
The Old and the New: Cardiovascular and Respiratory Alterations Induced by Acute JWH-018 Administration Compared to Δ9-THC—A Preclinical Study in Mice


 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Results
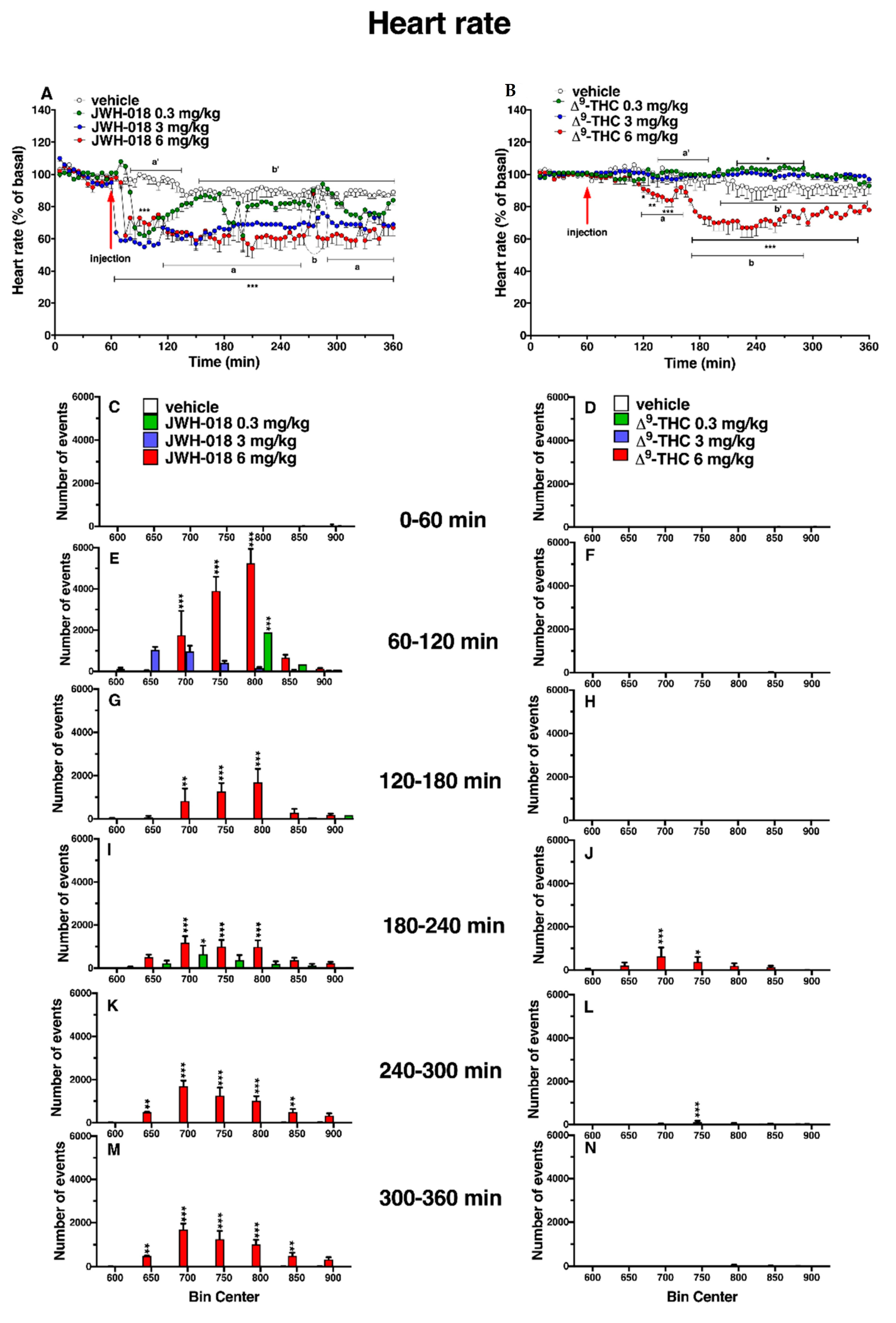
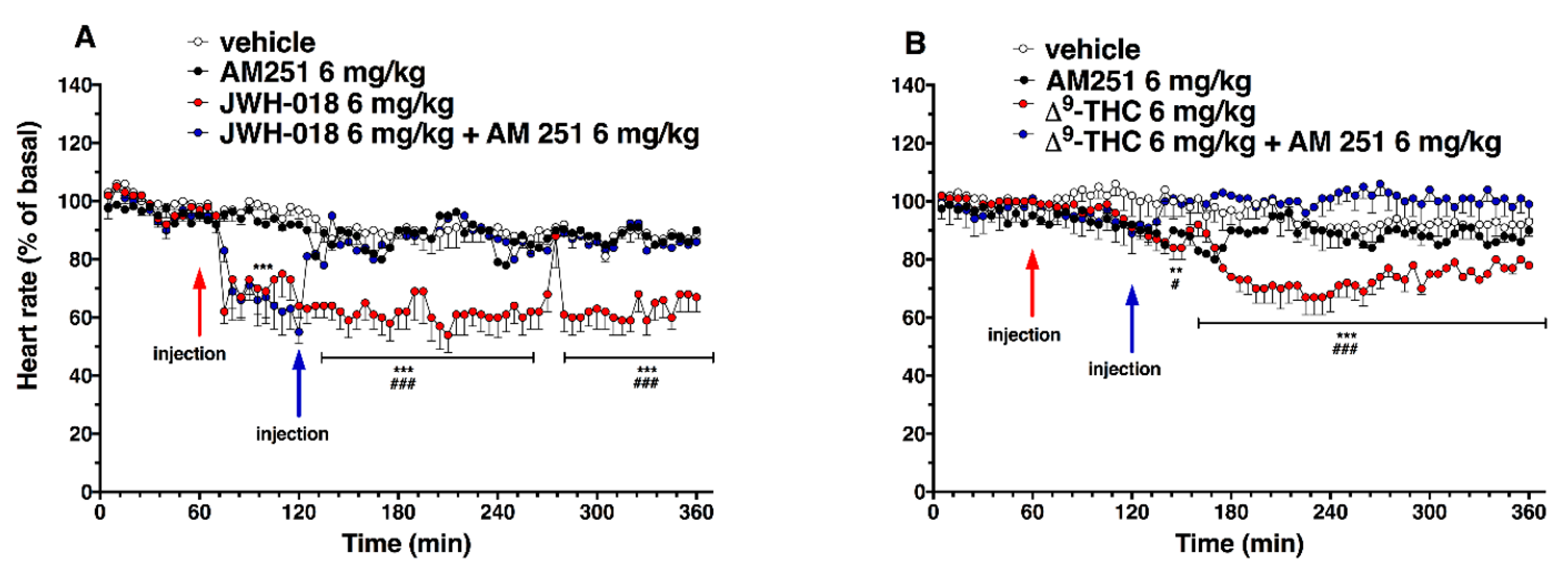
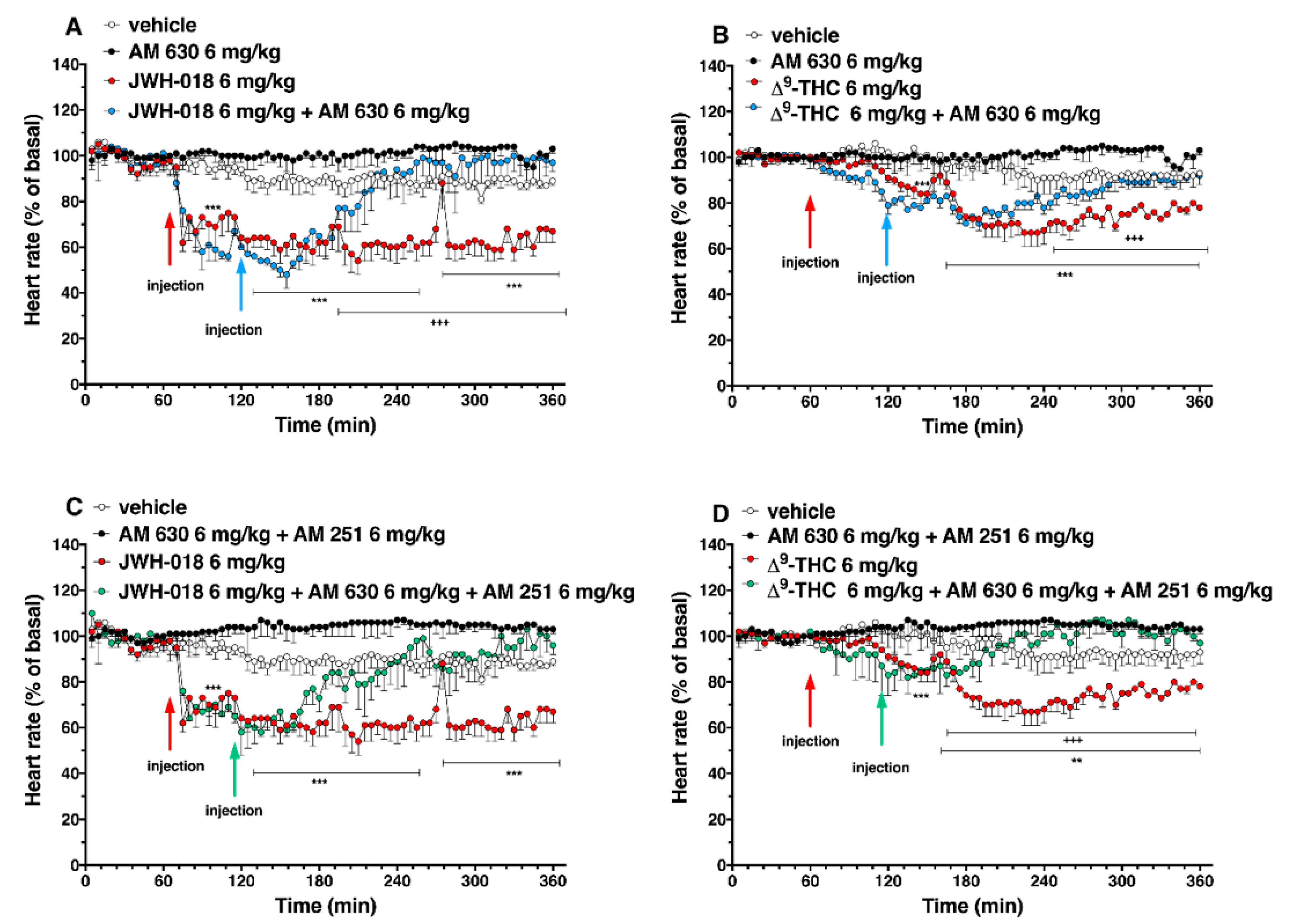
2.1. Heart Rate
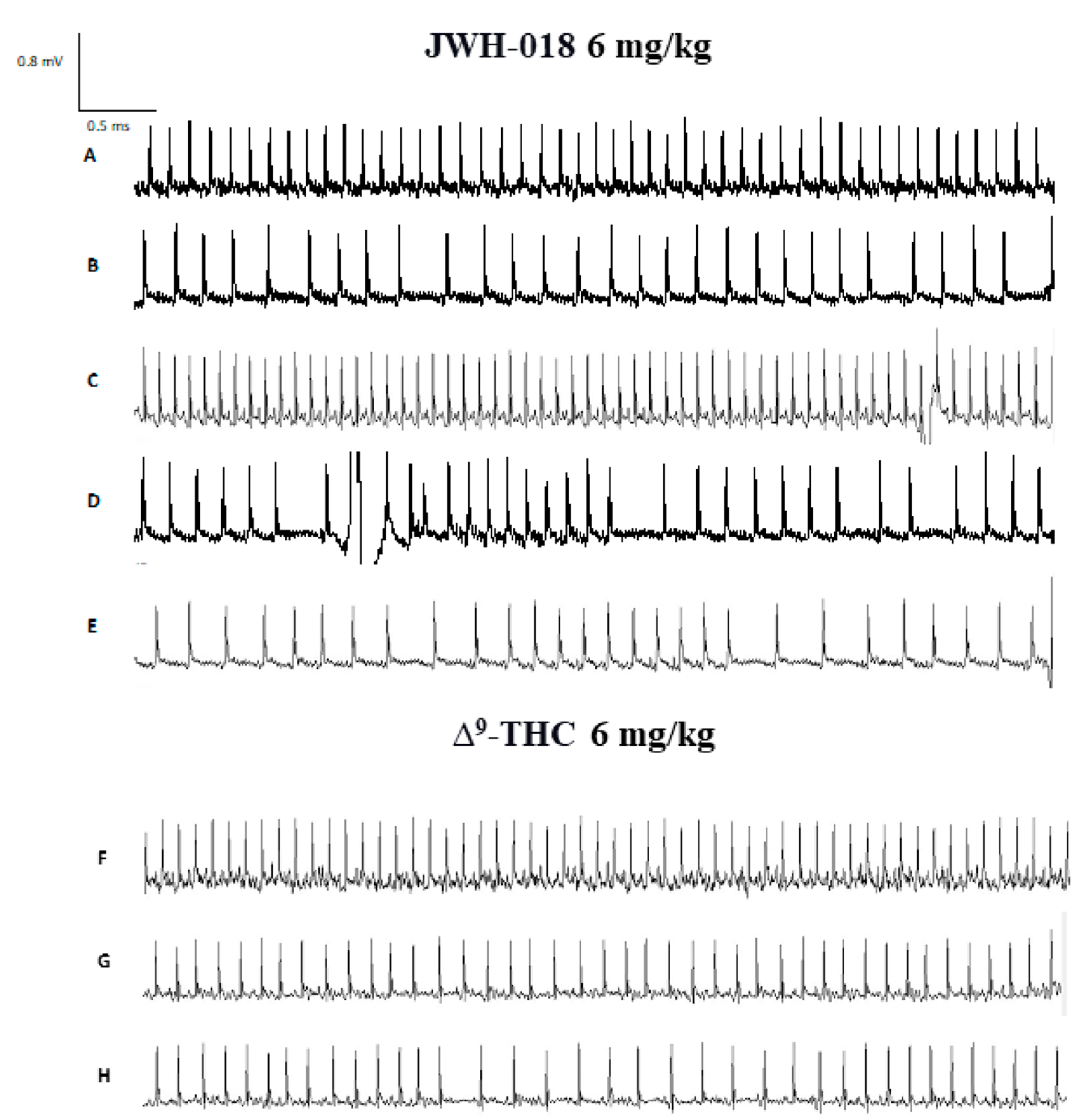
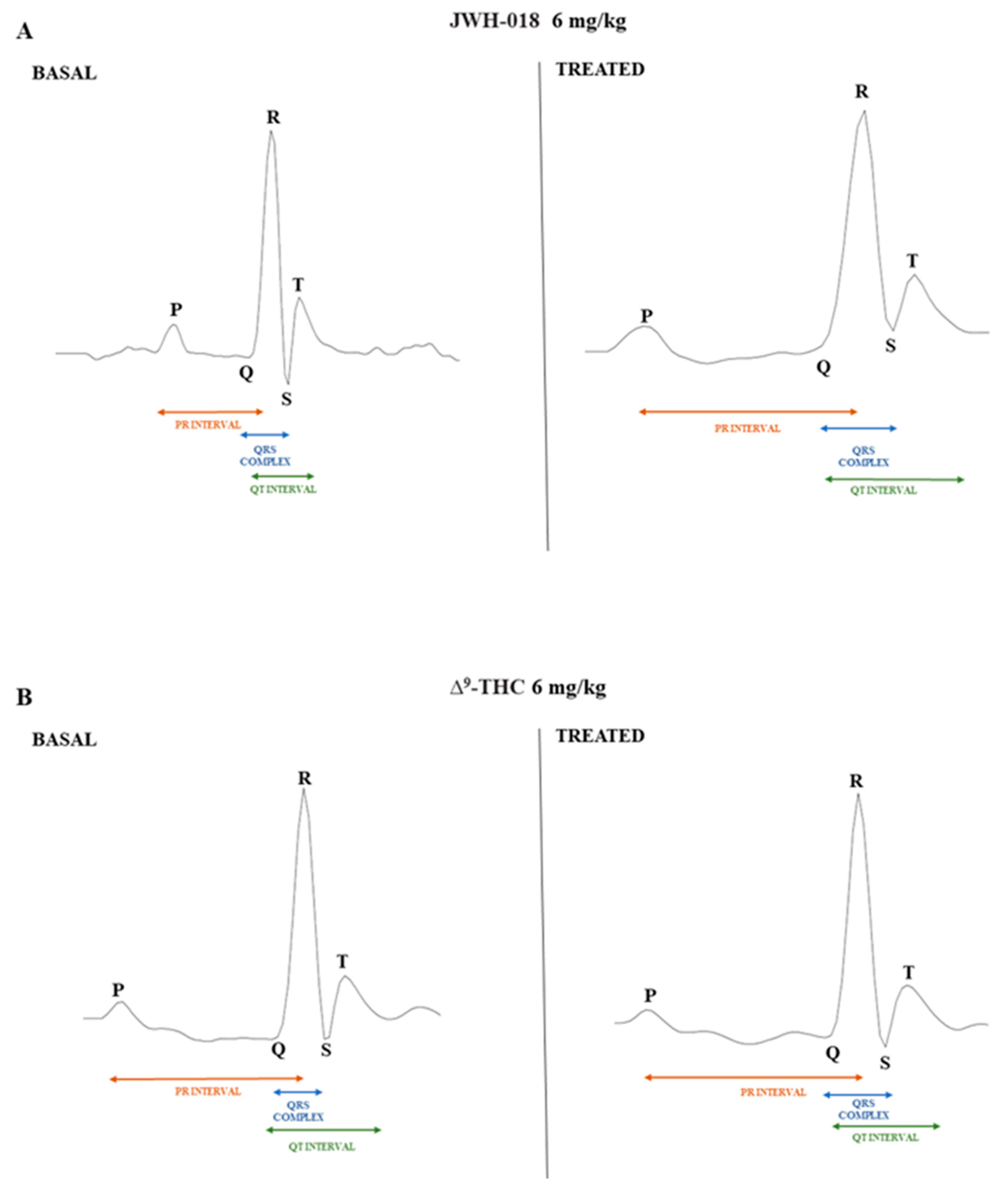
2.2. Electrocardiogram Parameters and Recording
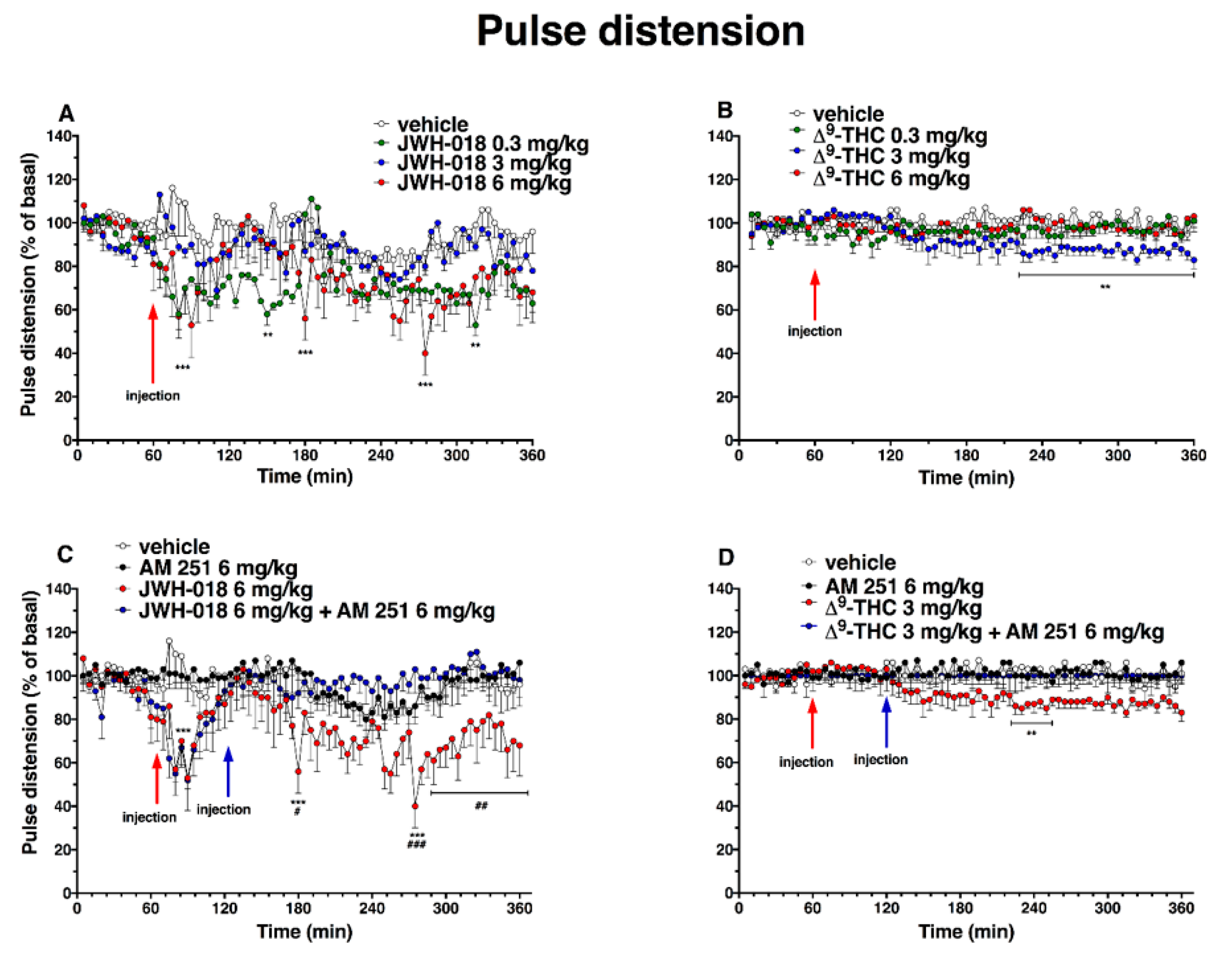
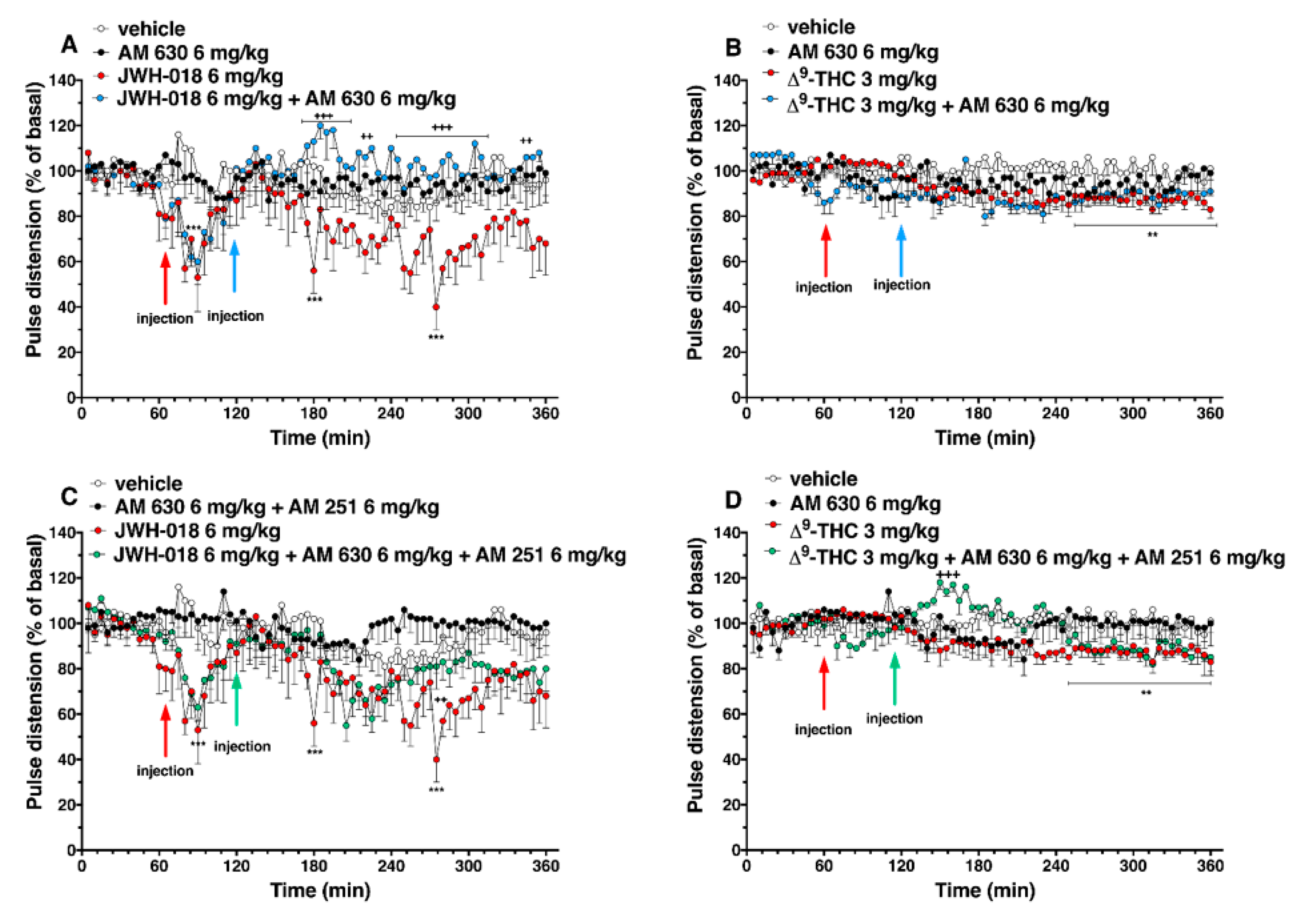
2.3. Pulse Distension
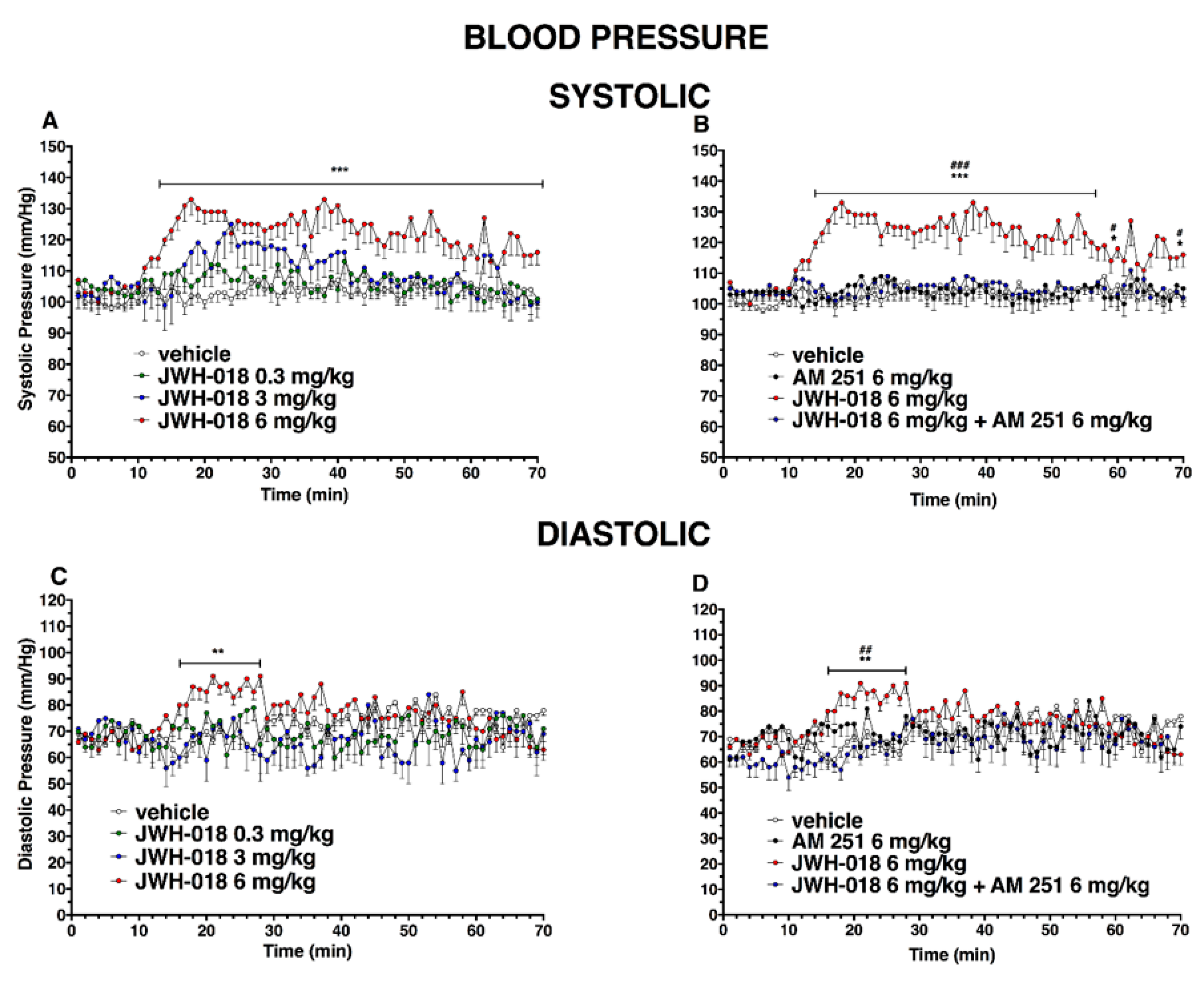
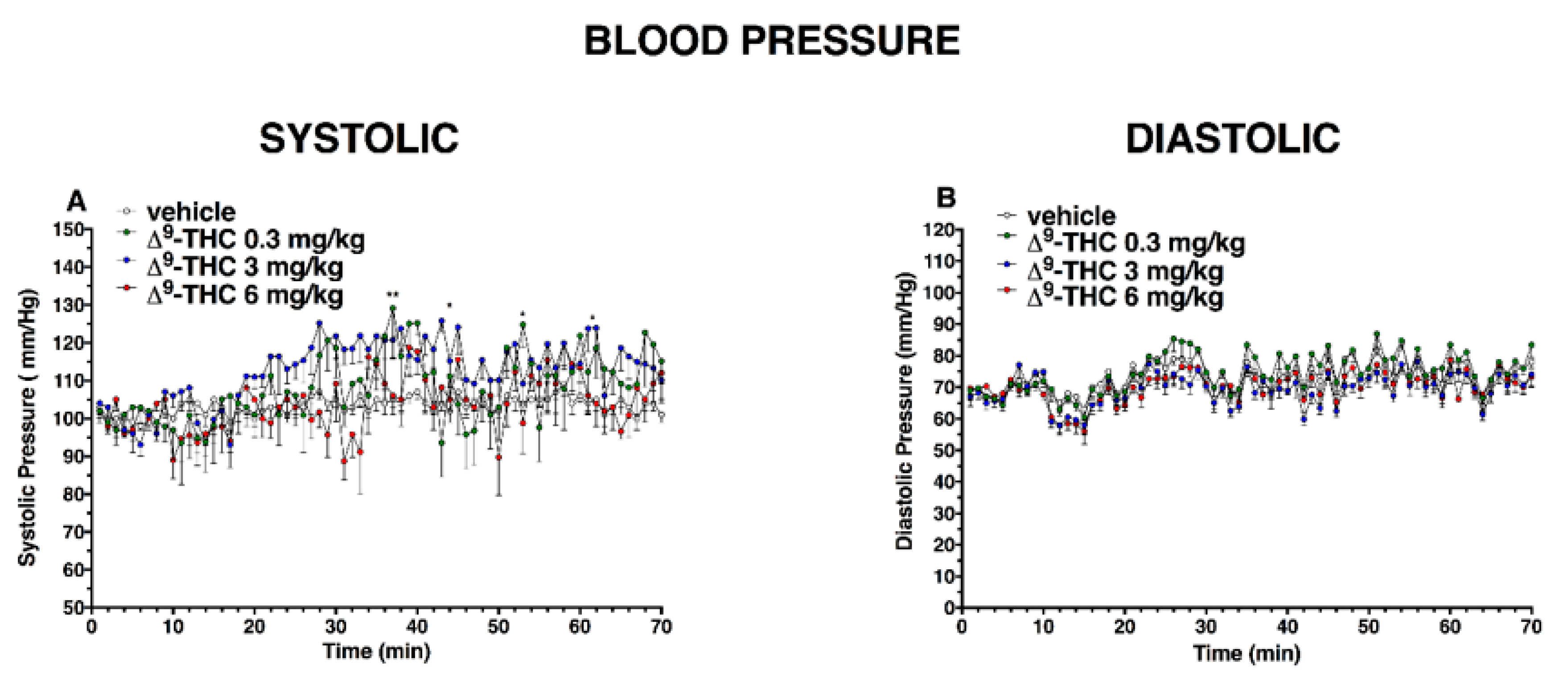
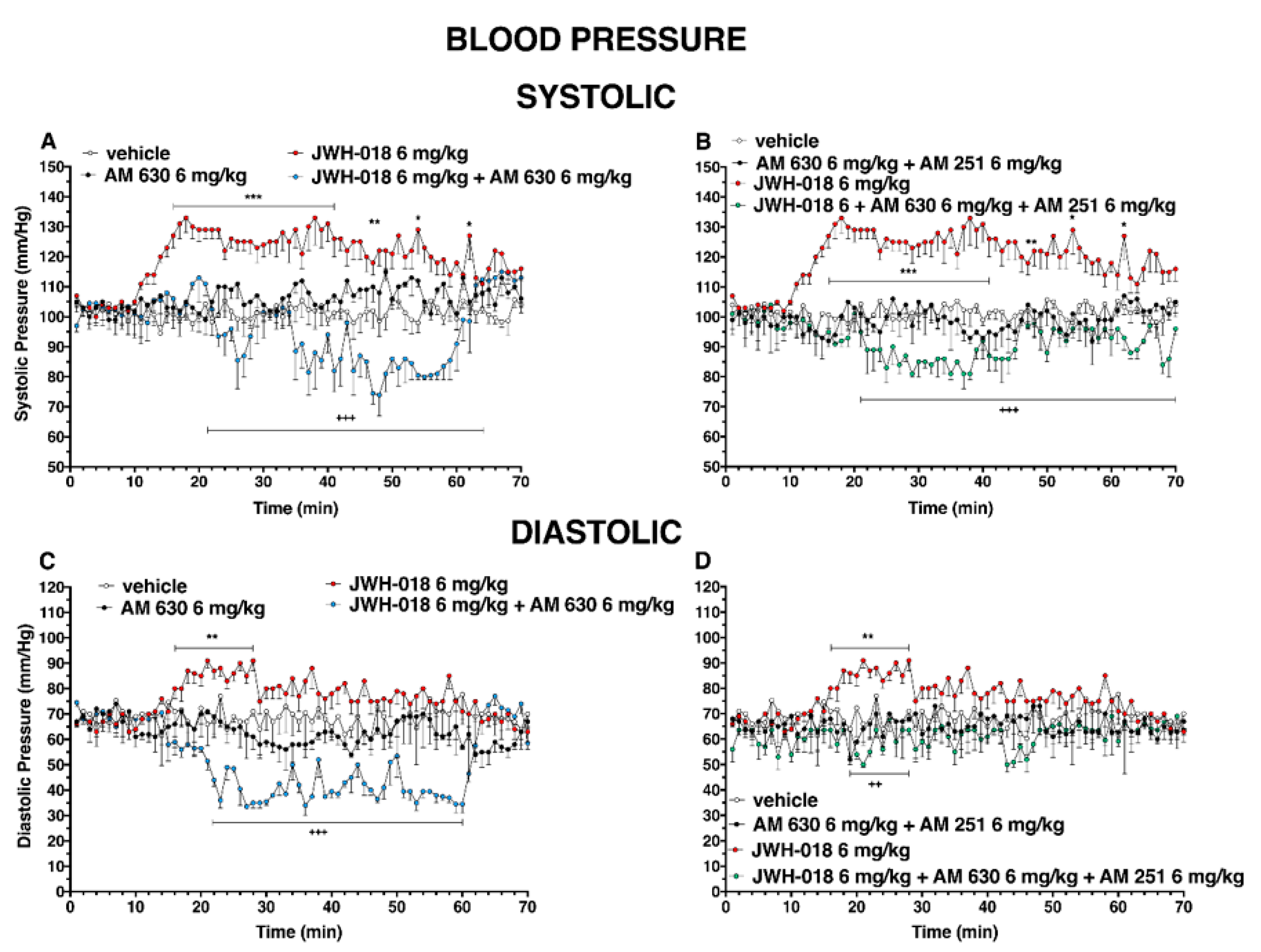
2.4. Blood Pressure
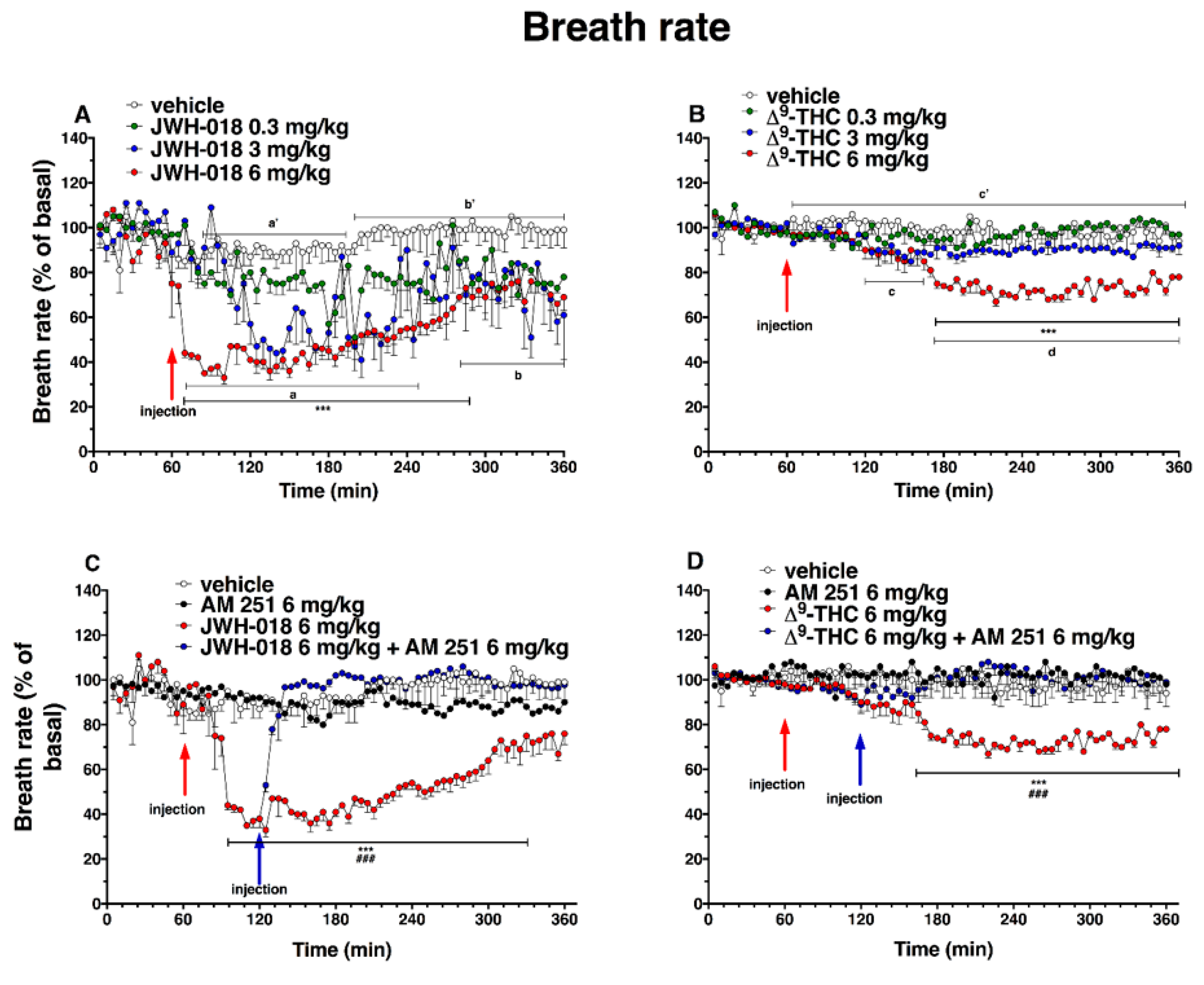
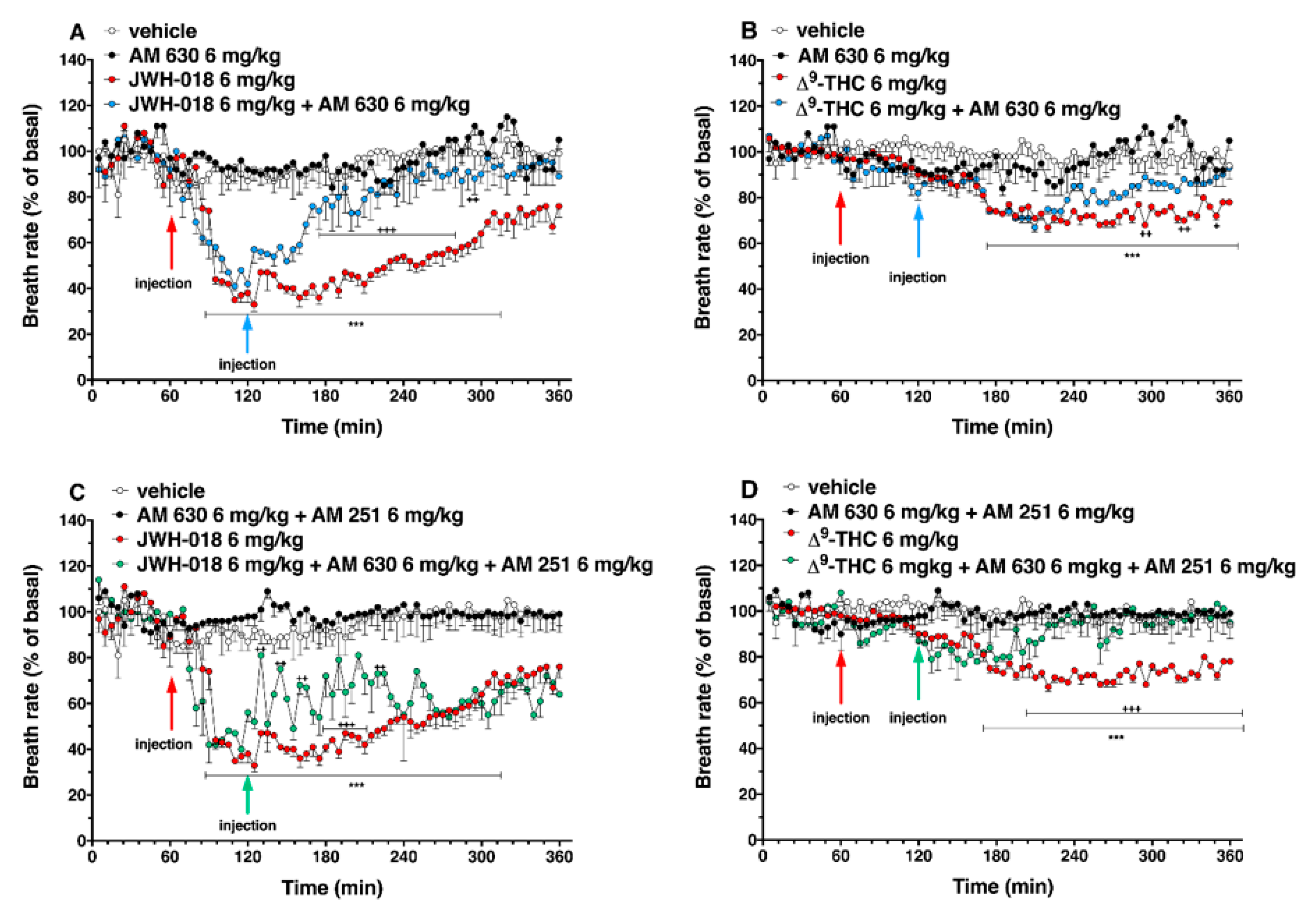
2.5. Breath Rate
2.6. Plethysmography
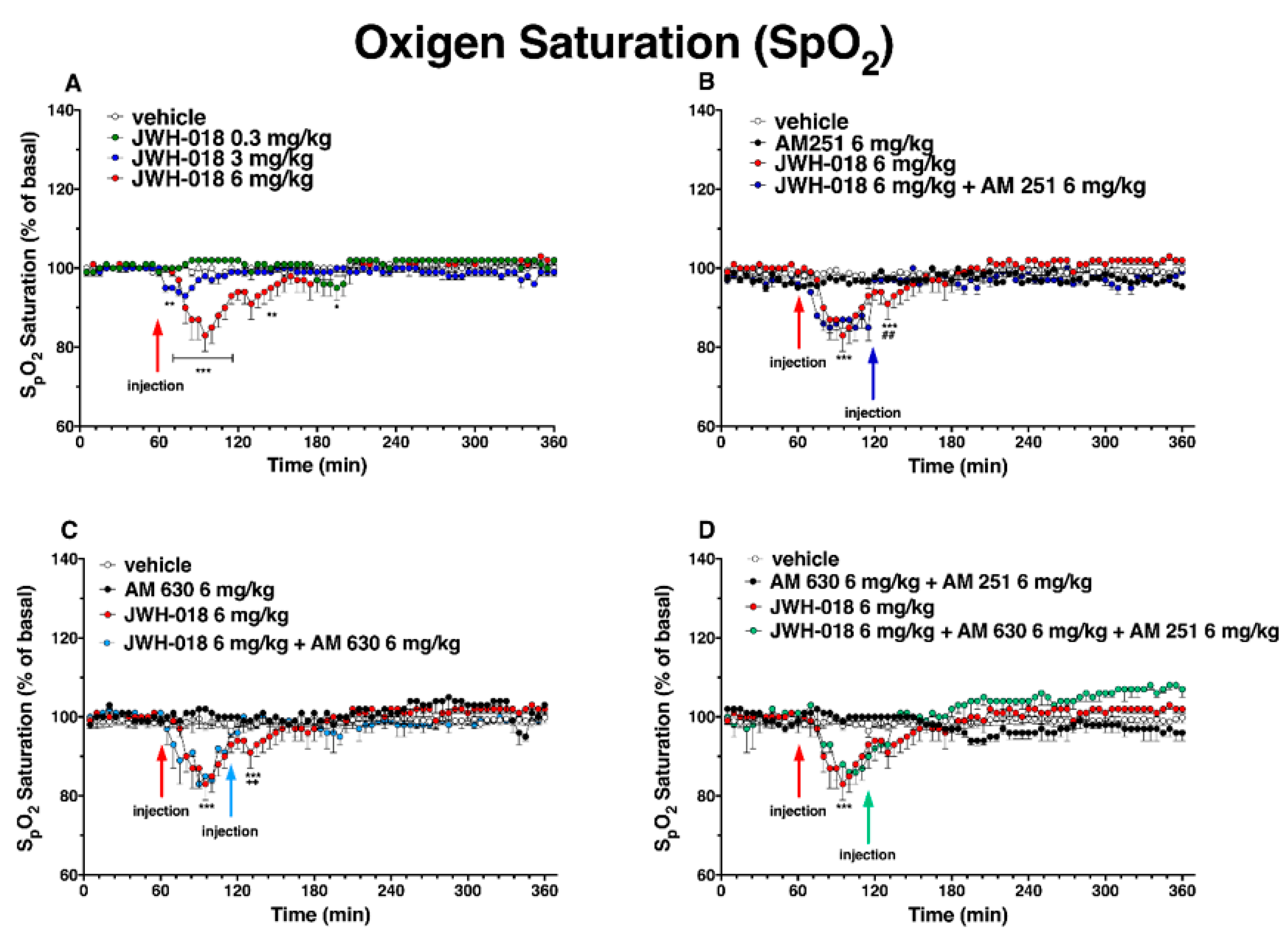
2.7. Oxygen Saturation
3. Discussion
3.1. Cardiovascular Effects
3.2. Respiratory Effects
4. Materials and Methods
4.1. Animals
4.2. Drug Preparation and Dose Selection
4.3. Evaluation of Cardiorespiratory and Blood Pressure Changes
4.4. Data and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Statement
Abbreviations
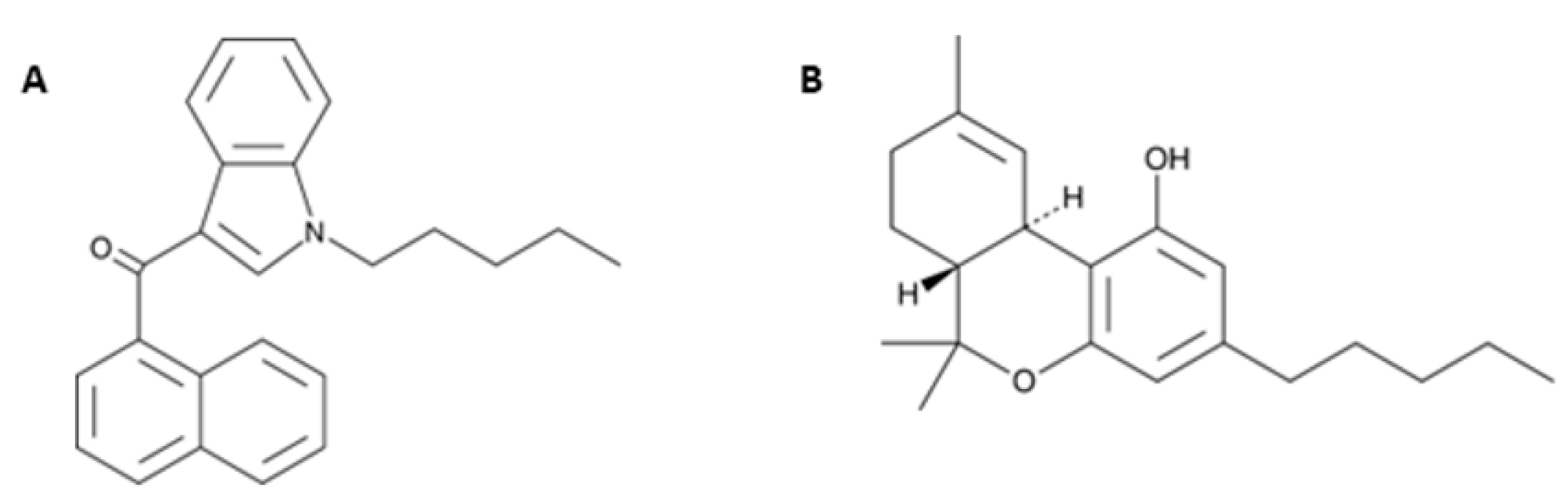
| JWH-018 | 1-naphthalenyl(1-pentyl-1H-indol-3-yl)-methanone |
| AM 251 | 1-(2,4-dichlorophenyl)-5-(4-iodophenyl)-4-methyl-N-(piperidin-1-yl)-1H-pyrazole-3-carboxamide |
| AM 630 | 6-Iodo-2-methyl-1-[2-(4-morpholinyl)ethyl]-1H-indol-3-yl](4-methoxyphenyl)methanone |
| Δ9-THC | (-)-Δ9-THC or Dronabinol® |
| NPS | Novel Psychoactive Substances |
| SCs | Synthetic Cannabinoids |
| CNS | Central Nervous System |
| ECG | Electrocardiogram |
| HR | Heart Rate |
| BR | Breath Rate |
References
- United Nations Office on Drugs and Crime (UNODC). The Challenge of New Psychoactive Substances: A Report from the Global SMART Programme: Vienna. 2013. Available online: https://www.unodc.org/documents/scientific/NPS_2013_SMART.pdf (accessed on 6 June 2022).
- Schifano, F.; Napoletano, F.; Chiappini, S.; Guirguis, A.; Corkery, J.M.; Bonaccorso, S.; Ricciardi, A.; Scherbaum, N.; Vento, A. New/emerging psychoactive substances and associated psychopathological consequences. Psychol. Med. 2021, 51, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Luethi, D.; Liechti, M.E. Designer drugs: Mechanism of action and adverse effects. Arch. Toxicol. 2020, 94, 1085–1133. [Google Scholar] [CrossRef] [PubMed]
- Fattore, L.; Fratta, W. Beyond THC: The New Generation of Cannabinoid Designer Drugs. Front. Behav. Neurosci. 2011, 5, 60. [Google Scholar] [CrossRef] [PubMed]
- Zawilska, J.B. “Legal Highs”—An Emerging Epidemic of Novel Psychoactive Substances. Int. Rev. Neurobiol. 2015, 120, 273–300. [Google Scholar] [CrossRef]
- Zimmermann, U.S.; Winkelmann, P.R.; Pilhatsch, M.; Nees, J.A.; Spanagel, R.; Schulz, K. Withdrawal phenomena and dependence syndrome after the consumption of “spice gold”. Dtsch. Arztebl. Int. 2009, 106, 464–467. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Synthetic Cannabinoids in Europe—A Review; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar]
- Giorgetti, A.; Busardò, F.P.; Tittarelli, R.; Auwärter, V.; Giorgetti, R. Post-Mortem Toxicology: A Systematic Review of Death Cases Involving Synthetic Cannabinoid Receptor Agonists. Front. Psychiatry 2020, 11, 464. [Google Scholar] [CrossRef]
- Locatelli, C.A.; Lonati, D.; Petrolini, V.M. New Drugs of Abuse and Cardiovascular Function. In Brain and Heart Dynamics; Springer: Cham, Switzerland, 2020; pp. 843–868. [Google Scholar] [CrossRef]
- Alves, V.L.; Gonçalves, J.L.; Aguiar, J.; Teixeira, H.M.; Câmara, J.S. The synthetic cannabinoids phenomenon: From structure to toxicological properties. A review. Crit. Rev. Toxicol. 2020, 50, 359–382. [Google Scholar] [CrossRef]
- Spaderna, M.; Addy, P.H.; D’Souza, D.C. Spicing things up: Synthetic cannabinoids. Psychopharmacology 2013, 228, 525–540. [Google Scholar] [CrossRef]
- Tait, R.J.; Caldicott, D.; Mountain, D.; Hill, S.L.; Lenton, S.A. Systematic review of adverse events arising from the use of synthetic cannabinoids and their associated treatment. Clin. Toxicol. 2016, 54, 1–13. [Google Scholar] [CrossRef]
- Le Boisselier, R.; Alexandre, J.; Lelong-Boulouard, V.; Debruyne, D. Focus on cannabinoids and synthetic cannabinoids. Clin. Pharmacol. Ther. 2017, 101, 220–229. [Google Scholar] [CrossRef]
- Alexandre, J.; Malheiro, R.; Dias da Silva, D.; Carmo, H.; Carvalho, F.; Silva, J.P. The Synthetic Cannabinoids THJ-2201 and 5F-PB22 Enhance In Vitro CB1 Receptor-Mediated Neuronal Differentiation at Biologically Relevant Concentrations. Int. J. Mol. Sci. 2020, 21, 6277. [Google Scholar] [CrossRef] [PubMed]
- Young, A.C.; Schwarz, E.; Medina, G.; Obafemi, A.; Feng, S.Y.; Kane, C.; Kleinschmidt, K. Cardiotoxicity associated with the synthetic cannabinoid. K9. with laboratory confirmation. Am. J. Emerg. Med. 2012, 30, 1320.e5–1320.e7. [Google Scholar] [CrossRef] [PubMed]
- Hermanns-Clausen, M.; Kneisel, S.; Szabo, B.; Auwärter, V. Acute toxicity due to the confirmed consumption of synthetic cannabinoids: Clinical and laboratory findings. Addiction 2013, 108, 534–544. [Google Scholar] [CrossRef]
- Besli, G.E.; Ikiz, M.A.; Yildirim, S.; Saltik, S. Synthetic Cannabinoid Abuse in Adolescents: A Case Series. J. Emerg. Med. 2015, 49, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Yamanoglu, A.; Celebi Yamanoglu, N.G.; Evran, T.; Sogut, O. How much can synthetic cannabinoid damage the heart? A case of cardiogenic shock following resistant ventricular fibrillation after synthetic cannabinoid use. J. Clin. Ultrasound 2018, 46, 605–609. [Google Scholar] [CrossRef]
- Tse, R.; Kodur, S.; Squires, B.; Collins, N. Sudden cardiac death complicating acute myocardial infarction following synthetic cannabinoid use. Intern. Med. J. 2014, 44, 934–936. [Google Scholar] [CrossRef]
- McIlroy, G.; Ford, L.; Khan, J.M. Acute myocardial infarction. associated with the use of a synthetic adamantyl-cannabinoid: A case report. BMC Pharmacol. Toxicol. 2016, 17, 2. [Google Scholar] [CrossRef]
- Moeller, S.; Lücke, C.; Struffert, T.; Schwarze, B.; Gerner, S.T.; Schwab, S.; Köhrmann, M.; Machold, K.; Philipsen, A.; Müller, H.H. Ischemic stroke associated with the use of a synthetic cannabinoid (spice). Asian J. Psychiatr. 2017, 25, 127–130. [Google Scholar] [CrossRef]
- Alhadi, S.; Tiwari, A.; Vohra, R.; Gerona, R.; Acharya, J.; Bilello, K. High times. low sats: Diffuse pulmonary infiltrates associated with chronic synthetic cannabinoid use. J. Med. Toxicol. 2013, 9, 199–206. [Google Scholar] [CrossRef]
- Alon, M.H.; Saint-Fleur, M.O. Synthetic cannabinoid induced acute respiratory depression: Case series and literature review. Respir. Med. Case Rep. 2017, 22, 137–141. [Google Scholar] [CrossRef]
- Yamanoglu, A.; Cakmak, S.; Celebi Yamanoglu, N.G.; Sogut, O. A new side effect of synthetic cannabinoid use by the bucket (waterpipe) method: Acute respiratory distress syndrome (ARDS). Turk. J. Emerg. Med. 2017, 18, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Banister, S.D.; Wilkinson, S.M.; Longworth, M.; Stuart, J.; Apetz, N.; English, K.; Brooker, L.; Goebel, C.; Hibbs, D.E.; Glass, M.; et al. The synthesis and pharmacological evaluation of adamantane-derived indoles: Cannabimimetic drugs of abuse. ACS Chem. Neurosci. 2013, 4, 1081–1092. [Google Scholar] [CrossRef] [PubMed]
- Banister, S.D.; Stuart, J.; Kevin, R.C.; Edington, A.; Longworth, M.; Wilkinson, S.M.; Beinat, C.; Buchanan, A.S.; Hibbs, D.E.; Glass, M.; et al. Effects of bioisosteric fluorine in synthetic cannabinoid designer drugs JWH-018. AM-2201. UR-144. XLR-11. PB-22. 5F-PB-22. APICA. and STS-135. ACS Chem. Neurosci. 2015, 6, 1445–1458. [Google Scholar] [CrossRef] [PubMed]
- Schmid, K.; Niederhoffer, N.; Szabo, B. Analysis of the respiratory effects of cannabinoids in rats. Naunyn Schmiedebergs Arch. Pharmacol. 2003, 368, 301–308. [Google Scholar] [CrossRef]
- Bilel, S.; Tirri, M.; Arfè, R.; Stopponi, S.; Soverchia, L.; Ciccocioppo, R.; Frisoni, P.; Strano-Rossi, S.; Miliano, C.; De-Giorgio, F.; et al. Pharmacological and Behavioral Effects of the Synthetic Cannabinoid AKB48 in Rats. Front. Neurosci. 2019, 13, 1163. [Google Scholar] [CrossRef]
- Gardiner, S.M.; March, J.E.; Kemp, P.A.; Bennett, T. Regional haemodynamic responses to the cannabinoid agonist. WIN 55212-2. in conscious. normotensive rats. and in hypertensive. transgenic rats. Br. J. Pharmacol. 2001, 133, 445–453. [Google Scholar] [CrossRef]
- Gardiner, S.M.; March, J.E.; Kemp, P.A.; Bennett, T. Influence of the CB(1) receptor antagonist. AM 251. on the regional haemodynamic effects of WIN-55212-2 or HU 210 in conscious rats. Br. J. Pharmacol. 2002, 136, 581–587. [Google Scholar] [CrossRef]
- Schindler, C.W.; Gramling, B.R.; Justinova, Z.; Thorndike, E.B.; Baumann, M.H. Synthetic cannabinoids found in “spice” products alter body temperature and cardiovascular parameters in conscious male rats. Drug Alcohol Depend. 2017, 179, 387–394. [Google Scholar] [CrossRef]
- Steffens, S.; Pacher, P. Targeting cannabinoid receptor CB(2) in cardiovascular disorders: Promises and controversies. Br. J. Pharmacol. 2012, 167, 313–323. [Google Scholar] [CrossRef]
- Tahamtan, A.; Samieipoor, Y.; Nayeri, F.S.; Rahbarimanesh, A.A.; Izadi, A.; Rashidi-Nezhad, A.; Tavakoli-Yaraki, M.; Farahmand, M.; Bont, L.; Shokri, F.; et al. Effects of canna-binoid receptor type 2 in respiratory syncytial virus infection in human subjects and mice. Virulence 2018, 9, 217–230. [Google Scholar] [CrossRef]
- Pertwee, R.G. Receptors and channels targeted by synthetic cannabinoid receptor agonists and antagonists. Curr. Med. Chem. 2010, 17, 1360–1381. [Google Scholar] [CrossRef]
- Richards, J.R. Mechanisms for the Risk of Acute Coronary Syndrome and Arrhythmia Associated With Phytogenic and Synthetic Cannabinoid Use. J. Cardiovasc. Pharmacol. Ther. 2020, 25, 508–522. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, S.E. Endocannabinoids and the Cardiovascular System in Health and Disease. Handb. Exp. Pharmacol. 2015, 231, 393–422. [Google Scholar] [CrossRef] [PubMed]
- Kicman, A.; Pędzińska-Betiuk, A.; Kozłowska, H. The potential of cannabinoids and inhibitors of endocannabinoid degradation in respiratory diseases. Eur. J. Pharmacol. 2021, 911, 174560. [Google Scholar] [CrossRef]
- Fantauzzi, M.F.; Aguiar, J.A.; Tremblay, B.J.; Mansfield, M.J.; Yanagihara, T.; Chandiramohan, A.; Revill, S.; Ryu, M.H.; Carlsten, C.; Ask, K.; et al. Expression of endocannabinoid system components in human airway epithelial cells: Impact of sex and chronic respiratory disease status. ERJ Open Res. 2020, 6, 00128–02020. [Google Scholar] [CrossRef] [PubMed]
- Calignano, A.; Kátona, I.; Désarnaud, F.; Giuffrida, A.; La Rana, G.; Mackie, K.; Freund, T.F.; Piomelli, D. Bidirectional control of airway responsiveness by endogenous cannabinoids. Nature 2000, 408, 96–101. [Google Scholar] [CrossRef]
- Atwood, B.K.; Huffman, J.; Straiker, A.; Mackie, K. JWH018, a common constituent of ‘Spice’ herbal blends, is a potent and efficacious cannabinoid CB receptor agonist. Br. J. Pharmacol. 2010, 160, 585–593. [Google Scholar] [CrossRef]
- Vigolo, A.; Ossato, A.; Trapella, C.; Vincenzi, F.; Rimondo, C.; Seri, C.; Varani, K.; Serpelloni, G.; Marti, M. Novel halogenated derivates of JWH-018: Behavioral and binding studies in mice. Neuropharmacology 2015, 95, 68–82. [Google Scholar] [CrossRef]
- Auwärter, V.; Dresen, S.; Weinmann, W.; Müller, M.; Pütz, M.; Ferreirós, N. ‘Spice’ and other herbal blends: Harmless incense or cannabinoid designer drugs? J. Mass Spectrom. 2009, 44, 832–837. [Google Scholar] [CrossRef]
- Seely, K.A.; Lapoint, J.; Moran, J.H.; Fattore, L. Spice drugs are more than harmless herbal blends: A review of the pharmacology and toxicology of synthetic cannabinoids. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 39, 234–243. [Google Scholar] [CrossRef]
- Gurney, S.M.; Scott, K.S.; Kacinko, S.L.; Presley, B.C.; Logan, B.K. Pharmacology, Toxicology, and Adverse Effects of Synthetic Cannabinoid Drugs. Forensic Sci. Rev. 2014, 26, 53–78. [Google Scholar] [PubMed]
- Lapoint, J.; James, L.P.; Moran, C.L.; Nelson, L.S.; Hoffman, R.S.; Moran, J.H. Severe toxicity following synthetic cannabinoid ingestion. Clin. Toxicol. 2011, 49, 760–764. [Google Scholar] [CrossRef]
- Yeakel, J.K.; Logan, B.K. Blood synthetic cannabinoid concentrations in cases of suspected impaired driving. J. Anal. Toxicol. 2013, 37, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Castaneto, M.S.; Gorelick, D.A.; Desrosiers, N.A.; Hartman, R.L.; Pirard, S.; Huestis, M.A. Synthetic cannabinoids: Epidemiology. pharmacodynamics. and clinical implications. Drug Alcohol Depend. 2014, 144, 12–41. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Steffens, S.; Haskó, G.; Schindler, T.H.; Kunos, G. Cardiovascular effects of marijuana and synthetic cannabinoids: The good. the bad. and the ugly. Nat. Rev. Cardiol. 2018, 15, 151–166. [Google Scholar] [CrossRef] [PubMed]
- Kaschina, E. Cannabinoid CB1/CB2 Receptors in the Heart: Expression, Regulation, and Function. In Cannabinoids in Health and Disease; InTech: Rijeka, Croatia, 2016; pp. 169–185. [Google Scholar] [CrossRef]
- Niederhoffer, N.; Szabo, B. Effect of the cannabinoid receptor agonist WIN55212-2 on sympathetic cardiovascular regulation. Br. J. Pharmacol. 1999, 126, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, H.; Watanabe, S.; Oishi, R.; Ueki, S. Effects of delta-9-tetrahydrocannabinol on the cardiovascular system, and pressor and behavioral responses to brain stimulation in rats. Jpn. J. Pharmacol. 1980, 30, 493–502. [Google Scholar] [CrossRef]
- Vidrio, H.; Sánchez-Salvatori, M.; Medina, M. Cardiovascular Effects of (-)-11-OH-Δ8-Tetrahydrocannabinol-Dimethylheptyl in Rats. J. Cardiovasc. Pharmacol. 1996, 28, 332–336. [Google Scholar] [CrossRef]
- Niederhoffer, N.; Szabo, B. Cannabinoids cause central sympathoexcitation and bradycardia in rabbits. J. Pharmacol. Exp. Ther. 2000, 294, 707–713. [Google Scholar]
- Banister, S.D.; Moir, M.; Stuart, J.; Kevin, R.C.; Wood, K.E.; Longworth, M.; Wilkinson, S.M.; Beinat, C.; Buchanan, A.S.; Glass, M.; et al. Pharmacology of Indole and Indazole Synthetic Cannabinoid Designer Drugs AB-FUBINACA. ADB-FUBINACA. AB-PINACA. ADB-PINACA. 5F-AB-PINACA. 5F-ADB-PINACA. ADBICA. and 5F-ADBICA. ACS Chem. Neurosci. 2015, 6, 1546–1559. [Google Scholar] [CrossRef]
- Banister, S.D.; Longworth, M.; Kevin, R.; Sachdev, S.; Santiago, M.; Stuart, J.; Mack, J.B.; Glass, M.; McGregor, I.S.; Connor, M.; et al. Pharmacology of Valinate and tert-Leucinate Synthetic Cannabinoids 5F-AMBICA. 5F-AMB. 5F-ADB. AMB-FUBINACA. MDMB-FUBINACA. MDMB-CHMICA. and Their Analogues. ACS Chem. Neurosci. 2016, 7, 1241–1254. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, R.R.; Cavero, I.; Ertel, R.J.; Solomon, T.A.; Buckley, J.P. Role of the central autonomic nervous system in the hypotension and bradycardia induced by (-)-delta 9-trans-tetrahydrocannabinol. J. Pharm. Pharmacol. 1974, 26, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.A.C.; Ghuran, A.; Vadamalai, V.; Antonios, T. Cardiovascular complications induced by cannabis smoking: A case report and review of the literature. Emerg. Med. J. 2005, 22, 679–680. [Google Scholar] [CrossRef]
- Korantzopoulos, P.; Liu, T.; Papaioannides, D.; Li, G.; Goudevenos, J.A. Atrial fibrillation and marijuana smoking. Int. J. Clin. Pract. 2008, 62, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Wehrwein, E.A.; Joyner, M.J. Regulation of blood pressure by the arterial baroreflex and autonomic nervous system. Handb. Clin. Neurol. 2013, 117, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Dean, C.; Hillard, C.J.; Seagard, J.L.; Hopp, F.A.; Hogan, Q.H. Components of the cannabinoid system in the dorsal periaqueductal gray are related to resting heart rate. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 311, R254–R262. [Google Scholar] [CrossRef]
- Jones, R.T. Cardiovascular system effects of marijuana. J. Clin. Pharmacol. 2002, 42, 58S–63S. [Google Scholar] [CrossRef] [PubMed]
- Ishac, E.J.; Jiang, L.; Lake, K.D.; Varga, K.; Abood, M.E.; Kunos, G. Inhibition of exocytotic noradrenaline release by presynaptic cannabinoid CB1 receptors on peripheral sympathetic nerves. Br J Pharmacol. 1996, 118, 2023–2028. [Google Scholar] [CrossRef]
- Malinowska, B.; Godlewski, G.; Bucher, B.; Schlicker, E. Cannabinoid CB1 receptor-mediated inhibition of the neurogenic vasopressor response in the pithed rat. Naunyn Schmiedebergs Arch. Pharmacol. 1997, 356, 197–202. [Google Scholar] [CrossRef]
- Pertwee, R.G.; Joe-Adigwe, G.; Hawksworth, G.M. Further evidence for the presence of cannabinoid CB1 receptors in mouse vas deferens. Eur. J. Pharmacol. 1996, 296, 169–172. [Google Scholar] [CrossRef]
- Li, Q.; Ma, H.J.; Zhang, H.; Qi, Z.; Guan, Y.; Zhang, Y. Electrophysiological effects of anandamide on rat myocardium. Br. J. Pharmacol. 2009, 158, 2022–2029. [Google Scholar] [CrossRef] [PubMed]
- Akins, D.; Awdeh, M.R. Marijuana and second-degree AV block. South Med. J. 1981, 74, 371–373. [Google Scholar] [CrossRef]
- Sattout, A.H.; Nicol, M.F. Cardiac arrest following cannabis use: A case report. Cases J. 2009, 2, 208. [Google Scholar] [CrossRef] [PubMed]
- Casier, I.; Vanduynhoven, P.; Haine, S.; Vrints, C.; Jorens, P.G. Is recent cannabis use associated with acute coronary syndromes? An illustrative case series. Acta Cardiol. 2014, 69, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Atik, S.U.; Dedeoğlu, R.; Varol, F.; Çam, H.; Eroğlu, A.G.; Saltık, L. Cardiovascular side effects related with use of synthetic cannabinoids “bonzai”: Two case reports. Turk. Pediatr. Ars. 2015, 50, 61–64. [Google Scholar] [CrossRef]
- Von Der Haar, J.; Talebi, S.; Ghobadi, F.; Singh, S.; Chirurgi, R.; Rajeswari, P.; Kalantari, H.; Hassen, G.W. Synthetic Cannabinoids and Their Effects on the Cardiovascular System. J. Emerg. Med. 2016, 50, 258–262. [Google Scholar] [CrossRef]
- Krylatov, A.V.; Maslov, L.N.; Lasukova, O.V.; Pertwee, R.G. Cannabinoid receptor antagonists SR141716 and SR144528 exhibit properties of partial agonists in experiments on isolated perfused rat heart. Bull. Exp. Biol. Med. 2005, 139, 558–561. [Google Scholar] [CrossRef]
- Zaccolo, M. cAMP signal transduction in the heart: Understanding spatial control for the development of novel therapeutic strategies. Br. J. Pharmacol. 2009, 158, 50–60. [Google Scholar] [CrossRef]
- Wang, P.F.; Jiang, L.S.; Bu, J.; Huang, X.J.; Song, W.; Du, Y.P.; He, B. Cannabinoid-2 receptor activation protects against infarct and ischemia-reperfusion heart injury. J. Cardiovasc. Pharmacol. 2012, 59, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Randall, M.D.; Harris, D.; Kendall, D.A.; Ralevic, V. Cardiovascular effects of cannabinoids. Pharmacol. Ther. 2002, 95, 191–202. [Google Scholar] [CrossRef]
- Ho, W.S.; Gardiner, S.M. Acute hypertension reveals depressor and vasodilator effects of cannabinoids in conscious rats. Br. J. Pharmacol. 2009, 156, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Rudź, R.; Schlicker, E.; Baranowska, U.; Marciniak, J.; Karabowicz, P.; Malinowska, B. Acute myocardial infarction inhibits the neurogenic tachycardic and vasopressor response in rats via presynaptic cannabinoid type 1 receptor. J. Pharmacol. Exp. Ther. 2012, 343, 198–205. [Google Scholar] [CrossRef]
- Ralevic, V.; Kendall, D.A. Cannabinoid modulation of perivascular sympathetic and sensory neurotransmission. Curr. Vasc. Pharmacol. 2009, 7, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Dean, C. Cannabinoid and GABA modulation of sympathetic nerve activity and blood pressure in the dorsal periaqueductal gray of the rat. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 301, R1765–R1772. [Google Scholar] [CrossRef] [PubMed]
- Stanley, C.; O’Sullivan, S.E. Vascular targets for cannabinoids: Animal and human studies. Br. J. Pharmacol. 2014, 171, 1361–1378. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.S.V.; Kelly, M.E.M. Cannabinoids in the cardiovascular system. Adv. Pharm. 2017, 8, 329–366. [Google Scholar] [CrossRef]
- Hanus, L.; Breuer, A.; Tchilibon, S.; Shiloah, S.; Goldenberg, D.; Horowitz, M.; Pertwee, R.G.; Ross, R.A.; Mechoulam, R.; Fride, E. HU-308: A specific agonist for CB(2), a peripheral cannabinoid receptor. Proc. Natl. Acad. Sci. USA 1999, 96, 14228–14233. [Google Scholar] [CrossRef]
- Miller, R.H.; Dhingra, R.C.; Kanakis, C., Jr.; Amat-y-Leon, F.; Rose, K.M. The electrophysiological effects of delta-9-tetrahydrocannabinol (cannabis) on cardiac conduction in man. Am. Heart J. 1977, 94, 740–747. [Google Scholar] [CrossRef]
- Rattanawong, P.; Kewcharoen, J.; Techorueangwiwat, C.; Kanitsoraphan, C.; Mekritthikrai, R.; Prasitlumkum, N.; Puttapiban, P.; Mekraksakit, P.; Vutthikraivit, W.; Sorajja, D. Wide QRS complex and the risk of major arrhythmic events in Brugada syndrome patients: A systematic review and meta-analysis. J. Arrhythm. 2019, 36, 143–152. [Google Scholar] [CrossRef]
- Kariyanna, P.T.; Jayarangaiah, A.; Hegde, S.; Marmur, J.D.; Wengrofsky, P.; Yacoub, M.; Post, M.; McFarlane, S.I. Marijuana Induced Type I Brugada Pattern: A Case Report. Am. J. Med. Case Rep. 2018, 6, 134–136. [Google Scholar] [CrossRef]
- Antzelevitch, C.; Yan, G.X. J wave syndromes. Heart Rhythm 2010, 7, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Topçu, H.; Aksan, G.; Karakuş Yılmaz, B.; Tezcan, M.; Sığırcı, S. Osborn wave and new-onset atrial fibrillation related to hypothermia after synthetic cannabis (bonsai) abuse. Turk. Kardiyol. Dern. Ars. 2019, 47, 315–318. [Google Scholar] [CrossRef]
- Ossato, A.; Vigolo, A.; Trapella, C.; Seri, C.; Rimondo, C.; Serpelloni, G.; Marti, M. JWH-018 impairs sensorimotor functions in mice. Neuroscience 2015, 300, 174–188. [Google Scholar] [CrossRef]
- Canazza, I.; Ossato, A.; Trapella, C.; Fantinati, A.; De Luca, M.A.; Margiani, G.; Vincenzi, F.; Rimondo, C.; Di Rosa, F.; Gregori, A.; et al. Effect of the novel synthetic cannabinoids AKB48 and 5F-AKB48 on “tetrad”. sensorimotor. neurological and neurochemical responses in mice. In vitro and in vivo pharmacological studies. Psychopharmacology 2016, 233, 3685–3709. [Google Scholar] [CrossRef]
- Bilel, S.; Tirri, M.; Arfè, R.; Ossato, A.; Trapella, C.; Serpelloni, G.; Neri, M.; Fattore, L.; Marti, M. Novel halogenated synthetic cannabinoids impair sensorimotor functions in mice. Neurotoxicology 2020, 76, 17–32. [Google Scholar] [CrossRef]
- Yun, J.; Yoon, K.S.; Lee, T.H.; Lee, H.; Gu, S.M.; Song, Y.J.; Cha, H.J.; Han, K.M.; Seo, H.; Shin, J.; et al. Synthetic cannabinoid, JWH-030, induces QT prolongation through hERG channel inhibition. Toxicol. Res. 2016, 5, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.M.; Kupershmidt, S. From genes to channels: Normal mechanisms. Cardiovasc. Res. 1999, 42, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, M.A.; Bolaños, R.; Gonzalez, C.D.; Di Girolamo, G. QT interval prolongation: Preclinical and clinical testing arrhythmogenesis in drugs and regulatory implications. Curr. Drug Saf. 2010, 5, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D. Torsades de Pointes. Confed. Aust. Crit. Care Nurses J. 1990, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Khan, A.; See, V.Y.; Robinson, S. Cardiac arrest associated with synthetic cannabinoid use and acquired prolonged QTc interval: A case report and review of literature. Heart Rhythm Case Rep. 2020, 6, 283–286. [Google Scholar] [CrossRef]
- Schumacher, K.; Büttner, P.; Dagres, N.; Sommer, P.; Dinov, B.; Hindricks, G.; Bollmann, A.; Kornej, J. Association between PR interval prolongation and electro-anatomical substrate in patients with atrial fibrillation. PLoS ONE 2018, 13, e0206933. [Google Scholar] [CrossRef] [PubMed]
- Efe, T.H.; Felekoglu, M.A.; Çimen, T.; Doğan, M. Atrial fibrillation following synthetic cannabinoid abuse. Turk. Kardiyol. Dern. Ars. 2017, 45, 362–364. [Google Scholar] [CrossRef] [PubMed]
- Coumel, P. Paroxysmal atrial fibrillation: A disorder of autonomic tone? Eur. Heart J. 1994, 15 (Suppl. A), 9–16. [Google Scholar] [CrossRef]
- Dimmer, C.; Tavernier, R.; Gjorgov, N.; Van Nooten, G.; Clement, D.L.; Jordaens, L. Variations of autonomic tone preceding onset of atrial fibrillation after coronary artery bypass grafting. Am. J. Cardiol. 1998, 82, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Amar, D.; Zhang, H.; Miodownik, S.; Kadish, A.H. Competing autonomic mechanisms precede the onset of postoperative atrial fibrillation. J. Am. Coll. Cardiol. 2003, 42, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.J.; Zipes, D.P. Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ. Res. 2014, 114, 1004–1021. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, A.; Frontera, A.; Bond, R.; Duncan, E.; Thomas, G. Vagal atrial fibrillation: What is it and should we treat it? Int. J. Cardiol. 2015, 201, 415–421. [Google Scholar] [CrossRef]
- Wijffels, M.C.; Kirchhof, C.J.; Dorland, R.; Allessie, M.A. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation 1995, 92, 1954–1968. [Google Scholar] [CrossRef]
- Bers, D.M. Cardiac excitation-contraction coupling. Nature 2002, 415, 198–205. [Google Scholar] [CrossRef]
- Patterson, E.; Lazzara, R.; Szabo, B.; Liu, H.; Tang, D.; Li, Y.H.; Scherlag, B.J.; Po, S.S. Sodium-calcium exchange initiated by the Ca2+ transient: An arrhythmia trigger within pulmonary veins. J. Am. Coll. Cardiol. 2006, 47, 1196–1206. [Google Scholar] [CrossRef]
- Nerbonne, J.M.; Kass, R.S. Molecular physiology of cardiac repolarization. Physiol. Rev. 2005, 85, 1205–1253. [Google Scholar] [CrossRef] [PubMed]
- Yahud, E.; Paul, G.; Rahkovich, M.; Vasilenko, L.; Kogan, Y.; Lev, E.; Laish-Farkash, A. Cannabis induced cardiac arrhythmias: A case series. Eur. Heart J. Case Rep. 2020, 4, 1–9. [Google Scholar] [CrossRef]
- Gagnon, L.R.; Sadasivan, C.; Perera, K.; Oudit, G.Y. Cardiac Complications of Common Drugs of Abuse: Pharmacology, Toxicology, and Management. Can. J. Cardiol. 2022, 38, 1331–1341. [Google Scholar] [CrossRef] [PubMed]
- Adami, P.E.; Koutlianos, N.; Baggish, A.; Bermon, S.; Cavarretta, E.; Deligiannis, A.; Furlanello, F.; Kouidi, E.; Marques-Vidal, P.; Niebauer, J.; et al. Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: A position statement of the sport cardiology and exercise nucleus of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 559–575. [Google Scholar] [CrossRef] [PubMed]
- Barana, A.; Amorós, I.; Caballero, R.; Gómez, R.; Osuna, L.; Lillo, M.P.; Blázquez, C.; Guzmán, M.; Delpón, E.; Tamargo, J. Endocannabinoids and cannabinoid analogues block cardiac hKv1.5 channels in a cannabinoid receptor-independent manner. Cardiovasc. Res. 2010, 85, 56–67. [Google Scholar] [CrossRef]
- Al Kury, L.T.; Voitychuk, O.I.; Yang, K.H.; Thayyullathil, F.T.; Doroshenko, P.; Ramez, A.M.; Shuba, Y.M.; Galadari, S.; Howarth, F.C.; Oz, M. Effects of the endogenous cannabinoid anandamide on voltage-dependent sodium and calcium channels in rat ventricular myocytes. Br. J. Pharmacol. 2014, 171, 3485–3498. [Google Scholar] [CrossRef]
- Bondarenko, A.; Waldeck-Weiermair, M.; Naghdi, S.; Poteser, M.; Malli, R.; Graier, W.F. GPR55-dependent and -independent ion signalling in response to lysophosphatidylinositol in endothelial cells. Br. J. Pharmacol. 2010, 161, 308–320. [Google Scholar] [CrossRef]
- Robertson-Gray, O.J.; Walsh, S.K.; Ryberg, E.; Jönsson-Rylander, A.C.; Lipina, C.; Wainwright, C.L. l-α-Lysophosphatidylinositol (LPI) aggravates myocardial ischemia/reperfusion injury via a GPR55/ROCK-dependent pathway. Pharmacol. Res. Perspect. 2019, 7, e00487. [Google Scholar] [CrossRef]
- Kark, T.; Bagi, Z.; Lizanecz, E.; Pásztor, E.T.; Erdei, N.; Czikora, A.; Papp, Z.; Edes, I.; Pórszász, R.; Tóth, A. Tissue-specific regulation of microvascular diameter: Opposite functional roles of neuronal and smooth muscle located vanilloid receptor-1. Mol. Pharmacol. 2008, 73, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Abd Alla, J.; Graemer, M.; Fu, X.; Quitterer, U. Inhibition of G-protein-coupled Receptor Kinase 2 Prevents the Dysfunctional Cardiac Substrate Metabolism in Fatty Acid Synthase Transgenic Mice. J. Biol. Chem. 2016, 291, 2583–2600. [Google Scholar] [CrossRef]
- Muller, C.; Morales, P.; Reggio, P.H. Cannabinoid Ligands Targeting TRP Channels. Front. Mol. Neurosci. 2019, 11, 487. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.N.; Turk, R.F.; Forney, R.B. Acute toxicity of delta-9-tetrahydrocannabinol in rats and mice. Proc. Soc. Exp. Biol. Med. 1971, 136, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.D.; Li, D.M. Cardiovascular and respiratory effects of cannabis in cat and rat. Br. J. Pharmacol. 1973, 49, 1–10. [Google Scholar] [CrossRef]
- Pfitzer, T.; Niederhoffer, N.; Szabo, B. Central effects of the cannabinoid receptor agonist WIN55212-2 on respiratory and cardiovascular regulation in anaesthetised rats. Br. J. Pharmacol. 2004, 142, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Moss, I.R.; Friedman, E. Delta9-tetrahydrocannabinol: Depression of ventilatory regulation; other respiratory and cardiovascular effects. Life Sci. 1976, 19, 99–104. [Google Scholar] [CrossRef]
- Doherty, P.A.; McCarthy, L.E.; Borison, H.L. Respiratory and cardiovascular depressant effects of nabilone. N-methyllevonantradol and delta 9-tetrahydrocannabinol in anesthetized cats. J. Pharmacol. Exp. Ther. 1983, 227, 508–516. [Google Scholar]
- Mendizabal-Zubiaga, J.; Melser, S.; Bénard, G.; Ramos, A.; Reguero, L.; Arrabal, S.; Elezgarai, I.; Gerrikagoitia, I.; Suarez, J.; Rodríguez De Fonseca, F.; et al. Cannabinoid CB1 Receptors Are Localized in Striated Muscle Mitochondria and Regulate Mitochondrial Respiration. Front. Physiol. 2016, 7, 476. [Google Scholar] [CrossRef]
- Simard, M.; Rakotoarivelo, V.; Di Marzo, V.; Flamand, N. Expression and Functions of the CB2 Receptor in Human Leukocytes. Front. Pharmacol. 2022, 13, 826400. [Google Scholar] [CrossRef]
- Bozkurt, T.E. Endocannabinoid System in the Airways. Molecules 2019, 24, 4626. [Google Scholar] [CrossRef]
- Frei, R.B.; Luschnig, P.; Parzmair, G.P.; Peinhaupt, M.; Schranz, S.; Fauland, A.; Wheelock, C.E.; Heinemann, A.; Sturm, E.M. Cannabinoid receptor 2 augments eosinophil responsiveness and aggravates allergen-induced pulmonary inflammation in mice. Allergy 2016, 71, 944–956. [Google Scholar] [CrossRef]
- Ossato, A.; Bilel, S.; Gregori, A.; Talarico, A.; Trapella, C.; Gaudio, R.M.; De-Giorgio, F.; Tagliaro, F.; Neri, M.; Fattore, L.; et al. Neurological. sensorimotor and cardiorespiratory alterations induced by methoxetamine. ketamine and phencyclidine in mice. Neuropharmacology 2018, 141, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Foti, F.; Marti, M.; Ossato, A.; Bilel, S.; Sangiorgi, E.; Botrè, F.; Cerbelli, B.; Baldi, A.; De-Giorgio, F. Phenotypic effects of chronic and acute use of methiopropamine in a mouse model. Int. J. Leg. Med. 2019, 133, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Bilel, S.; Tirri, M.; Arfè, R.; Sturaro, C.; Fantinati, A.; Cristofori, V.; Bernardi, T.; Boccuto, F.; Cavallo, M.; Cavalli, A.; et al. In Vitro and In Vivo Pharmaco-Toxicological Characterization of 1-Cyclohexyl-x-methoxybenzene Derivatives in Mice: Comparison with Tramadol and PCP. Int. J. Mol. Sci. 2021, 22, 7659. [Google Scholar] [CrossRef]
- Bilel, S.; Azevedo Neto, J.; Arfè, R.; Tirri, M.; Gaudio, R.M.; Fantinati, A.; Bernardi, T.; Boccuto, F.; Marchetti, B.; Corli, G.; et al. In vitro and in vivo pharmaco-dynamic study of the novel fentanyl derivatives: Acrylfentanyl. Ocfentanyl and Furanylfentanyl. Neuropharmacology 2022, 209, 109020. [Google Scholar] [CrossRef] [PubMed]
- Emeka, P.; Al-Ahmed, A. Effect of metformin on ECG. HR and BP of rats administered with cardiotoxic agent doxorubicin. Int. J. Basic Clin. Pharmacol. 2017, 6, 1054–1059. [Google Scholar] [CrossRef]
- Balmus, G.; Larrieu, D.; Barros, A.C.; Collins, C.; Abrudan, M.; Demir, M.; Geisler, N.J.; Lelliott, C.J.; White, J.K.; Karp, N.A.; et al. Targeting of NAT10 enhances healthspan in a mouse model of human accelerated aging syndrome. Nat. Commun. 2018, 9, 1700. [Google Scholar] [CrossRef]
- Fridericia, L.S. The duration of systole in an electrocardiogram in normal humans and in patients with heart disease. 1920. Ann. Noninvasive Electrocardiol. 2003, 8, 343–351. [Google Scholar] [CrossRef]
- Richig, W.J.M.; Sleeper, M. Electrocardiography of Laboratory Animals; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Showalter, V.M.; Compton, D.R.; Martin, B.R.; Abood, M.E. Evaluation of binding in a transfected cell line expressing a peripheral cannabinoid receptor (CB2): Identification of cannabinoid receptor subtype-selective ligands. J. Pharmacol. Exp. Ther. 1996, 278, 989–999. [Google Scholar]
- Stout, S.M.; Cimino, N.M. Exogenous cannabinoids as substrates. inhibitors. and inducers of human drug metabolizing enzymes: A systematic review. Drug Metab. Rev. 2014, 46, 86–95. [Google Scholar] [CrossRef]
- Tettey, J.N.A.; Crean, C.; Rodrigues, J.; Angeline Yap, T.W.; Lee, W.; Lim, J.; Shirley Lee, H.Z.; Ching, M. United Nations Office on Drugs and Crime: Recommended methods for the Identification and Analysis of Synthetic Cannabinoid Receptor Agonists in Seized Materials. Forensic Sci. Int. Synerg. 2021, 3, 100129. [Google Scholar] [CrossRef]
- Reagan-Shaw, S.; Nihal, M.; Ahmad, N. Dose translation from animal to human studies revisited. FASEB J. 2008, 22, 659–661. [Google Scholar] [CrossRef] [PubMed]
- Psychonautwiki JWH-018. Available online: https://psychonautwiki.org/wiki/JWH-018 (accessed on 23 November 2021).
- Erowid Experience Vaults JWH-018. Available online: https://erowid.org/experiences/exp.php?ID=76242 (accessed on 23 November 2021).
- Cooper, Z.D. Adverse Effects of Synthetic Cannabinoids: Management of Acute Toxicity and Withdrawal. Curr. Psychiatry Rep. 2016, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Kourouni, I.; Mourad, B.; Khouli, H.; Shapiro, J.M.; Mathew, J.P. Critical Illness Secondary to Synthetic Cannabinoid Ingestion. JAMA Netw. Open 2020, 3, e208516. [Google Scholar] [CrossRef] [PubMed]
- Dal Santo, F.; Velasco, Á.; De la Fuente-Tomás, L.; González-Blanco, L.; Rodríguez-Revuelta, J. Detection of synthetic cannabinoid intoxication in the Emergency Department: When routine toxicological tests are not enough. Adicciones 2019, 31, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Takakuwa, K.M.; Schears, R.M. The emergency department care of the cannabis and synthetic cannabinoid patient: A narrative review. Int. J. Emerg. Med. 2021, 14, 10. [Google Scholar] [CrossRef]
- Kanakis, C., Jr.; Pouget, J.M.; Rosen, K.M. The effects of delta-9-tetrahydrocannabinol (cannabis) on cardiac performance with and without beta blockade. Circulation 1976, 53, 703–707. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ECG Parameters | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vehicle of JWH-018 | Vehicle of ∆9-THC | ||||||||||||
| HR | RR | PR | QRS | QT | QTcF | HR | RR | PR | QRS | QT | QTcF | ||
| Basal | 681.61 ± 4.40 | 88.43 ± 0.58 | 21.07 ± 2.98 | 9.78 ± 0.32 | 25.27 ± 0.97 | 61.38 ±3.45 | Basal | 708.92 ± 1.51 | 85.77 ± 0.94 | 21.26 ± 2.47 | 9.32 ± 0.31 | 24.57 ± 0.78 | 55.94 ± 1.81 |
| a’ | 680.47 ± 3.55 | 88.55 ± 0.46 | 21.87 ± 2.96 | 9.03 + 0.30 | 25.62 ± 0.79 | 60.62 ± 2.94 | a’ | 709.92 ± 1.97 | 85.60 ± 0.91 | 21.40 ± 2.51 | 9.50 ± 0.33 | 25.05 ± 0.34 | 57.18 ± 1.94 |
| b’ | 615.63 ± 4.05 *** | 97.89 ± 0.62 *** | 21.48 ± 2.62 | 9.09 ± 0.36 | 25.14 ± 0.79 | 61.57 ± 2.48 | b’ | 645.22 ± 2.98 *** | 93.56 ± 0.92 *** | 21.50 ± 3.14 | 9.41 ± 0.36 | 24.44 ± 1.01 | 56.67 ± 2.45 |
| JWH-018 6 mg/kg | ∆9-THC 6 mg/kg | ||||||||||||
| Basal | 653.36 ± 4.50 | 92.14 ± 0.61 | 18.06 ± 1.16 | 9.71 ± 0.09 | 24.73 ± 0.23 | 54.86 ± 0.57 | Basal | 689.52 ± 7.04 | 87.84 ± 0.95 | 21.66 ± 0.65 | 9.34 ± 0.24 | 25.07 ± 0.42 | 56.72 ± 2.57 |
| a | 346.43 ± 12.21 *** | 181.50 ± 4.77 *** | 18.84 ± 0.97 | 10.12 ± 0.17 *** | 27.16 ± 0.42 *** | 48.38 ± 1.36 *** | a | 604.98 ± 7.48 *** | 96.30 ± 1.67 *** | 21.98 ± 0.54 | 9.56 ± 0.21 * | 25.32 ± 0.41 | 55.13 ± 2.49 |
| b | 759.82 ± 4.10 *** | 79.02 ± 4.50 *** | 24.37 ± 0.89 *** | 9.79 ± 0.16 | 25.33 ± 0.39 *** | 58.63 ± 1.30 *** | b | 540.87 ± 6.33 *** | 112.28 ± 0.95 *** | 22.09 ± 0.40 * | 9.62 ± 0.23 ** | 25.38 ± 0.45 | 54.81 ± 2.31 |
| Plethysmography Parameters | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Vehicle of JWH-018 | Vehicle of ∆9-THC | ||||||||||
| fr_ie | BB_ie | TV | exp/insp_V ratio__aver | RT | fr_ie | BB_ie | TV | exp/insp_V ratio__aver | RT | ||
| Basal | 230.83 ± 1.99 | 261.01 ± 2.77 | 0.15 ± 0.01 | 0.07 ± 1.15 | 116.79 ± 3.10 | Basal | 270.59 ± 3.41 | 223.62 ± 2.97 | 0.17 ± 0.01 | −0.05 ± 0.78 | 83.73 ± 1.40 |
| a’ | 201.47 ± 2.54 *** | 299.94 ± 4.01 *** | 0.15 ± 0.01 | 0.09 ± 0.79 | 117.90 ± 1.93 | a’ | 268.57 ± 3.70 | 225.36 ± 2.17 | 0.18 ± 0.01 | −0.08 ± 0.97 | 84.55 ± 1.79 |
| b’ | 230.48 ± 5.56 | 263.55 ± 5.51 | 0.16 ± 0.01 | −0.04 ± 0.97 | 114.70 ± 2.94 | ||||||
| JWH-018 6 mg/kg | ∆9-THC 6 mg/kg | ||||||||||
| Basal | 249.51 ± 5.51 | 243.64 ± 4.56 | 0.13 ± 0.003 | 0.06 ± 1.11 | 107.19 ± 4.36 | Basal | 256.09 ± 2.63 | 239.25 ± 3.83 | 0.18 ± 0.01 | −0.038 ± 0.63 | 93.65 ± 3.26 |
| a | 138.98 ± 2.07 *** | 433.77 ± 8.03 *** | 0.11 ± 0.002 *** | −0.07 ± 0.97 | 170.28 ± 9.02 *** | a | 219.31 ± 2.39 *** | 276.23 ± 2.78 *** | 0.18 ± 0.002 | 0.02 ± 0.69 | 114.08 ± 2.44 *** |
| b | 170.96 ± 2.76 *** | 353.61 ± 6.39 ** | 0.12 ± 0.002 *** | −0.07 ± 2.42 | 161.15 ± 6.35 *** | b | 178.49 ± 2.07 *** | 341.73 ± 4.37 *** | 0.17 ± 0.002 ** | 0.07 ± 0.92 | 131.05 ± 4.69 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchetti, B.; Bilel, S.; Tirri, M.; Arfè, R.; Corli, G.; Roda, E.; Locatelli, C.A.; Cavarretta, E.; De Giorgio, F.; Marti, M. The Old and the New: Cardiovascular and Respiratory Alterations Induced by Acute JWH-018 Administration Compared to Δ9-THC—A Preclinical Study in Mice. Int. J. Mol. Sci. 2023, 24, 1631. https://doi.org/10.3390/ijms24021631
Marchetti B, Bilel S, Tirri M, Arfè R, Corli G, Roda E, Locatelli CA, Cavarretta E, De Giorgio F, Marti M. The Old and the New: Cardiovascular and Respiratory Alterations Induced by Acute JWH-018 Administration Compared to Δ9-THC—A Preclinical Study in Mice. International Journal of Molecular Sciences. 2023; 24(2):1631. https://doi.org/10.3390/ijms24021631
Chicago/Turabian StyleMarchetti, Beatrice, Sabrine Bilel, Micaela Tirri, Raffaella Arfè, Giorgia Corli, Elisa Roda, Carlo Alessandro Locatelli, Elena Cavarretta, Fabio De Giorgio, and Matteo Marti. 2023. "The Old and the New: Cardiovascular and Respiratory Alterations Induced by Acute JWH-018 Administration Compared to Δ9-THC—A Preclinical Study in Mice" International Journal of Molecular Sciences 24, no. 2: 1631. https://doi.org/10.3390/ijms24021631
APA StyleMarchetti, B., Bilel, S., Tirri, M., Arfè, R., Corli, G., Roda, E., Locatelli, C. A., Cavarretta, E., De Giorgio, F., & Marti, M. (2023). The Old and the New: Cardiovascular and Respiratory Alterations Induced by Acute JWH-018 Administration Compared to Δ9-THC—A Preclinical Study in Mice. International Journal of Molecular Sciences, 24(2), 1631. https://doi.org/10.3390/ijms24021631