
A Novel Predictive Machine Learning Model Integrating Cytokines in Cervical-Vaginal Mucus Increases the Prediction Rate for Preterm Birth

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Cytokine Profile in Low and High Risk for PB
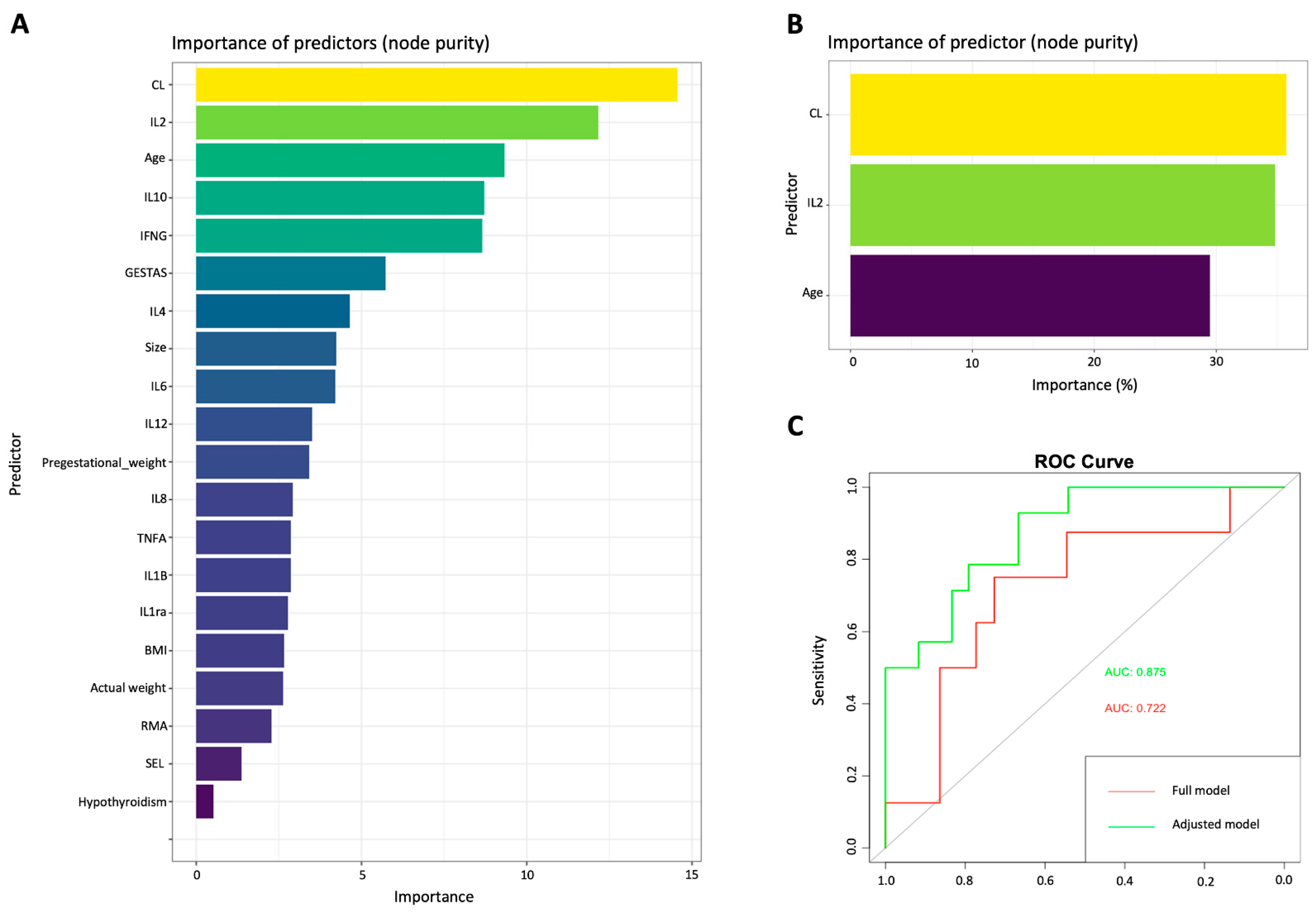
2.2. Machine Learning Predictive Model
3. Discussion
4. Materials and Methods
4.1. Ethics Statement
4.2. Study Population
4.3. Sample Collection
4.4. Cervical-Vaginal Cytokine Quantification
4.5. Statistical Analysis
4.6. Machine Learning Model
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Griggs, K.M.; Hrelic, D.A.; Williams, N.; McEwen-Campbell, M.; Cypher, R. Preterm Labor and Birth: A Clinical Review. MCN Am. J. Matern. Child. Nurs. 2020, 45, 328–337. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- Menon, R.; Torloni, M.R.; Voltolini, C.; Torricelli, M.; Merialdi, M.; Betrán, A.P.; Widmer, M.; Allen, T.; Davydova, I.; Khodjaeva, Z.; et al. Biomarkers of spontaneous preterm birth: An overview of the literature in the last four decades. Reprod. Sci. 2011, 18, 1046–1070. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, G.C.; Tosto, V.; Giardina, I. The biological basis and prevention of preterm birth. Best Pract. Res. Clin. Obstet. Gynecol. 2018, 52, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Fraser, W.; Luo, Z.C. Inflammatory cytokines and spontaneous preterm birth in asymptomatic women: A systematic review. Obstet. Gynecol. 2010, 116, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Simhan, H.N.; Bodnar, L.M.; Kim, K.H. Lower genital tract inflammatory milieu and the risk of subsequent preterm birth: An exploratory factor analysis. Paediatr. Perinat. Epidemiol. 2011, 25, 277–282. [Google Scholar] [CrossRef]
- Taylor, B.D.; Holzman, C.B.; Fichorova, R.N.; Tian, Y.; Jones, N.M.; Fu, W.; Senagore, P.K. Inflammation biomarkers in vaginal fluid and preterm delivery. Hum. Reprod. 2013, 28, 942–952. [Google Scholar] [CrossRef]
- Socha, M.W.; Flis, W.; Pietrus, M.; Wartęga, M.; Stankiewicz, M. Signaling Pathways Regulating Human Cervical Ripening in Preterm and Term Delivery. Cells 2022, 11, 3690. [Google Scholar] [CrossRef] [PubMed]
- Torbé, A.; Czajka, R. Proinflammatory cytokines and other indications of inflammation in cervico-vaginal secretions and preterm delivery. Int. J. Gynecol. Obstet. 2004, 87, 125–130. [Google Scholar] [CrossRef]
- Dowd, J.; Laham, N.; Rice, G.; Brennecke, S.; Permezel, M. Elevated interleukin-8 concentrations in cervical secretions are associated with preterm labour. Gynecol. Obstet. Investig. 2001, 51, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Ashford, K.; Chavan, N.R.; Wiggins, A.T.; Sayre, M.M.; McCubbin, A.; Critchfield, A.S.; O’Brien, J. Comparison of Serum and Cervical Cytokine Levels throughout Pregnancy between Preterm and Term Births. Am. J. Perinatol. Rep. 2018, 8, e113–e120. [Google Scholar] [CrossRef] [PubMed]
- Zaga-Clavellina, V.; Flores-Espinosa, P.; Pineda-Torres, M.; Sosa-González, I.; Vega-Sánchez, R.; Estrada-Gutierrez, G.; Espejel-Núñez, A.; Flores-Pliego, A.; Maida-Claros, R.; Estrada-Juárez, H.; et al. Tissue-specific IL-10 secretion profile from term human fetal membranes stimulated with pathogenic microorganisms associated with preterm labor in a two-compartment tissue culture system. J. Matern. Fetal Neonatal Med. 2014, 27, 1320–1327. [Google Scholar] [CrossRef]
- Gomez, R.; Romero, R.; Edwin, S.S.; David, C. Pathogenesis of preterm labor and preterm premature rupture of membranes associated with intraamniotic infection. Infect. Dis. Clin. N. Am. 1997, 11, 135–176. [Google Scholar] [CrossRef]
- Licini, C.; Tossetta, G.; Avellini, C.; Ciarmela, P.; Lorenzi, T.; Toti, P.; Gesuita, R.; Voltolini, C.; Petraglia, F.; Castellucci, M.; et al. Analysis of cell-cell junctions in human amnion and chorionic plate affected by chorioamnionitis. Histol. Histopathol. 2016, 31, 759–767. [Google Scholar] [CrossRef]
- Tossetta, G.; Paolinelli, F.; Avellini, C.; Salvolini, E.; Ciarmela, P.; Lorenzi, T.; Emanuelli, M.; Toti, P.; Giuliante, R.; Gesuita, R.; et al. IL-1β and TGF-β weaken the placental barrier through destruction of tight junctions: An in vivo and in vitro study. Placenta 2014, 35, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Celik, E.; To, M.; Gajewska, K.; Smith, G.C.; Nicolaides, K.H. Cervical length and obstetric history predict spontaneous preterm birth: Development and validation of a model to provide individualized risk assessment. Ultrasound Obstet. Gynecol. 2008, 31, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Cho, G.J.; Kwon, H.S. Applications of artificial intelligence in obstetrics. Ultrasonography 2023, 42, 2–9. [Google Scholar] [CrossRef]
- Arain, Z.; Iliodromiti, S.; Slabaugh, G.; David, A.L.; Chowdhury, T.T. Machine learning and disease prediction in obstetrics. Curr. Res. Physiol. 2023, 6, 100099. [Google Scholar] [CrossRef]
- Dodd, J.M.; Flenady, V.J.; Cincotta, R.; Crowther, C.A. Progesterone for the prevention of preterm birth: A systematic review. Obstet. Gynecol. 2008, 112, 127–134. [Google Scholar] [CrossRef]
- Meyyazhagan, A.; Kuchi Bhotla, H.; Pappuswamy, M.; Tsibizova, V.; Al Qasem, M.; Di Renzo, G.C. Cytokine see-saw across pregnancy, its related complexities and consequences. Int. J. Gynecol. Obstet. 2023, 160, 516–525. [Google Scholar] [CrossRef]
- Sandoval-Colin, D.E.; Godines-Enriquez, M.S.; Espejel-Núñez, A.; Beltrán-Montoya, J.J.; Picazo-Mendoza, D.A.; de la Cerda-Ángeles, J.C.; Bello-Chavolla, O.Y.; Meraz-Cruz, N.; Chavira-Suárez, E.; Vadillo-Ortega, F. Cervicovaginal Cytokines to Predict the Onset of Normal and Preterm Labor: A Pseudo-longitudinal Study. Reprod. Sci. 2023, 30, 221–232. [Google Scholar] [CrossRef]
- Park, J.W.; Park, K.H.; Lee, S.Y. Noninvasive prediction of intra-amniotic infection and/or inflammation in women with preterm labor: Various cytokines in cervicovaginal fluid. Reprod. Sci. 2013, 20, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Cetin, O.; Karaman, E.; Alisik, M.; Erel, O.; Kolusari, A.; Sahin, H.G. The evaluation of maternal systemic thiol/disulphide homeostasis for the short-term prediction of preterm birth in women with threatened preterm labour: A pilot study. J. Obstet. Gynecol. 2022, 42, 1972–1977. [Google Scholar] [CrossRef] [PubMed]
- Yavari Kia, P.; Baradaran, B.; Shahnazi, M.; Asghari Jafarabadi, M.; Khaze, V.; Pourasad Shahrak, S. Maternal Serum and Cervicovaginal IL-6 in Patients with Symptoms of Preterm Labor. Iran. J. Immunol. 2016, 13, 229–236. [Google Scholar] [PubMed]
- Hanna, N.; Bonifacio, L.; Reddy, P.; Hanna, I.; Weinberger, B.; Murphy, S.; Laskin, D.; Sharma, S. IFN-gamma-mediated inhibition of COX-2 expression in the placenta from term and preterm labor pregnancies. Am. J. Reprod. Immunol. 2004, 51, 311–318. [Google Scholar] [CrossRef]
- Buxton, M.A.; Meraz-Cruz, N.; Sanchez, B.N.; Foxman, B.; Castillo-Castrejon, M.; O’Neill, M.S.; Vadillo-Ortega, F. Timing of Cervico-Vaginal Cytokine Collection during Pregnancy and Preterm Birth: A Comparative Analysis in the PRINCESA Cohort. Int. J. Environ. Res. Public Health 2021, 18, 3436. [Google Scholar] [CrossRef]
- Chatterjee, P.; Chiasson, V.L.; Bounds, K.R.; Mitchell, B.M. Regulation of the Anti-Inflammatory Cytokines Interleukin-4 and Interleukin-10 during Pregnancy. Front. Immunol. 2014, 5, 253. [Google Scholar] [CrossRef]
- Park, J.S.; Park, C.W.; Lockwood, C.J.; Norwitz, E.R. Role of cytokines in preterm labor and birth. Minerva Ginecol. 2005, 57, 349–366. [Google Scholar]
- Wang, L.; Liu, Z.; Huang, D.; Ran, Y.; Zhang, H.; He, J.; Yin, N.; Qi, H. IL-37 Exerts Anti-Inflammatory Effects in Fetal Membranes of Spontaneous Preterm Birth via the NF-κB and IL-6/STAT3 Signaling Pathway. Mediat. Inflamm. 2020, 2020, 1069563. [Google Scholar] [CrossRef]
- Gilman-Sachs, A.; Dambaeva, S.; Salazar Garcia, M.D.; Hussein, Y.; Kwak-Kim, J.; Beaman, K. Inflammation induced preterm labor and birth. J. Reprod. Immunol. 2018, 129, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Goepfert, A.R.; Goldenberg, R.L.; Andrews, W.W.; Hauth, J.C.; Mercer, B.; Iams, J.; Meis, P.; Moawad, A.; Thom, E.; VanDorsten, J.P.; et al. The Preterm Prediction Study: Association between cervical interleukin 6 concentration and spontaneous preterm birth. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am. J. Obstet. Gynecol. 2001, 184, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Challis, J.R.; Lockwood, C.J.; Myatt, L.; Norman, J.E.; Strauss, J.F., 3rd; Petraglia, F. Inflammation and pregnancy. Reprod. Sci. 2009, 16, 206–215. [Google Scholar] [CrossRef]
- Paternoster, D.M.; Stella, A.; Gerace, P.; Manganelli, F.; Plebani, M.; Snijders, D.; Nicolini, U. Biochemical markers for the prediction of spontaneous pre-term birth. Int. J. Gynecol. Obstet. 2002, 79, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Helmo, F.R.; Alves, E.A.R.; Moreira, R.A.A.; Severino, V.O.; Rocha, L.P.; Monteiro, M.; Reis, M.A.D.; Etchebehere, R.M.; Machado, J.R.; Corrêa, R.R.M. Intrauterine infection, immune system and premature birth. J. Matern. Fetal Neonatal Med. 2018, 31, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.; Humphries, S.E. Cytokine and cytokine receptor gene polymorphisms and their functionality. Cytokine Growth Factor Rev. 2009, 20, 43–59. [Google Scholar] [CrossRef]
- Gonçalves, L.F.; Chaiworapongsa, T.; Romero, R. Intrauterine infection and prematurity. Ment. Retard. Dev. Disabil. Res. Rev. 2002, 8, 3–13. [Google Scholar] [CrossRef]
- Mitsuyama, K.; Matsumoto, S.; Rose-John, S.; Suzuki, A.; Hara, T.; Tomiyasu, N.; Handa, K.; Tsuruta, O.; Funabashi, H.; Scheller, J.; et al. STAT3 activation via interleukin 6 trans-signalling contributes to ileitis in SAMP1/Yit mice. Gut 2006, 55, 1263–1269. [Google Scholar] [CrossRef]
- Gaffen, S.L.; Liu, K.D. Overview of interleukin-2 function, production and clinical applications. Cytokine 2004, 28, 109–123. [Google Scholar] [CrossRef]
- Alvarez-de-la-Rosa, M.; Rebollo, F.J.; Codoceo, R.; Gonzalez Gonzalez, A. Maternal serum interleukin 1, 2, 6, 8 and interleukin-2 receptor levels in preterm labor and delivery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 57–60. [Google Scholar] [CrossRef]
- Cao, X.L.; Zhou, X.Y.; Xu, N.X.; Chen, S.C.; Xu, C.M. Association of IL-4 and IL-10 Polymorphisms with Preterm Birth Susceptibility: A Systematic Review and Meta-Analysis. Front. Immunol. 2022, 13, 917383. [Google Scholar] [CrossRef]
- Busse, M.; Zenclussen, A.C. IL-10 Producing B Cells Protect against LPS-Induced Murine Preterm Birth by Promoting PD1- and ICOS-Expressing T Cells. Cells 2022, 11, 2690. [Google Scholar] [CrossRef] [PubMed]
- Vogel, I.; Goepfert, A.R.; Thorsen, P.; Skogstrand, K.; Hougaard, D.M.; Curry, A.H.; Cliver, S.; Andrews, W.W. Early second-trimester inflammatory markers and short cervical length and the risk of recurrent preterm birth. J. Reprod. Immunol. 2007, 75, 133–140. [Google Scholar] [CrossRef]
- Bertini, A.; Salas, R.; Chabert, S.; Sobrevia, L.; Pardo, F. Using Machine Learning to Predict Complications in Pregnancy: A Systematic Review. Front. Bioeng. Biotechnol. 2021, 9, 780389. [Google Scholar] [CrossRef]
- Mohammad, N.S.; Nazli, R.; Zafar, H.; Fatima, S. Effects of lipid based Multiple Micronutrients Supplement on the birth outcome of underweight pre-eclamptic women: A randomized clinical trial. Pak. J. Med. Sci. 2022, 38, 219–226. [Google Scholar] [CrossRef]
- Saberi-Karimian, M.; Khorasanchi, Z.; Ghazizadeh, H.; Tayefi, M.; Saffar, S.; Ferns, G.A.; Ghayour-Mobarhan, M. Potential value and impact of data mining and machine learning in clinical diagnostics. Crit. Rev. Clin. Lab. Sci. 2021, 58, 275–296. [Google Scholar] [CrossRef]
- Oskovi Kaplan, Z.A.; Ozgu-Erdinc, A.S. Prediction of Preterm Birth: Maternal Characteristics, Ultrasound Markers, and Biomarkers: An Updated Overview. J. Pregnancy 2018, 2018, 8367571. [Google Scholar] [CrossRef] [PubMed]
- Glover, A.V.; Manuck, T.A. Screening for spontaneous preterm birth and resultant therapies to reduce neonatal morbidity and mortality: A review. Semin. Fetal Neonatal Med. 2018, 23, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.Y.; Park, J.W.; Ryu, A.; Lee, S.Y.; Cho, S.H.; Park, K.H. Prediction of impending preterm delivery based on sonographic cervical length and different cytokine levels in cervicovaginal fluid in preterm labor. J. Obstet. Gynecol. Res. 2016, 42, 158–165. [Google Scholar] [CrossRef]
- Norman, J.E. Progesterone and preterm birth. Int. J. Gynecol. Obstet. 2020, 150, 24–30. [Google Scholar] [CrossRef]
- Lee, K.S.; Ahn, K.H. Artificial Neural Network Analysis of Spontaneous Preterm Labor and Birth and Its Major Determinants. J. Korean Med. Sci. 2019, 34, e128. [Google Scholar] [CrossRef] [PubMed]
- Giouleka, S.; Tsakiridis, I.; Kostakis, N.; Koutsouki, G.; Kalogiannidis, I.; Mamopoulos, A.; Athanasiadis, A.; Dagklis, T. Preterm Labor: A Comprehensive Review of Guidelines on Diagnosis, Management, Prediction and Prevention. Obstet. Gynecol. Surv. 2022, 77, 302–317. [Google Scholar] [CrossRef] [PubMed]
- Berghella, V.; Palacio, M.; Ness, A.; Alfirevic, Z.; Nicolaides, K.H.; Saccone, G. Cervical length screening for prevention of preterm birth in singleton pregnancy with threatened preterm labor: Systematic review and meta-analysis of randomized controlled trials using individual patient-level data. Ultrasound Obstet. Gynecol. 2017, 49, 322–329. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Low Risk for Preterm Delivery (n = 40) | High Risk for Preterm Delivery (n = 20) | p-Value | |
|---|---|---|---|
| Age (years) | 29 (±7.1) | 31 (±5.8) | 0.25 |
| Pregestational weight (Kg) | 63.7 (±13.7) | 67.8 (±13.5) | 0.08 |
| Pregestational BMI (Kg/m2) | 25.2 (±5.4) | 27.5 (±5.3) | 0.12 |
| Socio-economic level, Median (Minimum and maximum value) | 2 (1–4) | 2 (1–5) | 0.12 |
| Smoking n (%) | 1 (2.5) | 0 (0) | 0.45 |
| History of preterm delivery n (%) | 0 (0) | 8 (40) | 0.01 ** |
| Gestational age at time of cervical length measurement, (weeks of gestation) | 21.0 (±1.5) | 21.2 (±2.0) | 0.25 |
| Cervical length (mm) | 33.8 (±5.8) | 13.1 (±7.7) | 0.02 * |
| SPB < 28 WG n (%) | 0 | 2 (10%) | 0.001 *** |
| SPB 28–34 WG n (%) | 2 (5%) | 6 (30%) | 0.001 *** |
| SPB > 34 WG n (%) | 1 (2.5%) | 1 (5%) | 0.01 ** |
| Cytokine | Risk Group for Preterm Birth | Mean ± SD pg/mL | p-Value |
|---|---|---|---|
| Pro-inflammatory cytokines | |||
| IL-1β | High Risk | 763.87 (±1505.99) | 0.814 |
| Low Risk | 587.94 (±1432.56) | ||
| IL-2 | High Risk | 5.63 (±1.48) | 0.01 ** |
| Low Risk | 3.60 (±6.07) | ||
| IL-6 | High Risk | 856.29 (±1.98) | 0.001 *** |
| Low Risk | 118.32 (±0.48) | ||
| IL-8 | High Risk | 5882.35 (±5638.79) | 0.381 |
| Low Risk | 9695.78 (±11,070.29) | ||
| IL-12 | High Risk | 0.49 (±0.49) | 0.304 |
| Low Risk | 0.34 (0.29) | ||
| TNF-α | High Risk | 104.17 (±74.62) | 0.115 |
| Low Risk | 78.63 (±50.32) | ||
| IFN-γ | High Risk | 117.49 (±53.42) | 0.001 *** |
| Low Risk | 54.17 (±26.37) | ||
| Anti-inflammatory cytokines | |||
| IL-4 | High Risk | 20.98 (±10.78) | 0.001 *** |
| Low Risk | 10.83 (±8.92) | ||
| IL-10 | High Risk | 40.44 (±41.23) | 0.001 *** |
| Low Risk | 3.56 (±5.22) | ||
| IL-1ra | High Risk | 29,768 (±17,596) | 0.002 *** |
| Low Risk | 58,377 (±40,841) | ||
| Random Forest “Full Model” | Random Forest “Adjusted Model” | Fetal Medicine Foundation Calculator | ||||||
|---|---|---|---|---|---|---|---|---|
| Predicted | Real | Predicted | Real | Predicted | Real | |||
| Term | Preterm | Term | Preterm | Term | Preterm | |||
| Term | 14 | 6 | Term | 20 | 1 | Term | 36 | 4 |
| Preterm | 2 | 1 | Preterm | 2 | 7 | Preterm | 7 | 13 |
| Detection rate | 65% | Detection rate | 87.7% | Detection rate | 79% | |||
| False positive rate | 12% | False positives rate | 3.33% | False positives rate | 6.6% | |||
| False negative rate | 28% | False negatives rate | 6.66% | False negatives rate | 11.66% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borboa-Olivares, H.; Rodríguez-Sibaja, M.J.; Espejel-Nuñez, A.; Flores-Pliego, A.; Mendoza-Ortega, J.; Camacho-Arroyo, I.; González-Camarena, R.; Echeverría-Arjonilla, J.C.; Estrada-Gutierrez, G. A Novel Predictive Machine Learning Model Integrating Cytokines in Cervical-Vaginal Mucus Increases the Prediction Rate for Preterm Birth. Int. J. Mol. Sci. 2023, 24, 13851. https://doi.org/10.3390/ijms241813851
Borboa-Olivares H, Rodríguez-Sibaja MJ, Espejel-Nuñez A, Flores-Pliego A, Mendoza-Ortega J, Camacho-Arroyo I, González-Camarena R, Echeverría-Arjonilla JC, Estrada-Gutierrez G. A Novel Predictive Machine Learning Model Integrating Cytokines in Cervical-Vaginal Mucus Increases the Prediction Rate for Preterm Birth. International Journal of Molecular Sciences. 2023; 24(18):13851. https://doi.org/10.3390/ijms241813851
Chicago/Turabian StyleBorboa-Olivares, Hector, Maria Jose Rodríguez-Sibaja, Aurora Espejel-Nuñez, Arturo Flores-Pliego, Jonatan Mendoza-Ortega, Ignacio Camacho-Arroyo, Ramón González-Camarena, Juan Carlos Echeverría-Arjonilla, and Guadalupe Estrada-Gutierrez. 2023. "A Novel Predictive Machine Learning Model Integrating Cytokines in Cervical-Vaginal Mucus Increases the Prediction Rate for Preterm Birth" International Journal of Molecular Sciences 24, no. 18: 13851. https://doi.org/10.3390/ijms241813851
APA StyleBorboa-Olivares, H., Rodríguez-Sibaja, M. J., Espejel-Nuñez, A., Flores-Pliego, A., Mendoza-Ortega, J., Camacho-Arroyo, I., González-Camarena, R., Echeverría-Arjonilla, J. C., & Estrada-Gutierrez, G. (2023). A Novel Predictive Machine Learning Model Integrating Cytokines in Cervical-Vaginal Mucus Increases the Prediction Rate for Preterm Birth. International Journal of Molecular Sciences, 24(18), 13851. https://doi.org/10.3390/ijms241813851