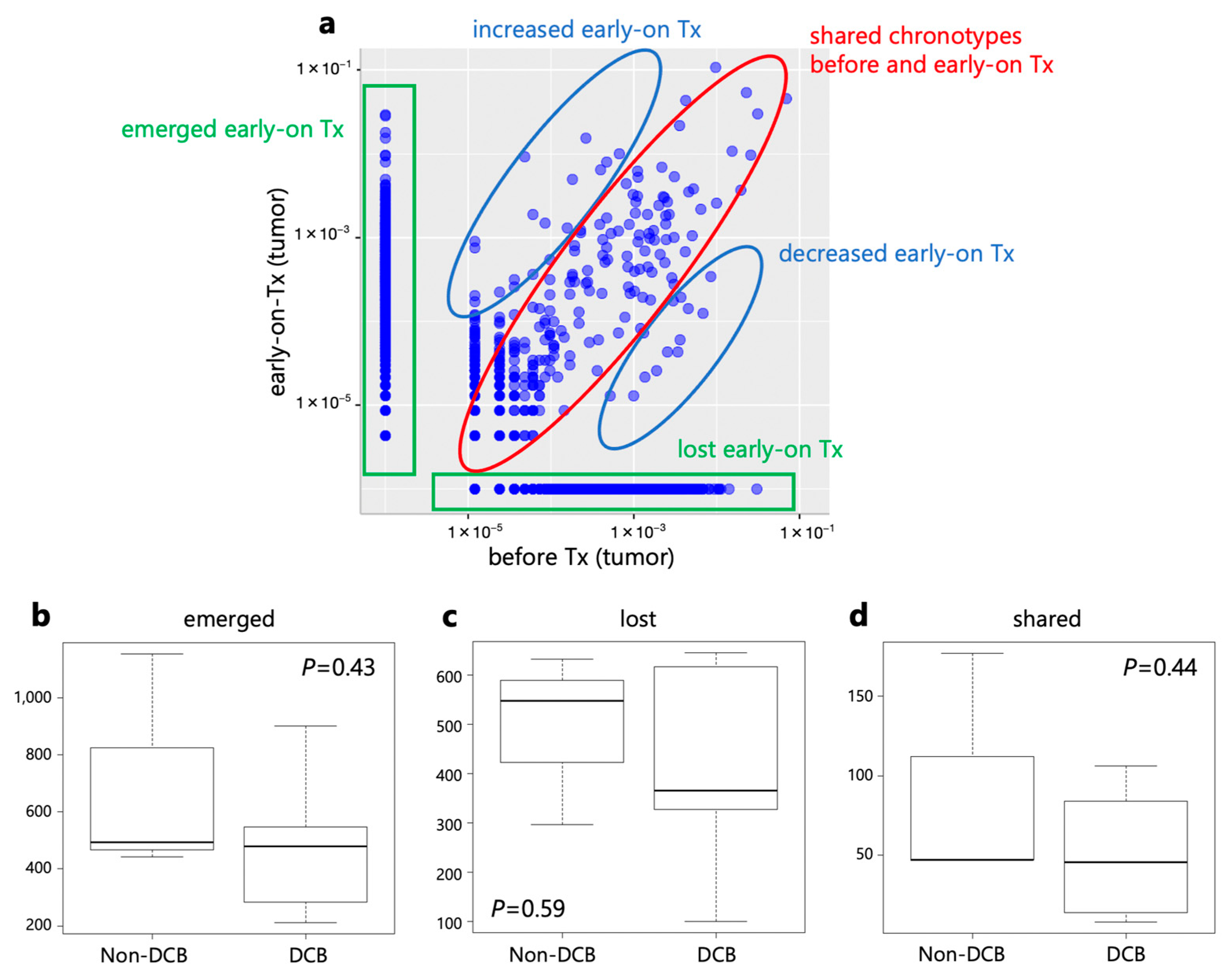
2.5. TCR Repertoire Analysis
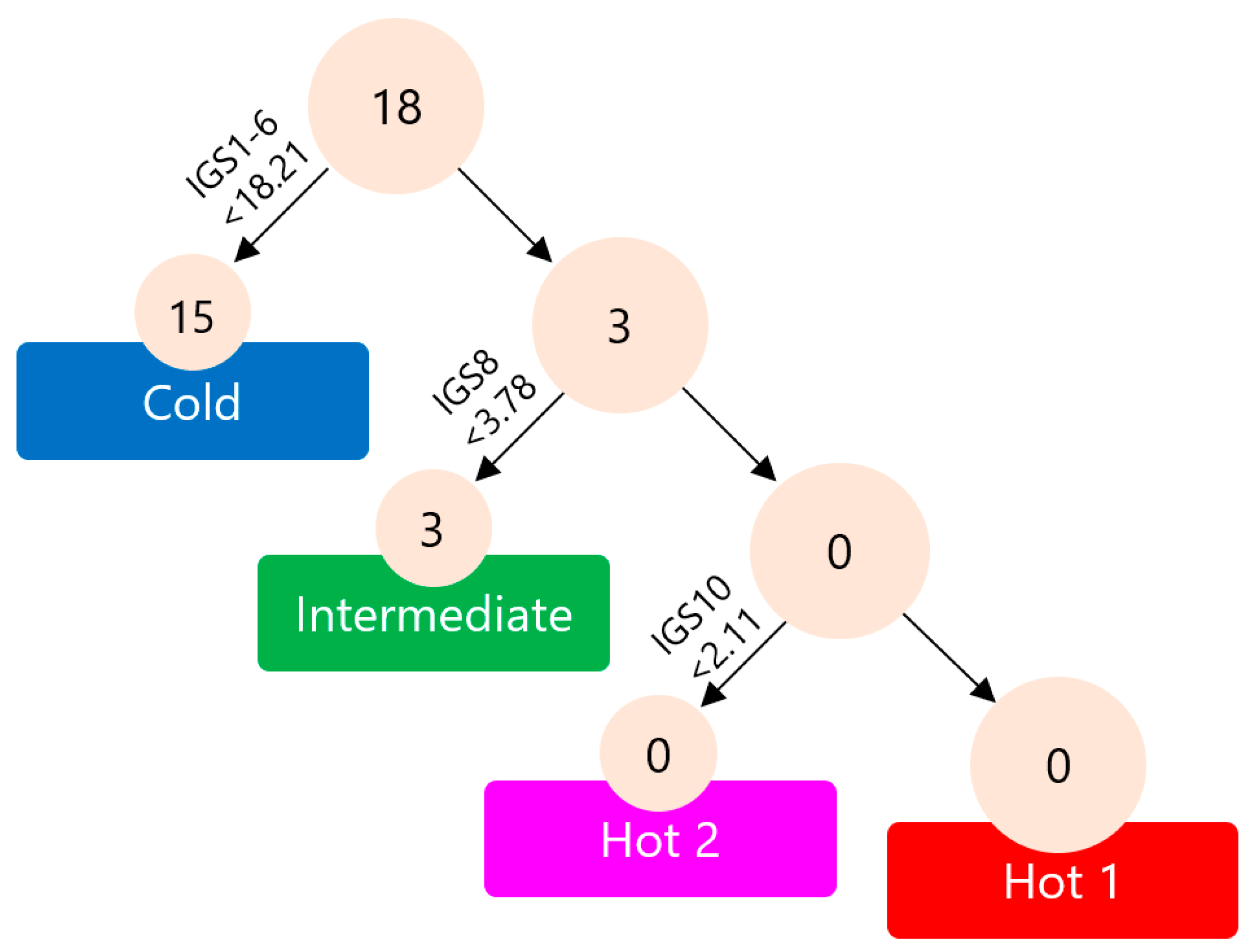
2.6. Immunological Classification of Gastric Cancer
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Clinical Sample Processing and RNA Extraction
4.3. RNA-Sequence (RNA-Seq)
4.4. Computational Methods to Analyze RNA-Seq Data
4.5. TCR Repertoire Analysis
4.6. Hierarchical Clustering
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Glossary
| DCB | Durable clinical benefit |
| TCR | T cell receptor |
| ORR | Objective response rate |
| PFS | Progression-free survival |
| OS | Overall survival |
| Treg | Regulatory T cell |
| ICI | Immune-checkpoint inhibitor |
| PD-L1 | Programmed cell death ligand 1 |
| PD-1 | Programmed death receptor 1 |
| HR | Hazard ratio |
| RNA-seq | RNA sequencing |
| TIL | Tumor-infiltrating T lymphocyte |
| DCBR | Durable clinical benefit rate |
| DCR | Disease control rate |
| HER2 | Human epidermal growth factor receptor 2 |
| ssGSEA | Single-sample gene-set enrichment analysis |
| TME | Tumor microenvironment |
| MSigDB | Molecular Signatures Database |
| UV | Ultraviolet |
| cDNA | Complementary DNA |
| CDR3 | Complementarity-determining region 3 |
| SWI | Shannon–Weaver index |
| ECOG | Eastern Cooperative Oncology Group |
| PS | Performance status |
| CAR-T | Chimeric antigen receptor T cell |
| CLDN | Claudin |
| Hb | Hemoglobin |
| PLT | Platelet count |
| T-Bil | Total bilirubin |
| AST | Aspartate aminotransferase |
| ALT | Alanine aminotransferase |
| Cre | Creatinine |
| NGS | Next-generation sequencing |
| FPKM | Fragments per kilobase of exon per million fragments mapped |
| TCGA | The Cancer Genome Atlas |
| M | Mean |
| SD | Standard deviation |
| CT | Computed tomography |
| CR | Complete response |
| PR | Partial response |
| SD | Stable disease |
| PD | Progressive disease |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cancer Information Service. Cancer Statistics in Japan 2021; Foundation for Promotion of Cancer Research: Tokyo, Japan, 2021.
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Chung, H.C.; Arkenau, H.T.; Lee, J.; Rha, S.Y.; Oh, D.Y.; Wyrwicz, L.; Kang, Y.K.; Lee, K.W.; Infante, J.R.; Lee, S.S.; et al. Avelumab (anti-PD-L1) as first-line switch-maintenance or second-line therapy in patients with advanced gastric or gastroesophageal junction cancer: Phase 1b results from the JAVELIN Solid Tumor trial. J. Immunother. Cancer 2019, 7, 30. [Google Scholar] [CrossRef]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2020, 24, 1–21. [CrossRef]
- Shitara, K.; Doi, T.; Dvorkin, M.; Mansoor, W.; Arkenau, H.T.; Prokharau, A.; Alsina, M.; Ghidini, M.; Faustino, C.; Gorbunova, V.; et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018, 19, 1437–1448. [Google Scholar] [CrossRef] [PubMed]
- Karasaki, T.; Nagayama, K.; Kuwano, H.; Nitadori, J.I.; Sato, M.; Anraku, M.; Hosoi, A.; Matsushita, H.; Morishita, Y.; Kashiwabara, K.; et al. An Immunogram for the Cancer-Immunity Cycle: Towards Personalized Immunotherapy of Lung Cancer. J. Thorac. Oncol. 2017, 12, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Kushihara, Y.; Saito, N.; Yamaguchi, S.; Kakimi, K. A novel scoring method based on RNA-Seq immunograms describing individual cancer-immunity interactions. Cancer Sci. 2020, 111, 4031–4040. [Google Scholar] [CrossRef]
- Sato, Y.; Wada, I.; Odaira, K.; Hosoi, A.; Kobayashi, Y.; Nagaoka, K.; Karasaki, T.; Matsushita, H.; Yagi, K.; Yamashita, H.; et al. Integrative immunogenomic analysis of gastric cancer dictates novel immunological classification and the functional status of tumor-infiltrating cells. Clin. Transl. Immunol. 2020, 9, e1194. [Google Scholar] [CrossRef]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Yost, K.E.; Satpathy, A.T.; Wells, D.K.; Qi, Y.; Wang, C.; Kageyama, R.; McNamara, K.L.; Granja, J.M.; Sarin, K.Y.; Brown, R.A.; et al. Clonal replacement of tumor-specific T cells following PD-1 blockade. Nat. Med. 2019, 25, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.D.; Madireddi, S.; de Almeida, P.E.; Banchereau, R.; Chen, Y.J.J.; Chitre, A.S.; Chiang, E.Y.; Iftikhar, H.; O’Gorman, W.E.; Au-Yeung, A.; et al. Peripheral T cell expansion predicts tumour infiltration and clinical response. Nature 2020, 579, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Luoma, A.M.; Suo, S.; Wang, Y.; Gunasti, L.; Porter, C.B.M.; Nabilsi, N.; Tadros, J.; Ferretti, A.P.; Liao, S.; Gurer, C.; et al. Tissue-resident memory and circulating T cells are early responders to pre-surgical cancer immunotherapy. Cell 2022, 185, 2918–2935.e29. [Google Scholar] [CrossRef] [PubMed]
- Nagasaki, J.; Inozume, T.; Sax, N.; Ariyasu, R.; Ishikawa, M.; Yamashita, K.; Kawazu, M.; Ueno, T.; Irie, T.; Tanji, E.; et al. PD-1 blockade therapy promotes infiltration of tumor-attacking exhausted T cell clonotypes. Cell Rep. 2022, 38, 110331. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Togashi, Y.; Tay, C.; Ha, D.; Sasaki, A.; Nakamura, Y.; Sato, E.; Fukuoka, S.; Tada, Y.; Tanaka, A.; et al. PD-1 + regulatory T cells amplified by PD-1 blockade promote hyperprogression of cancer. Proc. Natl. Acad. Sci. USA 2019, 116, 201822001. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Togashi, Y.; Kamada, T.; Sugiyama, E.; Nishinakamura, H.; Takeuchi, Y.; Vitaly, K.; Itahashi, K.; Maeda, Y.; Matsui, S.; et al. The PD-1 expression balance between effector and regulatory T cells predicts the clinical efficacy of PD-1 blockade therapies. Nat. Immunol. 2020, 21, 1346–1358. [Google Scholar] [CrossRef]
- Serratì, S.; Guida, M.; Di Fonte, R.; De Summa, S.; Strippoli, S.; Iacobazzi, R.M.; Quarta, A.; De Risi, I.; Guida, G.; Paradiso, A.; et al. Circulating extracellular vesicles expressing PD1 and PD-L1 predict response and mediate resistance to checkpoint inhibitors immunotherapy in metastatic melanoma. Mol. Cancer 2022, 21, 20. [Google Scholar] [CrossRef]
- Ohkuma, R.; Ieguchi, K.; Watanabe, M.; Takayanagi, D.; Goshima, T.; Onoue, R.; Hamada, K.; Kubota, Y.; Horiike, A.; Ishiguro, T.; et al. Increased plasma soluble pd-1 concentration correlates with disease progression in patients with cancer treated with anti-pd-1 antibodies. Biomedicines 2021, 9, 1929. [Google Scholar] [CrossRef]
- Sagawa, R.; Sakata, S.; Gong, B.; Seto, Y.; Takemoto, A.; Takagi, S.; Ninomiya, H.; Yanagitani, N.; Nakao, M.; Mun, M.; et al. Soluble PD-L1 works as a decoy in lung cancer immunotherapy via alternative polyadenylation. JCI Insight. 2022, 7, e153323. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Campos Bragagnoli, A.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Kang, Y.K.; Chen, L.T.; Ryu, M.H.; Oh, D.Y.; Oh, S.C.; Chung, H.C.; Lee, K.W.; Omori, T.; Shitara, K.; Sakuramoto, S.; et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): A randomised, multicentre, double-blind, placebo-contr. Lancet Oncol. 2022, 23, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; Gong, J.; Li, J.; Liu, D.; Qin, Y.; Ge, S.; Zhang, M.; Peng, Z.; Zhou, J.; Cao, Y.; et al. Claudin18.2-specific CAR T cells in gastrointestinal cancers: Phase 1 trial interim results. Nat. Med. 2022, 28, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Kitaura, K.; Shini, T.; Matsutani, T.; Suzuki, R. A new high-throughput sequencing method for determining diversity and similarity of T cell receptor (TCR) α and β repertoires and identifying potential new invariant TCR α chains. BMC Immunol. 2016, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Kodama, Y.; Mashima, J.; Kosuge, T.; Katayama, T.; Fujisawa, T.; Kaminuma, E.; Ogasawara, O.; Okubo, K.; Takagi, T.; Nakamura, Y. The DDBJ Japanese genotype-phenotype archive for genetic and phenotypic human data. Nucleic Acids Res. 2015, 43, D18–D22. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 19) | Immunological-Analysis Cases (n = 18) |
|---|---|---|
| Sex, n (%) | ||
| Male | 10 (53) | 9 (50) |
| Age, years | ||
| Median (range) | 67 (49–87) | 66 (49–87) |
| ECOG PS, n (%) | ||
| 0 | 4 (21) | 4 (22) |
| 1 | 8 (42) | 8 (44) |
| 2 | 7 (37) | 6 (33) |
| Histology, n (%) | ||
| Intestinal | 5 (26) | 4 (22) |
| Diffuse | 10 (53) | 10 (56) |
| Mixed | 2 (11) | 2 (11) |
| Special type | 0 (0) | 0 (0) |
| Unknown | 2 (11) | 2 (11) |
| HER2, n (%) | ||
| Positive | 2 (11) | 2 (11) |
| Negative | 13 (68) | 12 (67) |
| Unknown | 4 (21) | 4 (22) |
| Number of previous chemotherapies, n (%) | ||
| 0 | 0 (0) | 0 (0) |
| 1 | 0 (0) | 0 (0) |
| 2 | 14 (74) | 13 (72) |
| 3 | 3 (16) | 3 (17) |
| ≥4 | 2 (11) | 2 (11) |
| All (n = 19) | Immunological-Analysis Cases (n = 18) | |
|---|---|---|
| Primary endpoint | ||
| DCB, n (% (95% CI)) | 3 (15.8 (3.4–39.6)) | 3 (16.7) |
| Co-primary endpoints | ||
| Objective response, n (%) | 3 (15.8) | 3 (16.7) |
| Disease control, n (%) | 4 (21.0) | 4 (22.2) |
| PFS | ||
| Median (95% CI), months | 2.3 (1.3–2.8) | 2.4 (1.4–2.8) |
| 1-year rate (% (95% CI)) | 5.3 (0.4–21.4) | 5.6 (0.4–22.4) |
| OS | ||
| Median (95% CI), months | 5.5 (1.6–7.6) | 5.5 (2.5–8.7) |
| 1-year rate (95% CI), % | 17.1 (4.3–37.3) | 18.1% (4.5–39.0) |
| Pre-Treatment | Early-On Treatment | p Value | ||
|---|---|---|---|---|
| DCB | OG002 | 5.752 | 5.329 | |
| OG010 | 5.630 | 5.320 | ||
| OG017 | 3.908 | 3.674 | ||
| Average ± SD | 5.097 ± 1.032 | 4.774 ± 0.953 | 0.028 | |
| Non-DCB | OG003 | 5.143 | 5.482 | |
| OG007 | 4.181 | 5.564 | ||
| OG008 | 3.034 | 4.562 | ||
| OG009 | 3.702 | 3.320 | ||
| OG011 | 5.055 | 6.008 | ||
| OG014 | 4.899 | 5.618 | ||
| OG015 | 6.060 | 5.371 | ||
| OG016 | 4.314 | 4.216 | ||
| OG018 | 3.844 | 4.005 | ||
| OG019 | 4.451 | 4.577 | ||
| Average ± SD | 4.468 ± 0.860 | 4.872 ± 0.864 | 0.115 | |
| All | Average ± SD | 4.613 ± 0.899 | 4.850 ± 0.845 | 0.254 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, Y.; Yamashita, H.; Kobayashi, Y.; Nagaoka, K.; Hisayoshi, T.; Kawahara, T.; Kuroda, A.; Saito, N.; Iwata, R.; Okumura, Y.; et al. Alterations in Intratumoral Immune Response before and during Early-On Nivolumab Treatment for Unresectable Advanced or Recurrent Gastric Cancer. Int. J. Mol. Sci. 2023, 24, 16602. https://doi.org/10.3390/ijms242316602
Sato Y, Yamashita H, Kobayashi Y, Nagaoka K, Hisayoshi T, Kawahara T, Kuroda A, Saito N, Iwata R, Okumura Y, et al. Alterations in Intratumoral Immune Response before and during Early-On Nivolumab Treatment for Unresectable Advanced or Recurrent Gastric Cancer. International Journal of Molecular Sciences. 2023; 24(23):16602. https://doi.org/10.3390/ijms242316602
Chicago/Turabian StyleSato, Yasuyoshi, Hiroharu Yamashita, Yukari Kobayashi, Koji Nagaoka, Tetsuro Hisayoshi, Takuya Kawahara, Akihiro Kuroda, Noriyuki Saito, Ryohei Iwata, Yasuhiro Okumura, and et al. 2023. "Alterations in Intratumoral Immune Response before and during Early-On Nivolumab Treatment for Unresectable Advanced or Recurrent Gastric Cancer" International Journal of Molecular Sciences 24, no. 23: 16602. https://doi.org/10.3390/ijms242316602
APA StyleSato, Y., Yamashita, H., Kobayashi, Y., Nagaoka, K., Hisayoshi, T., Kawahara, T., Kuroda, A., Saito, N., Iwata, R., Okumura, Y., Yagi, K., Aiko, S., Nomura, S., Kakimi, K., & Seto, Y. (2023). Alterations in Intratumoral Immune Response before and during Early-On Nivolumab Treatment for Unresectable Advanced or Recurrent Gastric Cancer. International Journal of Molecular Sciences, 24(23), 16602. https://doi.org/10.3390/ijms242316602