
miRNA-Seq Tissue Diagnostic Signature: A Novel Model for NSCLC Subtyping

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
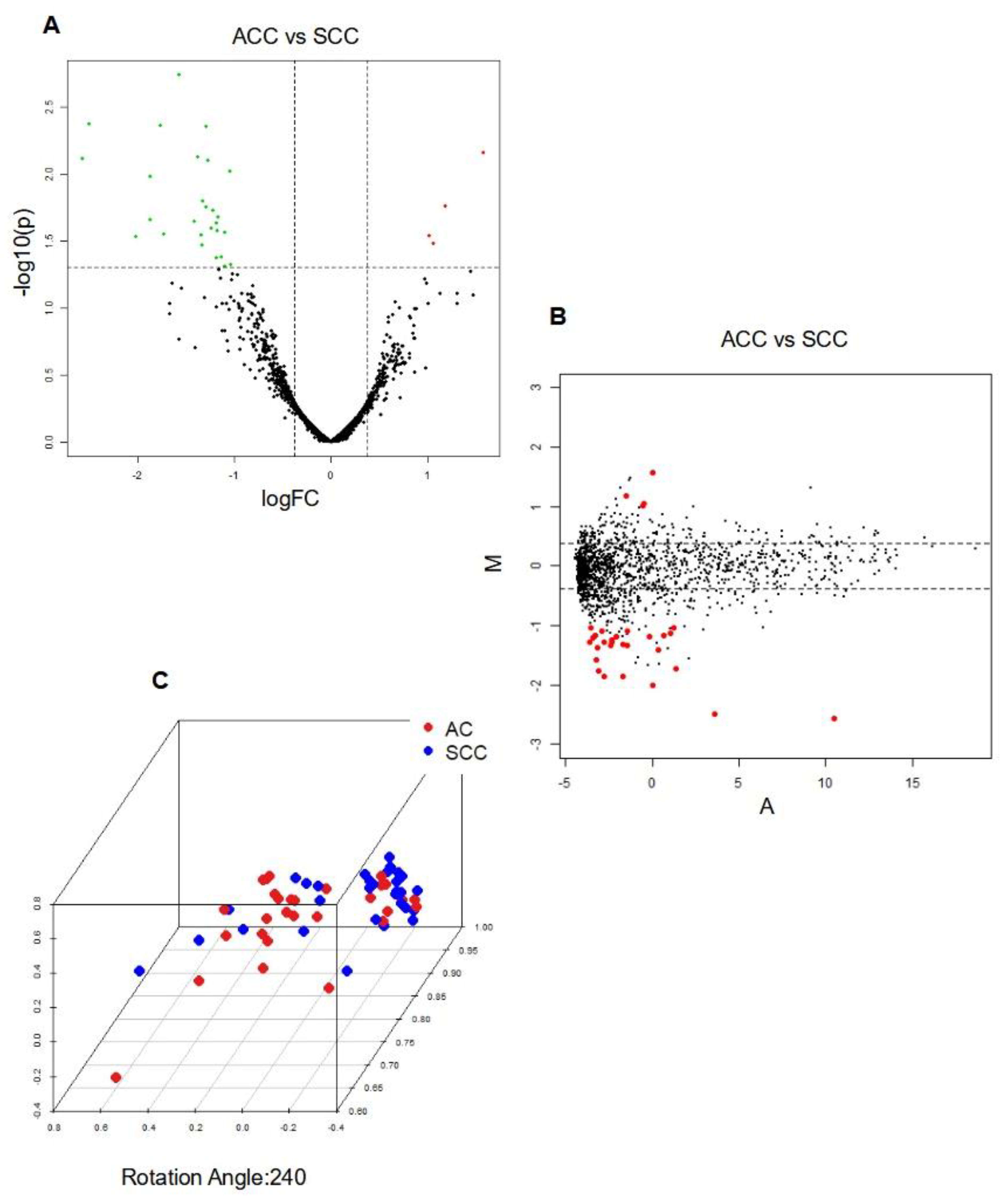
2.1. Differentially Expressed miRNA to Differentiate AC from SCC
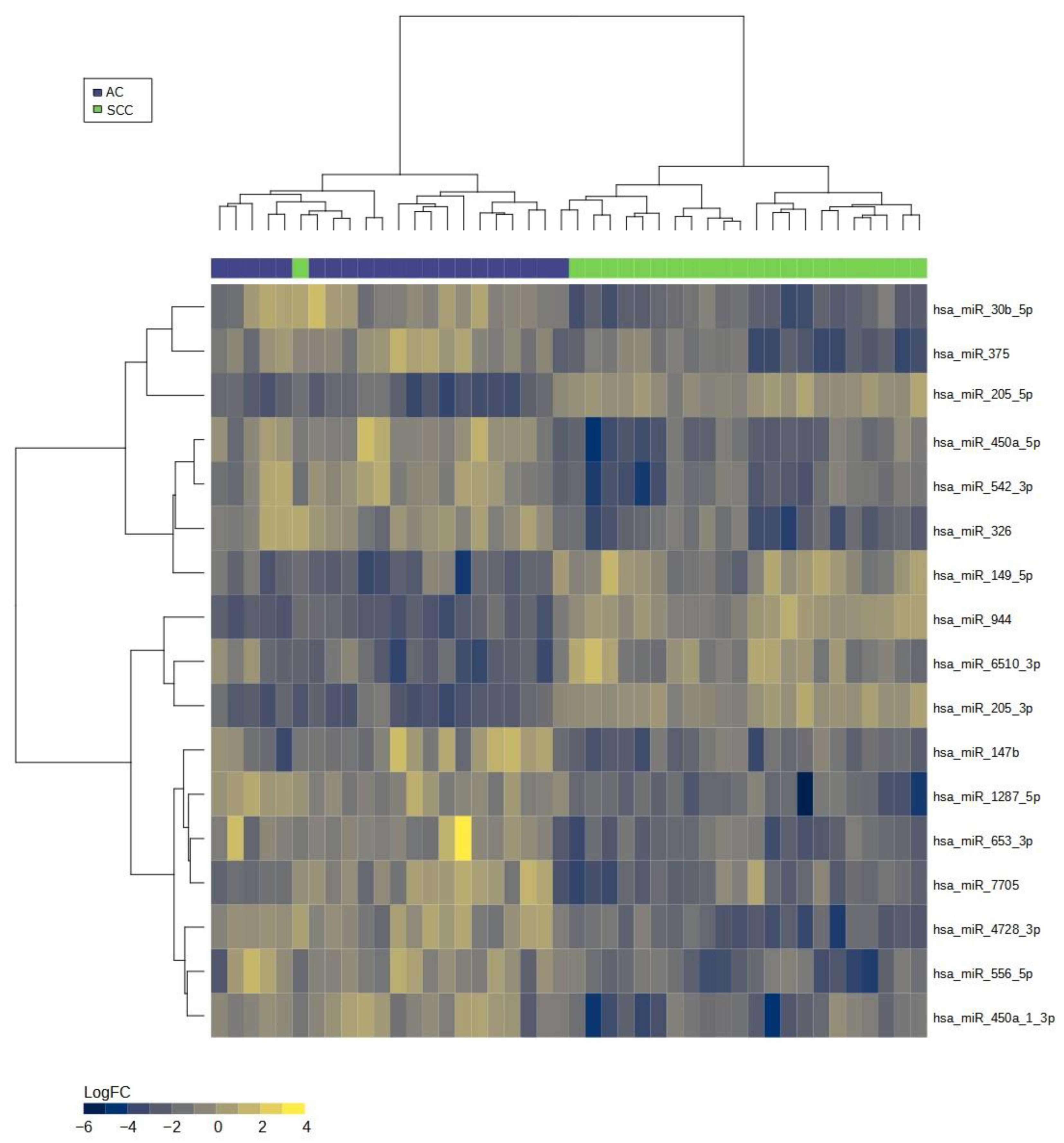
2.2. miRNA Signature to Differentiate AC from SCC
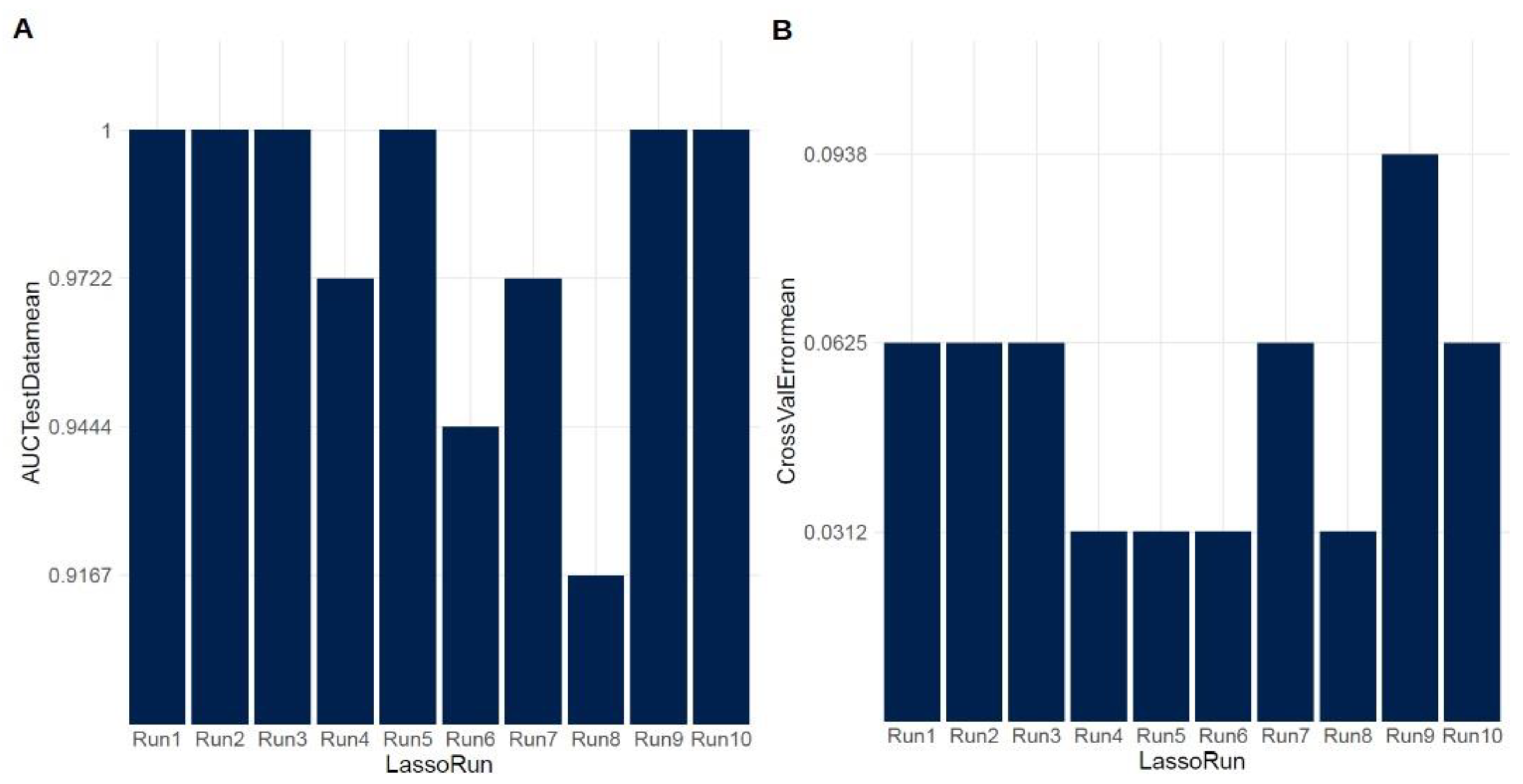
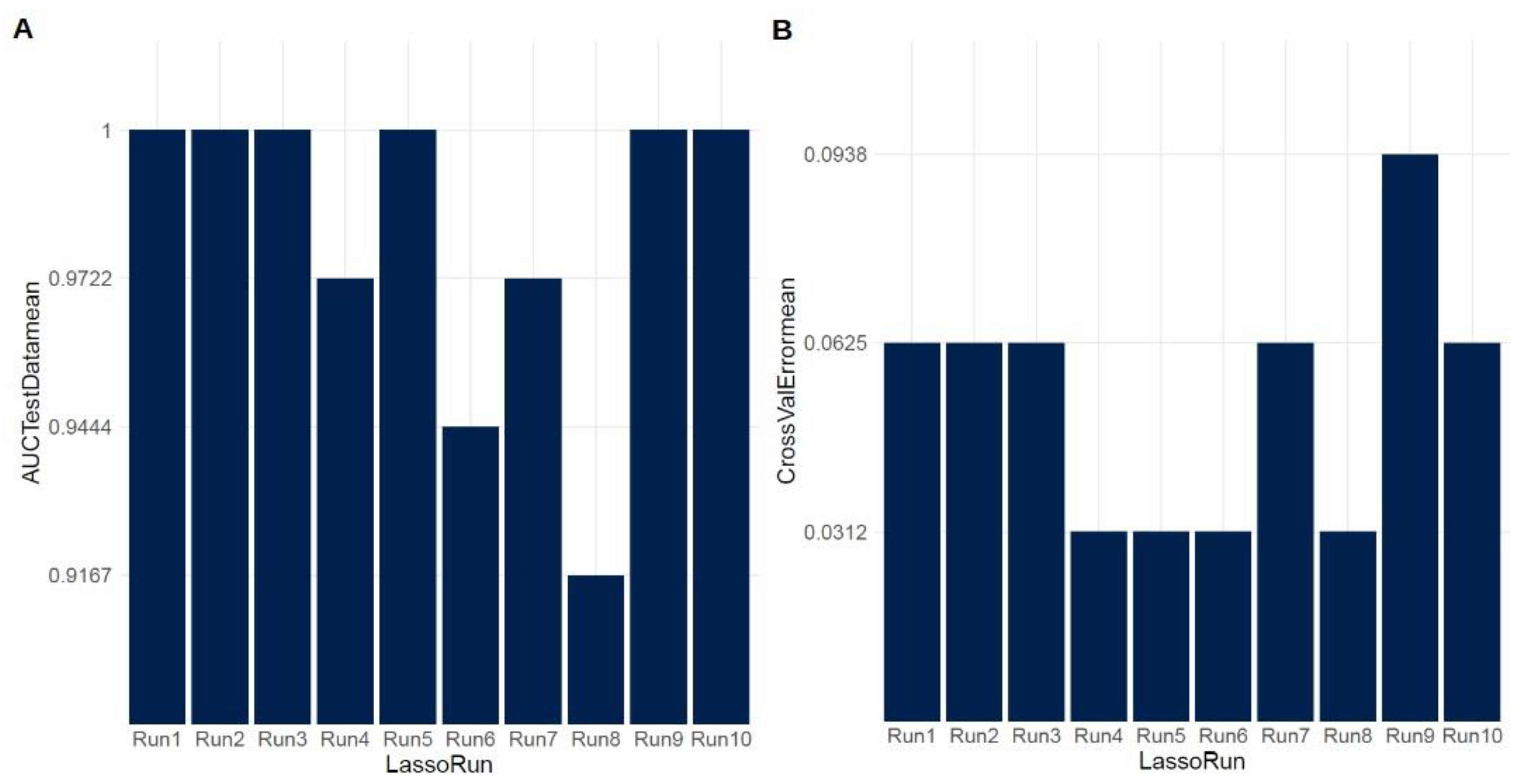
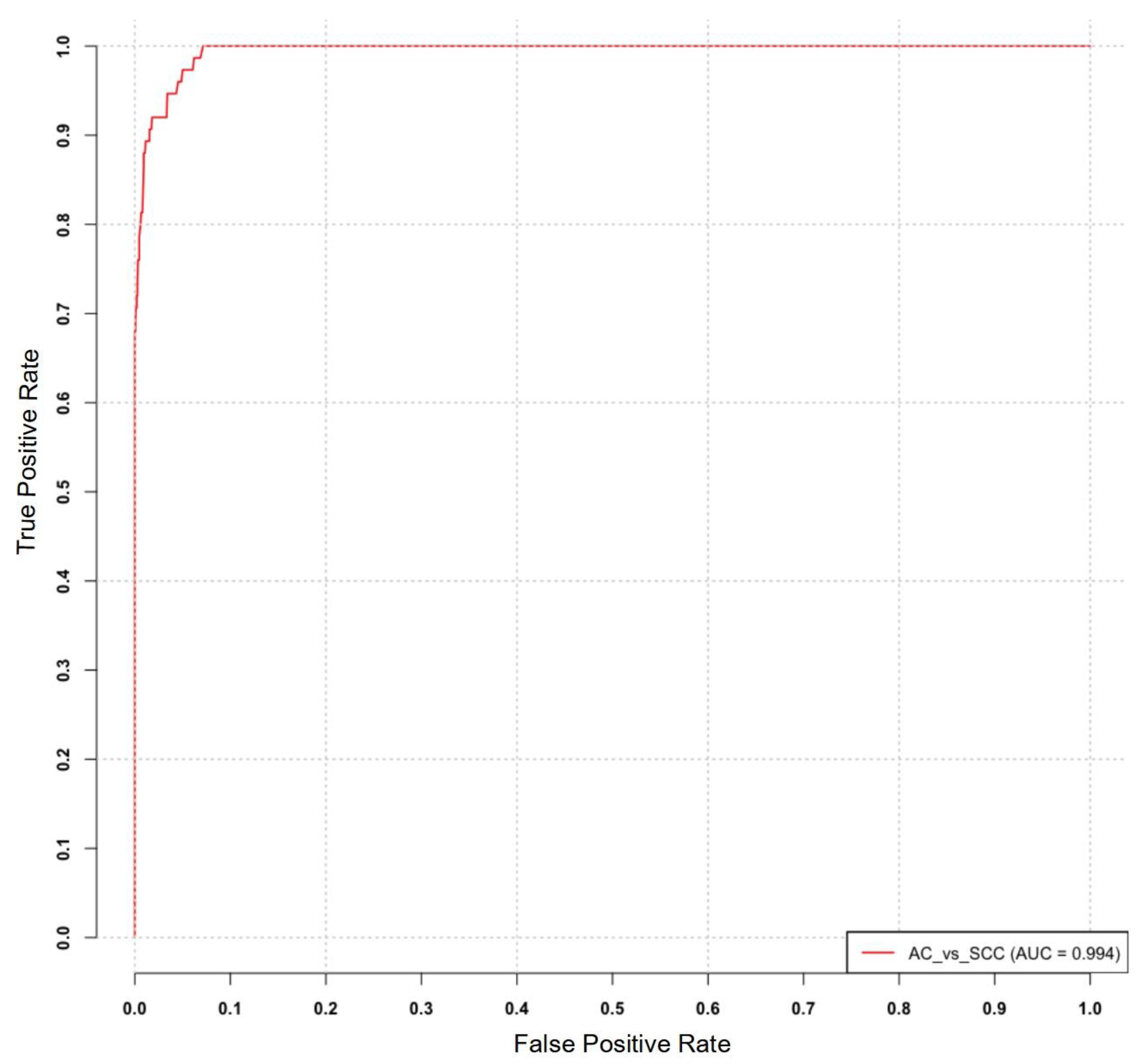
2.3. Evaluation of the Diagnostic Utility of the Identified miRNA Signature
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
4.2. Histopathological Diagnosis
4.3. RNA Isolation and Quality Control
4.4. Next Generation Sequencing Analysis
4.5. Bioinformatic Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, A.; Kumar, A. Non-small-cell lung cancer-associated gene mutations and inhibitors. Adv. Cancer Biol.—Metastasis 2022, 6, 100076. [Google Scholar] [CrossRef]
- Yang, S.; Huang, Y.; Zhao, Q. Epigenetic Alterations and Inflammation as Emerging Use for the Advancement of Treatment in Non-Small Cell Lung Cancer. Front. Immunol. 2022, 13, 878740. [Google Scholar] [CrossRef]
- Sulewska, A.; Pilz, L.; Manegold, C.; Ramlau, R.; Charkiewicz, R.; Niklinski, J. A Systematic Review of Progress toward Unlocking the Power of Epigenetics in NSCLC: Latest Updates and Perspectives. Cells 2023, 12, 905. [Google Scholar] [CrossRef]
- Zhong, S.; Golpon, H.; Zardo, P.; Borlak, J. miRNAs in lung cancer. A systematic review identifies predictive and prognostic miRNA candidates for precision medicine in lung cancer. Transl. Res. 2021, 230, 164–196. [Google Scholar] [CrossRef]
- Du, X.; Zhang, J.; Wang, J.; Lin, X.; Ding, F. Role of miRNA in Lung Cancer-Potential Biomarkers and Therapies. Curr. Pharm. Des. 2018, 23, 5997–6010. [Google Scholar] [CrossRef]
- Charkiewicz, R.; Pilz, L.; Sulewska, A.; Kozlowski, M.; Niklinska, W.; Moniuszko, M.; Reszec, J.; Manegold, C.; Niklinski, J. Validation for histology-driven diagnosis in non-small cell lung cancer using hsa-miR-205 and hsa-miR-21 expression by two different normalization strategies. Int. J. Cancer 2016, 138, 689–697. [Google Scholar] [CrossRef]
- Haranguș, A.; Lajos, R.; Budisan, L.; Zanoaga, O.; Ciocan, C.; Bica, C.; Pirlog, R.; Simon, I.; Simon, M.; Braicu, C.; et al. Identification of Potential microRNA Panels for Male Non-Small Cell Lung Cancer Identification Using Microarray Datasets and Bioinformatics Methods. J. Pers. Med. 2022, 12, 2056. [Google Scholar] [CrossRef]
- Imyanitov, E.N.; Iyevleva, A.G.; Levchenko, E. V Molecular testing and targeted therapy for non-small cell lung cancer: Current status and perspectives. Crit. Rev. Oncol. Hematol. 2021, 157, 103194. [Google Scholar] [CrossRef]
- Viñal, D.; Martínez, D.; Higuera, O.; Castro, J. de Genomic profiling in non-small-cell lung cancer in young patients. A systematic review. ESMO Open 2021, 6, 100045. [Google Scholar] [CrossRef]
- De Maglio, G.; Pasello, G.; Dono, M.; Follador, M.F.A.; Sciortino, M.; Malapelle, U.; Tiseo, M. The storm of NGS in NSCLC diagnostic-therapeutic pathway: How to sun the real clinical practice. Crit. Rev. Oncol. Hematol. 2022, 169, 103561. [Google Scholar] [CrossRef]
- Hussen, B.M.; Abdullah, S.T.; Salihi, A.; Sabir, D.K.; Sidiq, K.R.; Rasul, M.F.; Hidayat, H.J.; Ghafouri-Fard, S.; Taheri, M.; Jamali, E. The emerging roles of NGS in clinical oncology and personalized medicine. Pathol.—Res. Pract. 2022, 230, 153760. [Google Scholar] [CrossRef]
- Tane, S.; Nishio, W.; Ogawa, H.; Hokka, D.; Tane, K.; Tanaka, Y.; Tauchi, S.; Uchino, K.; Sakai, Y.; Ohbayashi, C.; et al. Clinical significance of the “not otherwise specified” subtype in candidates for resectable non-small cell lung cancer. Oncol. Lett. 2014, 8, 1017–1024. [Google Scholar] [CrossRef]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Herbst, R.S.; Heymach, J.V.; Lippman, S.M. Lung cancer. N. Engl. J. Med. 2008, 359, 1367–1380. [Google Scholar] [CrossRef]
- Shroff, G.S.; de Groot, P.M.; Papadimitrakopoulou, V.A.; Truong, M.T.; Carter, B.W. Targeted Therapy and Immunotherapy in the Treatment of Non-Small Cell Lung Cancer. Radiol. Clin. N. Am. 2018, 56, 485–495. [Google Scholar] [CrossRef]
- Sculier, J.-P.; Berghmans, T.; Meert, A.-P. Advances in target therapy in lung cancer. Eur. Respir. Rev. 2015, 24, 23–29. [Google Scholar] [CrossRef]
- Pal, S.K.; Figlin, R.A.; Reckamp, K. Targeted therapies for non-small cell lung cancer: An evolving landscape. Mol. Cancer Ther. 2010, 9, 1931–1944. [Google Scholar] [CrossRef]
- Lauro, S.; Onesti, C.E.; Righini, R.; Marchetti, P. The use of bevacizumab in non-small cell lung cancer: An update. Anticancer Res. 2014, 34, 1537–1545. [Google Scholar]
- Chen, Z.; Akbay, E.; Mikse, O.; Tupper, T.; Cheng, K.; Wang, Y.; Tan, X.; Altabef, A.; Woo, S.-A.; Chen, L.; et al. Co-clinical trials demonstrate superiority of crizotinib to chemotherapy in ALK-rearranged non-small cell lung cancer and predict strategies to overcome resistance. Clin. Cancer Res. 2014, 20, 1204–1211. [Google Scholar] [CrossRef]
- Thakur, M.K.; Wozniak, A.J. Spotlight on necitumumab in the treatment of non-small-cell lung carcinoma. Lung Cancer 2017, 8, 13–19. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Herbst, R.S.; Mann, H.; Rukazenkov, Y.; Marotti, M.; Tsuboi, M. ADAURA: Phase III, Double-blind, Randomized Study of Osimertinib Versus Placebo in EGFR Mutation-positive Early-stage NSCLC after Complete Surgical Resection. Clin. Lung Cancer 2018, 19, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Charkiewicz, R.; Niklinski, J.; Claesen, J.; Sulewska, A.; Kozlowski, M.; Michalska-Falkowska, A.; Reszec, J.; Moniuszko, M.; Naumnik, W.; Niklinska, W. Gene Expression Signature Differentiates Histology But Not Progression Status of Early-Stage NSCLC. Transl. Oncol. 2017, 10, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Sulewska, A.; Niklinski, J.; Charkiewicz, R.; Karabowicz, P.; Biecek, P.; Baniecki, H.; Kowalczuk, O.; Kozlowski, M.; Modzelewska, P.; Majewski, P.; et al. A Signature of 14 Long Non-Coding RNAs (lncRNAs) as a Step towards Precision Diagnosis for NSCLC. Cancers 2022, 14, 439. [Google Scholar] [CrossRef] [PubMed]
- Villalobos, P.; Wistuba, I.I. Lung Cancer Biomarkers. Hematol. Oncol. Clin. N. Am. 2017, 31, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.W.; Dhahbi, J. Lung adenocarcinoma and lung squamous cell carcinoma cancer classification, biomarker identification, and gene expression analysis using overlapping feature selection methods. Sci. Rep. 2021, 11, 13323. [Google Scholar] [CrossRef]
- Fauteux, F.; Surendra, A.; McComb, S.; Pan, Y.; Hill, J.J. Identification of transcriptional subtypes in lung adenocarcinoma and squamous cell carcinoma through integrative analysis of microarray and RNA sequencing data. Sci. Rep. 2021, 11, 8709. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef]
- Korthauer, K.; Kimes, P.K.; Duvallet, C.; Reyes, A.; Subramanian, A.; Mingxiang, T.; Shukla, C.; Alm, E.J.; Hicks, S.C. A practical guide to methods controlling false discoveries in computational biology. Genome Biol. 2019, 20, 118. [Google Scholar] [CrossRef]
- Van Iterson, M.; Boer, J.M.; Menezes, R.X. Filtering, FDR and power. BMC Bioinform. 2010, 11, 450. [Google Scholar] [CrossRef]
- Lu, Y.; Govindan, R.; Wang, L.; Liu, P.; Goodgame, B.; Wen, W.; Sezhiyan, A.; Pfeifer, J.; Li, Y.; Hua, X.; et al. MicroRNA profiling and prediction of recurrence/relapse-free survival in stage I lung cancer. Carcinogenesis 2012, 33, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, S.; Mallick, R.; Kannisto, E.; Sharma, R.; Bshara, W.; Yendamuri, S.; Dhillon, S.S. MiR-205 and MiR-375 microRNA assays to distinguish squamous cell carcinoma from adenocarcinoma in lung cancer biopsies. J. Thorac. Oncol. 2015, 10, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, E.; Gandellini, P. Unveiling the ups and downs of miR-205 in physiology and cancer: Transcriptional and post-transcriptional mechanisms. Cell Death Dis. 2020, 11, 980. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Wang, Q.; Liang, C.; Su, X.; Ke, Y.; Mao, Y.; Fang, J.; Duan, S. Novel Insights into miR-944 in Cancer. Cancers 2022, 14, 4232. [Google Scholar] [CrossRef] [PubMed]
- An, J.C.; Shi, H.-B.; Hao, W.-B.; Zhu, K.; Ma, B. miR-944 inhibits lung adenocarcinoma tumorigenesis by targeting STAT1 interaction. Oncol. Lett. 2019, 17, 3790–3798. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.-J.; Wan, J.; Wang, C.-B. MiR-326: Promising Biomarker for Cancer. Cancer Manag. Res. 2019, 11, 10411–10418. [Google Scholar] [CrossRef]
- Fan, K.; Spassova, I.; Gravemeyer, J.; Ritter, C.; Horny, K.; Lange, A.; Gambichler, T.; Ødum, N.; Schrama, D.; Schadendorf, D.; et al. Merkel cell carcinoma-derived exosome-shuttle miR-375 induces fibroblast polarization by inhibition of RBPJ and p53. Oncogene 2021, 40, 980–996. [Google Scholar] [CrossRef]
- Wang, R.; Chen, X.; Xu, T.; Xia, R.; Han, L.; Chen, W.; De, W.; Shu, Y. MiR-326 regulates cell proliferation and migration in lung cancer by targeting phox2a and is regulated by HOTAIR. Am. J. Cancer Res. 2016, 6, 173–186. [Google Scholar]
- Cheng, L.; Zhan, B.; Luo, P.; Wang, B. miRNA-375 regulates the cell survival and apoptosis of human non-small cell carcinoma by targeting HER2. Mol. Med. Rep. 2017, 15, 1387–1392. [Google Scholar] [CrossRef]
- Wang, N.; Guo, H.; Dong, Z.; Chen, Q.; Zhang, X.; Shen, W.; Bao, Y.; Wang, X. Establishment and validation of a 7-microRNA prognostic signature for non-small cell lung cancer. Cancer Manag. Res. 2018, 10, 3463–3471. [Google Scholar] [CrossRef]
- Chen, B.; Gao, T.; Yuan, W.; Zhao, W.; Wang, T.-H.; Wu, J. Prognostic Value of Survival of MicroRNAs Signatures in Non-small Cell Lung Cancer. J. Cancer 2019, 10, 5793–5804. [Google Scholar] [CrossRef] [PubMed]
- Cascone, T.; William, W.N., Jr.; Weissferdt, A.; Leung, C.H.; Lin, H.Y.; Pataer, A.; Godoy, M.C.B.; Carter, B.W.; Federico, L.; Reuben, A.; et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: The phase 2 randomized NEOSTAR trial. Nat. Med. 2021, 27, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Chaft, J.E.; Oezkan, F.; Kris, M.G.; Bunn, P.A.; Wistuba, I.I.; Kwiatkowski, D.J.; Owen, D.H.; Tang, Y.; Johnson, B.E.; Lee, J.M.; et al. Neoadjuvant atezolizumab for resectable non-small cell lung cancer: An open-label, single-arm phase II trial. Nat. Med. 2022, 28, 2155–2161. [Google Scholar] [CrossRef]
- Provencio, M.; Nadal, E.; González-Larriba, J.L.; Martínez-Martí, A.; Bernabé, R.; Bosch-Barrera, J.; Casal-Rubio, J.; Calvo, V.; Insa, A.; Ponce, S.; et al. Perioperative Nivolumab and Chemotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Niklinski, J.; Kretowski, A.; Moniuszko, M.; Reszec, J.; Michalska-Falkowska, A.; Niemira, M.; Ciborowski, M.; Charkiewicz, R.; Jurgilewicz, D.; Kozlowski, M.; et al. Systematic biobanking, novel imaging techniques, and advanced molecular analysis for precise tumor diagnosis and therapy: The Polish MOBIT project. Adv. Med. Sci. 2017, 62, 405–413. [Google Scholar] [CrossRef]
- Michalska-Falkowska, A.; Niklinski, J.; Juhl, H.; Sulewska, A.; Kisluk, J.; Charkiewicz, R.; Ciborowski, M.; Ramlau, R.; Gryczka, R.; Piwkowski, C.; et al. Applied Molecular-Based Quality Control of Biobanked Samples for Multi-Omics Approach. Cancers 2023, 15, 3742. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | logFC | FDR adj.P.Val | avgRank | Description |
|---|---|---|---|---|
| hsa-miR-944 | −2.50024399226404 | 0.99998120935031 | 1 | down |
| hsa-miR-205-5p | −2.56409590009272 | 0.99998120935031 | 2 | down |
| hsa-miR-383-5p | −1.76096646669423 | 0.99998120935031 | 3 | down |
| hsa-miR-3927-3p | −1.57116270312205 | 0.99998120935031 | 4 | down |
| hsa-miR-448 | −1.8650361500274 | 0.99998120935031 | 5 | down |
| hsa-miR-3617-5p | 1.58042497541289 | 0.99998120935031 | 6 | up |
| hsa-miR-1911-5p | −1.86824448648207 | 0.99998120935031 | 7 | down |
| hsa-miR-1224-5p | −1.37356958953855 | 0.99998120935031 | 8 | down |
| hsa-miR-205-3p | −2.01278722790899 | 0.99998120935031 | 9 | down |
| hsa-miR-6510-3p | −1.72338907430046 | 0.99998120935031 | 10 | down |
| hsa-miR-3929 | −1.28741708585196 | 0.99998120935031 | 11 | down |
| hsa-miR-4664-3p | −1.32276408748148 | 0.99998120935031 | 12 | down |
| hsa-miR-7974 | −1.40692830818463 | 0.99998120935031 | 13 | down |
| hsa-miR-6515-3p | −1.27296318882511 | 0.99998120935031 | 14 | down |
| hsa-miR-6765-3p | −1.29009752267163 | 0.99998120935031 | 15 | down |
| hsa-miR-4709-5p | 1.18615415483486 | 0.99998120935031 | 16 | up |
| hsa-miR-3616-5p | −1.34533033666886 | 0.99998120935031 | 17 | down |
| hsa-miR-6512-5p | −1.21523532625748 | 0.99998120935031 | 18 | down |
| hsa-miR-5094 | −1.2395769248493 | 0.99998120935031 | 19 | down |
| hsa-miR-6499-5p | −1.33109054696209 | 0.99998120935031 | 20 | down |
| hsa-miR-1248 | −1.16819512153751 | 0.99998120935031 | 23 | down |
| hsa-miR-3128 | −1.18019684918627 | 0.99998120935031 | 24 | down |
| hsa-miR-149-3p | −1.17066684727337 | 0.99998120935031 | 25 | down |
| hsa-miR-6814-5p | −1.03918923933257 | 0.99998120935031 | 27 | down |
| hsa-miR-1305 | −1.18333424370583 | 0.99998120935031 | 28 | down |
| hsa-miR-597-3p | −1.09652869609583 | 0.99998120935031 | 30 | down |
| hsa-miR-3609 | −1.13169522785434 | 0.99998120935031 | 32 | down |
| hsa-miR-1294 | 1.05850886870655 | 0.99998120935031 | 35 | up |
| hsa-miR-5579-3p | −1.0917337298003 | 0.99998120935031 | 37 | down |
| hsa-miR-4636 | 1.01236329971682 | 0.99998120935031 | 39 | up |
| hsa-miR-3200-3p | −1.03714338280713 | 0.99998120935031 | 41 | down |
| qlogFC | AveExpr | t | p-Value | adj.P.Val | B | Name | Direction |
|---|---|---|---|---|---|---|---|
| 1.29 | 4.84 | 4.57 | 4.55 × 10−5 | 0.0051 | 1.73 | hsa-miR-326 | up |
| 1.14 | 7.40 | 4.49 | 5.89 × 10−5 | 0.0055 | 1.48 | hsa-miR-450a-5p | up |
| 1.33 | 2.04 | 4.40 | 7.70 × 10−5 | 0.0057 | 1.23 | hsa-miR-1287-5p | up |
| 1.83 | 1.47 | 4.36 | 8.73 × 10−5 | 0.0057 | 1.11 | hsa-miR-556-5p | up |
| 1.26 | 6.56 | 4.19 | 0.00015 | 0.0081 | 0.59 | hsa-miR-542-3p | up |
| 1.01 | 10.95 | 4.17 | 0.000158 | 0.0081 | 0.54 | hsa-miR-30b-5p | up |
| 1.08 | 0.036 | 4.00 | 0.000265 | 0.0124 | 0.045 | hsa-miR-4728-3p | up |
| 1.24 | 1.07 | 3.95 | 0.0003 | 0.0131 | −0.082 | hsa-miR-450a-1-3p | up |
| 2.61 | 9.06 | 3.57 | 0.00093 | 0.0314 | −1.15 | hsa-miR-375 | up |
| 1.89 | 2.22 | 3.57 | 0.000947 | 0.0314 | −1.16 | hsa-miR-147b | up |
| 1.14 | 2.00 | 3.47 | 0.0012 | 0.0378 | −1.42 | hsa-miR-7705 | up |
| 1.51 | 2.52 | 3.46 | 0.00127 | 0.0378 | −1.44 | hsa-miR-653-3p | up |
| −5.49 | 3.80 | −9.72 | 3.81 × 10−12 | 1.61 × 10−9 | 17.59 | hsa-miR-944 | down |
| −6.19 | 10.90 | −9.59 | 5.72 × 10−12 | 1.61 × 10−9 | 17.20 | hsa-miR-205-5p | down |
| −5.60 | 0.3 | −8.37 | 2.30 × 10−10 | 4.33 × 10−8 | 13.60 | hsa-miR-205-3p | down |
| −2.29 | 6.45 | −5.18 | 6.41 × 10−6 | 0.0009 | 3.63 | hsa-miR-149-5p | down |
| −3.34 | 1.42 | −4.35 | 9.06 × 10−5 | 0.0057 | 1.07 | hsa-miR-6510-3p | down |
| Characteristics | n = 59 | |
|---|---|---|
| Age (years) | Mean ± SD * | 65.64 ± 6.95 |
| Median | 65 | |
| Range | 49–77 | |
| Sex | Female | 23 (39%) |
| Male | 36 (61%) | |
| Tumor stage | IA | 10 (17%) |
| IB | 15 (25.4%) | |
| IIA | 10 (17%) | |
| IIB | 9 (15.2%) | |
| IIIA | 13 (22%) | |
| IIIB | 2 (3.4%) | |
| Histology | SCC | 31 (52.5%) |
| AC | 28 (47.5%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charkiewicz, R.; Sulewska, A.; Charkiewicz, A.; Gyenesei, A.; Galik, B.; Ramlau, R.; Piwkowski, C.; Stec, R.; Biecek, P.; Karabowicz, P.; et al. miRNA-Seq Tissue Diagnostic Signature: A Novel Model for NSCLC Subtyping. Int. J. Mol. Sci. 2023, 24, 13318. https://doi.org/10.3390/ijms241713318
Charkiewicz R, Sulewska A, Charkiewicz A, Gyenesei A, Galik B, Ramlau R, Piwkowski C, Stec R, Biecek P, Karabowicz P, et al. miRNA-Seq Tissue Diagnostic Signature: A Novel Model for NSCLC Subtyping. International Journal of Molecular Sciences. 2023; 24(17):13318. https://doi.org/10.3390/ijms241713318
Chicago/Turabian StyleCharkiewicz, Radoslaw, Anetta Sulewska, Alicja Charkiewicz, Attila Gyenesei, Bence Galik, Rodryg Ramlau, Cezary Piwkowski, Rafal Stec, Przemyslaw Biecek, Piotr Karabowicz, and et al. 2023. "miRNA-Seq Tissue Diagnostic Signature: A Novel Model for NSCLC Subtyping" International Journal of Molecular Sciences 24, no. 17: 13318. https://doi.org/10.3390/ijms241713318
APA StyleCharkiewicz, R., Sulewska, A., Charkiewicz, A., Gyenesei, A., Galik, B., Ramlau, R., Piwkowski, C., Stec, R., Biecek, P., Karabowicz, P., Michalska-Falkowska, A., Miltyk, W., & Niklinski, J. (2023). miRNA-Seq Tissue Diagnostic Signature: A Novel Model for NSCLC Subtyping. International Journal of Molecular Sciences, 24(17), 13318. https://doi.org/10.3390/ijms241713318