
Association of HDL Subfraction Profile with the Progression of Insulin Resistance
 , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Study Groups
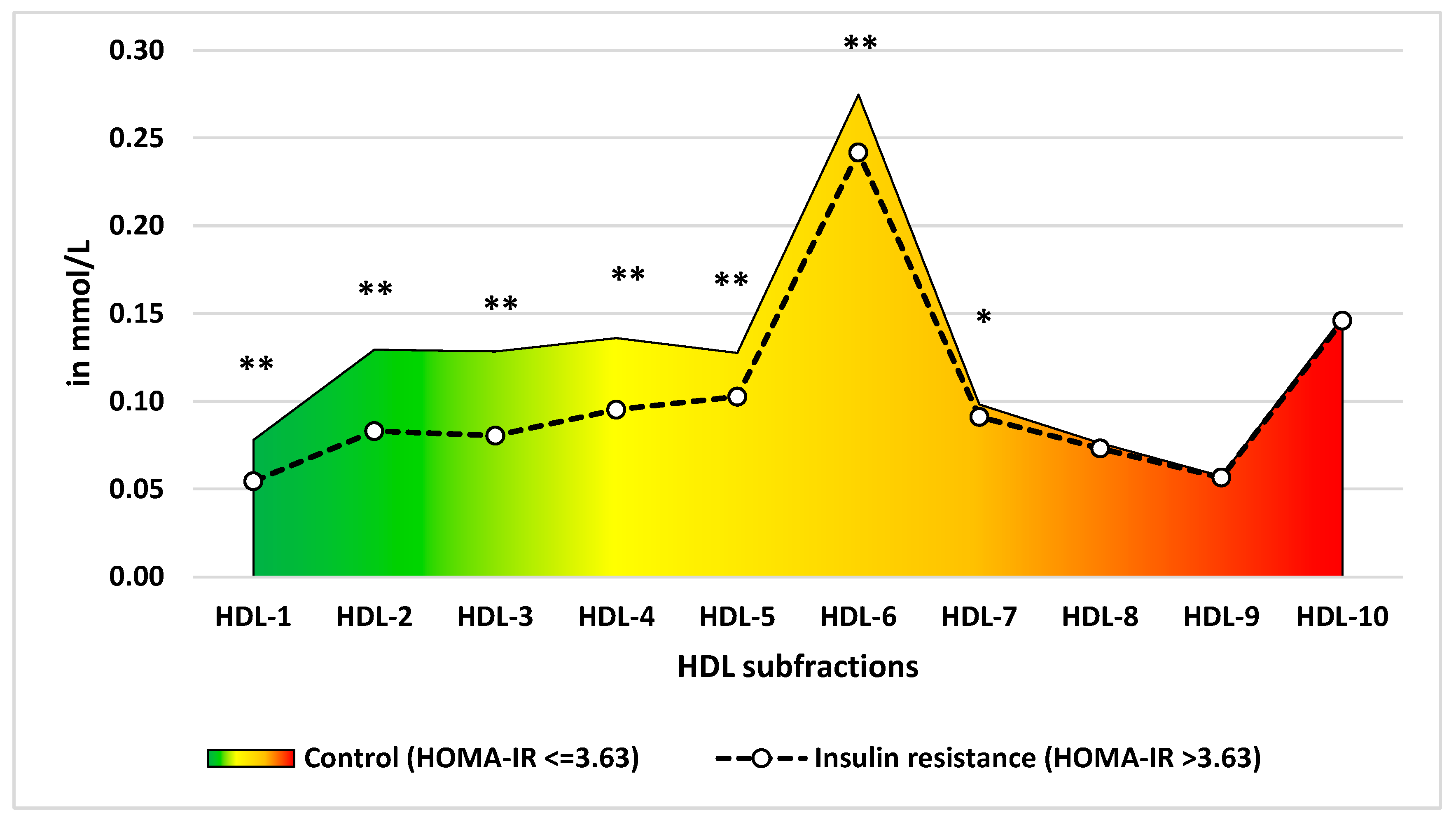
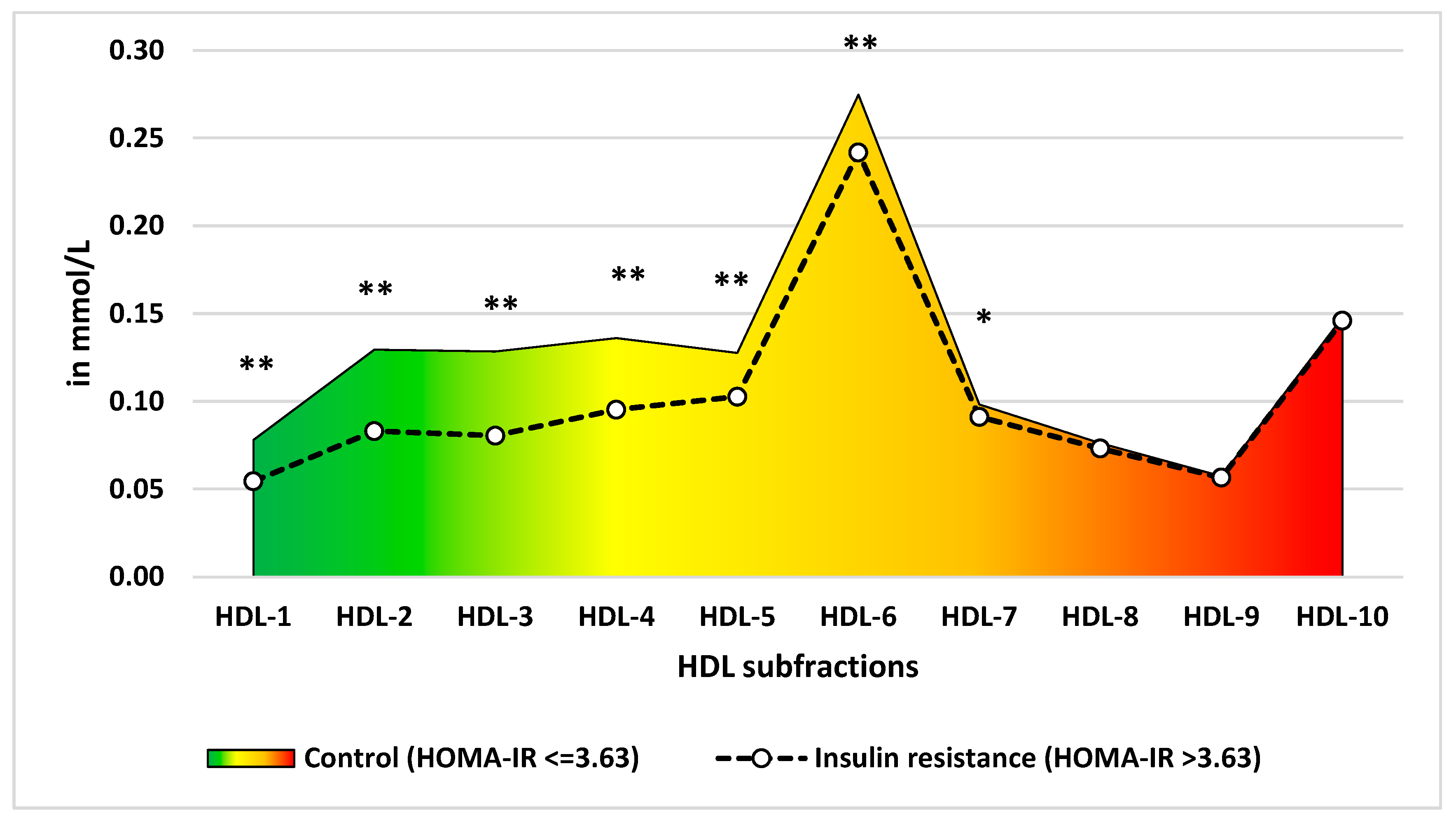
2.2. Comparison of HDL Subfractionation Profile between the IR and Control Groups
2.3. Association of HDL and Its Subfractions with Fasting Insulin, Fasting Glucose Levels and HbA1c
2.4. Association of HDL and Its Subfractions with HOMA-IR Levels and Insulin Resistance
2.5. Determination of Optimal Cut-Off Points and Their Association with the Risk of Insulin Resistance
3. Discussion
4. Materials and Methods
4.1. Study Design and Populations
4.2. Analysis of HDL Subfractions
4.3. Data Used to Identify Insulin Resistance
4.4. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Assoc, A.D. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2009, 32, S62–S67. [Google Scholar] [CrossRef]
- Martín-Timón, I.; Sevillano-Collantes, C.; Segura-Galindo, A.; Del Cañizo-Gómez, F.J. Type 2 diabetes and cardiovascular disease: Have all risk factors the same strength? World J. Diabetes 2014, 5, 444–470. [Google Scholar] [CrossRef]
- Freeman, A.M.; Pennings, N. Insulin Resistance. In StatPearls; StatPearls Publishing Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Jellinger, P.S. Metabolic consequences of hyperglycemia and insulin resistance. Clin. Cornerstone 2007, 8 (Suppl. 7), S30–S42. [Google Scholar] [CrossRef]
- Parhofer, K.G. Interaction between Glucose and Lipid Metabolism: More than Diabetic Dyslipidemia. Diabetes Metab. J. 2015, 39, 353–362. [Google Scholar] [CrossRef]
- Podlipskyte, A.; Kazukauskiene, N.; Varoneckas, G.; Mickuviene, N. Association of Insulin Resistance With Cardiovascular Risk Factors and Sleep Complaints: A 10-Year Follow-Up. Front. Public Health 2022, 10, 848284. [Google Scholar] [CrossRef]
- Siebel, A.L.; Heywood, S.E.; Kingwell, B.A. HDL and glucose metabolism: Current evidence and therapeutic potential. Front. Pharmacol. 2015, 6, 258. [Google Scholar] [CrossRef]
- Jomard, A.; Osto, E. High Density Lipoproteins: Metabolism, Function, and Therapeutic Potential. Front. Cardiovasc. Med. 2020, 7, 39. [Google Scholar] [CrossRef]
- Generoso, G.; Bensenor, I.M.; Santos, R.D.; Staniak, H.L.; Sharovsky, R.; Santos, I.S.; Goulart, A.C.; Jones, S.R.; Kulkarni, K.R.; Blaha, M.J.; et al. High-density Lipoprotein-cholesterol Subfractions and Coronary Artery Calcium: The ELSA-Brasil Study. Arch. Med. Res. 2019, 50, 362–367. [Google Scholar] [CrossRef]
- Maeda, S.; Nakanishi, S.; Yoneda, M.; Awaya, T.; Yamane, K.; Hirano, T.; Kohno, N. Associations between Small Dense LDL, HDL Subfractions (HDL2, HDL3) and Risk of Atherosclerosis in Japanese-Americans. J. Atheroscler. Thromb. 2012, 19, 444–452. [Google Scholar] [CrossRef]
- Lappegard, K.T.; Kjellmo, C.A.; Hovland, A. High-Density Lipoprotein Subfractions: Much Ado about Nothing or Clinically Important? Biomedicines 2021, 9, 836. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.; Muniz, N.; Di Guida, O. Evaluation of HDL subclasses using the Lipoprint (R) HDL system. Clin. Chem. 2006, 52, A118. [Google Scholar]
- Rosenson, R.S.; Brewer, H.B.; Chapman, M.J.; Fazio, S.; Hussain, M.M.; Kontush, A.; Krauss, R.M.; Otvos, J.D.; Remaley, A.T.; Schaefer, E.J. HDL Measures, Particle Heterogeneity, Proposed Nomenclature, and Relation to Atherosclerotic Cardiovascular Events. Clin. Chem. 2011, 57, 392–410. [Google Scholar] [CrossRef]
- Fisher, E.A.; Feig, J.E.; Hewing, B.; Hazen, S.L.; Smith, J.D. High-Density Lipoprotein Function, Dysfunction, and Reverse Cholesterol Transport. Arter. Thromb. Vasc. Biol. 2012, 32, 2813–2820. [Google Scholar] [CrossRef] [PubMed]
- Sasahara, T.; Nestel, P.; Fidge, N.; Sviridov, D. Cholesterol transport between cells and high density lipoprotein subfractions from obese and lean subjects. J. Lipid Res. 1998, 39, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.A.; McQueen, J. Reverse cholesterol transport—A review of the process and its clinical implications. Clin. Biochem. 1997, 30, 517–525. [Google Scholar] [CrossRef]
- Connelly, M.A.; Klein, S.M.; Azhar, S.; Abumrad, N.A.; Williams, D.L. Comparison of class B scavenger receptors, CD36 and scavenger receptor BI (SR-BI), shows that both receptors mediate high density lipoprotein-cholesteryl ester selective uptake but SR-BI exhibits a unique enhancement of cholesteryl ester uptake. J. Biol. Chem. 1999, 274, 41–47. [Google Scholar] [CrossRef]
- Annema, W.; Tietge, U.J.F. Regulation of reverse cholesterol transport—A comprehensive appraisal of available animal studies. Nutr. Metab. 2012, 9, 25. [Google Scholar] [CrossRef]
- Graversen, J.H.; Castro, G.; Kandoussi, A.; Nielsen, H.; Christensen, E.I.; Norden, A.; Moestrup, S.K. A pivotal role of the human kidney in catabolism of HDL protein components apolipoprotein A-I and A-IV but not of A-II. Lipids 2008, 43, 467–470. [Google Scholar] [CrossRef]
- Tran-Dinh, A.; Diallo, D.; Delbosc, S.; Varela-Perez, L.M.; Dang, Q.B.; Lapergue, B.; Burillo, E.; Michel, J.B.; Levoye, A.; Martin-Ventura, J.L.; et al. HDL and endothelial protection. Br. J. Pharmacol. 2013, 169, 493–511. [Google Scholar] [CrossRef]
- Bajer, B.; Radikova, Z.; Havranova, A.; Zitnanova, I.; Vlcek, M.; Imrich, R.; Sabaka, P.; Bendzala, M.; Penesova, A. Effect of 8-weeks intensive lifestyle intervention on LDL and HDL subfractions. Obes. Res. Clin. Pract. 2019, 13, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Manichukal, A.; Goff, D.C.; Mora, S.; Ordovas, J.M.; Pajewski, N.M.; Post, W.S.; Rotter, J.I.; Sale, M.M.; Santorico, S.A.; et al. Genetic associations with lipoprotein subfraction measures differ by ethnicity in the multi-ethnic study of atherosclerosis (MESA). Hum. Genet. 2017, 136, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Nikolic, D.; Katsiki, N.; Montalto, G.; Isenovic, E.R.; Mikhailidis, D.P.; Rizzo, M. Lipoprotein Subfractions in Metabolic Syndrome and Obesity: Clinical Significance and Therapeutic Approaches. Nutrients 2013, 5, 928–948. [Google Scholar] [CrossRef] [PubMed]
- Iwani, A.K.N.Z.; Jalaludin, M.Y.; Yahya, A.; Mansor, F.; Zain, F.M.; Hong, J.Y.H.; Zin, R.M.W.M.; Mokhtar, A.H. TG: HDL-C Ratio as Insulin Resistance Marker for Metabolic Syndrome in Children With Obesity. Front. Endocrinol. 2022, 13, 852290. [Google Scholar] [CrossRef]
- Chauhan, A.; Singhal, A.; Goyal, P. TG/HDL Ratio: A marker for insulin resistance and atherosclerosis in prediabetics or not? J. Fam. Med. Prim. Care 2021, 10, 3700–3705. [Google Scholar] [CrossRef] [PubMed]
- Eng, D.; Gregg, B.; Singer, K.; Lee, J.M. TG/HDL Ratio as a Predictor of Insulin Resistance in US Adolescents: Do Age and Sex Percentiles Matter? Diabetes 2022, 71. [Google Scholar] [CrossRef]
- Generoso, G.; Bensenor, I.M.; Santos, R.D.; Santos, I.S.; Goulart, A.C.; Jones, S.R.; Kulkarni, K.R.; Blaha, M.J.; Toth, P.P.; Lotufo, P.A.; et al. Association between high-density lipoprotein subfractions and low-grade inflammation, insulin resistance, and metabolic syndrome components: The ELSA-Brasil study. J. Clin. Lipidol. 2018, 12, 1290–1297. [Google Scholar] [CrossRef]
- Hsu, H.; Hsu, P.; Cheng, M.H.; Ito, Y.; Kanda, E.; Schaefer, E.J.; Ai, M. Lipoprotein Subfractions and Glucose Homeostasis in Prediabetes and Diabetes in Taiwan. J. Atheroscler. Thromb. 2019, 26, 890–914. [Google Scholar] [CrossRef]
- Ochoa-Guzmán, A.; Guillén-Quintero, D.; Muñoz-Hernández, L.; García, A.; Díaz-Díaz, E.; Pérez-Méndez, O.; Rodríguez-Guillén, R.; Mitre-Aguilar, I.B.; Zentella-Dehesa, A.; Aguilar-Salinas, C.A.; et al. The influence of high-density lipoprotein (HDL) and HDL subfractions on insulin secretion and cholesterol efflux in pancreatic derived β-cells. J. Endocrinol. Investig. 2021, 44, 1897–1904. [Google Scholar] [CrossRef]
- Piko, P.; Kosa, Z.; Sandor, J.; Seres, I.; Paragh, G.; Adany, R. The profile of HDL-C subfractions and their association with cardiovascular risk in the Hungarian general and Roma populations. Sci. Rep. 2022, 12, 10915. [Google Scholar] [CrossRef]
- Moriyama, K.; Negami, M.; Takahashi, E. HDL2-cholesterol/HDL3-cholesterol ratio was associated with insulin resistance, high-molecular-weight adiponectin, and components for metabolic syndrome in Japanese. Diabetes Res. Clin. Pr. 2014, 106, 360–365. [Google Scholar] [CrossRef]
- Mattock, M.B.; Salter, A.M.; Fuller, J.H.; Omer, T.; Elgohari, R.; Redmond, S.D.; Keen, H. High-Density Lipoprotein Subfractions in Insulin-Dependent Diabetic and Normal Subjects. Atherosclerosis 1982, 45, 67–79. [Google Scholar] [CrossRef]
- Durrington, P.N. Serum High-Density Lipoprotein Cholesterol Subfractions in Type-I (Insulin-Dependent) Diabetes-Mellitus. Clin. Chim. Acta 1982, 120, 21–28. [Google Scholar] [CrossRef]
- Brunham, L.R.; Kruit, J.K.; Hayden, M.R.; Verchere, C.B. Cholesterol in beta-cell Dysfunction: The Emerging Connection Between HDL Cholesterol and Type 2 Diabetes. Curr. Diabetes Rep. 2010, 10, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Hoang, H.H.; Padgham, S.V.; Meininger, C.J. L-arginine, tetrahydrobiopterin, nitric oxide and diabetes. Curr. Opin. Clin. Nutr. 2013, 16, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Mineo, C.; Shaul, P.W. Regulation of Enos in Caveolae. Adv. Exp. Med. Biol. 2012, 729, 51–62. [Google Scholar] [CrossRef]
- Vallance, P.; Chan, N. Endothelial function and nitric oxide: Clinical relevance. Heart 2001, 85, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Cutuli, L.; Pirillo, A.; Uboldi, P.; Kuehn, H.; Catapano, A.L. 15-Lipoxygenase-Mediated Modification of HDL3 Impairs eNOS Activation in Human Endothelial Cells. Lipids 2014, 49, 317–326. [Google Scholar] [CrossRef]
- Kontush, A. HDL particle number and size as predictors of cardiovascular disease. Front. Pharmacol. 2015, 6, 218. [Google Scholar] [CrossRef]
- Li, J.J.; Zhang, Y.; Li, S.; Cui, C.J.; Zhu, C.G.; Guo, Y.L.; Wu, N.Q.; Xu, R.X.; Liu, G.; Dong, Q.; et al. Large HDL Subfraction But Not HDL-C Is Closely Linked With Risk Factors, Coronary Severity and Outcomes in a Cohort of Nontreated Patients With Stable Coronary Artery Disease: A Prospective Observational Study. Medicine 2016, 95, e2600. [Google Scholar] [CrossRef]
- McGarrah, R.W.; Craig, D.M.; Haynes, C.; Dowdy, Z.E.; Shah, S.H.; Kraus, W.E. High-density lipoprotein subclass measurements improve mortality risk prediction, discrimination and reclassification in a cardiac catheterization cohort. Atherosclerosis 2016, 246, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Woudberg, N.J.; Goedecke, J.H.; Blackhurst, D.; Frias, M.; James, R.; Opie, L.H.; Lecour, S. Association between ethnicity and obesity with high-density lipoprotein (HDL) function and subclass distribution. Lipids Health Dis. 2016, 15, 92. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C.; D’Agostino, R.B.; Haffner, S.M.; Otvos, J.D. Insulin resistance and adiposity influence lipoprotein size and subclass concentrations. Results from the Insulin Resistance Atherosclerosis Study. Metabolism 2005, 54, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Stancakova, A.; Soininen, P.; Kangas, A.J.; Paananen, J.; Kuusisto, J.; Ala-Korpela, M.; Laakso, M. Lipoprotein subclass profiles in individuals with varying degrees of glucose tolerance: A population-based study of 9399 Finnish men. J. Intern. Med. 2012, 272, 562–572. [Google Scholar] [CrossRef]
- Dullaart, R.P.F.; Otvos, J.D.; James, R.W. Serum paraoxonase-1 activity is more closely related to HDL particle concentration and large HDL particles than to HDL cholesterol in Type 2 diabetic and non-diabetic subjects. Clin. Biochem. 2014, 47, 1022–1027. [Google Scholar] [CrossRef]
- Adany, R.; Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Biro, E.; Kosa, K.; Paragh, G.; Bacsne Baba, E.; Veres-Balajti, I.; et al. Prevalence of Insulin Resistance in the Hungarian General and Roma Populations as Defined by Using Data Generated in a Complex Health (Interview and Examination) Survey. Int. J. Environ. Res. Public Health 2020, 17, 4833. [Google Scholar] [CrossRef]
- Chary, A.; Hedayati, M. Review of Laboratory Methods to Determine HDL and LDL Subclasses and Their Clinical Importance. Rev. Cardiovasc. Med. 2022, 23, 147. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Tobin, J.D.; Andres, R. Glucose clamp technique: A method for quantifying insulin secretion and resistance. Am. J. Physiol. 1979, 237, E214–E223. [Google Scholar] [CrossRef]
- Singh, Y.; Garg, M.K.; Tandon, N.; Marwaha, R.K. A Study of Insulin Resistance by HOMA-IR and its Cut-off Value to Identify Metabolic Syndrome in Urban Indian Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 245–251. [Google Scholar] [CrossRef]
- Horakova, D.; Stepanek, L.; Janout, V.; Janoutova, J.; Pastucha, D.; Kollarova, H.; Petrakova, A.; Stepanek, L.; Husar, R.; Martinik, K. Optimal Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) Cut-Offs: A Cross-Sectional Study in the Czech Population. Medicina 2019, 55, 158. [Google Scholar] [CrossRef]
- Rajala, U.; Laakso, M.; Paivansalo, M.; Pelkonen, O.; Suramo, I.; Keinanen-Kiukaanniemi, S. Low insulin sensitivity measured by both quantitative insulin sensitivity check index and homeostasis model assessment method as a risk factor of increased intima-media thickness of the carotid artery. J. Clin. Endocrinol. Metab. 2002, 87, 5092–5097. [Google Scholar] [CrossRef] [PubMed]
- Ruopp, M.D.; Perkins, N.J.; Whitcomb, B.W.; Schisterman, E.F. Youden index and optimal cut-point estimated from observations affected by a lower limit of detection. Biom. J. 2008, 50, 419–430. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Control (HOMA-IR ≤ 3.63) n = 240 | Insulin Resistance (HOMA-IR > 3.63) n = 137 | p-Value | |
|---|---|---|---|
| Mean (95%CI) | |||
| Age (in years) | 40.73 (39.16–42.29) | 41.47 (39.42–43.53) | 0.552 |
| BMI (kg/m2) | 25.86 (25.15–26.56) | 30.62 (29.59–31.66) | <0.001 * |
| Fasting glucose (mg/dL) | 82.54 (80.77–84.31) | 112.66 (105.90–119.41) | <0.001 * |
| Fasting insulin (mU/L) | 8.43 (9.91–8.95) | 37.92 (33.34–42.50) | <0.001 * |
| HbA1c (%) | 5.33 (5.27–5.40) | 5.77 (5.61–5.93) | <0.001 * |
| Fasting LDL-C (mmol/L) | 2.87 (2.77–2.96) | 3.16 (2.97–3.34) | 0.007 * |
| Fasting TAG (mmol/L) | 1.35 (1.24–1.47) | 2.24 (2.04–2.44) | <0.001 * |
| Systolic BP (mmHg) | 121.80 (119.77–123.84) | 126.68 (124.17–129.19) | 0.002 * |
| Prevalence in % (95%CI) | p-Value | ||
| Roma ethnicity | 57.08 (50.77–63.23) | 54.74 (46.38–62.91) | 0.660 |
| Women | 67.08 (60.96–72.80) | 66.42 (58.24–73.92) | 0.896 |
| Antihypertensive treatment | 21.25 (16.44–26.75) | 34.31 (26.75–42.52) | 0.005 * |
| Antidiabetic treatment | 2.92 (1.31–5.64) | 14.60 (9.45–21.23) | <0.001 * |
| Current smoker | 56.49 (50.15–62.66) | 50.74 (42.39–59.05) | 0.282 |
| Fasting Insulin Level (U/dL) | Fasting Glucose Level (mmol/L) | HbA1c (%) | ||||
|---|---|---|---|---|---|---|
| B (SE) | p-Value | B (SE) | p-Value | B (SE) | p-Value | |
| HDL-C | −16.55 (2.79) | 7.45 × 10−9 ** | 0.28 (0.23) | 0.224 | −0.22 (0.10) | 0.028 * |
| HDL-1 | −120.25 (27.39) | 1.50 × 10−5 ** | 3.66 (2.14) | 0.088 | −2.52 (0.95) | 0.008 * |
| HDL-2 | −104.92 (16.42) | 5.65 × 10−10 ** | 0.51 (1.37) | 0.711 | −1.05 (0.61) | 0.087 |
| HDL-3 | −78.47 (15.41) | 5.81 × 10−7 ** | −0.60 (1.24) | 0.629 | −0.67 (0.55) | 0.229 |
| HDL-4 | −72.03 (16.76) | 2.20 × 10−5 ** | −2.12 (1.31) | 0.106 | 0.25 (0.60) | 0.669 |
| HDL-5 | −123.69 (26.09) | 0.30 × 10−6 ** | −2.07 (2.07) | 0.318 | −0.65 (0.93) | 0.485 |
| HDL-6 | −72.75 (15.13) | 2.00 × 10−6 ** | 2.65 (1.19) | 0.026 * | −1.45 (0.53) | 0.006 * |
| HDL-7 | −141.19 (36.48) | 1.29 × 10−4 ** | 10.30 (2.74) | 1.96 × 10−4 ** | −3.74 (1.24) | 0.003 ** |
| HDL-8 | −129.89 (45.31) | 0.004 ** | 11.92 (3.35) | 4.23 × 10−4 ** | −3.28 (1.54) | 0.033 * |
| HDL-9 | −71.28 (56.85) | 0.211 | 8.37 (4.23) | 0.049 * | −1.50 (1.91) | 0.434 |
| HDL-10 | −14.80 (19.25) | 0.443 | 1.73 (1.43) | 0.229 | −0.54 (0.64) | 0.406 |
| Large HDL | −38.72 (6.64) | 1.23 × 10−8 ** | 0.21 (0.54) | 0.696 | −0.46 (0.24) | 0.059 |
| Intermediate HDL | −30.06 (5.65) | 1.80 × 10−7 ** | 0.44 (0.45) | 0.331 | −0.40 (0.20) | 0.049 * |
| Small HDL | −16.40 (12.21) | 0.180 | 1.93 (0.91) | 0.034 * | −0.55 (0.41) | 0.182 |
| HOMA-IR | Insulin Resistance (HOMA-IR ≥ 3.63) | |||
|---|---|---|---|---|
| B (SE) | p-Value | B (SE) | p-Value | |
| HDL-C | −5.75 (1.01) | 2.41 × 10−8 ** | −1.91 (0.45) | 2.00 × 10−5 ** |
| HDL-1 | −37.00 (9.99) | 2.45 × 10−4 ** | −8.66 (3.98) | 0.030 * |
| HDL-2 | −40.37 (5.83) | 2.08 × 10−11 ** | −11.26 (2.65) | 2.20 × 10−5 ** |
| HDL-3 | −32.95 (5.41) | 3.01 × 10−9 ** | −8.53 (2.34) | 2.67 × 10−4 ** |
| HDL-4 | −35.07 (5.82) | 4.14 × 10−9 ** | −8.94 (2.51) | 3.70 × 10−4 ** |
| HDL-5 | −54.37 (9.10) | 5.73 × 10−9 ** | −14.85 (3.93) | 1.16 × 10−4 ** |
| HDL-6 | −20.70 (5.53) | 2.14 × 10−4 ** | −7.83 (1.83) | 8.47 × 10−4 ** |
| HDL-7 | −21.73 (13.33) | 0.104 | −11.50 (5.41) | 0.034 * |
| HDL-8 | −10.98 (16.43) | 0.504 | −11.22 (6.64) | 0.091 |
| HDL-9 | −0.95 (20.55) | 0.963 | −9.27 (8.29) | 0.264 |
| HDL-10 | −0.01 (6.90) | 0.999 | −2.51 (2.77) | 0.364 |
| Large HDL | −14.85 (2.36) | 9.52 × 10−10 ** | −3.85 (1.03) | 1.99 × 10−4 ** |
| Intermediate HDL | −10.66 (2.03) | 2.80 × 10−7 ** | −3.43 (0.89) | 1.13 × 10−4 ** |
| Small HDL | 0.09 (4.40) | 0.984 | −2.37 (1.78) | 0.183 |
| AUC | Sens./Spec. | Youden Index | Optimal Cut-Off Point (in mmol/L) | |
|---|---|---|---|---|
| HDL-C | 0.715 | 0.696/0.628 | 0.324 | 1.045 |
| HDL-1 | 0.676 | 0.646/0.679 | 0.325 | 0.057 |
| HDL-2 | 0.722 | 0.579/0.796 | 0.375 | 0.102 |
| HDL-3 | 0.715 | 0.621/0.737 | 0.358 | 0.093 |
| HDL-4 | 0.709 | 0.567/0.803 | 0.370 | 0.113 |
| HDL-5 | 0.711 | 0.692/0.672 | 0.363 | 0.106 |
| HDL-6 | 0.661 | 0.633/0.620 | 0.254 | 0.250 |
| HDL-7 | 0.584 | 0.796/0.365 | 0.161 | 0.082 |
| HDL-8 | 0.540 | 0.821/0.285 | 0.106 | 0.060 |
| HDL-9 | 0.504 | 0.850/0.234 | 0.084 | 0.043 |
| HDL-10 | 0.507 | 0.296/0.752 | 0.048 | 0.173 |
| Large HDL | 0.723 | 0.604/0.803 | 0.407 | 0.264 |
| Intermediate HDL | 0.699 | 0.546/0.781 | 0.327 | 0.584 |
| Small HDL | 0.518 | 0.625/0.431 | 0.056 | 0.253 |
| HOMA-IR | Insulin Resistance (HOMA-IR ≥ 3.63) | |||
|---|---|---|---|---|
| B (SE) | p-Value | OR (95%CI) | p-Value | |
| HDL-C (<1.045 mmol/L) | 3.22 (0.70) | 5.00 × 10−6 ** | 2.94 (1.71–5.06) | 1.01 × 10−4 ** |
| HDL-1 (<0.057 mmol/L) | 2.48 (0.73) | 7.05 × 10−4 ** | 2.08 (1.21–3.59) | 0.009 * |
| HDL-2 (<0.102 mmol/L) | 4.39 (0.73) | 4.02 × 10−9 ** | 3.81 (2.06–7.02) | 1.80 × 10−5 ** |
| HDL-3 (<0.093 mmol/L) | 3.49 (0.73) | 3.00 × 10−6 ** | 2.87 (1.62–5.10) | 3.09 × 10−4 ** |
| HDL-4 (<0.113 mmol/L) | 3.68 (0.69) | 1.62 × 10−7 ** | 3.80 (2.12–6.80) | 7.00 × 10−6 ** |
| HDL-5 (<0.106 mmol/L) | 3.24 (0.68) | 3.00 × 10−6 ** | 3.03 (1.78–5.16) | 4.3 × 10−5 ** |
| HDL-6 (<0.250 mmol/L) | 2.37 (0.67) | 4.33 × 10−4 ** | 2.37 (1.40–4.02) | 0.001 ** |
| HDL-7 (<0.082 mmol/L) | 1.51 (0.73) | 0.039 * | 2.06 (1.19–3.56) | 0.010 * |
| HDL-8 (<0.060 mmol/L) | 1.85 (0.80) | 0.021 * | 2.22 (1.20–4.10) | 0.011 * |
| HDL-9 (<0.043 mmol/L) | 1.10 (0.85) | 0.198 | 2.00 (1.05–3.83) | 0.036 * |
| HDL-10 (<0.173 mmol/L) | −0.09 (0.73) | 0.905 | 1.28 (0.73–2.24) | 0.393 |
| Large HDL (<0.264 mmol/L) | 4.57 (0.73) | 1.09 × 10−9 ** | 4.73 (2.53–8.86) | 1.00 × 10−6 ** |
| Intermediate HDL (<0.584 mmol/L) | 3.50 (0.65) | 1.55 × 10−7 ** | 3.47 (1.98–6.06) | 1.30 × 10−5 ** |
| Small HDL (<0.253 mmol/L) | 0.08 (0.69) | 0.905 | 1.63 (0.95–2.77) | 0.075 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piko, P.; Jenei, T.; Kosa, Z.; Sandor, J.; Kovacs, N.; Seres, I.; Paragh, G.; Adany, R. Association of HDL Subfraction Profile with the Progression of Insulin Resistance. Int. J. Mol. Sci. 2023, 24, 13563. https://doi.org/10.3390/ijms241713563
Piko P, Jenei T, Kosa Z, Sandor J, Kovacs N, Seres I, Paragh G, Adany R. Association of HDL Subfraction Profile with the Progression of Insulin Resistance. International Journal of Molecular Sciences. 2023; 24(17):13563. https://doi.org/10.3390/ijms241713563
Chicago/Turabian StylePiko, Peter, Tibor Jenei, Zsigmond Kosa, Janos Sandor, Nora Kovacs, Ildiko Seres, Gyorgy Paragh, and Roza Adany. 2023. "Association of HDL Subfraction Profile with the Progression of Insulin Resistance" International Journal of Molecular Sciences 24, no. 17: 13563. https://doi.org/10.3390/ijms241713563
APA StylePiko, P., Jenei, T., Kosa, Z., Sandor, J., Kovacs, N., Seres, I., Paragh, G., & Adany, R. (2023). Association of HDL Subfraction Profile with the Progression of Insulin Resistance. International Journal of Molecular Sciences, 24(17), 13563. https://doi.org/10.3390/ijms241713563