
A Novel Multi-Component Formulation Reduces Inflammation In Vitro and Clinically Lessens the Symptoms of Chronic Eczematous Skin

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Results
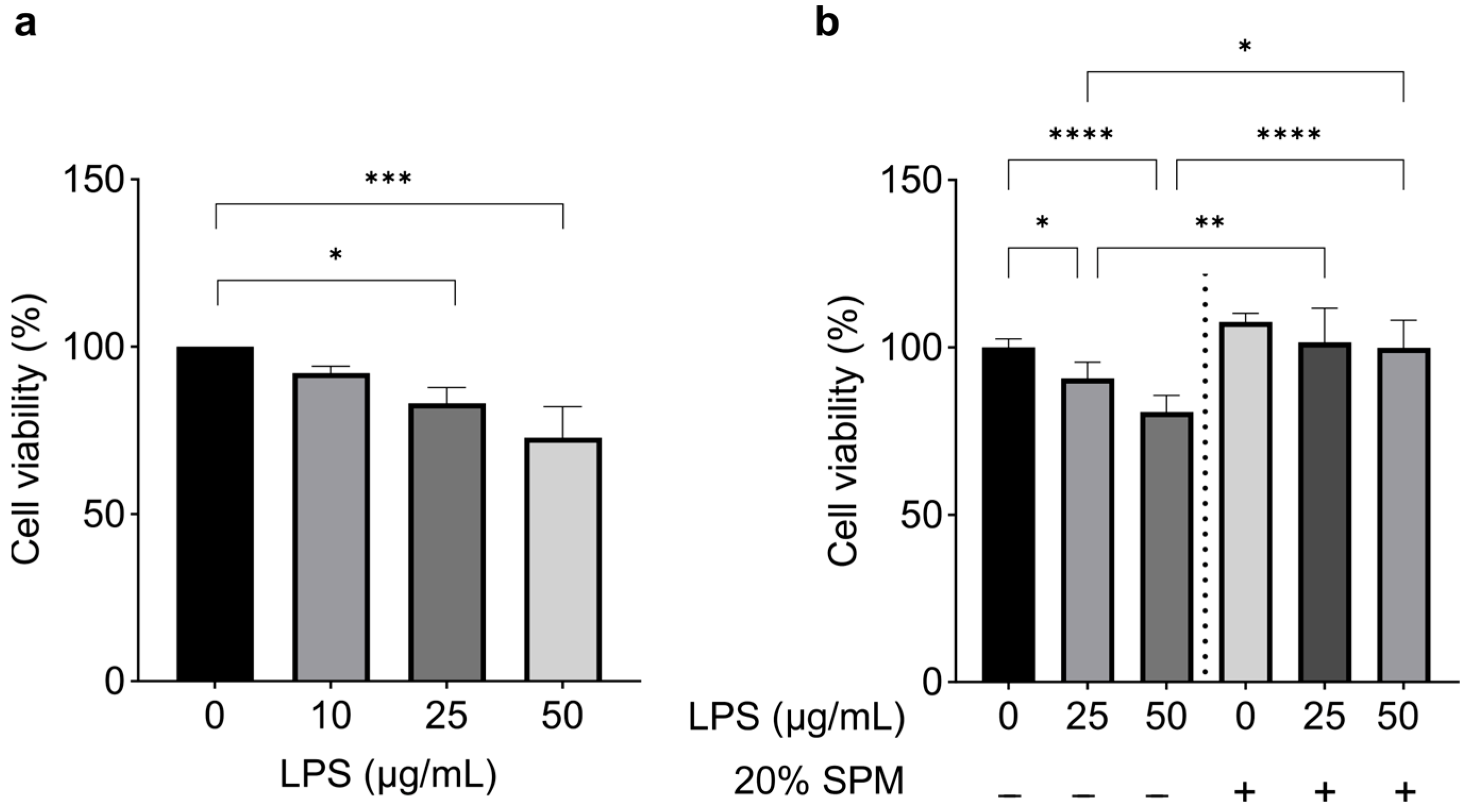
2.1. SPM Treatment Suppresses Inflammatory Response Induced by LPS
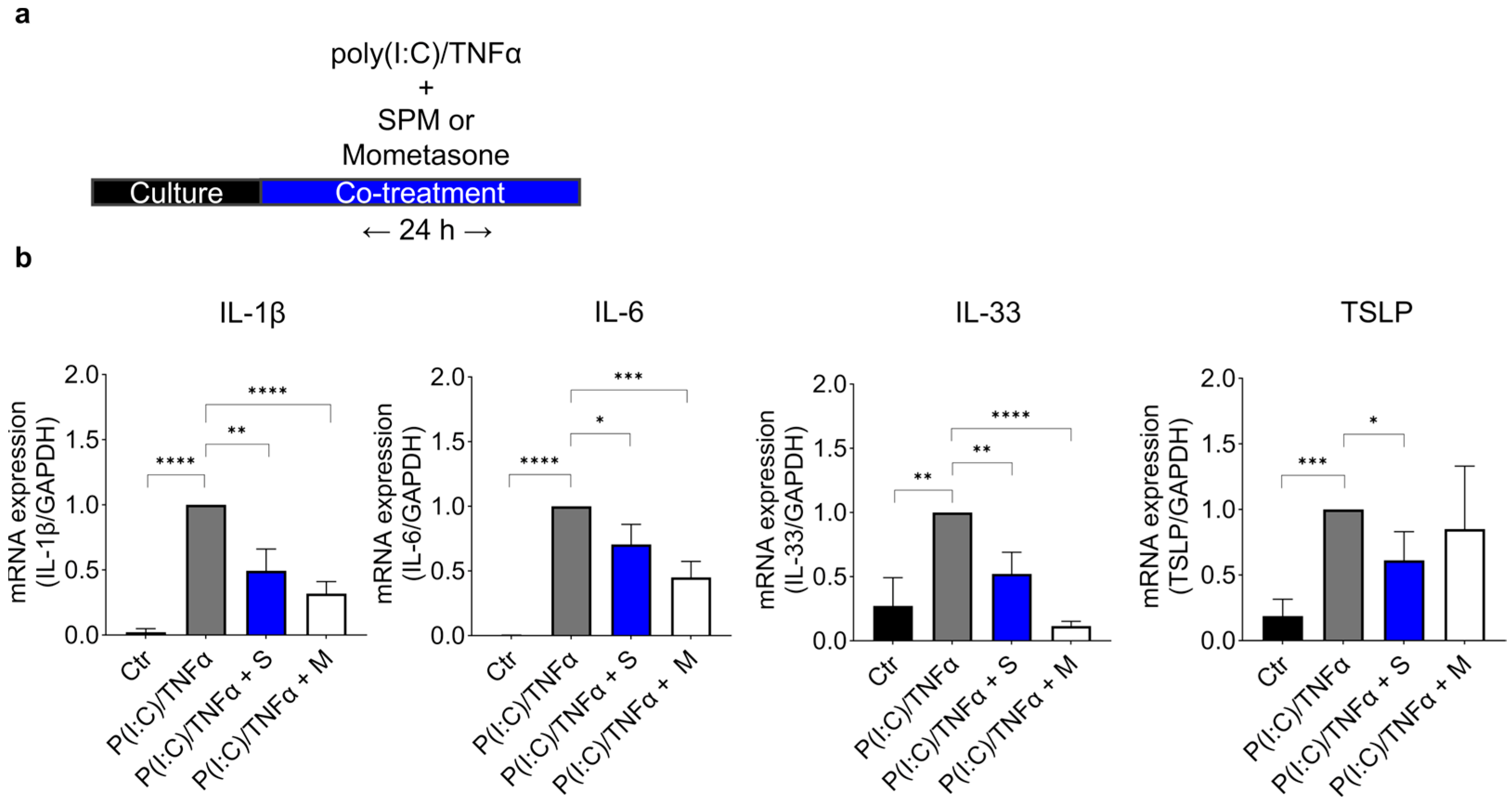
2.2. SPM Treatment Downregulates the Expression of Cytokines Induced by Poly (I:C)/TNFα in HaCaT Cells
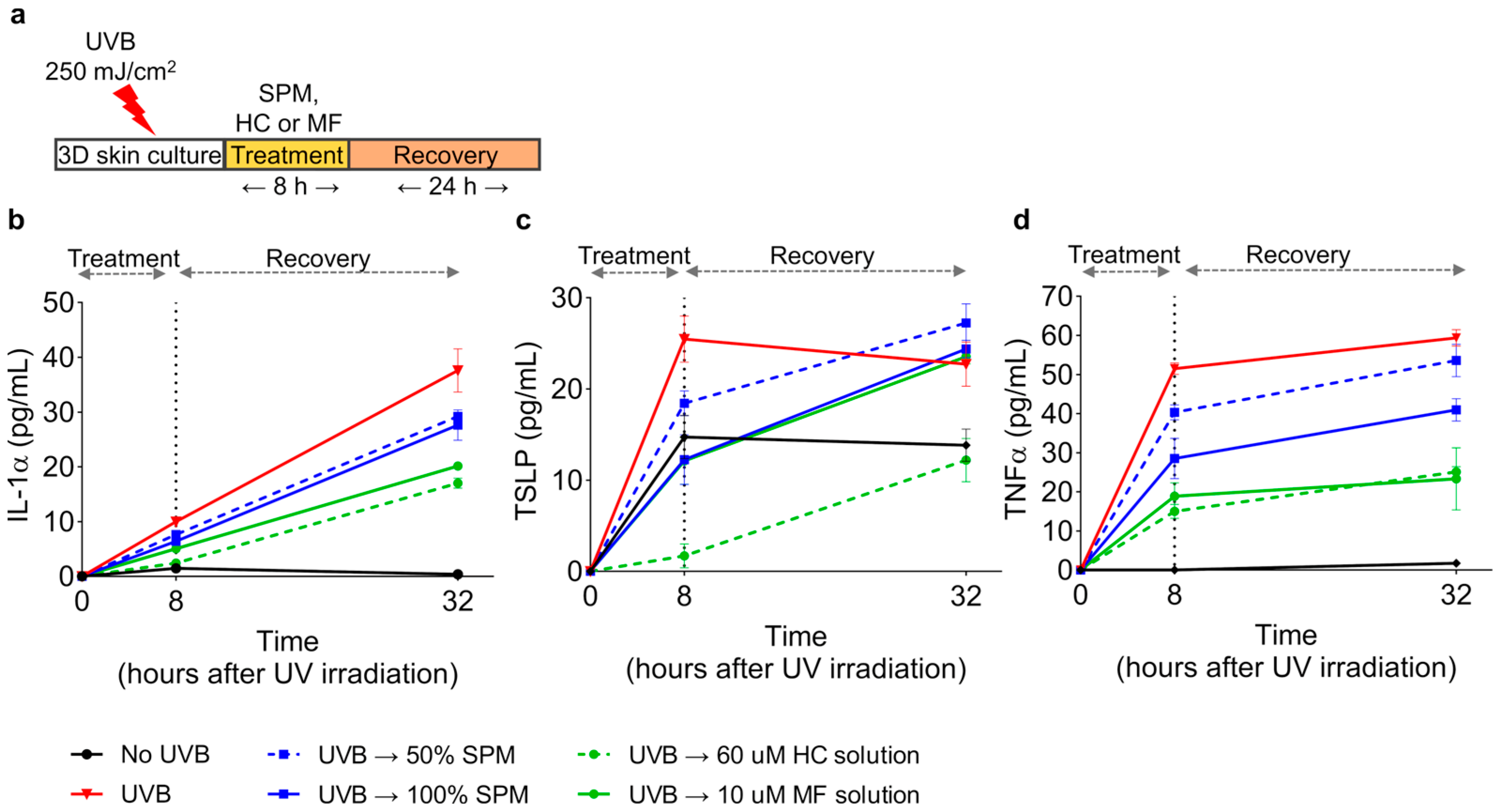
2.3. SPM Suppresses the UVB-Induced Production of Inflammatory Cytokines in a Human Epidermis Model
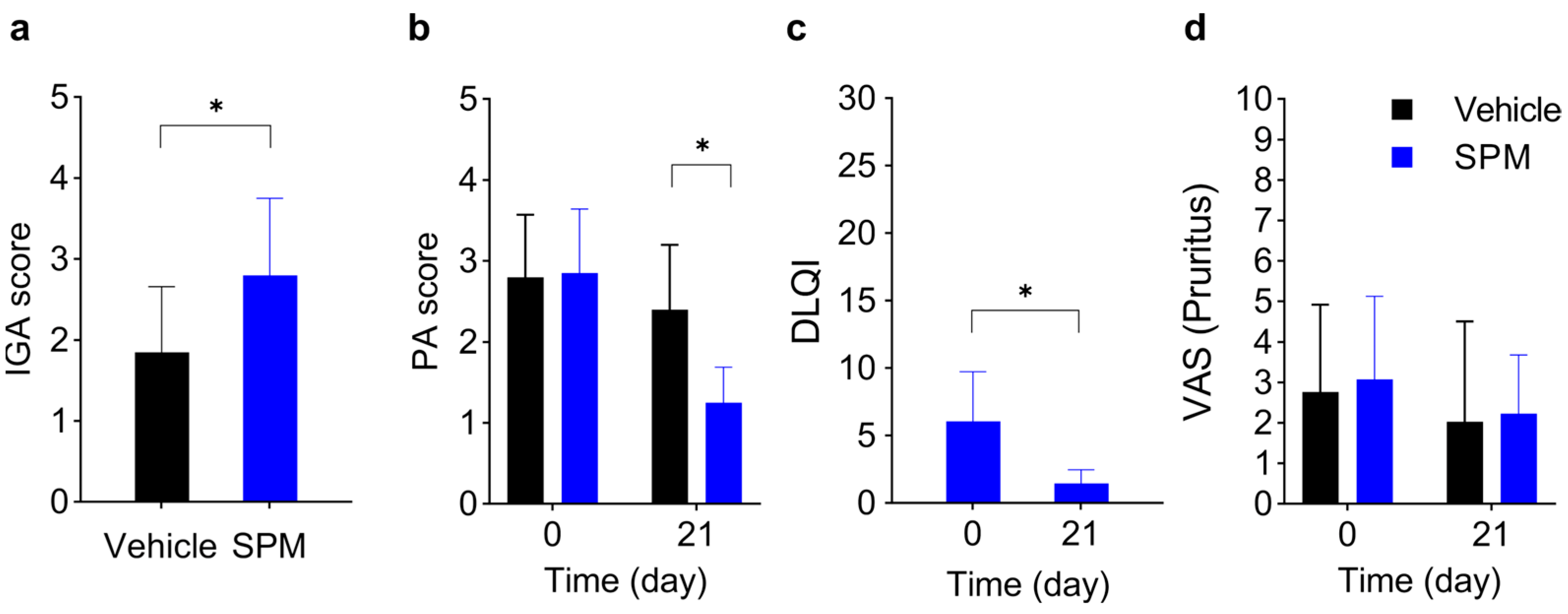
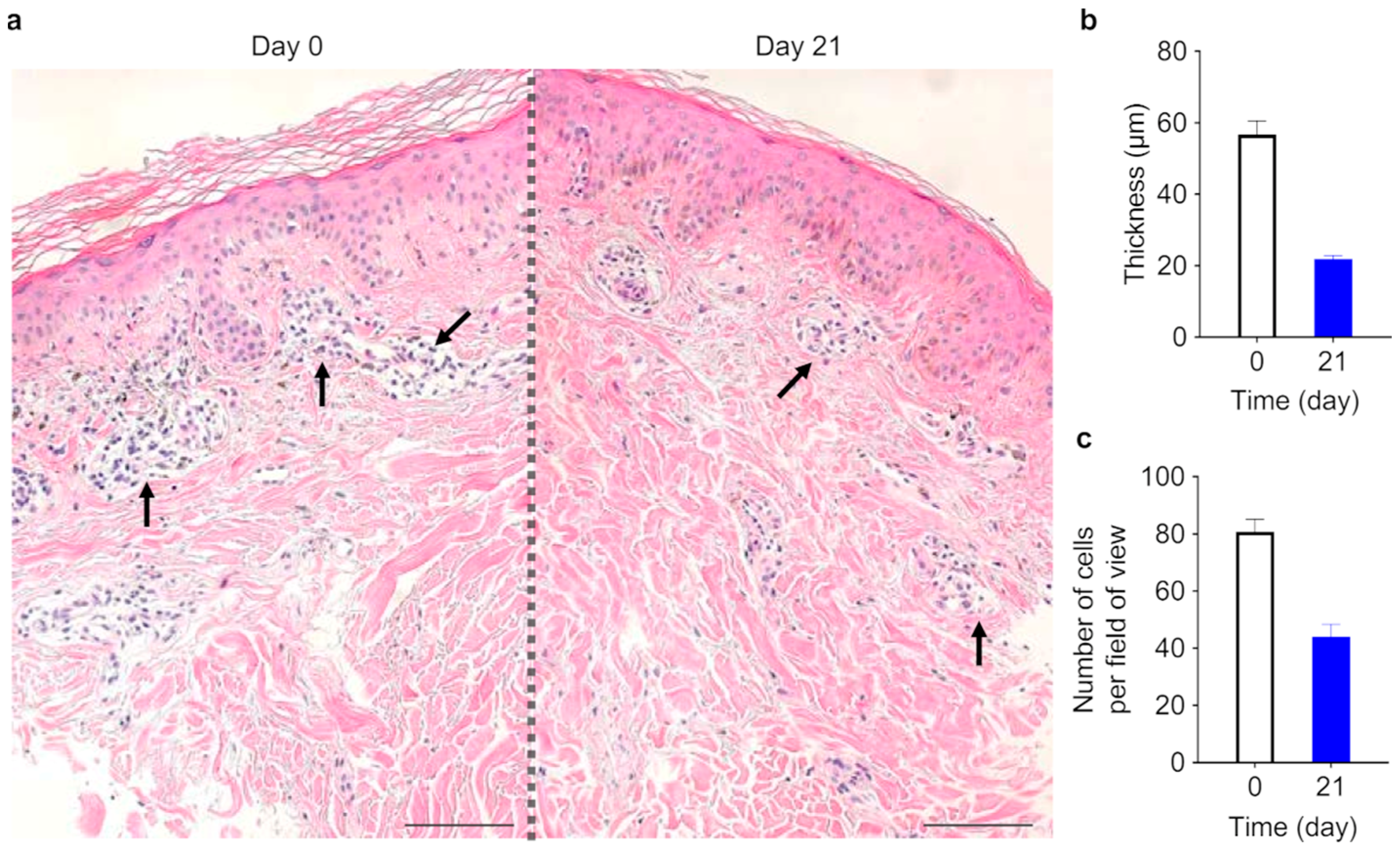
2.4. SPM Ameliorates Symptoms and Signs of Eczematous Dermatitis
3. Discussion
4. Materials and Methods
4.1. Cell Culture
4.2. Cell Viability Assay
4.3. Cell Stimulation
4.4. Human Skin Model
4.5. Enzyme-Linked Immunosorbent Assay (ELISA)
4.6. Statistical Analysis
4.7. Clinical Study
4.8. Statistical Analysis of Clinical Data
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verdier-Sévrain, S.; Bonté, F. Skin Hydration: A Review on Its Molecular Mechanisms. J. Cosmet. Dermatol. 2007, 6, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Tsuchisaka, A.; Furumura, M.; Hashimoto, T. Cytokine Regulation during Epidermal Differentiation and Barrier Formation. J. Investig. Dermatol. 2014, 134, 1194–1196. [Google Scholar] [CrossRef] [PubMed]
- Schröder, J.M. The Role of Keratinocytes in Defense against Infection. Curr. Opin. Infect. Dis. 2010, 23, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Coates, M.; Blanchard, S.; MacLeod, A.S. Innate Antimicrobial Immunity in the Skin: A Protective Barrier against Bacteria, Viruses, and Fungi. PLoS Pathog. 2018, 14, e1007353. [Google Scholar] [CrossRef]
- Handfield, C.; Kwock, J.; MacLeod, A.S. Innate Antiviral Immunity in the Skin. Trends Immunol. 2018, 39, 328–340. [Google Scholar] [CrossRef] [PubMed]
- Kabashima, K.; Honda, T.; Ginhoux, F.; Egawa, G. The Immunological Anatomy of the Skin. Nat. Rev. Immunol. 2019, 19, 19–30. [Google Scholar] [CrossRef]
- Bernard, F.-X.; Morel, F.; Camus, M.; Pedretti, N.; Barrault, C.; Garnier, J.; Lecron, J.-C. Keratinocytes under Fire of Proinflammatory Cytokines: Bona Fide Innate Immune Cells Involved in the Physiopathology of Chronic Atopic Dermatitis and Psoriasis. J. Allergy 2012, 2012, 718725. [Google Scholar] [CrossRef] [PubMed]
- Malajian, D.; Guttman-Yassky, E. New Pathogenic and Therapeutic Paradigms in Atopic Dermatitis. Cytokine 2015, 73, 311–318. [Google Scholar] [CrossRef]
- Asahina, R.; Maeda, S. A Review of the Roles of Keratinocyte-Derived Cytokines and Chemokines in the Pathogenesis of Atopic Dermatitis in Humans and Dogs. Vet. Dermatol. 2017, 28, 16-e5. [Google Scholar] [CrossRef]
- De Vuyst, E.; Salmon, M.; Evrard, C.; de Rouvroit, C.L.; Poumay, Y. Atopic Dermatitis Studies through in Vitro Models. Front. Med. 2017, 4, 119. [Google Scholar] [CrossRef]
- Dainichi, T.; Kitoh, A.; Otsuka, A.; Nakajima, S.; Nomura, T.; Kaplan, D.H.; Kabashima, K. The Epithelial Immune Microenvironment (EIME) in Atopic Dermatitis and Psoriasis. Nat. Immunol. 2018, 19, 1286–1298. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.W.; Kim, Y.J. Cosmetic Composition Containing, as Active Ingredient, Albumin, Hyaluronic Acid or Collagen in Cell Culture Medium. U.S. Patent US011071706B2, 27 July 2021. [Google Scholar]
- Tanno, O.; Ota, Y.; Kitamura, N.; Katsube, T.; Inoue, S. Nicotinamide Increases Biosynthesis of Ceramides as Well as Other Stratum Corneum Lipids to Improve the Epidermal Permeability Barrier. Br. J. Dermatol. 2000, 143, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.L.; Phillips, T.J. Nutrition and Wound Healing. Clin. Dermatol. 2010, 28, 432–439. [Google Scholar] [CrossRef]
- Sinno, S.; Lee, D.S.; Khachemoune, A. Vitamins and Cutaneous Wound Healing. J. Wound Care 2011, 20, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Wohlrab, J.; Kreft, D. Niacinamide-Mechanisms of Action and Its Topical Use in Dermatology. Ski. Pharmacol. Physiol. 2014, 27, 311–315. [Google Scholar] [CrossRef]
- Parra, M.; Stahl, S.; Hellmann, H. Vitamin B6 and Its Role in Cell Metabolism and Physiology. Cells 2018, 7, 84. [Google Scholar] [CrossRef]
- Rembe, J.-D.; Fromm-Dornieden, C.; Stuermer, E.K. Effects of Vitamin B Complex and Vitamin C on Human Skin Cells. Adv. Ski. Wound Care 2018, 31, 225–233. [Google Scholar] [CrossRef]
- Arora, M. Cell Culture Media: A Review. Mater. Methods 2013, 3, 175. [Google Scholar] [CrossRef]
- Chuang, V.T.G.; Kragh-Hansen, U.; Otagiri, M. Pharmaceutical Strategies Utilizing Recombinant Human Serum Albumin. Pharm. Res. 2002, 19, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Merlot, A.M.; Kalinowski, D.S.; Richardson, D.R. Unraveling the Mysteries of Serum Albumin-More than Just a Serum Protein. Front. Physiol. 2014, 5, 299. [Google Scholar] [CrossRef]
- Myburgh, J.A.; Mythen, M.G. Resuscitation Fluids. N. Engl. J. Med. 2013, 369, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Navasa, M.; Garcia-Pagan, J.C.; G-Abraldes, J.; Jiménez, W.; Bosch, J.; Arroyo, V. Effect of Intravenous Albumin on Systemic and Hepatic Hemodynamics and Vasoactive Neurohormonal Systems in Patients with Cirrhosis and Spontaneous Bacterial Peritonitis. J. Hepatol. 2004, 41, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Del-Arbol, L.; Monescillo, A.; Arocena, C.; Valer, P.; Ginès, P.; Moreira, V.; Milicua, J.M.; Jiménez, W.; Arroyo, V. Circulatory Function and Hepatorenal Syndrome in Cirrhosis. Hepatology 2005, 42, 439–447. [Google Scholar] [CrossRef]
- Finfer, S.; McEvoy, S.; Bellomo, R.; McArthur, C.; Myburgh, J.; Norton, R.; French, J.; Doig, G.; Hayek, M.; O’Donnell, S.; et al. Impact of Albumin Compared to Saline on Organ Function and Mortality of Patients with Severe Sepsis. Intensive Care Med. 2011, 37, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Caraceni, P.; Navickis, R.J.; Wilkes, M.M. Albumin Infusion in Patients Undergoing Large-Volume Paracentesis: A Meta-Analysis of Randomized Trials. Hepatology 2012, 55, 1172–1181.e1. [Google Scholar] [CrossRef]
- Salerno, F.; Navickis, R.J.; Wilkes, M.M. Albumin Infusion Improves Outcomes of Patients with Spontaneous Bacterial Peritonitis: A Meta-Analysis of Randomized Trials. Clin. Gastroenterol. Hepatol. 2013, 11, 123–130.e1. [Google Scholar] [CrossRef]
- Arroyo, V.; García-Martinez, R.; Salvatella, X. Human Serum Albumin, Systemic Inflammation, and Cirrhosis. J. Hepatol. 2014, 61, 396–407. [Google Scholar] [CrossRef]
- Denda, M.; Fuziwara, S.; Inoue, K. Influx of Calcium and Chloride Ions into Epidermal Keratinocytes Regulates Exocytosis of Epidermal Lamellar Bodies and Skin Permeability Barrier Homeostasis. J. Investig. Dermatol. 2003, 121, 362–367. [Google Scholar] [CrossRef]
- Inoue, K.; Takei, K.; Denda, M. Functional Glycine Receptor in Cultured Human Keratinocytes. Exp. Dermatol. 2015, 24, 307–309. [Google Scholar] [CrossRef]
- Tan, B.; Yin, Y.; Kong, X.; Li, P.; Li, X.; Gao, H.; Li, X.; Huang, R.; Wu, G. L-Arginine Stimulates Proliferation and Prevents Endotoxin-Induced Death of Intestinal Cells. Amino Acids 2010, 38, 1227–1235. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kanazawa, S.; Ichibori, R.; Tanigawa, T.; Magome, T.; Shingaki, K.; Miyata, S.; Tohyama, M.; Hosokawa, K. L-Arginine Stimulates Fibroblast Proliferation through the GPRC6A-ERK1/2 and PI3K/Akt Pathway. PLoS ONE 2014, 9, e92168. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Wang, C.; Ding, L.; Shen, Y.; Cui, H.; Wang, M.; Wang, H. Arginine Relieves the Inflammatory Response and Enhances the Casein Expression in Bovine Mammary Epithelial Cells Induced by Lipopolysaccharide. Mediat. Inflamm. 2016, 2016, 9618795. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Yang, X.; Wang, L.; Gao, K.; Jiang, Z. L-Arginine Inhibited Inflammatory Response and Oxidative Stress Induced by Lipopolysaccharide via Arginase-1 Signaling in IPEC-J2 Cells. Int. J. Mol. Sci. 2019, 20, 1800. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I. Atopic Dermatitis Treatment: Current State of the Art and Emerging Therapies. Allergy Asthma Proc. 2017, 38, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Abrol, S.; Wani, M. Misuse of Topical Corticosteroids on Facial Skin. A Study of 200 Patients. J. Dermatol. Case Rep. 2017, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Rossol, M.; Heine, H.; Meusch, U.; Quandt, D.; Klein, C.; Sweet, M.J.; Hauschildt, S. LPS-Induced Cytokine Production in Human Monocytes and Macrophages. Crit. Rev. Trade Immunol. 2011, 31, 379–446. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, Y. Resveratrol Alleviates LPS-Induced Injury in Human Keratinocyte Cell Line HaCaT by up-Regulation of MiR-17. Biochem. Biophys. Res. Commun. 2018, 501, 106–112. [Google Scholar] [CrossRef]
- Basso, F.G.; Soares, D.G.; Pansani, T.N.; Turrioni, A.P.S.; Scheffel, D.L.; de Souza Costa, C.A.; Hebling, J. Effect of LPS Treatment on the Viability and Chemokine Synthesis by Epithelial Cells and Gingival Fibroblasts. Arch. Oral. Biol. 2015, 60, 1117–1121. [Google Scholar] [CrossRef]
- Pivarcsi, A.; Bodai, L.; Réthi, B.; Kenderessy-Szabó, A.; Koreck, A.; Széll, M.; Beer, Z.; Bata-Csörgo, Z.; Magócsi, M.; Rajnavölgyi, E.; et al. Expression and Function of Toll-like Receptors 2 and 4 in Human Keratinocytes. Int. Immunol. 2003, 15, 721–730. [Google Scholar] [CrossRef]
- Hoshino, K.; Takeuchi, O.; Kawai, T.; Sanjo, H.; Ogawa, T.; Takeda, Y.; Takeda, K.; Akira, S. Cutting Edge: Toll-Like Receptor 4 (TLR4)-Deficient Mice Are Hyporesponsive to Lipopolysaccharide: Evidence for TLR4 as the Lps Gene Product. J. Immunol. 1999, 162, 3749–3752. [Google Scholar] [CrossRef]
- Gaidt, M.M.; Ebert, T.S.; Chauhan, D.; Schmidt, T.; Schmid-Burgk, J.L.; Rapino, F.; Robertson, A.A.B.; Cooper, M.A.; Graf, T.; Hornung, V. Human Monocytes Engage an Alternative Inflammasome Pathway. Immunity 2016, 44, 833–846. [Google Scholar] [CrossRef] [PubMed]
- Pang, G.; Couch, L.; Batey, R.; Clancy, R.; Cripps, A. GM-CSF, IL-1 Alpha, IL-1 Beta, IL-6, IL-8, IL-10, ICAM-1 and VCAM-1 Gene Expression and Cytokine Production in Human Duodenal Fibroblasts Stimulated with Lipopolysaccharide, IL-1 Alpha and TNF-Alpha. Clin. Exp. Immunol. 1994, 96, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Kent, L.W.; Rahemtulla, F.; Hockett, R.D.; Gilleland, R.C.; Michalek, S.M. Effect of Lipopolysaccharide and Inflammatory Cytokines on Interleukin-6 Production by Healthy Human Gingival Fibroblasts. Infect. Immun. 1998, 66, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Chakravortty, D.; Kumar, K.S.N. Interaction of Lipopolysaccharide with Human Small Intestinal Lamina Propria Fibroblasts Favors Neutrophil Migration and Peripheral Blood Mononuclear Cell Adhesion by the Production of Proinflammatory Mediators and Adhesion Molecules. Biochim. Biophys. Acta-Mol. Basis Dis. 1999, 1453, 261–272. [Google Scholar] [CrossRef]
- Wang, P.L.; Shirasu, S.; Shinohar, M.; Azuma, Y.; Daito, M.; Yasuda, H.; Ohura, K. IL-10 Inhibits Porphyromonas Gingivalis LPS-Stimulated Human Gingival Fibroblasts Production of IL-6. Biochem. Biophys. Res. Commun. 1999, 263, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wu, L.; Qu, J.M. Inhibited Proliferation of Human Lung Fibroblasts by LPS Is through IL-6 and IL-8 Release. Cytokine 2011, 54, 289–295. [Google Scholar] [CrossRef]
- Cho, J.S.; Kang, J.H.; Um, J.Y.; Han, I.H.; Park, I.H.; Heung, H.L. Lipopolysaccharide Induces Pro-Inflammatory Cytokines and Mmp Production via TLR4 in Nasal Polyp-Derived Fibroblast and Organ Culture. PLoS ONE 2014, 9, e90683. [Google Scholar] [CrossRef] [PubMed]
- Le, T.A.; Takai, T.; Vu, A.T.; Kinoshita, H.; Ikeda, S.; Ogawa, H.; Okumura, K. Glucocorticoids Inhibit Double-Stranded RNA-Induced Thymic Stromal Lymphopoietin Release from Keratinocytes in an Atopic Cytokine Milieu More Effectively than Tacrolimus. Int. Arch. Allergy Immunol. 2010, 153, 27–34. [Google Scholar] [CrossRef]
- Takada, K.; Komine-Aizawa, S.; Hirohata, N.; Trinh, Q.D.; Nishina, A.; Kimura, H.; Hayakawa, S. Poly I: C Induces Collective Migration of HaCaT Keratinocytes via IL-8. BMC Immunol. 2017, 18, 19. [Google Scholar] [CrossRef]
- Kong, L.; Liu, J.; Wang, J.; Luo, Q.; Zhang, H.; Liu, B.; Xu, F.; Pang, Q.; Liu, Y.; Dong, J. Icariin Inhibits TNF-α/IFN-γ Induced Inflammatory Response via Inhibition of the Substance P and P38-MAPK Signaling Pathway in Human Keratinocytes. Int. Immunopharmacol. 2015, 29, 401–407. [Google Scholar] [CrossRef]
- Tashiro, N.; Segawa, R.; Tobita, R.; Asakawa, S.; Mizuno, N.; Hiratsuka, M.; Hirasawa, N. Hypoxia Inhibits TNF-α-Induced TSLP Expression in Keratinocytes. PLoS ONE 2019, 14, e0224705. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.; Lee, W.H.; Woo Jeong, J.; Park, M.; Ko, J.Y.; Wook Kwon, O.; Lee, J.; Kim, Y.J. Pyropia Yezoensis Extract Suppresses Ifn-Gamma and Tnf-Alpha-Induced Proinflammatory Chemokine Production in Hacat Cells via the down-Regulation of Nf-Κb. Nutrients 2020, 12, 1238. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.C.; Brown, S.J. Atopic Eczema Treatment Now and in the Future: Targeting the Skin Barrier and Key Immune Mechanisms in Human Skin. World J. Dermatol. 2017, 6, 42. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Dinarello, C.A.; Molgora, M.; Garlanda, C. Interleukin-1 and Related Cytokines in the Regulation of Inflammation and Immunity. Immunity 2019, 50, 778–795. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Xue, F.; Quan, C.; Qu, M.; Liu, N.; Zhang, Y.; Fleming, C.; Hu, X.; Zhang, H.-g.; Weichselbaum, R.; et al. A Critical Role of the IL-1β–IL-1R Signaling Pathway in Skin Inflammation and Psoriasis Pathogenesis. J. Investig. Dermatol. 2019, 139, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Sedger, L.M.; McDermott, M.F. TNF and TNF-Receptors: From Mediators of Cell Death and Inflammation to Therapeutic Giants—Past, Present and Future. Cytokine Growth Factor Rev. 2014, 25, 453–472. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, U.; Hvid, M.; Johansen, C.; Buchner, M.; Fölster-Holst, R.; Deleuran, M.; Vestergaard, C. TSLP, IL-31, IL-33 and SST2 Are New Biomarkers in Endophenotypic Profiling of Adult and Childhood Atopic Dermatitis. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1930–1938. [Google Scholar] [CrossRef]
- Savinko, T.; Matikainen, S.; Saarialho-Kere, U.; Lehto, M.; Wang, G.; Lehtimäki, S.; Karisola, P.; Reunala, T.; Wolff, H.; Lauerma, A.; et al. IL-33 and ST2 in Atopic Dermatitis: Expression Profiles and Modulation by Triggering Factors. J. Investig. Dermatol. 2012, 132, 1392–1400. [Google Scholar] [CrossRef]
- Salimi, M.; Barlow, J.L.; Saunders, S.P.; Xue, L.; Gutowska-Owsiak, D.; Wang, X.; Huang, L.C.; Johnson, D.; Scanlon, S.T.; McKenzie, A.N.J.; et al. A Role for IL-25 and IL-33–Driven Type-2 Innate Lymphoid Cells in Atopic Dermatitis. J. Exp. Med. 2013, 210, 2939. [Google Scholar] [CrossRef]
- Dinarello, C.A. The IL-1 Family of Cytokines and Receptors in Rheumatic Diseases. Nat. Rev. Rheumatol. 2019, 15, 612–632. [Google Scholar] [CrossRef]
- Witte-Händel, E.; Wolk, K.; Tsaousi, A.; Irmer, M.L.; Mößner, R.; Shomroni, O.; Lingner, T.; Witte, K.; Kunkel, D.; Salinas, G.; et al. The IL-1 Pathway Is Hyperactive in Hidradenitis Suppurativa and Contributes to Skin Infiltration and Destruction. J. Investig. Dermatol. 2019, 139, 1294–1305. [Google Scholar] [CrossRef] [PubMed]
- Gough, P.; Myles, I.A. Tumor Necrosis Factor Receptors: Pleiotropic Signaling Complexes and Their Differential Effects. Front. Immunol. 2020, 11, 585880. [Google Scholar] [CrossRef] [PubMed]
- Genever, P.G.; Maxfield, S.J.; Kennovin, G.D.; Maltman, J.; Bowgen, C.J.; Raxworthy, M.J.; Skerry, T.M. Evidence for a Novel Glutamate-Mediated Signaling Pathway in Keratinocytes. J. Investig. Dermatol. 1999, 112, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Skerry, T.M.; Genever, P.G. Glutamate Signalling in Non-Neuronal Tissues. Trends Pharmacol. Sci. 2001, 22, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Cibrian, D.; de la Fuente, H.; Sánchez-Madrid, F. Metabolic Pathways That Control Skin Homeostasis and Inflammation. Trends Mol. Med. 2020, 26, 975–986. [Google Scholar] [CrossRef]
- Fernández-Villa, D.; Gómez-Lavín, M.J.; Abradelo, C.; Román, J.S.; Rojo, L. Tissue Engineering Therapies Based on Folic Acid and Other Vitamin B Derivatives. Functional Mechanisms and Current Applications in Regenerative Medicine. Int. J. Mol. Sci. 2018, 19, 4068. [Google Scholar] [CrossRef] [PubMed]
- Schnellbaecher, A.; Binder, D.; Bellmaine, S.; Zimmer, A. Vitamins in Cell Culture Media: Stability and Stabilization Strategies. Biotechnol. Bioeng. 2019, 116, 1537–1555. [Google Scholar] [CrossRef]
- Proksch, E.; Fölster-Holst, R.; Jensen, J.M. Skin Barrier Function, Epidermal Proliferation and Differentiation in Eczema. J. Dermatol. Sci. 2006, 43, 159–169. [Google Scholar] [CrossRef]
- Furue, M. Regulation of Filaggrin, Loricrin, and Involucrin by IL-4, IL-13, IL-17A, IL-22, AHR, and NRF2: Pathogenic Implications in Atopic Dermatitis. Int. J. Mol. Sci. 2020, 21, 5382. [Google Scholar] [CrossRef]
- Trautmann, A.; Altznauer, F.; Akdis, M.; Simon, H.U.; Disch, R.; Bröcker, E.B.; Blaser, K.; Akdis, C.A. The Differential Fate of Cadherins during T-Cell-Induced Keratinocyte Apoptosis Leads to Spongiosis in Eczematous Dermatitis. J. Investig. Dermatol. 2001, 117, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, G.; Dellambra, E.; Golisano, O.; Martinelli, E.; Fantozzi, I.; Bondanza, S.; Ponzin, D.; McKeon, F.; De Luca, M. P63 Identifies Keratinocyte Stem Cells. Proc. Natl. Acad. Sci. USA 2001, 98, 3156. [Google Scholar] [CrossRef]
- Senoo, M.; Pinto, F.; Crum, C.P.; McKeon, F. P63 Is Essential for the Proliferative Potential of Stem Cells in Stratified Epithelia. Cell 2007, 129, 523–536. [Google Scholar] [CrossRef] [PubMed]
- Botchkarev, V.A.; Flores, E.R. P53/P63/P73 in the Epidermis in Health and Disease. Cold Spring Harb. Perspect. Med. 2014, 4, a015248. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Liu, F.; Wang, J.; Chen, X.; Xie, J.; Xiong, K. Epidermal Stem Cells in Wound Healing and Their Clinical Applications. Stem Cell Res. Ther. 2019, 10. [Google Scholar] [CrossRef]
- Eyermann, C.E.; Chen, X.; Somuncu, O.S.; Li, J.; Joukov, A.N.; Chen, J.; Alexandrova, E.M. ΔNp63 Controls Stemness and Inflammation in the Adult Epidermis. bioRxiv 2022. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Number of Patients | 20 |
|---|---|
| Female | 16 |
| Male | 4 |
| Mean age Ethnicity Fitzpatrick Skin Type | 43 ± 14 (23~80) Korean II~III |
| Disease distribution; Xerotic eczema/xerosis cutis Atopic dermatitis Seborrheic dermatitis | 14 4 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Jung, E.; Yang, W.; Kim, C.-K.; Durnaoglu, S.; Oh, I.-R.; Kim, C.-W.; Sinskey, A.J.; Mihm, M.C., Jr.; Lee, J.H. A Novel Multi-Component Formulation Reduces Inflammation In Vitro and Clinically Lessens the Symptoms of Chronic Eczematous Skin. Int. J. Mol. Sci. 2023, 24, 12979. https://doi.org/10.3390/ijms241612979
Kim J, Jung E, Yang W, Kim C-K, Durnaoglu S, Oh I-R, Kim C-W, Sinskey AJ, Mihm MC Jr., Lee JH. A Novel Multi-Component Formulation Reduces Inflammation In Vitro and Clinically Lessens the Symptoms of Chronic Eczematous Skin. International Journal of Molecular Sciences. 2023; 24(16):12979. https://doi.org/10.3390/ijms241612979
Chicago/Turabian StyleKim, Jihee, Eunjoong Jung, Wonmi Yang, Chun-Kang Kim, Serpen Durnaoglu, In-Rok Oh, Chan-Wha Kim, Anthony J. Sinskey, Martin C. Mihm, Jr., and Ju Hee Lee. 2023. "A Novel Multi-Component Formulation Reduces Inflammation In Vitro and Clinically Lessens the Symptoms of Chronic Eczematous Skin" International Journal of Molecular Sciences 24, no. 16: 12979. https://doi.org/10.3390/ijms241612979
APA StyleKim, J., Jung, E., Yang, W., Kim, C.-K., Durnaoglu, S., Oh, I.-R., Kim, C.-W., Sinskey, A. J., Mihm, M. C., Jr., & Lee, J. H. (2023). A Novel Multi-Component Formulation Reduces Inflammation In Vitro and Clinically Lessens the Symptoms of Chronic Eczematous Skin. International Journal of Molecular Sciences, 24(16), 12979. https://doi.org/10.3390/ijms241612979