
Pulsed Electromagnetic Field (PEMF) Treatment Ameliorates Murine Model of Collagen-Induced Arthritis

 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
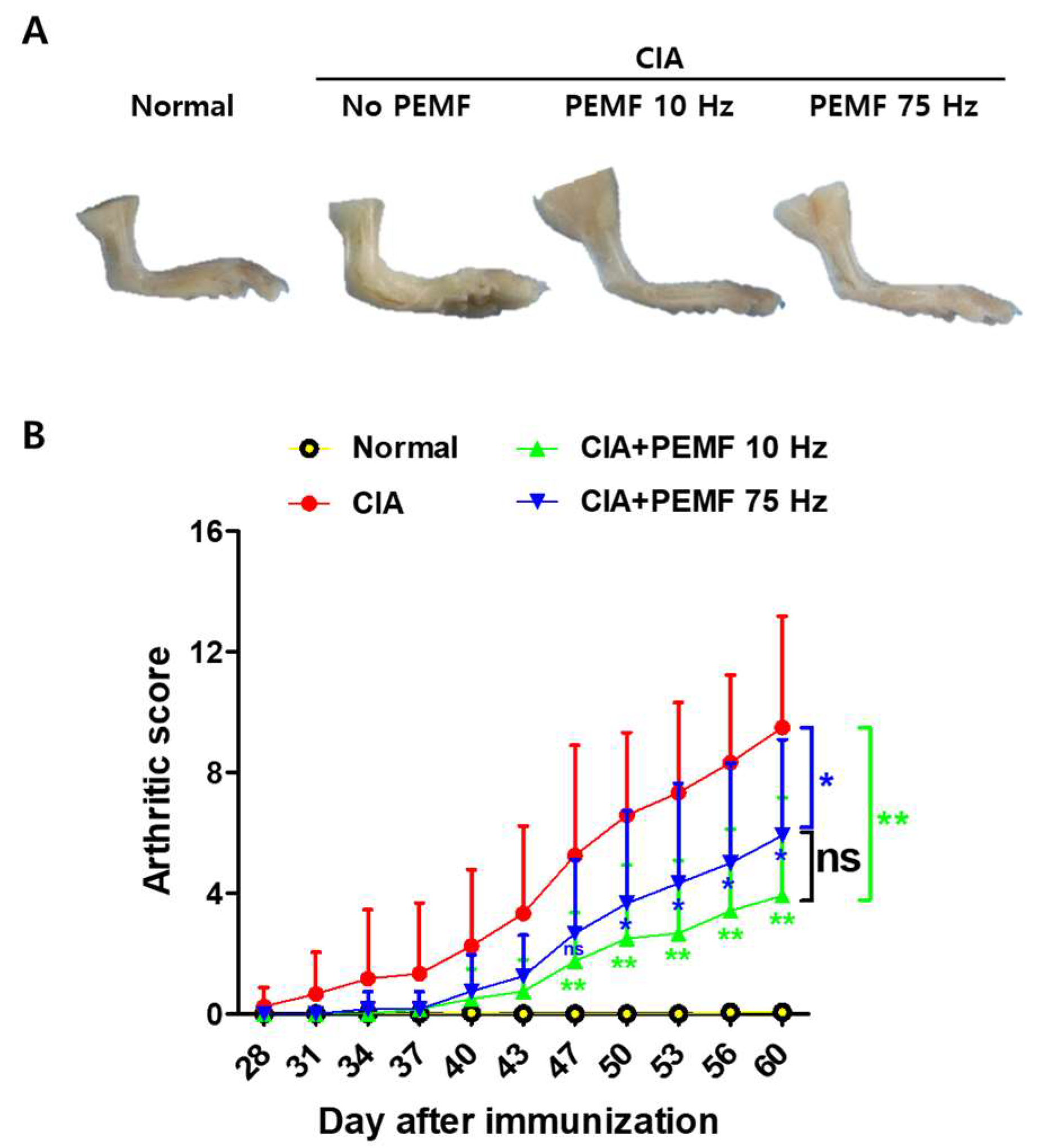
2.1. PEMF Ameliorates CIA in Mice
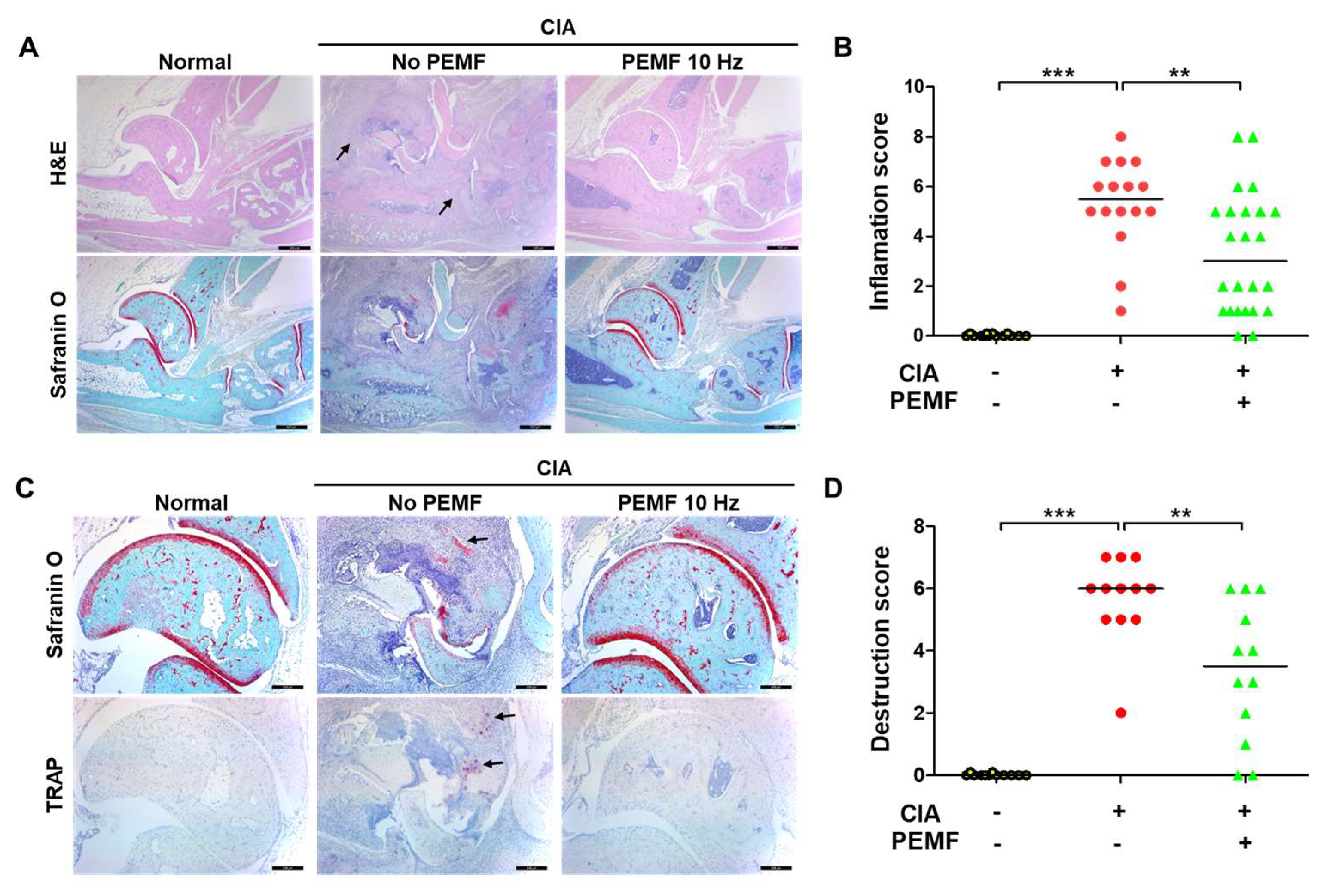
2.2. PEMF Reduces Articular Inflammation and Erosion
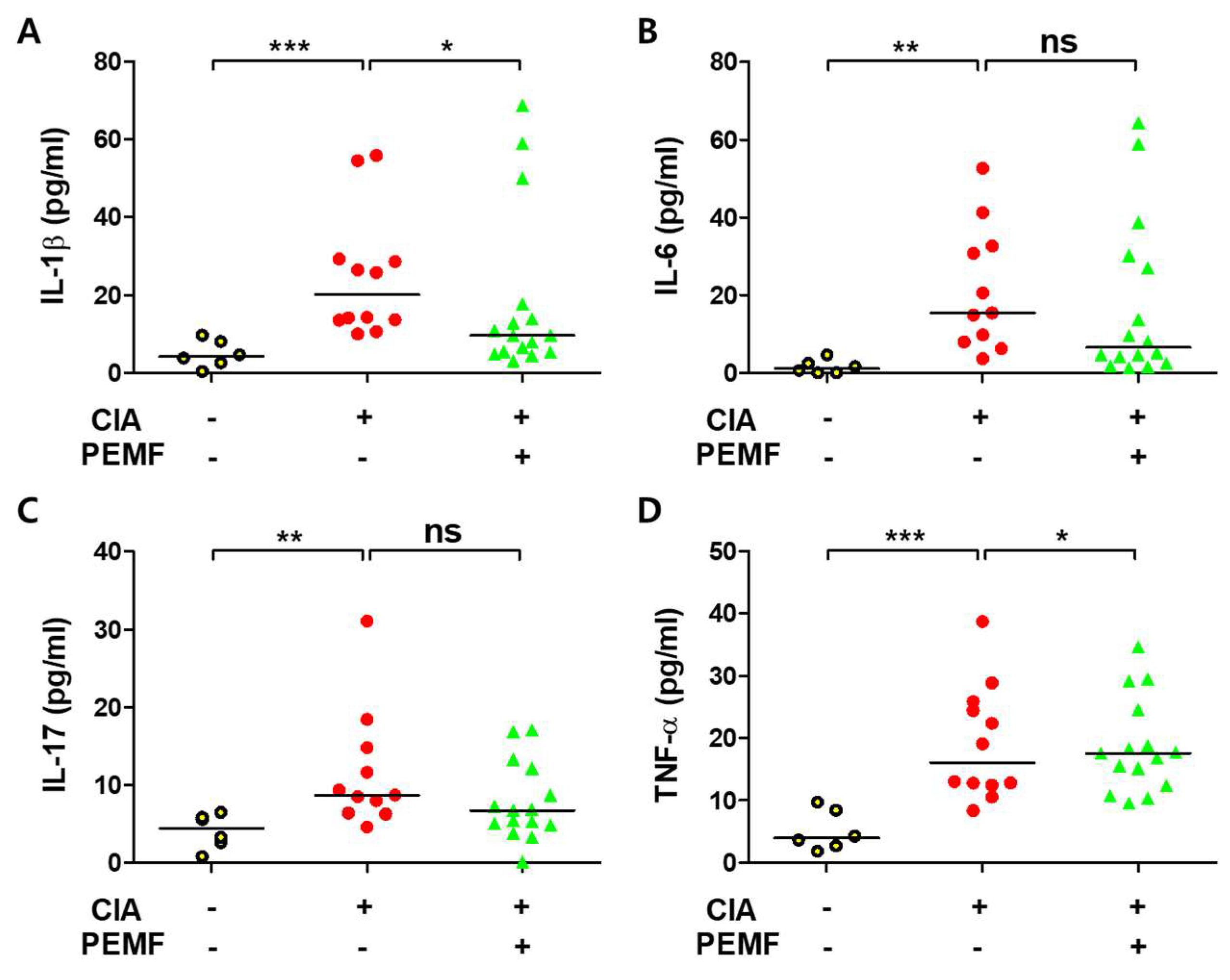
2.3. PEMF Does Not Decrease Serum Proinflammatory Cytokines
2.4. PEMF Does Not Inhibit Autoantibody Formation in CIA Mice
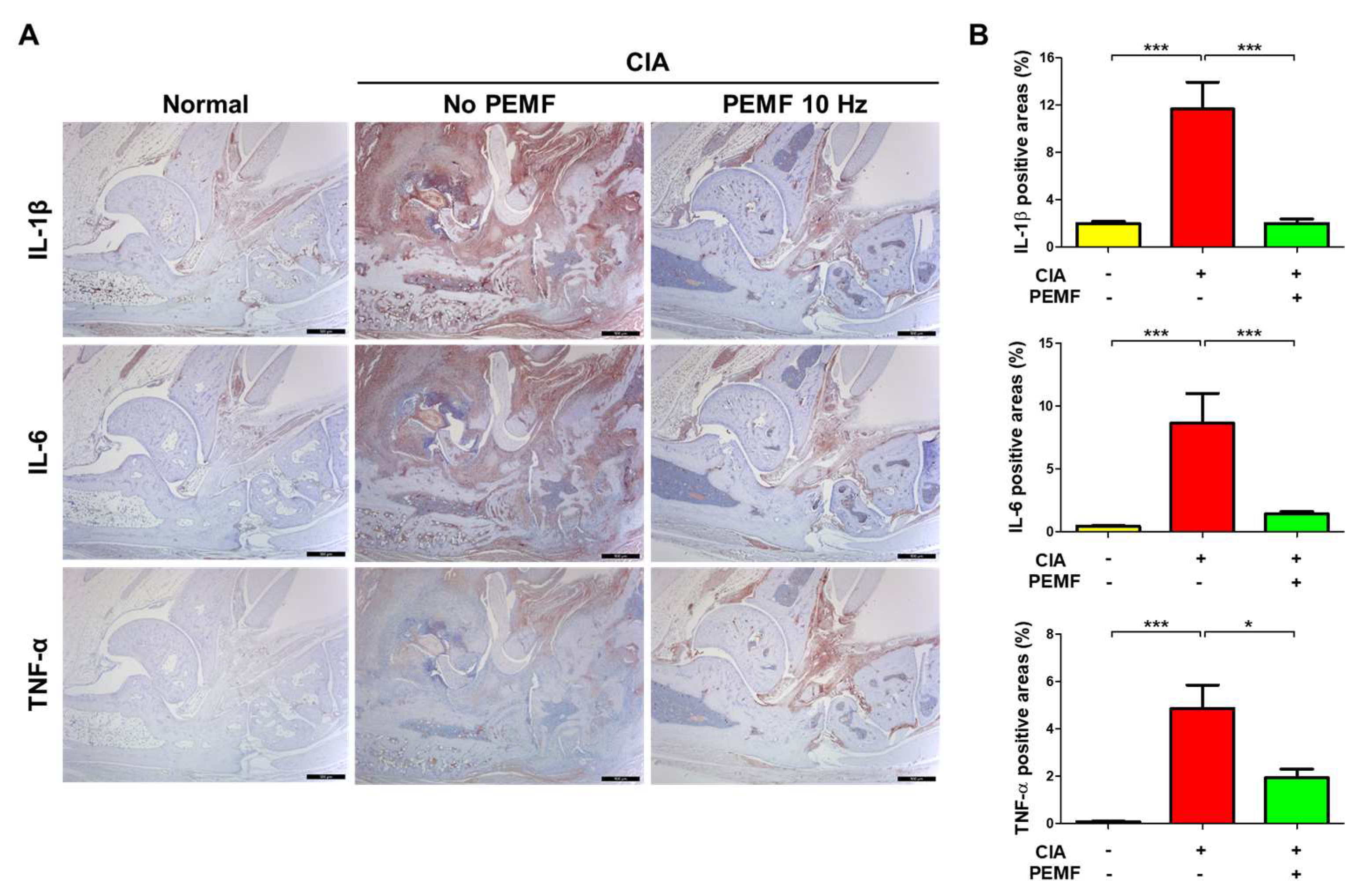
2.5. PEMF Decreases Proinflammatory Cytokines in Ankle Joint Tissues
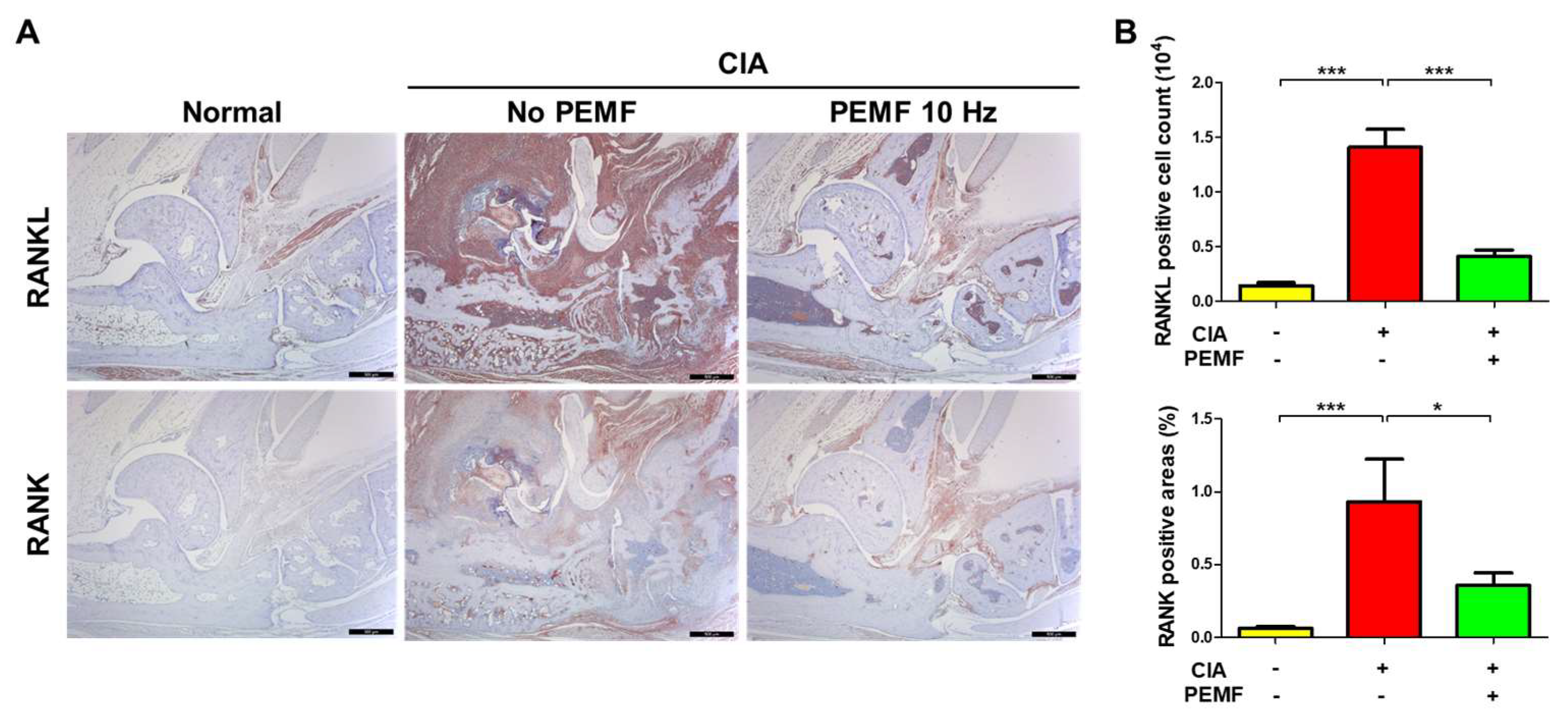
2.6. PEMF Reduces RANKL and RANK Levels in Ankle Joint Tissues
2.7. PEMF Reduces IL-6R and TNFR1 Levels in Ankle Joint Tissues
3. Discussion
4. Materials and Methods
4.1. Animal Studies
4.2. Clinical Assessment of CIA
4.3. Assessment of Arthritis and Histologic Score
4.4. Immunohistopathological Analyses of Arthritis
4.5. Tartrate-Resistant Acid Phosphatase (TRAP) Staining
4.6. Enzyme-Linked Immunosorbent Assay (ELISA)
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef] [PubMed]
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef]
- Falconer, J.; Murphy, A.N.; Young, S.P.; Clark, A.R.; Tiziani, S.; Guma, M.; Buckley, C.D. Review: Synovial cell metabolism and chronic inflammation in rheumatoid arthritis. Arthritis Rheumatol. 2018, 70, 984–999. [Google Scholar] [CrossRef]
- Ollier, W.E.; Harrison, B.; Symmons, D. What is the natural history of rheumatoid arthritis? Best Pract. Res. Clin. Rheumatol. 2001, 15, 27–48. [Google Scholar] [CrossRef] [PubMed]
- Visser, H.; le Cessie, S.; Vos, K.; Breedveld, F.C.; Hazes, J.M. How to diagnose rheumatoid arthritis early: A prediction model for persistent (erosive) arthritis. Arthritis Rheum. 2002, 46, 357–365. [Google Scholar] [CrossRef]
- van der Woude, D.; van der Helm-van Mil, A.H.M. Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 174–187. [Google Scholar] [CrossRef]
- Pope, J.E. Management of Fatigue in Rheumatoid Arthritis. RMD Open 2020, 6, e001084. [Google Scholar] [CrossRef] [PubMed]
- Upchurch, K.S.; Kay, J. Evolution of treatment for rheumatoid arthritis. Rheumatology 2012, 51 (Suppl. 6), vi28–vi36. [Google Scholar] [CrossRef]
- Segal, N.A.; Toda, Y.; Huston, J.; Saeki, Y.; Shimizu, M.; Fuchs, H.; Shimaoka, Y.; Holcomb, R.; McLean, M.J. Two configurations of static magnetic fields for treating rheumatoid arthritis of the knee: A double-blind clinical trial. Arch. Phys. Med. Rehabil. 2001, 82, 1453–1460. [Google Scholar] [CrossRef]
- Feldman, D.E.; Bernatsky, S.; Houde, M.; Beauchamp, M.E.; Abrahamowicz, M. Early consultation with a rheumatologist for RA: Does it reduce subsequent use of orthopaedic surgery? Rheumatology 2013, 52, 452–459. [Google Scholar] [CrossRef]
- Funk, R.H.; Monsees, T.; Ozkucur, N. Electromagnetic effects—From cell biology to medicine. Prog. Histochem. Cytochem. 2009, 43, 177–264. [Google Scholar] [CrossRef]
- Waldorff, E.I.; Zhang, N.; Ryaby, J.T. Pulsed electromagnetic field applications: A corporate perspective. J. Orthop. Translat. 2017, 9, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, K.; Gengadharan, A.C.; Balachandran, C.; Manohar, B.M.; Puvanakrishnan, R. Low frequency pulsed electromagnetic field—A viable alternative therapy for arthritis. Indian J. Exp. Biol. 2009, 47, 939–948. [Google Scholar] [PubMed]
- Ross, C.L.; Zhou, Y.; McCall, C.E.; Soker, S.; Criswell, T.L. The use of pulsed electromagnetic field to modulate inflammation and improve tissue regeneration: A review. Bioelectricity 2019, 1, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Yang, W.; Zeng, Q.; Chen, W.; Zhu, Y.; Liu, W.; Wang, S.; Wang, B.; Shao, Z.; Zhang, Y. Promising application of pulsed electromagnetic fields (PEMFs) in musculoskeletal disorders. Biomed. Pharmacother. 2020, 131, 110767. [Google Scholar] [CrossRef]
- Shupak, N.M.; McKay, J.C.; Nielson, W.R.; Rollman, G.B.; Prato, F.S.; Thomas, A.W. Exposure to a specific pulsed low-frequency magnetic field: A double-blind placebo-controlled study of effects on pain ratings in rheumatoid arthritis and fibromyalgia patients. Pain Res. Manag. 2006, 11, 85–90. [Google Scholar] [CrossRef]
- Yang, X.; Guo, H.; Ye, W.; Yang, L.; He, C. Pulsed electromagnetic field attenuates osteoarthritis progression in a murine destabilization-induced model through inhibition of TNF-α and IL-6 signaling. Cartilage 2021, 13, 1665S–1675S. [Google Scholar] [CrossRef]
- Miyoshi, M.; Liu, S. Collagen-induced arthritis models. Methods Mol. Biol. 2018, 1868, 3–7. [Google Scholar] [CrossRef]
- Brand, D.D.; Latham, K.A.; Rosloniec, E.F. Collagen-induced arthritis. Nat. Protoc. 2007, 2, 1269–1275. [Google Scholar] [CrossRef]
- Mori, T.; Miyamoto, T.; Yoshida, H.; Asakawa, M.; Kawasumi, M.; Kobayashi, T.; Morioka, H.; Chiba, K.; Toyama, Y.; Yoshimura, A. IL-1β and TNFα-initiated IL-6-STAT3 pathway is critical in mediating inflammatory cytokines and RANKL expression in inflammatory arthritis. Int. Immunol. 2011, 23, 701–712. [Google Scholar] [CrossRef]
- Foey, A.D.; Parry, S.L.; Williams, L.M.; Feldmann, M.; Foxwell, B.M.; Brennan, F.M. Regulation of monocyte IL-10 synthesis by endogenous IL-1 and TNF-α: Role of the p38 and p42/44 mitogen-activated protein kinases. J. Immunol. 1998, 160, 920–928. [Google Scholar] [CrossRef]
- Ilchovska, D.D.; Barrow, D.M. An Overview of the NF-kB mechanism of pathophysiology in rheumatoid arthritis, investigation of the NF-kB ligand RANKL and related nutritional interventions. Autoimmun. Rev. 2021, 20, 102741. [Google Scholar] [CrossRef]
- Markovics, A.; Rosenthal, K.S.; Mikecz, K.; Carambula, R.E.; Ciemielewski, J.C.; Zimmerman, D.H. Restoring the balance between pro-inflammatory and anti-inflammatory cytokines in the treatment of rheumatoid arthritis: New insights from animal models. Biomedicines 2021, 10, 44. [Google Scholar] [CrossRef]
- Ross, C.L.; Ang, D.C.; Almeida-Porada, G. Targeting mesenchymal stromal cells/pericytes (MSCs) with pulsed electromagnetic field (PEMF) has the potential to treat rheumatoid arthritis. Front. Immunol. 2019, 10, 266. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Lee, J.Y.; Lee, J.W.; Lee, S.K.; Park, C.S.; Yang, S.J.; Lee, Y.H. Evaluation of atopic dermatitis improvement caused by low-level, low-frequency pulsed electromagnetic fields. Bioelectromagnetics 2022, 43, 268–277. [Google Scholar] [CrossRef] [PubMed]
- van Delft, M.A.M.; Huizinga, T.W.J. An overview of autoantibodies in rheumatoid arthritis. J. Autoimmun. 2020, 110, 102392. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Bozec, A.; Ramming, A.; Schett, G. Anti-inflammatory and immune-regulatory cytokines in rheumatoid arthritis. Nat. Rev. Rheumatol. 2019, 15, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Fang, Q.; Zhou, C.; Nandakumar, K.S. Molecular and cellular pathways contributing to joint damage in rheumatoid arthritis. Mediators Inflamm. 2020, 2020, 3830212. [Google Scholar] [CrossRef] [PubMed]
- Avci, A.B.; Feist, E.; Burmester, G.R. Targeting IL-6 or IL-6 receptor in rheumatoid arthritis: What’s the difference? BioDrugs 2018, 32, 531–546. [Google Scholar] [CrossRef]
- Zhao, M.; He, H.; Yin, J. CARD6 protects against collagen-induced rheumatoid arthritis in mice through attenuating the inflammatory response and joint destruction via suppression of TNFR1/TRAF2 signaling. Biochem. Biophys. Res. Commun. 2020, 526, 1092–1099. [Google Scholar] [CrossRef]
- Won, S.; Cho, S.K.; Kim, D.; Han, M.; Lee, J.; Jang, E.J.; Sung, Y.K.; Bae, S.C. Update on the prevalence and incidence of rheumatoid arthritis in Korea and an analysis of medical care and drug utilization. Rheumatol. Int. 2018, 38, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Dekkers, J.S.; Schoones, J.W.; Huizinga, T.W.; Toes, R.E.; van der Helm-van Mil, A.H. Possibilities for preventive treatment in rheumatoid arthritis? Lessons from experimental animal models of arthritis: A systematic literature review and meta-analysis. Ann. Rheum. Dis. 2017, 76, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Gramling, A.; O’Dell, J.R. Initial management of rheumatoid arthritis. Rheum. Dis. Clin. N. Am. 2012, 38, 311–325. [Google Scholar] [CrossRef]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 15. [Google Scholar] [CrossRef]
- Marcacci, M.; Filardo, G.; Kon, E. Treatment of cartilage lesions: What works and why? Injury 2013, 44 (Suppl. 1), S11–S15. [Google Scholar] [CrossRef]
- Ross, C.L.; Siriwardane, M.; Almeida-Porada, G.; Porada, C.D.; Brink, P.; Christ, G.J.; Harrison, B.S. The effect of low-frequency electromagnetic field on human bone marrow stem/progenitor cell differentiation. Stem Cell Res. 2015, 15, 96–108. [Google Scholar] [CrossRef]
- Massari, L.; Benazzo, F.; Falez, F.; Perugia, D.; Pietrogrande, L.; Setti, S.; Osti, R.; Vaienti, E.; Ruosi, C.; Cadossi, R. Biophysical stimulation of bone and cartilage: State of the art and future perspectives. Int. Orthop. 2019, 43, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Mansourian, M.; Shanei, A. Evaluation of pulsed electromagnetic field effects: A systematic review and meta-analysis on highlights of two decades of research in vitro studies. Biomed. Res. Int. 2021, 2021, 6647497. [Google Scholar] [CrossRef]
- Selvam, R.; Ganesan, K.; Narayana Raju, K.V.; Gangadharan, A.C.; Manohar, B.M.; Puvanakrishnan, R. Low frequency and low intensity pulsed electromagnetic field exerts its antiinflammatory effect through restoration of plasma membrane calcium ATPase activity. Life Sci. 2007, 80, 2403–2410. [Google Scholar] [CrossRef]
- Fonseca Velásquez, A.; Rodríguez Sarmiento, L.A.; Cantillo Bermúdez, J.I.P.; Vaca-González, J.J. Electromagnetic fields as a non-invasive alternative therapy for the treatment of musculoskeletal diseases. J. Appl. Res. Technol. 2022, 20, 245–259. [Google Scholar] [CrossRef]
- Gomez-Ochoa, I.; Gomez-Ochoa, P.; Gomez-Casal, F.; Cativiela, E.; Larrad-Mur, L. Pulsed electromagnetic fields decrease proinflammatory cytokine secretion (IL-1β and TNF-α) on human fibroblast-like cell culture. Rheumatol. Int. 2011, 31, 1283–1289. [Google Scholar] [CrossRef]
- Zhou, P.; Zheng, T.; Zhao, B. Cytokine-mediated immunomodulation of osteoclastogenesis. Bone 2022, 164, 116540. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, M.; Hayakawa, N.; Mihara, M. IL-6 trans-signalling directly induces RANKL on fibroblast-like synovial cells and is involved in RANKL induction by TNF-α and IL-17. Rheumatology 2008, 47, 1635–1640. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.J.; Jones, R.H.; Rademacher, T.W. Correlation between IgG anti-type II collagen levels and arthritic severity in murine arthritis. Autoimmunity 1998, 27, 201–207. [Google Scholar] [CrossRef]
- Kruglov, A.; Drutskaya, M.; Schlienz, D.; Gorshkova, E.; Kurz, K.; Morawietz, L.; Nedospasov, S. Contrasting contributions of TNF from distinct cellular sources in arthritis. Ann. Rheum. Dis. 2020, 79, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Holmdahl, R.; Jansson, L.; Gullberg, D.; Rubin, K.; Forsberg, P.O.; Klareskog, L. Incidence of arthritis and autoreactivity of anti-collagen antibodies after immunization of DBA/1 mice with heterologous and autologous collagen II. Clin. Exp. Immunol. 1985, 62, 639–646. [Google Scholar] [PubMed]
- Coutant, F. Pathogenic effects of anti-citrullinated protein antibodies in rheumatoid arthritis—Role for glycosylation. Joint Bone Spine 2019, 86, 562–567. [Google Scholar] [CrossRef]
- Hansson, A.S.; Lu, S.; Holmdahl, R. Extra-articular cartilage affected in collagen-induced, but not pristane-induced, arthritis models. Clin. Exp. Immunol. 2002, 127, 37–42. [Google Scholar] [CrossRef][Green Version]
- Lee, C.G.; Park, C.; Hwang, S.; Hong, J.E.; Jo, M.; Eom, M.; Lee, Y.; Rhee, K.J. Pulsed electromagnetic field (PEMF) treatment reduces lipopolysaccharide-induced septic shock in mice. Int. J. Mol. Sci. 2022, 23, 5661. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.-E.; Lee, C.-G.; Hwang, S.; Kim, J.; Jo, M.; Kang, D.-H.; Yoo, S.-H.; Kim, W.-S.; Lee, Y.; Rhee, K.-J. Pulsed Electromagnetic Field (PEMF) Treatment Ameliorates Murine Model of Collagen-Induced Arthritis. Int. J. Mol. Sci. 2023, 24, 1137. https://doi.org/10.3390/ijms24021137
Hong J-E, Lee C-G, Hwang S, Kim J, Jo M, Kang D-H, Yoo S-H, Kim W-S, Lee Y, Rhee K-J. Pulsed Electromagnetic Field (PEMF) Treatment Ameliorates Murine Model of Collagen-Induced Arthritis. International Journal of Molecular Sciences. 2023; 24(2):1137. https://doi.org/10.3390/ijms24021137
Chicago/Turabian StyleHong, Ju-Eun, Chang-Gun Lee, Soonjae Hwang, Junyoung Kim, Minjeong Jo, Da-Hye Kang, Sang-Hyeon Yoo, Woo-Seung Kim, Yongheum Lee, and Ki-Jong Rhee. 2023. "Pulsed Electromagnetic Field (PEMF) Treatment Ameliorates Murine Model of Collagen-Induced Arthritis" International Journal of Molecular Sciences 24, no. 2: 1137. https://doi.org/10.3390/ijms24021137
APA StyleHong, J.-E., Lee, C.-G., Hwang, S., Kim, J., Jo, M., Kang, D.-H., Yoo, S.-H., Kim, W.-S., Lee, Y., & Rhee, K.-J. (2023). Pulsed Electromagnetic Field (PEMF) Treatment Ameliorates Murine Model of Collagen-Induced Arthritis. International Journal of Molecular Sciences, 24(2), 1137. https://doi.org/10.3390/ijms24021137