
Late-Onset Pompe Disease with Normal Creatine Kinase Levels: The Importance of Rheumatological Suspicion

 ,
,
Abstract
:1. Introduction
2. Case Presentation
2.1. Patients
2.2. Sample Collection
2.3. Enzymatic Assay
2.4. DNA Extraction
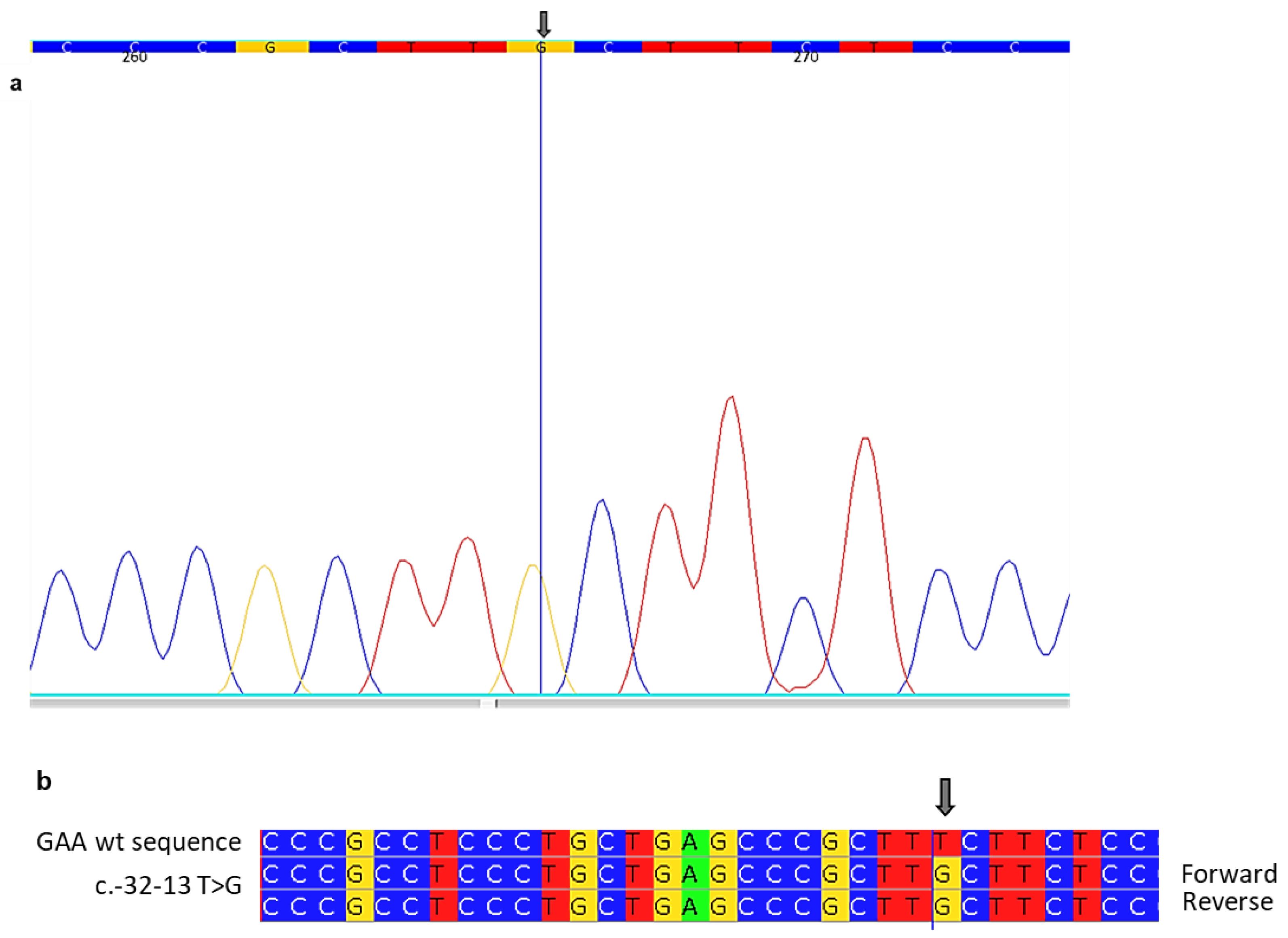
2.5. Genetic Analysis-PCR and Sanger Sequencing
2.6. Clinical and Laboratory Findings
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kohler, L.; Puertollano, R.; Raben, N. Pompe Disease: From Basic Science to Therapy. Neurotherapeutics 2018, 15, 928–942. [Google Scholar] [CrossRef] [PubMed]
- Dasouki, M.; Jawdat, O.; Almadhoun, O.; Pasnoor, M.; McVey, A.L.; Abuzinadah, A.; Herbelin, L.; Barohn, R.J.; Dimachkie, M.M. Pompe disease: Literature review and case series. Neurol. Clin. 2014, 32, 751–776. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S. Carrier frequency and predicted genetic prevalence of Pompe disease based on a general population database. Mol. Genet. Metab. Rep. 2021, 27, 100734. [Google Scholar] [CrossRef] [PubMed]
- Taverna, S.; Cammarata, G.; Colomba, P.; Sciarrino, S.; Zizzo, C.; Francofonte, D.; Zora, M.; Scalia, S.; Brando, C.; Curto, A.L.; et al. Pompe disease: Pathogenesis, molecular genetics and diagnosis. Aging 2020, 12, 15856–15874. [Google Scholar] [CrossRef] [PubMed]
- Dons-Sinke, I.J.; Dirckx, M.; Scoones, G.P. Anaesthetic management of two patients with pompe disease for caesarean section. Case Rep. Anesthesiol. 2014, 2014, 650310. [Google Scholar] [CrossRef]
- Wencel, M.; Shaibani, A.; Goyal, N.A.; Dimachkie, M.M.; Trivedi, J.; Johnson, N.E.; Gutmann, L.; Wicklund, M.P.; Bandyopadhay, S.; Genge, A.L.; et al. Investigating Late-Onset Pompe Prevalence in Neuromuscular Medicine Academic Practices: The IPaNeMA Study. Neurol. Genet. 2021, 7, e623. [Google Scholar] [CrossRef]
- Meena, N.K.; Raben, N. Pompe Disease: New Developments in an Old Lysosomal Storage Disorder. Biomolecules 2020, 10, 1339. [Google Scholar] [CrossRef]
- Goina, E.; Peruzzo, P.; Bembi, B.; Dardis, A.; Buratti, E. Glycogen Reduction in Myotubes of Late-Onset Pompe Disease Patients Using Antisense Technology. Mol. Ther. 2017, 25, 2117–2128. [Google Scholar] [CrossRef]
- Chien, Y.H.; Hwu, W.L.; Lee, N.C. Pompe disease: Early diagnosis and early treatment make a difference. Pediatr. Neonatol. 2013, 54, 219–227. [Google Scholar] [CrossRef]
- Tang, H.; Feuchtbaum, L.; Sciortino, S.; Matteson, J.; Mathur, D.; Bishop, T.; Olney, R.S. The First Year Experience of Newborn Screening for Pompe Disease in California. Int. J. Neonatal Screen. 2020, 6, 9. [Google Scholar] [CrossRef]
- Sawada, T.; Kido, J.; Nakamura, K. Newborn Screening for Pompe Disease. Int. J. Neonatal Screen. 2020, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Toscano, A.; Rodolico, C.; Musumeci, O. Multisystem late onset Pompe disease (LOPD): An update on clinical aspects. Ann. Transl. Med. 2019, 7, 284. [Google Scholar] [CrossRef] [PubMed]
- Parisi, D.; Musumeci, O.; Mondello, S.; Brizzi, T.; Oteri, R.; Migliorato, A.; Ciranni, A.; Mongini, T.E.; Rodolico, C.; Vita, G.; et al. Vacuolated PAS-Positive Lymphocytes on Blood Smear: An Easy Screening Tool and a Possible Biomarker for Monitoring Therapeutic Responses in Late Onset Pompe Disease (LOPD). Front. Neurol. 2018, 9, 880. [Google Scholar] [CrossRef] [PubMed]
- Niño, M.Y.; Wijgerde, M.; de Faria, D.O.S.; Hoogeveen-Westerveld, M.; Bergsma, A.J.; Broeders, M.; van der Beek, N.A.M.E.; Hout, H.J.M.v.D.; van der Ploeg, A.T.; Verheijen, F.W.; et al. Enzymatic diagnosis of Pompe disease: Lessons from 28 years of experience. Eur. J. Hum. Genet. 2021, 29, 434–446. [Google Scholar] [CrossRef]
- Er, T.K.; Chen, C.C.; Chien, Y.H.; Liang, W.C.; Kan, T.M.; Jong, Y.J. Development of a feasible assay for the detection of GAA mutations in patients with Pompe disease. Clin. Chim. Acta 2014, 429, 18–25. [Google Scholar] [CrossRef]
- Kroos, M.A.; Mullaart, R.A.; Van Vliet, L.; Pomponio, R.J.; Amartino, H.; Kolodny, E.H.; Pastores, G.M.; Wevers, R.A.; Van der Ploeg, A.T.; Halley, D.J.J.; et al. p.[G576S; E689K]: Pathogenic combination or polymorphism in Pompe disease? Eur. J. Hum. Genet. 2008, 16, 875–879. [Google Scholar] [CrossRef]
- Niño, M.Y.; In ‘t Groen, S.L.M.; Bergsma, A.J.; van der Beek, N.A.; Kroos, M.; Hoogeveen-Westerveld, M.; Van Der Ploeg, A.T.; Pijnappel, W.P. Extension of the Pompe mutation database by linking disease-associated variants to clinical severity. Hum. Mutat. 2019, 40, 1954–1967. [Google Scholar] [CrossRef]
- Dardis, A.; Zanin, I.; Zampieri, S.; Stuani, C.; Pianta, A.; Romanello, M.; Baralle, F.E.; Bembi, B.; Buratti, E. Functional characterization of the common c.-32-13T>G mutation of GAA gene: Identification of potential therapeutic agents. Nucleic Acids Res. 2014, 42, 1291–1302. [Google Scholar] [CrossRef]
- Li, Y.; Scott, C.R.; Chamoles, N.A.; Ghavami, A.; Pinto, B.M.; Turecek, F.; Gelb, M.H. Direct multiplex assay of lysosomal enzymes in dried blood spots for newborn screening. Clin. Chem. 2004, 50, 1785–1796. [Google Scholar] [CrossRef]
- Chamoles, N.A.; Niizawa, G.; Blanco, M.; Gaggioli, D.; Casentini, C. Glycogen storage disease type II: Enzymatic screening in dried blood spots on filter paper. Clin. Chim. Acta 2004, 347, 97–102. [Google Scholar] [CrossRef]
- Spada, M.; Porta, F.; Vercelli, L.; Pagliardini, V.; Chiadò-Piat, L.; Boffi, P.; Pagliardini, S.; Remiche, G.; Ronchi, D.; Comi, G.; et al. Screening for later-onset Pompe’s disease in patients with paucisymptomatic hyperCKemia. Mol. Genet. Metab. 2013, 109, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, O.; Thieme, A.; Claeys, K.G.; Wenninger, S.; Kley, R.A.; Kuhn, M.; Lukacs, Z.; Deschauer, M.; Gaeta, M.; Toscano, A.; et al. Homozygosity for the common GAA gene splice site mutation c.-32-13T>G in Pompe disease is associated with the classical adult phenotypical spectrum. Neuromuscul. Disord. 2015, 25, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Lee, C.C.; Hsu, C.M.; Hwu, W.L.; Yang, C.C.; Tsai, C.H.; Tsai, F.J. Identification of eight novel mutations of the acid alpha-glucosidase gene causing the infantile or juvenile form of glycogen storage disease type II. J. Neurol. 2008, 255, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.L.; Bembi, B.; Donnarumma, M.; Filocamo, M.; Parenti, G.; Rossi, M.; Merlini, L.; Buratti, E.; De Filippi, P.; Dardis, A.; et al. Mutation profile of the GAA gene in 40 Italian patients with late onset glycogen storage disease type II. Hum. Mutat. 2006, 27, 999–1006. [Google Scholar] [CrossRef]
- Singh, R.K.; Cooper, T.A. Pre-mRNA splicing in disease and therapeutics. Trends Mol. Med. 2012, 18, 472–482. [Google Scholar] [CrossRef]
- Ren, P.; Lu, L.; Cai, S.; Chen, J.; Lin, W.; Han, F. Alternative Splicing: A New Cause and Potential Therapeutic Target in Autoimmune Disease. Front. Immunol. 2021, 12, 713540. [Google Scholar] [CrossRef]
- Kroos, M.A.; Pomponio, R.J.; Hagemans, M.L.; Keulemans, J.; Phipps, M.; DeRiso, M.; Palmer, R.E.; Ausems, M.G.; Van der Beek, N.A.; Van Diggelen, O.P.; et al. Broad spectrum of Pompe disease in patients with the same c.-32-13T->G haplotype. Neurology 2007, 68, 110–115. [Google Scholar] [CrossRef]
- Laforêt, P.; Nicolino, M.; Eymard, P.B.; Puech, J.P.; Caillaud, C.; Poenaru, L.; Fardeau, M. Juvenile and adult-onset acid maltase deficiency in France: Genotype-phenotype correlation. Neurology 2000, 55, 1122–1128. [Google Scholar] [CrossRef]
- Rairikar, M.V.; Case, L.E.; Bailey, L.A.; Kazi, Z.B.; Desai, A.K.; Berrier, K.L.; Coats, J.; Gandy, R.; Quinones, R.; Kishnani, P.S. Insight into the phenotype of infants with Pompe disease identified by newborn screening with the common c.-32-13T>G “late-onset” GAA variant. Mol. Genet. Metab. 2017, 122, 99–107. [Google Scholar] [CrossRef]
- Nardin, R.A.; Zarrin, A.R.; Horowitz, G.L.; Tarulli, A.W. Effect of newly proposed CK reference limits on neuromuscular diagnosis. Muscle Nerve 2009, 39, 494–497. [Google Scholar] [CrossRef]

{kind=link}
| Types of Pompe Disease | Classic Infantile Form | Non-Classic Infantile Form | Adult Onset |
|---|---|---|---|
| Onset | Shortly after birth (usually within the first 3 months) | Delayed onset (within the child’s first year of life) | Any age |
| Symptoms | Generalized muscle weakness (facial muscles, diaphragm, intercostal muscles) Feeding and hearing disturbances Symptoms of malnutrition ‘Failure to thrive’ Poor weight gain Breathing problems Lung infections Floppiness Head lag Hypertrophic cardiomyopathy that results in heart failure Enlarged liver and tongue | Less severe forms Usually slower progression. Progressive muscle weakness and the delayed development of motor Skills such as rolling over and sitting. Severe respiratory problems due to damage and weakness in the muscles involved in breathing. Abnormally enlarged heart with a lower chance of heart failure compared to the classical form | Milder clinical manifestations and course Respiratory complications due to the weakness of the diaphragm and intercostal muscles Frequent lung infections Most common cause of death is lung failure Myopathy Mobility problems Morning headaches tiredness Weight loss Scoliosis Reduced heart involvement compared to the other form |
| Allele ID | Variant Type | Variant Length | Cytogenetic Location | Genomic Location |
|---|---|---|---|---|
| 1013211 | single nucleotide variant | 1 bp | 17q25.3 | 17: 80104542 (GRCh38) |
| Patient No | Sex | Age | Kinship | Mutation | GAA Activity (nmol/mL/h) Normal Range: >6.0 |
|---|---|---|---|---|---|
| 1 | M | 58 | Index Case | c.-32-13T>G homozygous | 0.8 |
| 2 | M | 59 | Brother of Index Case | c.-32-13T>G homozygous | 0.7 |
| 3 | M | 52 | Brother of Index Case | c.-32-13T>G homozygous | 1.6 |
| 4 | F | 81 | Mother of Index Case | c.-32-13T>G heterozygous | 6.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marotto, D.; Moschetti, M.; Lo Curto, A.; Spezzigu, A.M.; Giacomarra, M.; Marsana, E.M.; Zizzo, C.; Duro, G.; Colomba, P. Late-Onset Pompe Disease with Normal Creatine Kinase Levels: The Importance of Rheumatological Suspicion. Int. J. Mol. Sci. 2023, 24, 15924. https://doi.org/10.3390/ijms242115924
Marotto D, Moschetti M, Lo Curto A, Spezzigu AM, Giacomarra M, Marsana EM, Zizzo C, Duro G, Colomba P. Late-Onset Pompe Disease with Normal Creatine Kinase Levels: The Importance of Rheumatological Suspicion. International Journal of Molecular Sciences. 2023; 24(21):15924. https://doi.org/10.3390/ijms242115924
Chicago/Turabian StyleMarotto, Daniela, Marta Moschetti, Alessia Lo Curto, Anna M. Spezzigu, Miriam Giacomarra, Emanuela M. Marsana, Carmela Zizzo, Giovanni Duro, and Paolo Colomba. 2023. "Late-Onset Pompe Disease with Normal Creatine Kinase Levels: The Importance of Rheumatological Suspicion" International Journal of Molecular Sciences 24, no. 21: 15924. https://doi.org/10.3390/ijms242115924
APA StyleMarotto, D., Moschetti, M., Lo Curto, A., Spezzigu, A. M., Giacomarra, M., Marsana, E. M., Zizzo, C., Duro, G., & Colomba, P. (2023). Late-Onset Pompe Disease with Normal Creatine Kinase Levels: The Importance of Rheumatological Suspicion. International Journal of Molecular Sciences, 24(21), 15924. https://doi.org/10.3390/ijms242115924