
Antiepileptogenic Effects of Anakinra, Lamotrigine and Their Combination in a Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Rats


 and
and
Abstract
:1. Introduction
2. Results
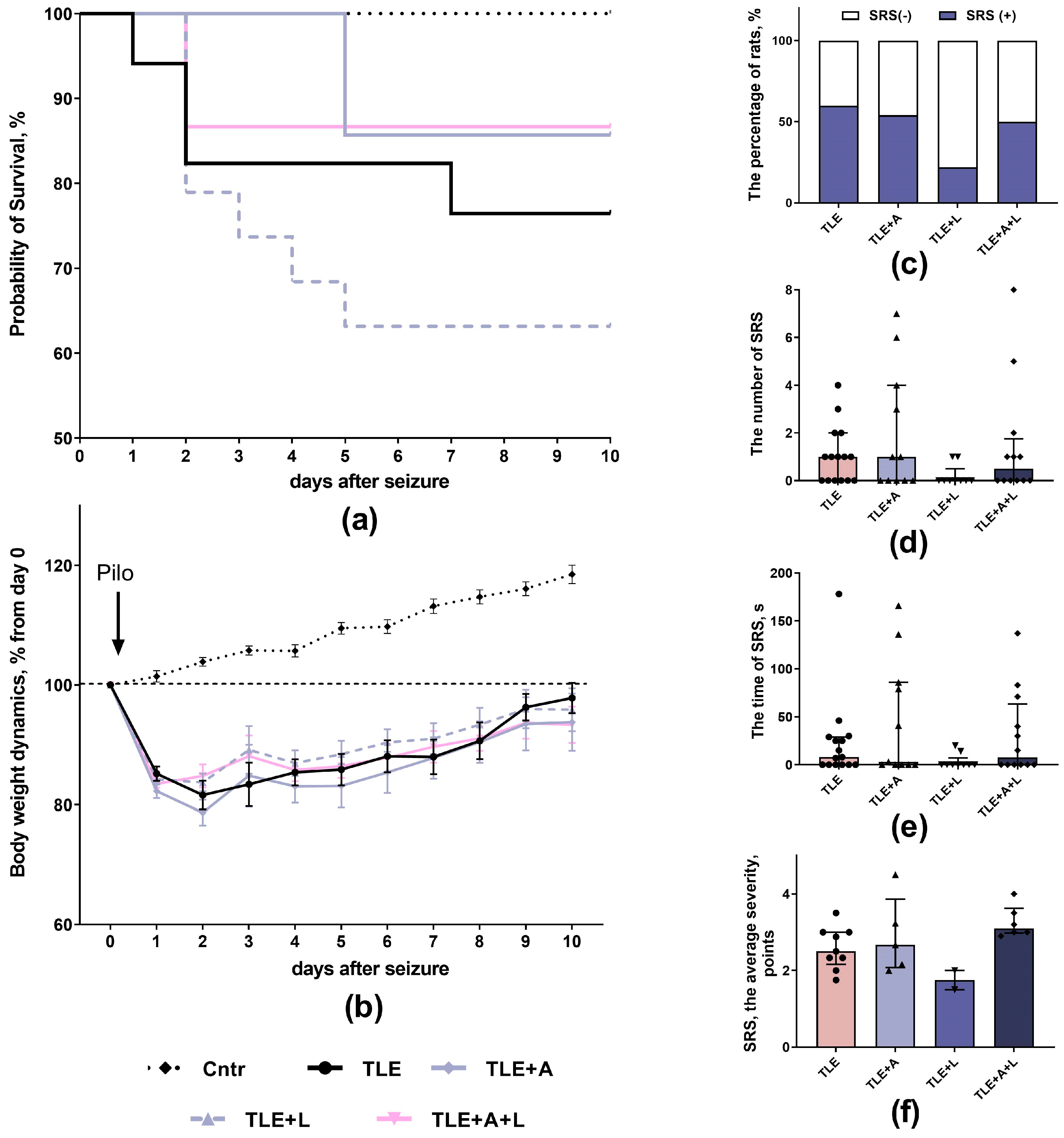
2.1. The Effect of Treatment with Anakinra, Lamotrigine, and Their Combination Effect on Neurological Parameters
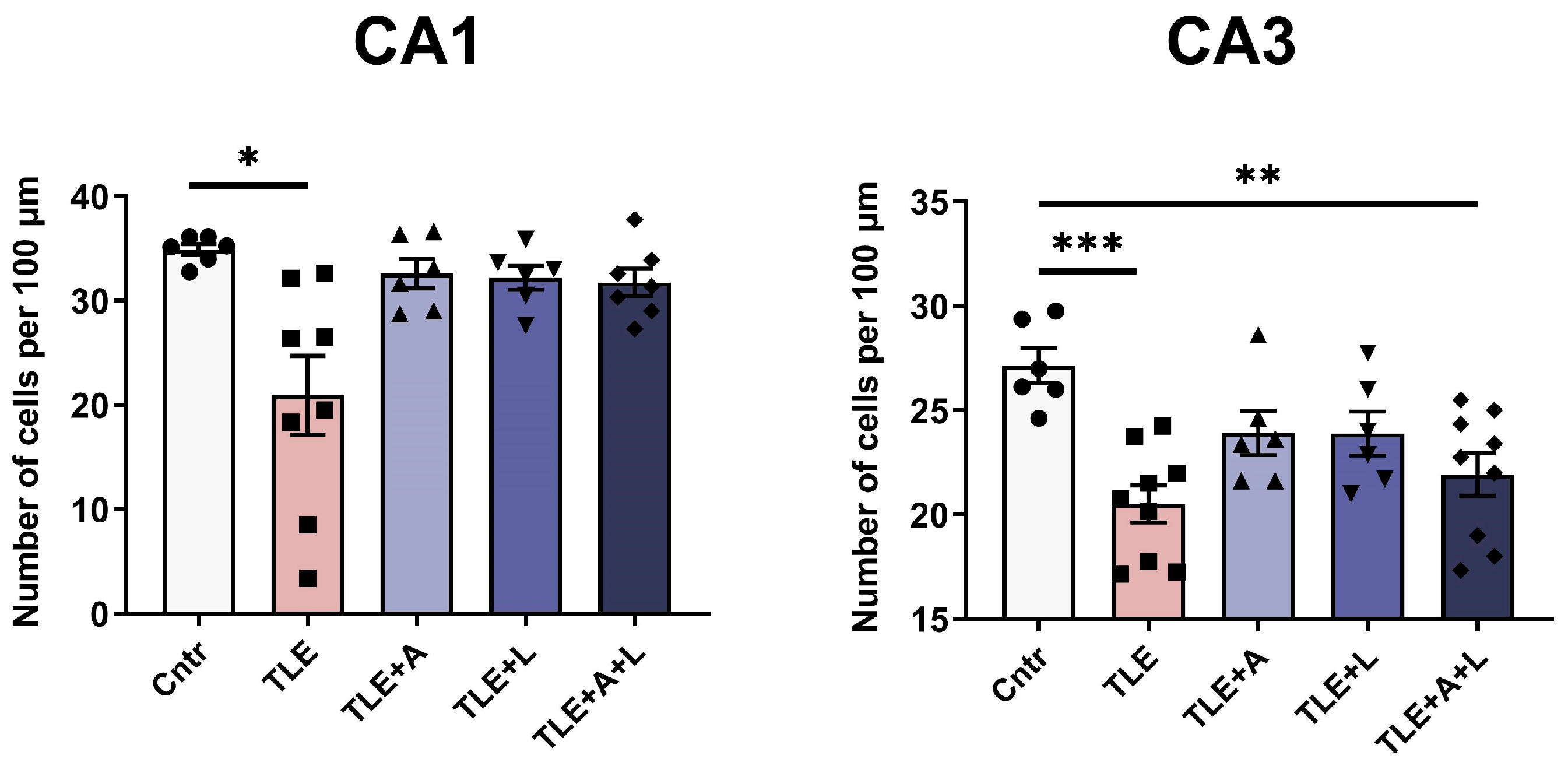
2.2. Anakinra, Lamotrigine, or Their Combination Can Prevent Neuronal Death in the Hippocampus following Pilocarpine-Induced Status Epilepticus
2.3. Behavioral Disturbances May Be Improved with Anakinra, Lamotrigine, or Their Combination
2.3.1. Treatment Effects on Activity Levels, Exploratory Behavior, and Anxiety in Experimental and Control Animals in the Open Field Test
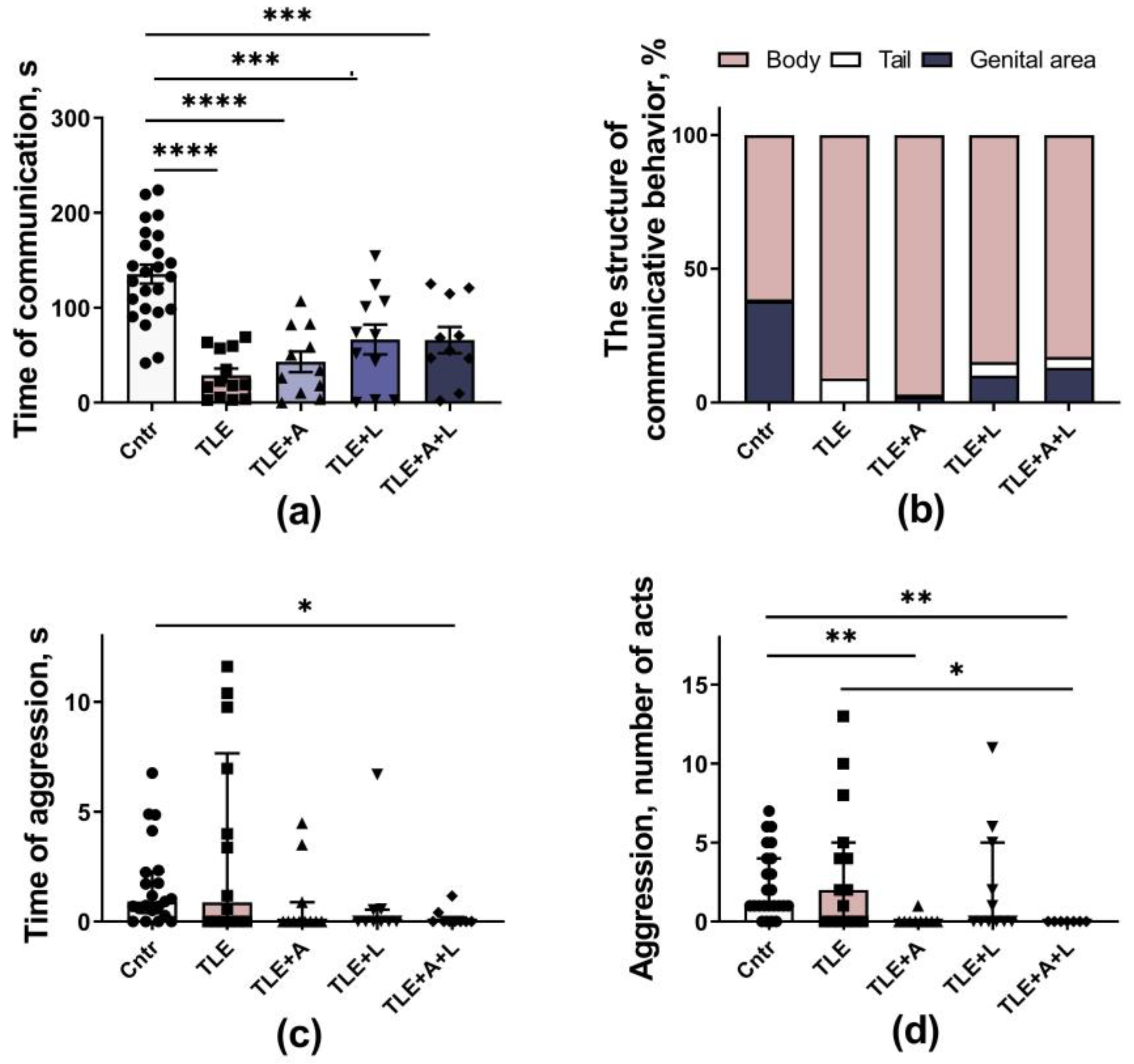
2.3.2. Social Behavior
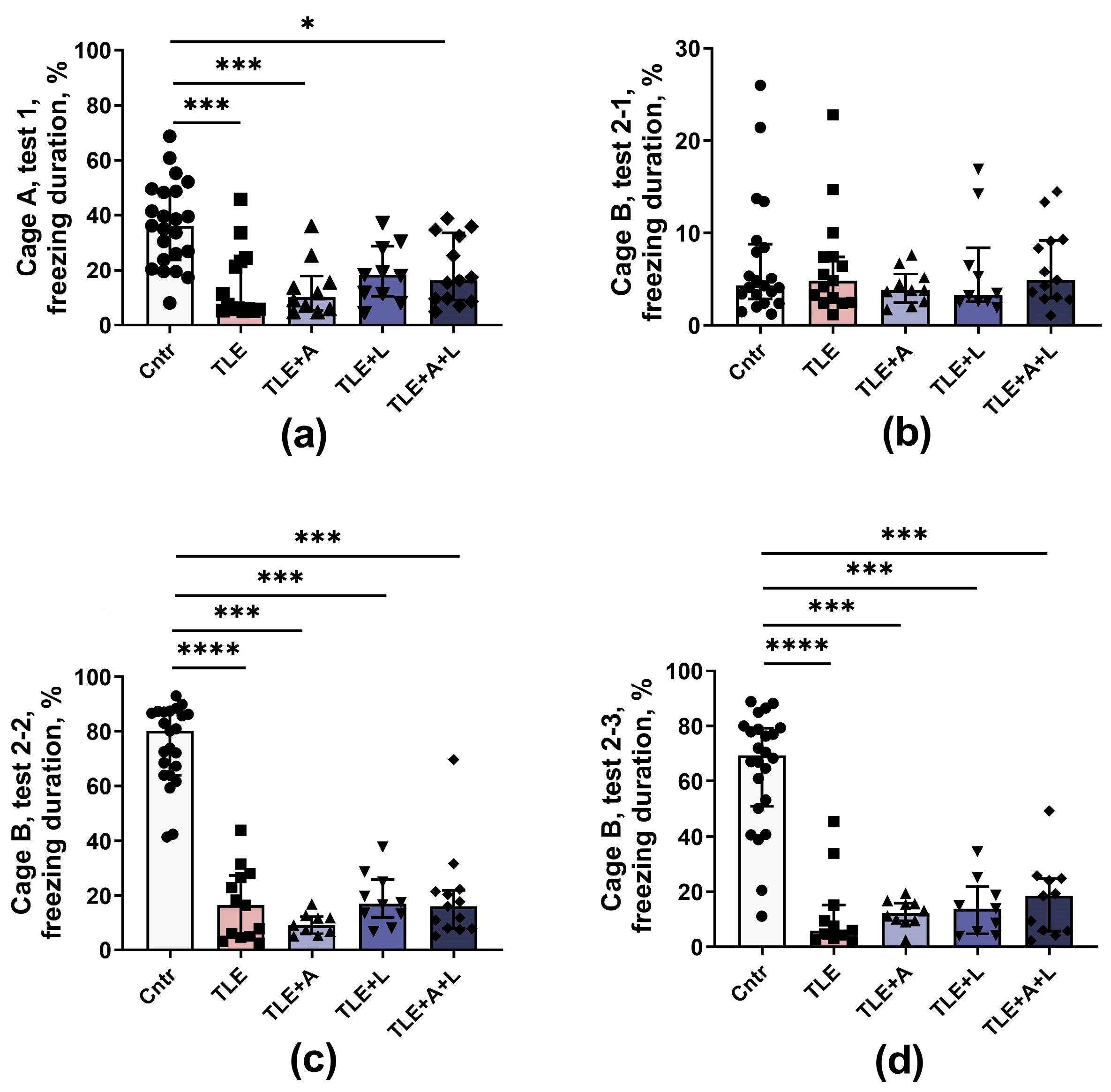
2.3.3. The Memory Impairments
Fear Conditioning Test
Morris Water Maze
3. Discussion
4. Materials and Methods
4.1. Animals
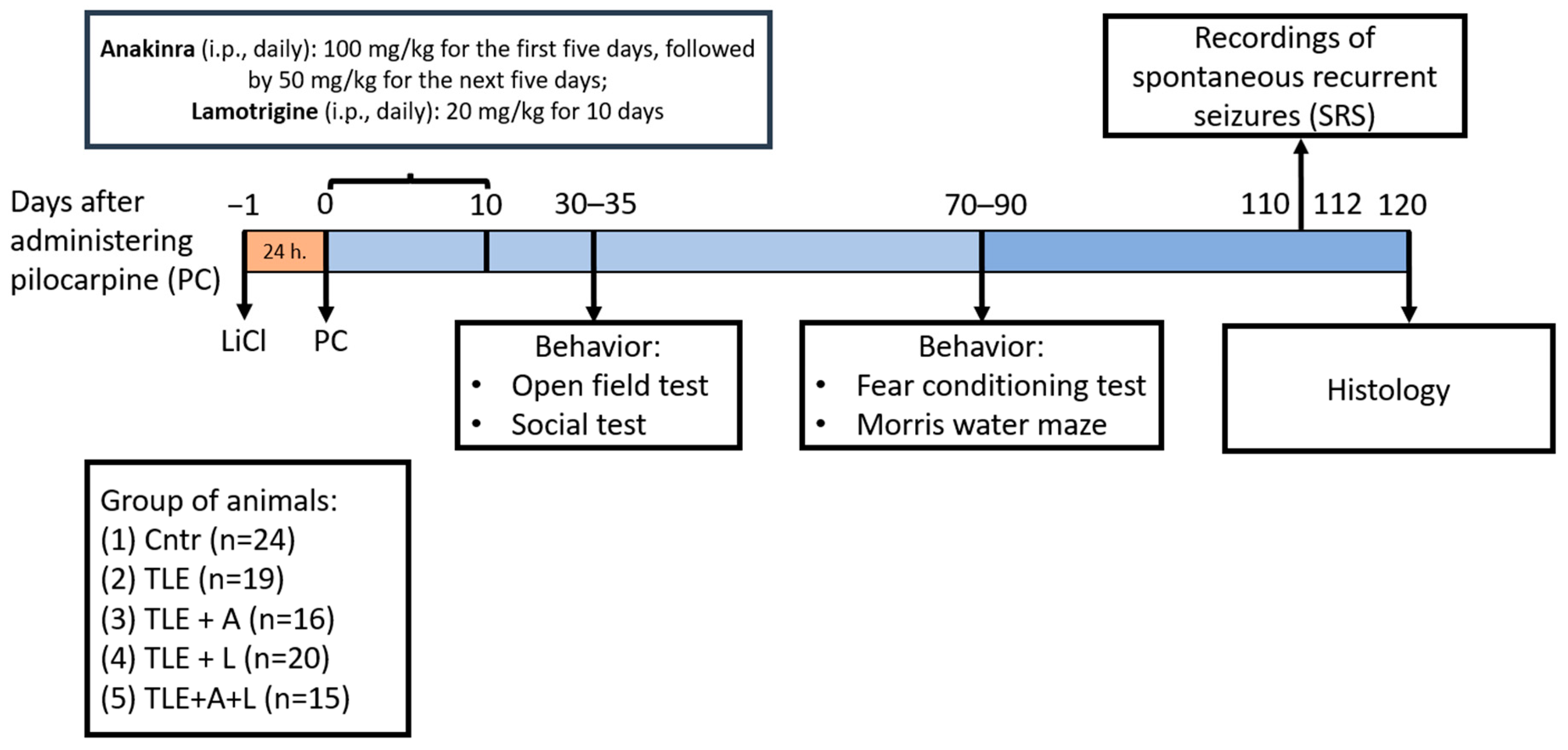
4.2. The Lithium-Pilocarpine Model and Treatment
4.3. Survival Rate and Body Weight
4.4. Spontaneous Recurrent Seizures (SRS)
4.5. Behavioral Testing
4.5.1. Open Field Test
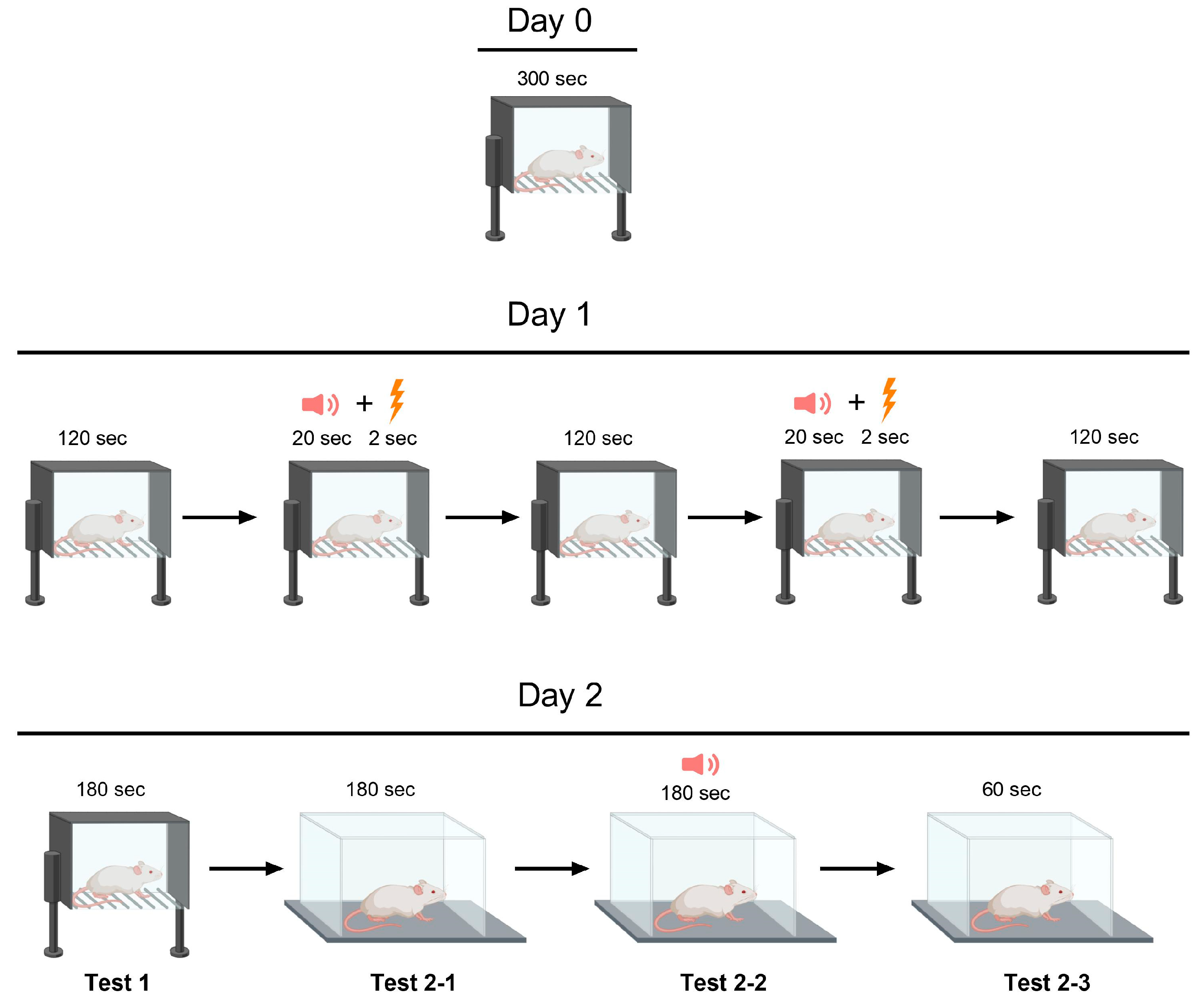
4.5.2. Fear Conditioning Test
4.5.3. Social Interaction Test
4.5.4. Morris Water Maze
4.6. Histology
4.7. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Indicators | Untreated TLE Rats (−3) vs. Treated with Anakinra (TLE+A; +1); Lamotrigine (TLE+L; +1) and Combined Treatment (TLE+A+L; +1) | Untreated TLE Rats (−2) vs. Treated with Anakinra (TLE+A; +1) and Combined Treatment (TLE+A+L; +1) | Untreated TLE Rats (−2) vs. Treated with Lamotrigine (TLE+L; +1) and Combined Treatment (TLE+A+L; +1) | Monotherapy with Anakinra (−1) and Lamotrigine (−1) vs. Combined Therapy (TLE+A+L; +2) |
|---|---|---|---|---|
| Histological studies | ||||
| Neuronal death in CA1 hippocampal regions | t = 2.93; p = 0.02 | t = 2.89; p = 0.02 | t = 2.85; p = 0.022 | t = 0.4; p = 0.70 |
| Neuronal death in CA3 hippocampal regions | t = 2.50; p = 0.022 | t = 2.08; p > 0.05 | t = 1.56; p >0.05 | t = 1.56; p = 0.14 |
| The Open Field test | ||||
| Time of locomotion | t = 1.30; p = 0.20 | t = 1.10; p = 0.28 | t = 1.24; p = 0.22 | t = 0.30; p = 0.76 |
| Number of climbing | t = 2.55; p = 0.013 | t = 2.50; p = 0.015 | t = 2.68; p = 0.009 | t = 1.15; p = 0.25 |
| Number of acts | t = 2.66; p = 0.01 | t = 2.31; p = 0.02 | t = 2.74; p = 0.98 | t = 1.15; p = 0.88 |
| Time in the center | t = 1.40; p = 0.17 | t = 1.20; p = 0.24 | t = 0.24; p = 0.01 | t = 3.86; p = 0.001 |
| Social test | ||||
| Time of communication | t = 0.67; p = 0.50 | t = 0.37; p = 0.71 | t = 1.09; p = 0.28 | t = 0.60; p = 0.55 |
| Morris water maze | ||||
| Total distance during training | t = 0.25; p = 0.80 | t = 0.22; p = 0.83 | t = 0,56; p = 0.58 | t = 0.26; p = 0.80 |
| Time in the target area (during 90 s) | t = 0.085; p = 0.93 | t = 0.17; p = 0.87 | t = 0,19; p = 0.87 | t = 0.19; p = 0.85 |
| Time in the target area (during 30 s) | t = 0.33; p = 0.74 | t = 0.18; p = 0.86 | t = 0,39; p = 0.70 | t = 0.78; p = 0.45 |
References
- Thijs, R.D.; Surges, R.; O’Brien, T.J.; Sander, J.W. Epilepsy in Adults. Lancet 2019, 393, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, K.A.; Lopez Ramos, C.; Buch, V.P.; Mekary, R.A.; Amundson, J.R.; Shah, M.; Rattani, A.; Dewan, M.C.; Park, K.B. An Estimation of Global Volume of Surgically Treatable Epilepsy Based on a Systematic Review and Meta-Analysis of Epilepsy. J. Neurosurg. 2019, 130, 1127–1141. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Liu, Y.; Yu, X.; Wu, J.; Poon, A.N.; Demaio, A.; Wang, W.; Rudan, I.; Chan, K.Y. Prevalence of Epilepsy in China between 1990 and 2015: A Systematic Review and Meta–Analysis. J. Glob. Health 2017, 7, 020706. [Google Scholar] [CrossRef] [PubMed]
- Querol Pascual, M.R. Temporal Lobe Epilepsy: Clinical Semiology and Neurophysiological Studies. Semin. Ultrasound CT MRI 2007, 28, 416–423. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.O. Cellular and Molecular Basis of Epilepsy. J. Neurosci. 1994, 14, 3413–3425. [Google Scholar] [CrossRef] [PubMed]
- Téllez-Zenteno, J.F.; Hernández-Ronquillo, L. A Review of the Epidemiology of Temporal Lobe Epilepsy. Epilepsy Res. Treat. 2012, 2012, 630853. [Google Scholar] [CrossRef]
- Hendriks, M.P.H.; Aldenkamp, A.P.; van der Vlugt, H.; Alpherts, W.C.J.; Vermeulen, J. Memory Complaints in Medically Refractory Epilepsy: Relationship to Epilepsy-Related Factors. Epilepsy Behav. 2002, 3, 165–172. [Google Scholar] [CrossRef]
- Tramoni-Negre, E.; Lambert, I.; Bartolomei, F.; Felician, O. Long-Term Memory Deficits in Temporal Lobe Epilepsy. Rev. Neurol. 2017, 173, 490–497. [Google Scholar] [CrossRef]
- Swinkels, W.A.M.; Kuyk, J.; van Dyck, R.; Spinhoven, P. Psychiatric Comorbidity in Epilepsy. Epilepsy Behav. 2005, 7, 37–50. [Google Scholar] [CrossRef]
- Bonora, A.; Benuzzi, F.; Monti, G.; Mirandola, L.; Pugnaghi, M.; Nichelli, P.; Meletti, S. Recognition of Emotions from Faces and Voices in Medial Temporal Lobe Epilepsy. Epilepsy Behav. 2011, 20, 648–654. [Google Scholar] [CrossRef]
- Giovagnoli, A.R.; Franceschetti, S.; Reati, F.; Parente, A.; Maccagnano, C.; Villani, F.; Spreafico, R. Theory of Mind in Frontal and Temporal Lobe Epilepsy: Cognitive and Neural Aspects. Epilepsia 2011, 52, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Laxer, K.D.; Trinka, E.; Hirsch, L.J.; Cendes, F.; Langfitt, J.; Delanty, N.; Resnick, T.; Benbadis, S.R. The Consequences of Refractory Epilepsy and Its Treatment. Epilepsy Behav. 2014, 37, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, D.; Schachter, S.C. Drug Treatment of Epilepsy in Adults. BMJ 2014, 348, g254. [Google Scholar] [CrossRef] [PubMed]
- Löscher, W.; Schmidt, D. Modern Antiepileptic Drug Development Has Failed to Deliver: Ways out of the Current Dilemma. Epilepsia 2011, 52, 657–678. [Google Scholar] [CrossRef] [PubMed]
- Walia, K.S.; Khan, E.A.; Ko, D.H.; Raza, S.S.; Khan, Y.N. Side Effects of Antiepileptics—A Review. Pain Pract. 2004, 4, 194–203. [Google Scholar] [CrossRef]
- Mula, M.; Kanner, A.M.; Schmitz, B.; Schachter, S. Antiepileptic Drugs and Suicidality: An Expert Consensus Statement from the Task Force on Therapeutic Strategies of the ILAE Commission on Neuropsychobiology. Epilepsia 2013, 54, 199–203. [Google Scholar] [CrossRef]
- Schmidt, D. Is Antiepileptogenesis a Realistic Goal in Clinical Trials? Concerns and New Horizons. Epileptic Disord. 2012, 14, 105–113. [Google Scholar] [CrossRef]
- Galanopoulou, A.S.; Buckmaster, P.S.; Staley, K.J.; Moshé, S.L.; Perucca, E.; Engel, J., Jr.; Löscher, W.; Noebels, J.L.; Pitkänen, A.; Stables, J.; et al. Identification of New Epilepsy Treatments: Issues in Preclinical Methodology. Epilepsia 2012, 53, 571–582. [Google Scholar] [CrossRef]
- Rana, A.; Musto, A.E. The Role of Inflammation in the Development of Epilepsy. J. Neuroinflammation 2018, 15, 144. [Google Scholar] [CrossRef]
- Vezzani, A.; French, J.; Bartfai, T.; Baram, T.Z. The Role of Inflammation in Epilepsy. Nat. Rev. Neurol. 2011, 7, 31–40. [Google Scholar] [CrossRef]
- Shimada, T.; Takemiya, T.; Sugiura, H.; Yamagata, K. Role of Inflammatory Mediators in the Pathogenesis of Epilepsy. Mediat. Inflamm. 2014, 2014, 901902. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, A.; Ravizza, T.; Bedner, P.; Aronica, E.; Steinhäuser, C.; Boison, D. Astrocytes in the Initiation and Progression of Epilepsy. Nat. Rev. Neurol. 2022, 18, 707–722. [Google Scholar] [CrossRef]
- Dyomina, A.V.; Zubareva, O.E.; Smolensky, I.V.; Vasilev, D.S.; Zakharova, M.V.; Kovalenko, A.A.; Schwarz, A.P.; Ischenko, A.M.; Zaitsev, A.V. Anakinra Reduces Epileptogenesis, Provides Neuroprotection, and Attenuates Behavioral Impairments in Rats in the Lithium–Pilocarpine Model of Epilepsy. Pharmaceuticals 2020, 13, 340. [Google Scholar] [CrossRef] [PubMed]
- Dilena, R.; Mauri, E.; Aronica, E.; Bernasconi, P.; Bana, C.; Cappelletti, C.; Carrabba, G.; Ferrero, S.; Giorda, R.; Guez, S.; et al. Therapeutic Effect of Anakinra in the Relapsing Chronic Phase of Febrile Infection–Related Epilepsy Syndrome. Epilepsia Open 2019, 4, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Taraschenko, O.; Fox, H.S.; Zekeridou, A.; Pittock, S.J.; Eldridge, E.; Farukhuddin, F.; Al-Saleem, F.; Devi Kattala, C.; Dessain, S.K.; Casale, G.; et al. Seizures and Memory Impairment Induced by Patient-Derived Anti-N-Methyl-D-Aspartate Receptor Antibodies in Mice Are Attenuated by Anakinra, an Interleukin-1 Receptor Antagonist. Epilepsia 2021, 62, 671–682. [Google Scholar] [CrossRef]
- Costa, B.; Vale, N. Understanding Lamotrigine’s Role in the CNS and Possible Future Evolution. Int. J. Mol. Sci. 2023, 24, 6050. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; He, X.; Sun, Q.; Fang, Z.; Zhou, L. Effect of Lamotrigine on Seizure Development in a Rat Pentylenetetrazole Kindling Model. Brain Behav. 2017, 7, e00727. [Google Scholar] [CrossRef]
- Stratton, S.C.; Large, C.H.; Cox, B.; Davies, G.; Hagan, R.M. Effects of Lamotrigine and Levetiracetam on Seizure Development in a Rat Amygdala Kindling Model. Epilepsy Res. 2003, 53, 95–106. [Google Scholar] [CrossRef]
- Nissinen, J.; Large, C.H.; Stratton, S.C.; Pitkänen, A. Effect of Lamotrigine Treatment on Epileptogenesis: An Experimental Study in Rat. Epilepsy Res. 2004, 58, 119–132. [Google Scholar] [CrossRef]
- Wang, J.; Chen, Y.; Wang, Q.; van Luijtelaar, G.; Sun, M. The Effects of Lamotrigine and Ethosuximide on Seizure Frequency, Neuronal Loss, and Astrogliosis in a Model of Temporal-Lobe Epilepsy. Brain Res. 2019, 1712, 1–6. [Google Scholar] [CrossRef]
- Zubareva, O.E.; Dyomina, A.V.; Kovalenko, A.A.; Roginskaya, A.I.; Melik-Kasumov, T.B.; Korneeva, M.A.; Chuprina, A.V.; Zhabinskaya, A.A.; Kolyhan, S.A.; Zakharova, M.V.; et al. Beneficial Effects of Probiotic Bifidobacterium Longum in a Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Rats. Int. J. Mol. Sci. 2023, 24, 8451. [Google Scholar] [CrossRef] [PubMed]
- Mirabel, H.; Guinet, V.; Voltzenlogel, V.; Pradier, S.; Hennion, S. Social Cognition in Epilepsy: State of the Art and Perspectives. Rev. Neurol. 2020, 176, 468–479. [Google Scholar] [CrossRef] [PubMed]
- Smolensky, I.V.; Zubareva, O.E.; Kalemenev, S.V.; Lavrentyeva, V.V.; Dyomina, A.V.; Karepanov, A.A.; Zaitsev, A.V. Impairments in Cognitive Functions and Emotional and Social Behaviors in a Rat Lithium-Pilocarpine Model of Temporal Lobe Epilepsy. Behav. Brain Res. 2019, 372, 112044. [Google Scholar] [CrossRef] [PubMed]
- Cavalheiro, E.A. The Pilocarpine Model of Epilepsy. Ital. J. Neurol. Sci. 1995, 16, 33–37. [Google Scholar] [CrossRef]
- Löscher, W.; Potschka, H. Role of Multidrug Transporters in Pharmacoresistance to Antiepileptic Drugs. J. Pharmacol. Exp. Ther. 2002, 301, 7–14. [Google Scholar] [CrossRef]
- Löscher, W. Critical Review of Current Animal Models of Seizures and Epilepsy Used in the Discovery and Development of New Antiepileptic Drugs. Seizure 2011, 20, 359–368. [Google Scholar] [CrossRef]
- Morimoto, K.; Fahnestock, M.; Racine, R.J. Kindling and Status Epilepticus Models of Epilepsy: Rewiring the Brain. Prog. Neurobiol. 2004, 73, 1–60. [Google Scholar] [CrossRef]
- Reddy, D.S.; Bhimani, A.; Kuruba, R.; Park, M.J.; Sohrabji, F. Prospects of Modeling Poststroke Epileptogenesis. J. Neurosci. Res. 2017, 95, 1000–1016. [Google Scholar] [CrossRef]
- Pitkänen, A.; Lukasiuk, K.; Dudek, F.E.; Staley, K.J. Epileptogenesis. Cold Spring Harb. Perspect. Med. 2015, 5, a022822. [Google Scholar] [CrossRef]
- Hufthy, Y.; Bharadwaj, M.; Gupta, S.; Hussain, D.; Joseph, P.J.S.; Khan, A.; King, J.; Lahorgue, P.; Jayawardena, O.; Rostami-Hochaghan, D.; et al. Statins as Antiepileptogenic Drugs: Analyzing the Evidence and Identifying the Most Promising Statin. Epilepsia 2022, 63, 1889–1898. [Google Scholar] [CrossRef]
- Sills, G.J.; Rogawski, M.A. Mechanisms of Action of Currently Used Antiseizure Drugs. Neuropharmacology 2020, 168, 107966. [Google Scholar] [CrossRef]
- Kuo, C.-C.; Lu, L. Characterization of Lamotrigine Inhibition of Na + Channels in Rat Hippocampal Neurones. Br. J. Pharmacol. 1997, 121, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-J.; Huang, C.-C.; Hsu, K.-S.; Tsai, J.-J.; Gean, P.-W. Inhibition of N-Type Calcium Currents by Lamotrigine in Rat Amygdalar Neurones. Neuroreport 1996, 7, 3037–3040. [Google Scholar] [CrossRef] [PubMed]
- Stefani, A.; Spadoni, F.; Siniscalchi, A.; Bernardi, G. Lamotrigine Inhibits Ca2+ Currents in Cortical Neurons: Functional Implications. Eur. J. Pharmacol. 1996, 307, 113–116. [Google Scholar] [CrossRef]
- Bacher, A.; Zornow, M.H. Lamotrigine Inhibits Extracellular Glutamate Accumulation during Transient Global Cerebral Ischemia in Rabbits. Anesthesiology 1997, 86, 459–463. [Google Scholar] [CrossRef]
- Farber, N.B.; Jiang, X.-P.; Heinkel, C.; Nemmers, B. Antiepileptic Drugs and Agents That Inhibit Voltage-Gated Sodium Channels Prevent NMDA Antagonist Neurotoxicity. Mol. Psychiatry 2002, 7, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Amakhin, D.V.; Malkin, S.L.; Ergina, J.L.; Kryukov, K.A.; Veniaminova, E.A.; Zubareva, O.E.; Zaitsev, A.V. Alterations in Properties of Glutamatergic Transmission in the Temporal Cortex and Hippocampus Following Pilocarpine-Induced Acute Seizures in Wistar Rats. Front. Cell Neurosci. 2017, 11, 264. [Google Scholar] [CrossRef] [PubMed]
- Diespirov, G.P.; Postnikova, T.Y.; Griflyuk, A.V.; Kovalenko, A.A.; Zaitsev, A.V. Alterations in the Properties of the Rat Hippocampus Glutamatergic System in the Lithium-Pilocarpine Model of Temporal Lobe Epilepsy. Biochemistry 2023, 88, 353–363. [Google Scholar] [CrossRef]
- Deng, Y.; Wang, M.; Wang, W.; Ma, C.; He, N. Comparison and Effects of Acute Lamotrigine Treatment on Extracellular Excitatory Amino Acids in the Hippocampus of PTZ-Kindled Epileptic and PTZ-Induced Status Epilepticus Rats. Neurochem. Res. 2013, 38, 504–511. [Google Scholar] [CrossRef]
- Herman, E. Lamotrigine: A Depression Mood Stabiliser. Eur. Neuropsychopharmacol. 2004, 14, S89–S93. [Google Scholar] [CrossRef]
- Abu-rish, E.Y.; Dahabiyeh, L.A.; Bustanji, Y.; Mohamed, Y.S.; Browning, M.J. Effect of Lamotrigine on in Vivo and in Vitro Cytokine Secretion in Murine Model of Inflammation. J. Neuroimmunol. 2018, 322, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Muscal, E.; Wells, E.; Shukla, N.; Eschbach, K.; Hyeong Lee, K.; Kaliakatsos, M.; Desai, N.; Wickström, R.; Viri, M.; et al. Anakinra Usage in Febrile Infection Related Epilepsy Syndrome: An International Cohort. Ann. Clin. Transl. Neurol. 2020, 7, 2467–2474. [Google Scholar] [CrossRef] [PubMed]
- Du, C.; Zheng, F.; Wang, X. Exploring Novel AEDs from Drugs Used for Treatment of Non-Epileptic Disorders. Expert Rev. Neurother. 2016, 16, 449–461. [Google Scholar] [CrossRef]
- Roginskaya, A.I.; Dyomina, A.V.; Kovalenko, A.A.; Zakharova, M.V.; Schwarz, A.P.; Melik-Kasumov, T.B.; Zubareva, O.E. Effect of Anakinra on the Gene Expression of Receptors Activated by the Peroxisome Proliferator in the Rat Brain in the Lithium Pilocarpine Model of Epilepsy. J. Evol. Biochem. Physiol. 2022, 58, 598–609. [Google Scholar] [CrossRef]
- Leal, B.; Chaves, J.; Carvalho, C.; Rangel, R.; Santos, A.; Bettencourt, A.; Lopes, J.; Ramalheira, J.; Silva, B.M.; da Silva, A.M.; et al. Brain Expression of Inflammatory Mediators in Mesial Temporal Lobe Epilepsy Patients. J. Neuroimmunol. 2017, 313, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Litovchenko, A.V.; Zabrodskaya, Y.M.; Sitovskaya, D.A.; Khuzhakhmetova, L.K.; Nezdorovina, V.G.; Bazhanova, E.D. Markers of Neuroinflammation and Apoptosis in the Temporal Lobe of Patients with Drug-Resistant Epilepsy. J. Evol. Biochem. Physiol. 2021, 57, 1040–1049. [Google Scholar] [CrossRef]
- Devinsky, O.; Vezzani, A.; Najjar, S.; De Lanerolle, N.C.; Rogawski, M.A. Glia and Epilepsy: Excitability and Inflammation. Trends Neurosci. 2013, 36, 174–184. [Google Scholar] [CrossRef]
- Viviani, B.; Bartesaghi, S.; Gardoni, F.; Vezzani, A.; Behrens, M.M.; Bartfai, T.; Binaglia, M.; Corsini, E.; Di Luca, M.; Galli, C.L.; et al. Interleukin-1β Enhances NMDA Receptor-Mediated Intracellular Calcium Increase through Activation of the Src Family of Kinases. J. Neurosci. 2003, 23, 8692–8700. [Google Scholar] [CrossRef]
- Komoltsev, I.G.; Frankevich, S.O.; Shirobokova, N.I.; Volkova, A.A.; Onufriev, M.V.; Moiseeva, J.V.; Novikova, M.R.; Gulyaeva, N.V. Neuroinflammation and Neuronal Loss in the Hippocampus Are Associated with Immediate Posttraumatic Seizures and Corticosterone Elevation in Rats. Int. J. Mol. Sci. 2021, 22, 5883. [Google Scholar] [CrossRef]
- Hu, S.; Sheng, W.S.; Ehrlich, L.C.; Peterson, P.K.; Chao, C.C. Cytokine Effects on Glutamate Uptake by Human Astrocytes. Neuroimmunomodulation 2000, 7, 153–159. [Google Scholar] [CrossRef]
- Zaitsev, A.V.; Smolensky, I.V.; Jorratt, P.; Ovsepian, S.V. Neurobiology, Functions, and Relevance of Excitatory Amino Acid Transporters (EAATs) to Treatment of Refractory Epilepsy. CNS Drugs 2020, 34, 1089–1103. [Google Scholar] [CrossRef] [PubMed]
- Mazarati, A.M.; Pineda, E.; Shin, D.; Tio, D.; Taylor, A.N.; Sankar, R. Comorbidity between Epilepsy and Depression: Role of Hippocampal Interleukin-1β. Neurobiol. Dis. 2010, 37, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Suleymanova, E.M. Behavioral Comorbidities of Epilepsy and Neuroinflammation: Evidence from Experimental and Clinical Studies. Epilepsy Behav. 2021, 117, 107869. [Google Scholar] [CrossRef] [PubMed]
- Noe, F.M.; Polascheck, N.; Frigerio, F.; Bankstahl, M.; Ravizza, T.; Marchini, S.; Beltrame, L.; Banderó, C.R.; Löscher, W.; Vezzani, A. Pharmacological Blockade of IL-1β/IL-1 Receptor Type 1 Axis during Epileptogenesis Provides Neuroprotection in Two Rat Models of Temporal Lobe Epilepsy. Neurobiol. Dis. 2013, 59, 183–193. [Google Scholar] [CrossRef]
- Dingledine, R.; Varvel, N.H.; Dudek, F.E. When and How Do Seizures Kill Neurons, and Is Cell Death Relevant to Epileptogenesis? In Issues in Clinical Epileptology: A View from the Bench; Advances in Experimental Medicine and Biology; Springer: Dordrecht, The Netherlands, 2014; Volume 813, pp. 109–122. [Google Scholar]
- Dyomina, A.V.; Kovalenko, A.A.; Zakharova, M.V.; Postnikova, T.Y.; Griflyuk, A.V.; Smolensky, I.V.; Antonova, I.V.; Zaitsev, A. V MTEP, a Selective MGluR5 Antagonist, Had a Neuroprotective Effect but Did Not Prevent the Development of Spontaneous Recurrent Seizures and Behavioral Comorbidities in the Rat Lithium–Pilocarpine Model of Epilepsy. Int. J. Mol. Sci. 2022, 23, 497. [Google Scholar] [CrossRef]
- Beesley, S.; Sullenberger, T.; Crotty, K.; Ailani, R.; D’Orio, C.; Evans, K.; Ogunkunle, E.O.; Roper, M.G.; Kumar, S.S. D-Serine Mitigates Cell Loss Associated with Temporal Lobe Epilepsy. Nat. Commun. 2020, 11, 4966. [Google Scholar] [CrossRef]
- Citraro, R.; Iannone, M.; Leo, A.; De Caro, C.; Nesci, V.; Tallarico, M.; Abdalla, K.; Palma, E.; Arturi, F.; De Sarro, G.; et al. Evaluation of the Effects of Liraglutide on the Development of Epilepsy and Behavioural Alterations in Two Animal Models of Epileptogenesis. Brain Res. Bull. 2019, 153, 133–142. [Google Scholar] [CrossRef]
- Scholl, E.A.; Dudek, F.E.; Ekstrand, J.J. Neuronal Degeneration Is Observed in Multiple Regions Outside the Hippocampus after Lithium Pilocarpine-Induced Status Epilepticus in the Immature Rat. Neuroscience 2013, 252, 45–59. [Google Scholar] [CrossRef]
- Vasilev, D.S.; Tumanova, N.L.; Kim, K.K.; Lavrentyeva, V.V.; Lukomskaya, N.Y.; Zhuravin, I.A.; Magazanik, L.G.; Zaitsev, A.V. Transient Morphological Alterations in the Hippocampus after Pentylenetetrazole-Induced Seizures in Rats. Neurochem. Res. 2018, 43, 1671–1682. [Google Scholar] [CrossRef]
- Postnikova, T.Y.; Trofimova, A.M.; Zakharova, M.V.; Nosova, O.I.; Brazhe, A.R.; Korzhevskii, D.E.; Semyanov, A.V.; Zaitsev, A.V. Delayed Impairment of Hippocampal Synaptic Plasticity after Pentylenetetrazole-Induced Seizures in Young Rats. Int. J. Mol. Sci. 2022, 23, 13461. [Google Scholar] [CrossRef]
- Postnikova, T.Y.; Griflyuk, A.V.; Amakhin, D.V.; Kovalenko, A.A.; Soboleva, E.B.; Zubareva, O.E.; Zaitsev, A.V. Early Life Febrile Seizures Impair Hippocampal Synaptic Plasticity in Young Rats. Int. J. Mol. Sci. 2021, 22, 8218. [Google Scholar] [CrossRef]
- Fröhlich, F. Microcircuits of the Hippocampus. In Network Neuroscience; Elsevier: Amsterdam, The Netherlands, 2016; pp. 97–109. [Google Scholar]
- Ümit Sayin, H. A Bio-Electrical Tornado in the Hippocampus: Mechanisms of Temporal Lobe Epilepsy. NeuroQuantology 2017, 15, 92–103. [Google Scholar] [CrossRef]
- Hitiris, N.; Mohanraj, R.; Norrie, J.; Sills, G.J.; Brodie, M.J. Predictors of Pharmacoresistant Epilepsy. Epilepsy Res. 2007, 75, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Gastens, A.M.; Brandt, C.; Bankstahl, J.P.; Löscher, W. Predictors of Pharmacoresistant Epilepsy: Pharmacoresistant Rats Differ from Pharmacoresponsive Rats in Behavioral and Cognitive Abnormalities Associated with Experimentally Induced Epilepsy. Epilepsia 2008, 49, 1759–1776. [Google Scholar] [CrossRef] [PubMed]
- Rzezak, P.; Lima, E.M.; Gargaro, A.C.; Coimbra, E.; de Vincentiis, S.; Velasco, T.R.; Leite, J.P.; Busatto, G.F.; Valente, K.D. Everyday Memory Impairment in Patients with Temporal Lobe Epilepsy Caused by Hippocampal Sclerosis. Epilepsy Behav. 2017, 69, 31–36. [Google Scholar] [CrossRef]
- Stewart, E.; Catroppa, C.; Gonzalez, L.; Gill, D.; Webster, R.; Lawson, J.; Sabaz, M.; Mandalis, A.; Barton, B.; McLean, S.; et al. Theory of Mind and Social Competence in Children and Adolescents with Temporal Lobe Epilepsy. Neuropsychology 2019, 33, 986–995. [Google Scholar] [CrossRef]
- Montagrin, A.; Saiote, C.; Schiller, D. The Social Hippocampus. Hippocampus 2018, 28, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Marin, J.C.M.; Moura, P.J.; Cysneiros, R.M.; Colugnati, D.B.; Cavalheiro, E.A.; Scorza, F.A.; Xavier, G.F.; Zilbovicius, M.; Mercadante, M.T. Temporal Lobe Epilepsy and Social Behavior: An Animal Model for Autism? Epilepsy Behav. 2008, 13, 43–46. [Google Scholar] [CrossRef]
- Jiang, Y.; Han, C.; Liu, H.; Wang, X.; Zhang, X.; Meng, F.; Zhang, J. Abnormal Hippocampal Functional Network and Related Memory Impairment in Pilocarpine-treated Rats. Epilepsia 2018, 59, 1785–1795. [Google Scholar] [CrossRef]
- Seo, J.; Jung, S.; Lee, S.-Y.; Yang, H.; Kim, B.S.; Choi, J.; Bang, M.; Shin, H.-S.; Jeon, D. Early Deficits in Social Behavior and Cortical Rhythms in Pilocarpine-Induced Mouse Model of Temporal Lobe Epilepsy. Exp. Neurol. 2013, 241, 38–44. [Google Scholar] [CrossRef]
- Miller, J.M.; Kustra, R.P.; Vuong, A.; Hammer, A.E.; Messenheimer, J.A. Depressive Symptoms in Epilepsy. Drugs 2008, 68, 1493–1509. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Fukatsu, N.; Noguchi, T.; Oshima, T.; Tadokoro, Y.; Kanemoto, K. Lamotrigine Improves Aggression in Patients with Temporal Lobe Epilepsy. Epilepsy Behav. 2011, 21, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Mahfoz, A.M.; Abdel-Wahab, A.F.; Afify, M.A.; Shahzad, N.; Ibrahim, I.A.A.; ElSawy, N.A.; Bamagous, G.A.; Al Ghamdi, S.S. Neuroprotective Effects of Vitamin D Alone or in Combination with Lamotrigine against Lithium-Pilocarpine Model of Status Epilepticus in Rats. Naunyn. Schmiedebergs Arch. Pharmacol. 2017, 390, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Racine, R.J. Modification of Seizure Activity by Electrical Stimulation. II. Motor Seizure. Electroencephalogr. Clin. Neurophysiol. 1972, 32, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Postnikova, T.Y.; Diespirov, G.P.; Amakhin, D.V.; Vylekzhanina, E.N.; Soboleva, E.B.; Zaitsev, A.V. Impairments of Long-Term Synaptic Plasticity in the Hippocampus of Young Rats during the Latent Phase of the Lithium-Pilocarpine Model of Temporal Lobe Epilepsy. Int. J. Mol. Sci. 2021, 22, 13355. [Google Scholar] [CrossRef] [PubMed]
- Furr, R.M. A Contrast Analysis Approach to Change. Educ. Res. Eval. 2008, 14, 335–362. [Google Scholar] [CrossRef]
- Konietschke, F.; Bösiger, S.; Brunner, E.; Hothorn, L.A. Are Multiple Contrast Tests Superior to the ANOVA? Int. J. Biostat. 2013, 9, 63–73. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zubareva, O.E.; Sinyak, D.S.; Kalita, A.D.; Griflyuk, A.V.; Diespirov, G.P.; Postnikova, T.Y.; Zaitsev, A.V. Antiepileptogenic Effects of Anakinra, Lamotrigine and Their Combination in a Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Rats. Int. J. Mol. Sci. 2023, 24, 15400. https://doi.org/10.3390/ijms242015400
Zubareva OE, Sinyak DS, Kalita AD, Griflyuk AV, Diespirov GP, Postnikova TY, Zaitsev AV. Antiepileptogenic Effects of Anakinra, Lamotrigine and Their Combination in a Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Rats. International Journal of Molecular Sciences. 2023; 24(20):15400. https://doi.org/10.3390/ijms242015400
Chicago/Turabian StyleZubareva, Olga E., Denis S. Sinyak, Alisa D. Kalita, Alexandra V. Griflyuk, Georgy P. Diespirov, Tatiana Y. Postnikova, and Aleksey V. Zaitsev. 2023. "Antiepileptogenic Effects of Anakinra, Lamotrigine and Their Combination in a Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Rats" International Journal of Molecular Sciences 24, no. 20: 15400. https://doi.org/10.3390/ijms242015400
APA StyleZubareva, O. E., Sinyak, D. S., Kalita, A. D., Griflyuk, A. V., Diespirov, G. P., Postnikova, T. Y., & Zaitsev, A. V. (2023). Antiepileptogenic Effects of Anakinra, Lamotrigine and Their Combination in a Lithium–Pilocarpine Model of Temporal Lobe Epilepsy in Rats. International Journal of Molecular Sciences, 24(20), 15400. https://doi.org/10.3390/ijms242015400