
Genotype Prevalence of Lactose Deficiency, Vitamin D Deficiency, and the Vitamin D Receptor in a Chilean Inflammatory Bowel Disease Cohort: Insights from an Observational Study

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Characterization of the Chilean Inflammatory Bowel Disease Cohort
2.1.1. Characterization of Lactose-Malabsorption Genotypes
2.1.2. Characterization of Vitamin D-Deficiency-Associated SNPs
2.1.3. Characterization of Vitamin D Receptor SNPs
3. Discussion
4. Materials and Methods
4.1. Study Group
4.2. Genotyping
4.3. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ugidos-Rodríguez, S.; Matallana-González, M.C.; Sánchez-Mata, M.C. Lactose malabsorption and intolerance: A review. Food Funct. 2018, 9, 4056–4068. [Google Scholar] [CrossRef]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on lactose malabsorption and intolerance: Pathogenesis, diagnosis and clinical management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef]
- Nardone, O.M.; Manfellotto, F.; D’onofrio, C.; Rocco, A.; Annona, G.; Sasso, F.; De Luca, P.; Imperatore, N.; Testa, A.; de Sire, R.; et al. Lactose intolerance assessed by analysis of genetic polymorphism, breath test and symptoms in patients with inflammatory bowel disease. Nutrients 2021, 13, 1290. [Google Scholar] [CrossRef] [PubMed]
- Enattah, N.S.; Trudeau, A.; Pimenoff, V.; Maiuri, L.; Auricchio, S.; Greco, L.; Rossi, M.; Lentze, M.; Seo, J.; Rahgozar, S.; et al. Evidence of Still-Ongoing Convergence Evolution of the Lactase Persistence T-13910 Alleles in Humans. Am. J. Hum. Genet. 2007, 81, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.R.; Bello, H.; Warren, A.P.; Brown, G.E. Prevalence of lactose maldigestion. Dig. Dis. Sci. 1994, 39, 1519–1524. [Google Scholar] [CrossRef] [PubMed]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 738–746. [Google Scholar] [CrossRef]
- Morales, E.; Azocar, L.; Maul, X.; Perez, C.; Chianale, J.; Miquel, J.F. The European lactase persistence genotype determines the lactase persistence state and correlates with gastrointestinal symptoms in the Hispanic and Amerindian Chilean population: A case-control and population-based study. BMJ Open 2011, 1, e000125. [Google Scholar] [CrossRef]
- Latorre, G.; Besa, P.; Parodi, C.G.; Ferrer, V.; Azocar, L.; Quirola, M.; Villarroel, L.; Miquel, J.F.; Agosin, E.; Chianale, J. Prevalence of Lactose Intolerance in Chile: A Double-Blind Placebo Study. Digestion 2014, 90, 18–26. [Google Scholar] [CrossRef]
- Eadala, P.; Matthews, S.B.; Waud, J.P.; Green, J.T.; Campbell, A.K. Association of lactose sensitivity with inflammatory bowel disease—Demonstrated by analysis of genetic polymorphism, breath gases and symptoms. Aliment. Pharmacol. Ther. 2011, 34, 735–746. [Google Scholar] [CrossRef]
- Szilagyi, A.; Galiatsatos, P.; Xue, X. Systematic review and meta-analysis of lactose digestion, its impact on intolerance and nutritional effects of dairy food restriction in inflammatory bowel diseases. Nutr. J. 2016, 15, 67. [Google Scholar] [CrossRef] [PubMed]
- Kotze, P.G.; Underwood, F.E.; Damião, A.O.M.C.; Ferraz, J.G.P.; Saad-Hossne, R.; Toro, M.; Iade, B.; Bosques-Padilla, F.; Teixeira, F.V.; Juliao-Banos, F.; et al. Progression of Inflammatory Bowel Diseases Throughout Latin America and the Caribbean: A Systematic Review. Clin. Gastroenterol. Hepatol. 2020, 18, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Benchimol, E.I.; Bitton, A.; Murthy, S.K.; Nguyen, G.C.; Lee, K.; Cooke-Lauder, J.; Kaplan, G.G. The Impact of Inflammatory Bowel Disease in Canada 2018: Extra-intestinal Diseases in IBD. J. Can. Assoc. Gastroenterol. 2019, 2 (Suppl. S1), S73–S80. [Google Scholar] [CrossRef] [PubMed]
- Koutroubakis, I.E.; Zavos, C.; Damilakis, J.; Papadakis, G.Z.; Neratzoulakis, J.; Karkavitsas, N.; Kouroumalis, E.A. Low bone mineral density in Greek patients with inflammatory bowel disease: Prevalence and risk factors. Ann. Gastroenterol. 2011, 24, 41–46. [Google Scholar] [PubMed]
- Krela-Kaźmierczak, I.; Michalak, M.; Szymczak-Tomczak, A.; Łykowska-Szuber, L.; Stawczyk-Eder, K.; Waszak, K.; Kucharski, M.A.; Dobrowolska, A.; Eder, P. Prevalence of osteoporosis and osteopenia in a population of patients with inflammatory bowel diseases from the Wielkopolska Region. Pol. Arch. Intern. Med. 2018, 128, 447–454. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Allegra, A.; Sirufo, M.M.; Tonacci, A.; Pioggia, G.; Raggiunti, M.; Ginaldi, L.; Gangemi, S. Vitamin D deficiency, osteoporosis and effect on autoimmune diseases and hematopoiesis: A review. Int. J. Mol. Sci. 2021, 22, 8855. [Google Scholar] [CrossRef]
- Gubatan, J.; Mitsuhashi, S.; Zenlea, T.; Rosenberg, L.; Robson, S.; Moss, A.C. Low Serum Vitamin D during Remission Increases Risk of Clinical Relapse in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2017, 15, 240–246.e1. [Google Scholar] [CrossRef]
- Sahay, T.; Ananthakrishnan, A.N. Vitamin D deficiency is associated with community-acquired clostridium difficile infection: A case–control study. BMC Infect. Dis. 2014, 14, 661. [Google Scholar] [CrossRef]
- Mechie, N.-C.; Mavropoulou, E.; Ellenrieder, V.; Kunsch, S.; Cameron, S.; Amanzada, A. Distinct Association of Serum Vitamin D Concentration with Disease Activity and Trough Levels of Infliximab and Adalimumab during Inflammatory Bowel Disease Treatment. Digestion 2020, 101, 761–770. [Google Scholar] [CrossRef]
- Winter, R.W.; Collins, E.; Cao, B.; Carrellas, M.; Crowell, A.M.; Korzenik, J.R. Higher 25-hydroxyvitamin D levels are associated with greater odds of remission with anti-tumour necrosis factor-α medications among patients with inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2017, 45, 653–659. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Cagan, A.; Gainer, V.S.; Cai, T.; Cheng, S.-C.; Savova, G.; Chen, P.; Szolovits, P.; Xia, Z.; De Jager, P.L.; et al. Normalization of Plasma 25-Hydroxy Vitamin D Is Associated with Reduced Risk of Surgery in Crohn’s Disease. Inflamm. Bowel Dis. 2013, 19, 1921–1927. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Cheng, S.; Cai, T.; Cagan, A.; Gainer, V.S.; Szolovits, P.; Shaw, S.Y.; Churchill, S.; Karlson, E.W.; Murphy, S.N.; et al. Association between Reduced Plasma 25-Hydroxy Vitamin D and Increased Risk of Cancer in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2014, 12, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Khalili, H.; Higuchi, L.M.; Bao, Y.; Korzenik, J.R.; Giovannucci, E.L.; Richter, J.M.; Fuchs, C.S.; Chan, A.T. Higher Predicted Vitamin D Status Is Associated with Reduced Risk of Crohn’s Disease. Gastroenterology 2012, 142, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Del Pinto, R.; Ferri, C.; Cominelli, F. Vitamin D axis in inflammatory bowel diseases: Role, current uses and future perspectives. Int. J. Mol. Sci. 2017, 18, 2360. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, O.H.; Rejnmark, L.; Moss, A.C. Role of Vitamin D in the Natural History of Inflammatory Bowel Disease. J. Crohn’s Colitis 2018, 12, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.H.; Kim, Y.S.; Lee, B.K.; Choi, J.H.; Woo, Y.M.; Kim, J.Y.; Moon, J.S. Vitamin D deficiency is associated with disease activity in patients with Crohn’s disease. Intest. Res. 2019, 17, 70–77. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Dankers, W.; Colin, E.M.; van Hamburg, J.P.; Lubberts, E. Vitamin D in Autoimmunity: Molecular Mechanisms and Therapeutic Potential. Front. Immunol. 2017, 7, 697. [Google Scholar] [CrossRef] [PubMed]
- Gois, P.H.F.; Ferreira, D.; Olenski, S.; Seguro, A.C. Vitamin D and Infectious Diseases: Simple Bystander or Contributing Factor? Nutrients 2017, 9, 651. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Liu, D.; Deng, F. The Role of Vitamin D in Immune System and Inflammatory Bowel Disease. J. Inflamm. Res. 2022, 15, 3167–3185. [Google Scholar] [CrossRef]
- NIH. GWAS Catolog. Vitamin D deficiency. EFO_0003762. Available online: https://www.ebi.ac.uk/gwas/efotraits/EFO_0003762 (accessed on 17 July 2023).
- Carvalho, A.; Bishop, K.S.; Han, D.Y.; Ellett, S.; Jesuthasan, A.; Lam, W.J.; Ferguson, L.R. The Role of Vitamin D Level and Related Single Nucleotide Polymorphisms in Crohn’s Disease. Nutrients 2013, 5, 3898–3909. [Google Scholar] [CrossRef]
- Zheng, S.; Zhang, D.-G.; Wu, H.; Jiang, L.-J.; Jin, J.; Lin, X.-Q.; Ding, R.; Jiang, Y. The association between vitamin D receptor polymorphisms and serum 25-hydroxyvitamin D levels with ulcerative colitis in Chinese Han population. Clin. Res. Hepatol. Gastroenterol. 2017, 41, 110–117. [Google Scholar] [CrossRef]
- Simmons, J.D.; Mullighan, C.; Welsh, K.I.; Jewell, D.P. Vitamin D receptor gene polymorphism: Association with Crohn’s disease susceptibility. Gut 2000, 47, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.J.; McManus, R.; Neary, P.; O’morain, C.; O’sullivan, M. Common variation in the vitamin D receptor gene and risk of inflammatory bowel disease in an Irish case–control study. Eur. J. Gastroenterol. Hepatol. 2011, 23, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Cagan, A.; Cai, T.; Gainer, V.S.; Shaw, S.Y.; Churchill, S.; Karlson, E.W.; Murphy, S.N.; Kohane, I.; Liao, K.P.; et al. Common Genetic Variants Influence Circulating Vitamin D Levels in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2015, 21, 2507–2514. [Google Scholar] [CrossRef]
- Xue, L.-N.; Xu, K.-Q.; Zhang, W.; Wang, Q.; Wu, J.; Wang, X.-Y. Associations between Vitamin D Receptor Polymorphisms and Susceptibility to Ulcerative Colitis and Crohn’s Disease. Inflamm. Bowel Dis. 2013, 19, 54–60. [Google Scholar] [CrossRef]
- Thomas, A.S.; Criss, Z.K.; Shroyer, N.F.; Abraham, B.P. Vitamin D Receptor Gene Single Nucleotide Polymorphisms and Association with Vitamin D Levels and Endoscopic Disease Activity in Inflammatory Bowel Disease Patients: A Pilot Study. Inflamm. Bowel Dis. 2021, 27, 1263–1269. [Google Scholar] [CrossRef] [PubMed]
- Bentley, R.W.; Keown, D.; Merriman, T.R.; Krishnan, M.R.; Gearry, R.B.; Barclay, M.L.; Roberts, R.L.; Day, A.S. Vitamin D receptor gene polymorphism associated with inflammatory bowel disease in New Zealand males. Aliment. Pharmacol. Ther. 2011, 33, 855–856. [Google Scholar] [CrossRef]
- Damas, O.M.; Maldonado-Contreras, A. Breaking Barriers in Dietary Research: Strategies to Diversify Recruitment in Clinical Studies and Develop Culturally Tailored Diets for Hispanic Communities Living with Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2023, 21, 2169–2173. [Google Scholar] [CrossRef]
- Santonocito, C.; Scapaticci, M.; Guarino, D.; Annicchiarico, E.B.; Lisci, R.; Penitente, R.; Gasbarrini, A.; Zuppi, C.; Capoluongo, E. Lactose intolerance genetic testing: Is it useful as routine screening? Results on 1426 south–central Italy patients. Clin. Chim. Acta 2015, 439, 14–17. [Google Scholar] [CrossRef]
- Di Stefano, M.; Terulla, V.; Tana, P.; Mazzocchi, S.; Romero, E.; Corazza, G. Genetic test for lactase non-persistence and hydrogen breath test: Is genotype better than phenotype to diagnose lactose malabsorption? Dig. Liver Dis. 2009, 41, 474–479. [Google Scholar] [CrossRef]
- Vivinus-Nébot, M.; Frin-Mathy, G.; Bzioueche, H.; Dainese, R.; Bernard, G.; Anty, R.; Filippi, J.; Saint-Paul, M.C.; Tulic, M.K.; Verhasselt, V.; et al. Functional bowel symptoms in quiescent inflammatory bowel diseases: Role of epithelial barrier disruption and low-grade inflammation. Gut 2014, 63, 744–752. [Google Scholar] [CrossRef]
- Morton, H.; Pedley, K.C.; Stewart, R.J.C.; Coad, J. Inflammatory Bowel Disease: Are Symptoms and Diet Linked? Nutrients 2020, 12, 2975. [Google Scholar] [CrossRef] [PubMed]
- Ratajczak, A.E.; Rychter, A.M.; Zawada, A.; Dobrowolska, A.; Krela-Kaźmierczak, I. Lactose intolerance in patients with inflammatory bowel diseases and dietary management in prevention of osteoporosis. Nutrition 2021, 82, 111043. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, A.; Ishayek, N. Lactose Intolerance, Dairy Avoidance, and Treatment Options. Nutrients 2018, 10, 1994. [Google Scholar] [CrossRef] [PubMed]
- Sun, J. VDR/vitamin D receptor regulates autophagic activity through ATG16L1. Autophagy 2016, 12, 1057–1058. [Google Scholar] [CrossRef]
- Salem, M.; Ammitzboell, M.; Nys, K.; Seidelin, J.B.; Nielsen, O.H. ATG16L1: A multifunctional susceptibility factor in Crohn disease. Autophagy 2015, 11, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Luettig, J.; Rosenthal, R.; Barmeyer, C.; Schulzke, J. Claudin-2 as a mediator of leaky gut barrier during intestinal inflammation. Tissue Barriers 2015, 3, e977176. [Google Scholar] [CrossRef]
- Stio, M.; Retico, L.; Annese, V.; Bonanomi, A.G. Vitamin D regulates the tight-junction protein expression in active ulcerative colitis. Scand. J. Gastroenterol. 2016, 51, 1193–1199. [Google Scholar] [CrossRef]
- Barbáchano, A.; Fernández-Barral, A.; Ferrer-Mayorga, G.; Costales-Carrera, A.; Larriba, M.J.; Muñoz, A. The endocrine vitamin D system in the gut. Mol. Cell. Endocrinol. 2017, 453, 79–87. [Google Scholar] [CrossRef]
- Gombart, A.F.; Borregaard, N.; Koeffler, H.P. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly up-regulated in myeloid cells by 1,25-dihydroxyvitamin D3. FASEB J. 2005, 19, 1067–1077. [Google Scholar] [CrossRef]
- Wang, T.-T.; Dabbas, B.; Laperriere, D.; Bitton, A.J.; Soualhine, H.; Tavera-Mendoza, L.E.; Dionne, S.; Servant, M.J.; Bitton, A.; Seidman, E.G.; et al. Direct and Indirect Induction by 1,25-Dihydroxyvitamin D3 of the NOD2/CARD15-Defensin β2 Innate Immune Pathway Defective in Crohn Disease. J. Biol. Chem. 2010, 285, 2227–2231. [Google Scholar] [CrossRef] [PubMed]
- Konya, V.; Czarnewski, P.; Forkel, M.; Rao, A.; Kokkinou, E.; Villablanca, E.J.; Almer, S.; Lindforss, U.; Friberg, D.; Höög, C.; et al. Vitamin D downregulates the IL-23 receptor pathway in human mucosal group 3 innate lymphoid cells. J. Allergy Clin. Immunol. 2018, 141, 279–292. [Google Scholar] [CrossRef]
- Bartels, L.E.; Jørgensen, S.P.; Bendix, M.; Hvas, C.L.; Agnholt, J.; Agger, R.; Dahlerup, J.F. 25-Hydroxy vitamin D3 modulates dendritic cell phenotype and function in Crohn’s disease. Inflammopharmacology 2013, 21, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Bartels, L.E.; Bendix, M.; Hvas, C.L.; Jørgensen, S.P.; Agnholt, J.; Agger, R.; Dahlerup, J.F. Oral vitamin D3 supplementation reduces monocyte-derived dendritic cell maturation and cytokine production in Crohn’s disease patients. Inflammopharmacology 2014, 22, 95–103. [Google Scholar] [CrossRef]
- Basson, A. Vitamin D and Crohn’s Disease in the Adult Patient. J. Parenter. Enter. Nutr. 2014, 38, 438–458. [Google Scholar] [CrossRef]
- Bartels, L.E.; Jørgensen, S.P.; Agnholt, J.; Kelsen, J.; Hvas, C.L.; Dahlerup, J.F. 1,25-dihydroxyvitamin D3 and dexamethasone increase interleukin-10 production in CD4+ T cells from patients with Crohn’s disease. Int. Immunopharmacol. 2007, 7, 1755–1764. [Google Scholar] [CrossRef]
- Reich, K.M. Vitamin D improves inflammatory bowel disease outcomes: Basic science and clinical review. World J. Gastroenterol. 2014, 20, 4934. [Google Scholar] [CrossRef]
- Heine, G.; Niesner, U.; Chang, H.-D.; Steinmeyer, A.; Zügel, U.; Zuberbier, T.; Radbruch, A.; Worm, M. 1,25-dihydroxyvitamin D3 promotes IL-10 production in human B cells. Eur. J. Immunol. 2008, 38, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, A.V.; Luu, W.; Li, D.; Sharpe, L.J.; Brown, A.J. DHCR7: A vital enzyme switch between cholesterol and vitamin D production. Prog. Lipid Res. 2016, 64, 138–151. [Google Scholar] [CrossRef]
- Prabhu, A.V.; Luu, W.; Sharpe, L.J.; Brown, A.J. Cholesterol-mediated Degradation of 7-Dehydrocholesterol Reductase Switches the Balance from Cholesterol to Vitamin D Synthesis. J. Biol. Chem. 2016, 291, 8363–8373. [Google Scholar] [CrossRef] [PubMed]
- Guerini, F.R.; Bolognesi, E.; Chiappedi, M.; Mensi, M.M.; Fumagalli, O.; Rogantini, C.; Zanzottera, M.; Ghezzo, A.; Zanette, M.; Agliardi, C.; et al. Vitamin D Receptor Polymorphisms Associated with Autism Spectrum Disorder. Autism Res. 2020, 13, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Agliardi, C.; Guerini, F.R.; Saresella, M.; Caputo, D.; Leone, M.A.; Zanzottera, M.; Bolognesi, E.; Marventano, I.; Barizzone, N.; Fasano, M.E.; et al. Vitamin D receptor (VDR) gene SNPs influence VDR expression and modulate protection from multiple sclerosis in HLA-DRB1*15-positive individuals. Brain Behav. Immun. 2011, 25, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn’s Colitis 2019, 13, 144–164K. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.T.; Ananthakrishnan, A.N.; Siegel, C.A.; Sauer, B.G.; Long, M.D. ACG Clinical Guideline: Ulcerative Colitis in Adults. Am. J. Gastroenterol. 2019, 114, 384–413. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Loftus, E.V.; Isaacs, K.L.; Regueiro, M.D.; Gerson, L.B.; Sands, B.E. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am. J. Gastroenterol. Am. J. Gastroenterol. 2018, 113, 481–517. [Google Scholar] [CrossRef]

{kind=link}
| LCT-13910 rs4988235 | TT | TC | CC | p-Value (Chi-Square) |
| Chilean IBD (N = 192) | 5 (2.6%) | 70 (36.4%) | 117 (61%) | 0.4 |
| Chilean Hispanic * (N = 219) | 3 (1.4%) | 90 (41.1%) | 126 (57.5%) | Reference |
| Amerindians * (N = 43) | 0 | 5 (2.6%) | 38 (88.4%) | 0.02 |
| (a) | ||||
| LCT-13910 rs4988235 | TT | TC | CC | p-Value (Chi-square) |
| Chilean IBD (N = 192) | 5 (2.6%) | 70 (36.4%) | 117 (61%) | Reference |
| All (N = 2504) | 197 (7.9%) | 414 (16.5%) | 1893 (75.6%) | 7.74 × 10−12 |
| European (N = 503) | 162 (32.2%) | 187 (37.2%) | 154 (30.6%) | <2.2 × 10−6 |
| American (N = 347) | 22 (63%) | 106 (30.6%) | 219 (63.1%) | 0.08 |
| East Asian (N = 504) | 0 | 0 | 504 (100%) | <2.2 × 10−6 |
| (b) | ||||
| Risk Variant | Chr | Gene | Risk Allele | Description | Allele Frequency | Genotype | |||
|---|---|---|---|---|---|---|---|---|---|
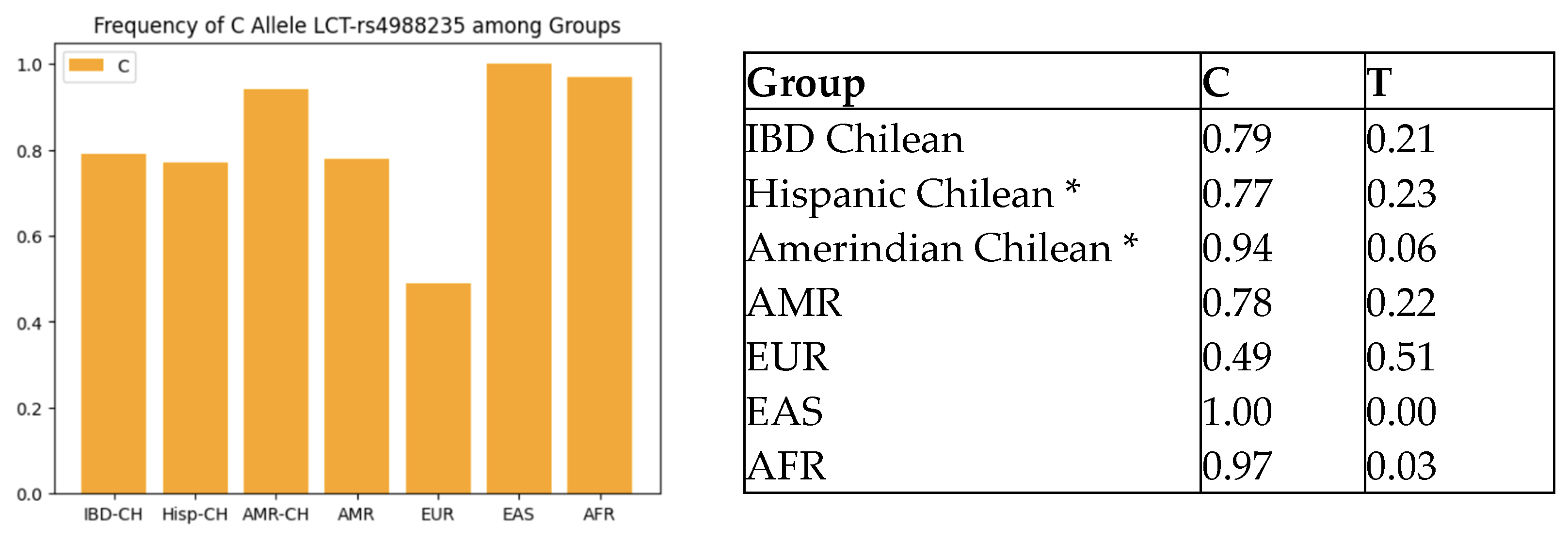
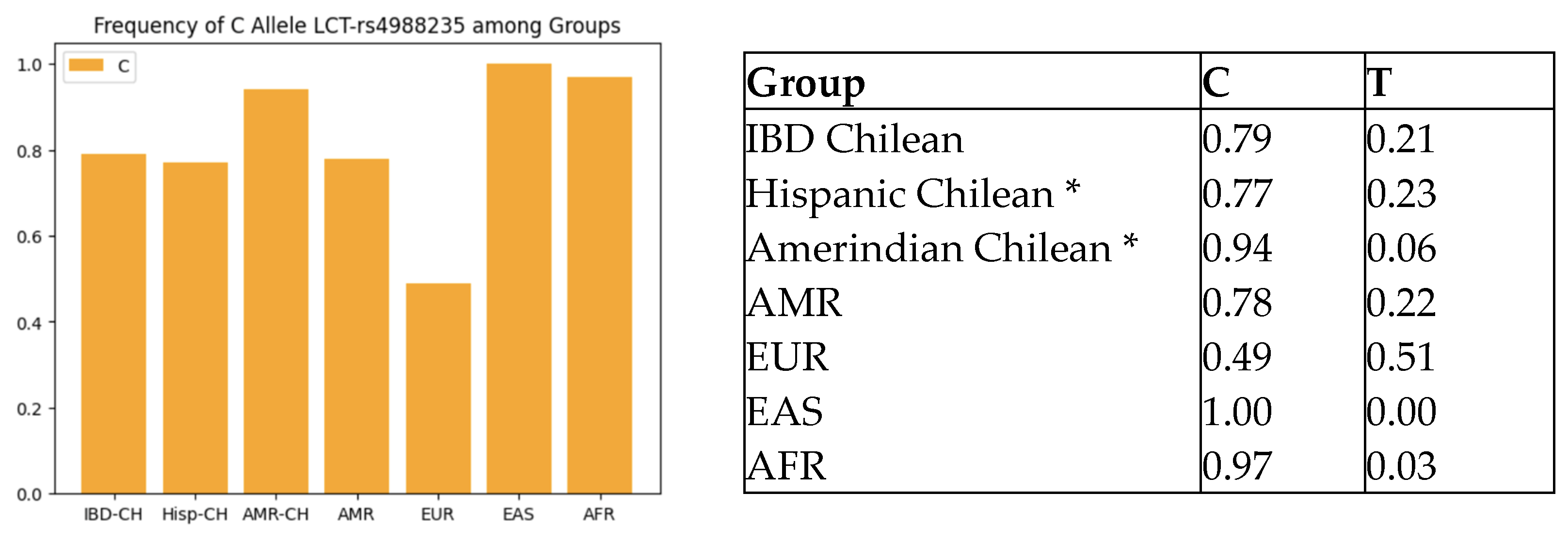
| Encodes for the lactase enzyme | C = 0.79 | CC | TC | TT | |||||
| rs4988235 | 2 | LCT | C | T = 0.21 | Lactose malabsorption | 117 (61%) | 70 (36.4%) | 5 (2.6%) | |
| Encodes human-group-specific component, which is the major vitamin D-binding protein (VDBP) in plasma | C = 0.22 A = 0.88 | Deficiency of vitamin D | CC | CA | AA | ||||
| rs2282679 | 4 | GC | A | 10 (5.2%) | 65 (33.8%) | 117 (61%) | |||
| Gene that produces the 7-dehydrocholesterol reductase enzyme, which catalyzes the production of cholesterol from 7-dehydrocholesterol using NADPH | G = 0.42 T = 0.58 | GG | GT | TT | |||||
| rs12785878 | 11 | DHCR7 | T | Deficiency of vitamin D | 37 (19.3%) | 88 (45.8%) | 67 (34.9%) | ||
| CYP2R1 gene has been linked by several studies to vitamin D serum concentrations | G = 0.67 | GG | AG | AA | |||||
| rs10741657 | 11 | CYP2R1 | A | A = 0.33 | Deficiency of vitamin D | 86 (44.8%) | 86 (44.8%) | 20 (10.4%) | |
| VDR (vitamin D receptor) gene variants | G = 0.758 A = 0.242 | AA | AG | GG | |||||
| rs1544410 | 12 | VDR | A | Related to autoimmune or inflammatory disease | 10 (5.2%) | 73 (38%) | 109 (56.78%) | ||
| VDR (vitamin D receptor) gene variants | G = 0.872 A = 0.127 | Related to autoimmune or inflammatory disease | AA | AG | GG | ||||
| rs11568820 | 12 | VDR | A | 5 (2.60%) | 39 (20.31%) | 148 (77.08%) | |||
| VDR (vitamin D receptor) gene variants | C = 0.531 A = 0.469 | Related to autoimmune or inflammatory disease | AA | AC | CC | ||||
| rs7975232 | 12 | VDR | A | 46 (23.96%) | 88 (45.83%) | 58 (30.21) | |||
| (a) | |||||||||||
| rs12785878 | Chilean IBD (N = 192) | All (N = 2504) | p-Value | ||||||||
| TT | 67 (34.9) | 433 (17.3%) | 1.32 × 10−14 | ||||||||
| GT | 88 (45.8%) | 907 (36.2%) | |||||||||
| GG | 37 (19.3%) | 1164 (46.5%) | |||||||||
| rs12785878 | Chilean IBD (N = 192) | European (N = 503) | p-value | ||||||||
| TT | 67 (34.9) | 251 (49.9%) | 0.0001 | ||||||||
| GT | 88 (45.8%) | 203 (40.4%) | |||||||||
| GG | 37 (19.3%) | 49 (9.7%) | |||||||||
| rs12785878 | Chilean IBD (N = 192) | American (N = 347) | p-value | ||||||||
| TT | 67 (34.9) | 76 (21.9%) | 0.0005 | ||||||||
| GT | 88 (45.8%) | 160 (46.1%) | |||||||||
| GG | 37 (19.3%) | 111 (32%) | |||||||||
| rs12785878 | Chilean IBD (N = 192) | East Asian (N = 504) | p-value | ||||||||
| TT | 67 (34.9) | 69 (13.7%) | 7.24 × 10−11 | ||||||||
| GT | 88 (45.8%) | 245 (48.6%) | |||||||||
| GG | 37 (19.3%) | 190 (37.7%) | |||||||||
| (b) | |||||||||||
| rs12785878 | Chilean IBD (N = 192) | American (N = 347) | OR | CI | p-Value | ||||||
| TT | 67 (34.9) | 76 (21.9%) | Reference | Reference | Reference | ||||||
| GT | 88 (45.8%) | 160 (46.1%) | 1.60 | 1.05–2.43 | 0.03 | ||||||
| GG | 37 (19.3%) | 111 (32%) | 2.64 | 1.61–4.32 | 0.0001 | ||||||
| (c) | |||||||||||
| rs12785878 | Chilean IBD N = 192 | Xavier N = 478 | p Value (Chi2) | ||||||||
| TT | 67 (34.9%) | 235 (49%) | 0.001 | ||||||||
| GT | 88 (45.8%) | 186 (39%) | |||||||||
| GG | 37 (19.39%) | 57 (12%) | |||||||||
| T vs. G | 0.57 | 0.68 | |||||||||
| (a) | |||||||||||
| rs1544410 | Chilean IBD (N = 192) | All (N = 2504) | p-Value | ||||||||
| GG | 109 (56.8%) | 1303 (52%) | 0.03 | ||||||||
| AG | 73 (38%) | 920 (36.8%) | |||||||||
| AA | 10 (5.2%) | 281 (11.2%) | |||||||||
| rs1544410 | Chilean IBD (N = 192) | European (N = 503) | p-Value | ||||||||
| GG | 109 (56.8%) | 186 (37%) | 3.47 × 10−7 | ||||||||
| AG | 73 (38%) | 228 (45.3%) | |||||||||
| AA | 10 (5.2%) | 89 (17.7%) | |||||||||
| rs1544410 | Chilean IBD (N = 192) | American | p-Value | ||||||||
| GG | 109 (56.8%) | 196 (56.2%) | 0.5 | ||||||||
| AG | 73 (38%) | 124 (35.7%) | |||||||||
| AA | 10 (5.2%) | 27 (7.8%) | |||||||||
| rs1544410 | Chilean IBD (N = 192) | East Asian | p-Value | ||||||||
| GG | 109 (56.8%) | 439 (87.1%) | <2.2 × 10−16 | ||||||||
| AG | 73 (38%) | 65 (12.9%) | |||||||||
| AA | 10 (5.2%) | 0 | |||||||||
| (b) | |||||||||||
| rs1544410 | Chilean IBD (N = 192) | American | OR | CI | p-Value | ||||||
| GG | 109 (56.8%) | 196 (56.2%) | Reference | Reference | Reference | ||||||
| AG | 73 (38%) | 124 (35.7%) | 0.94 | 0.65–1.37 | 0.76 | ||||||
| AA | 10 (5.2%) | 27 (7.8%) | 1.50 | 0.70–3.21 | 0.29 | ||||||
| (a) | |||||||||||
| rs7975232 | Chilean IBD (N = 192) | All (N = 2504) | p-Value | ||||||||
| CC | 58 (30%) | 657 (26.2%) | 0.24 | ||||||||
| AA | 46 (24%) | 734 (29.3%) | |||||||||
| AC | 88 (46%) | 1113 (44.4%) | |||||||||
| rs7975232 | Chilean IBD (N = 192) | European (N = 503) | p-Value | ||||||||
| CC | 58 (30%) | 115 (22.9%)) | 0.02 | ||||||||
| AA | 46 (34%) | 170 (33.8%) | |||||||||
| AC | 88 (46%) | 218 (43.3%) | |||||||||
| rs7975232 | Chilean IBD (N = 192) | American (N = 347) | p-Value | ||||||||
| CC | 58 (30%) | 116 (33.4%) | 0.69 | ||||||||
| AA | 46 (34%) | 75 (21.6%) | |||||||||
| AC | 88 (46%) | 156 (45%) | |||||||||
| rs7975232 | Chilean IBD (N = 192) | Asian (N = 504) | p-Value | ||||||||
| CC | 58 (30%) | 261 (51.8%) | 1.56 × 10−8 | ||||||||
| AA | 46 (34%) | 50 (9.9%) | |||||||||
| AC | 88 (46%) | 193 (38.3%) | |||||||||
| (b) | |||||||||||
| rs7975232 | Chilean IBD (N = 192) | American (N = 347) | OR | CI | p-Value | ||||||
| CC | 58 | 116 (33.4%) | Reference | Reference | Reference | ||||||
| AA | 46 | 75 (21.6%) | 0.81 | 0.50–1.32 | 0.40 | ||||||
| AC | 88 | 156 (45%) | 0.88 | 0.58–1.33 | 0.56 | ||||||
| (a) | |||||||||||
| rs11568820 | Chilean IBD (N = 192) | All (N = 2504) | p-Value | ||||||||
| GG | 148 (77.1%) | 941 (37.6%) | <2.2 × 10−16 | ||||||||
| GA | 39 (20.3%) | 838 (33.5%) | |||||||||
| AA | 5 (2.6%) | 725 (29%) | |||||||||
| rs11568820 | Chilean IBD (N = 192) | European (N = 503) | p-Value | ||||||||
| GG | 148 (77.1%) | 303 (60.2%) | 0.0001 | ||||||||
| GA | 39 (20.3%) | 171 (34%) | |||||||||
| AA | 5 (2.6%) | 29 (5.8%) | |||||||||
| rs11568820 | Chilean IBD (N = 192) | East Asian (N = 504) | p-Value | ||||||||
| GG | 148 (77.1%) | 189 (37.5%) | <2.2 × 10−16 | ||||||||
| GA | 39 (20.3%) | 231 (45.8%) | |||||||||
| AA | 5 (2.6%) | 84 (16.7%) | |||||||||
| rs11568820 | Chilean IBD (N = 192) | American (N = 347) | p-Value | ||||||||
| GG | 148 (77.1%) | 235 (67.7%) | 0.06 | ||||||||
| GA | 39 (20.3%) | 97 (28%) | |||||||||
| AA | 5 (2.6%) | 15 (4.3%) | |||||||||
| (b) | |||||||||||
| rs11568820 | Chilean IBD (N = 192) | American (N = 347) | OR | CI | p-Value | ||||||
| GG | 148 (77.1%) | 235 (67.7%) | Reference | Reference | Reference | ||||||
| GA | 39 (20.3%) | 97 (28%) | 1.56 | 1.02–2.39 | 0.03 | ||||||
| AA | 5 (2.6%) | 15 (4.3%) | 1.88 | 0.67–5.30 | 0.22 | ||||||
| SNP | Inflammatory Bowel Disease Group Study | |||
|---|---|---|---|---|
| rs1544410 (Bsml) | Chilean IBD N = 192 | 0’Sullivan N = 645 | Abraham N = 50 | Zheng N = 404 |
| GG | 109 (57%) | 216 (33.5%) | 9 (18%) | 366 (90.6%) |
| GA | 73 (38%) | 312 (48.4%) | 24 (48%) | 38 (9.4%) |
| AA | 10 (5%) | 117 (18.1%) | 17 (34%) | 0 |
| G vs. A | 0.76 | 0.42 | 0.42 | 0.95 |
| rs7975232 (Apal) | Chilean IBD N = 192 | 0′Sullivan N = 641 | Zheng N = 404 | |
| AA | 46 (34%) | 205 (32%) | 196 (48.5%) | |
| CA | 88 (46%) | 306 (47.7%) | 185 (45.8%) | |
| CC | 58 (30%) | 130 (20.3%) | 23 (5.7%) | |
| A vs. C | 0.47 | 0.44 | 0.29 | |
| rs11568820 | Chilean IBD N = 192 | Bentley N = 897 | ||
| AA | 5 (2.6%) | 44 (5% ) | ||
| AG | 39 (20.3%) | 308 (34%) | ||
| GG | 148 (77.1%) | 545 (61%) | ||
| A vs. G | 0.13 | 0.22 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Jeldres, T.; Bustamante, M.L.; Segovia-Melero, R.; Aguilar, N.; Magne, F.; Ascui, G.; Uribe, D.; Azócar, L.; Hernández-Rocha, C.; Estela, R.; et al. Genotype Prevalence of Lactose Deficiency, Vitamin D Deficiency, and the Vitamin D Receptor in a Chilean Inflammatory Bowel Disease Cohort: Insights from an Observational Study. Int. J. Mol. Sci. 2023, 24, 14866. https://doi.org/10.3390/ijms241914866
Pérez-Jeldres T, Bustamante ML, Segovia-Melero R, Aguilar N, Magne F, Ascui G, Uribe D, Azócar L, Hernández-Rocha C, Estela R, et al. Genotype Prevalence of Lactose Deficiency, Vitamin D Deficiency, and the Vitamin D Receptor in a Chilean Inflammatory Bowel Disease Cohort: Insights from an Observational Study. International Journal of Molecular Sciences. 2023; 24(19):14866. https://doi.org/10.3390/ijms241914866
Chicago/Turabian StylePérez-Jeldres, Tamara, M. Leonor Bustamante, Roberto Segovia-Melero, Nataly Aguilar, Fabien Magne, Gabriel Ascui, Denisse Uribe, Lorena Azócar, Cristián Hernández-Rocha, Ricardo Estela, and et al. 2023. "Genotype Prevalence of Lactose Deficiency, Vitamin D Deficiency, and the Vitamin D Receptor in a Chilean Inflammatory Bowel Disease Cohort: Insights from an Observational Study" International Journal of Molecular Sciences 24, no. 19: 14866. https://doi.org/10.3390/ijms241914866
APA StylePérez-Jeldres, T., Bustamante, M. L., Segovia-Melero, R., Aguilar, N., Magne, F., Ascui, G., Uribe, D., Azócar, L., Hernández-Rocha, C., Estela, R., Silva, V., De La Vega, A., Arriagada, E., Gonzalez, M., Onetto, G.-F., Escobar, S., Baez, P., Zazueta, A., Pavez-Ovalle, C., ... Álvarez-Lobos, M. (2023). Genotype Prevalence of Lactose Deficiency, Vitamin D Deficiency, and the Vitamin D Receptor in a Chilean Inflammatory Bowel Disease Cohort: Insights from an Observational Study. International Journal of Molecular Sciences, 24(19), 14866. https://doi.org/10.3390/ijms241914866