
Transforming Psoriasis Care: Probiotics and Prebiotics as Novel Therapeutic Approaches
 ,
,
Abstract
1. Introduction
2. Results and Discussion
2.1. Patients and Background Characteristics
2.2. PASI, DLQI, and Anthropometric Measures
2.3. Inflammatory Markers
2.4. Metabolic Parameters
2.5. Ultrasound Assessments
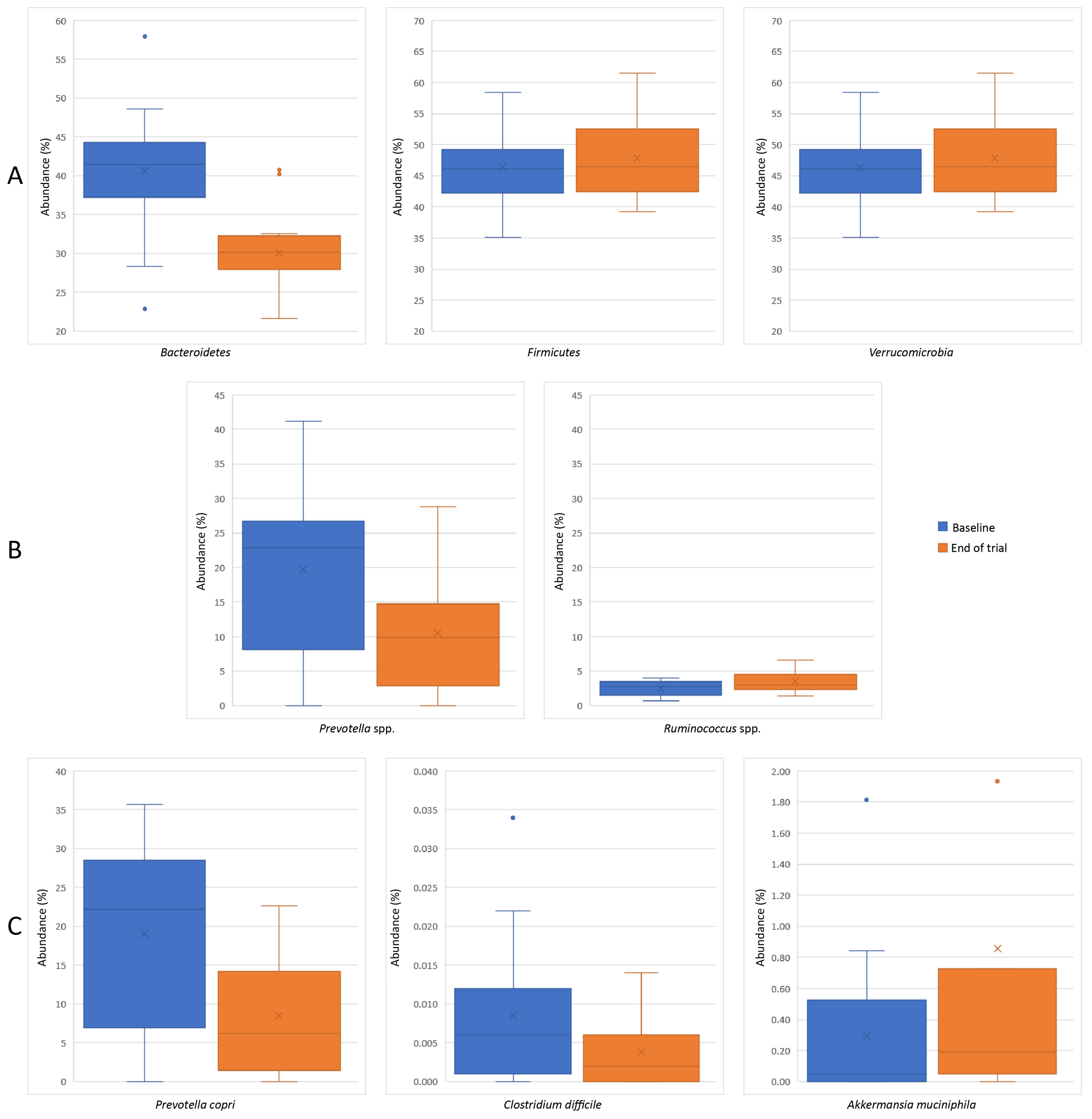
2.6. Gut Microbiota Changes
2.7. Limitations
3. Materials and Methods
3.1. Ethical Considerations
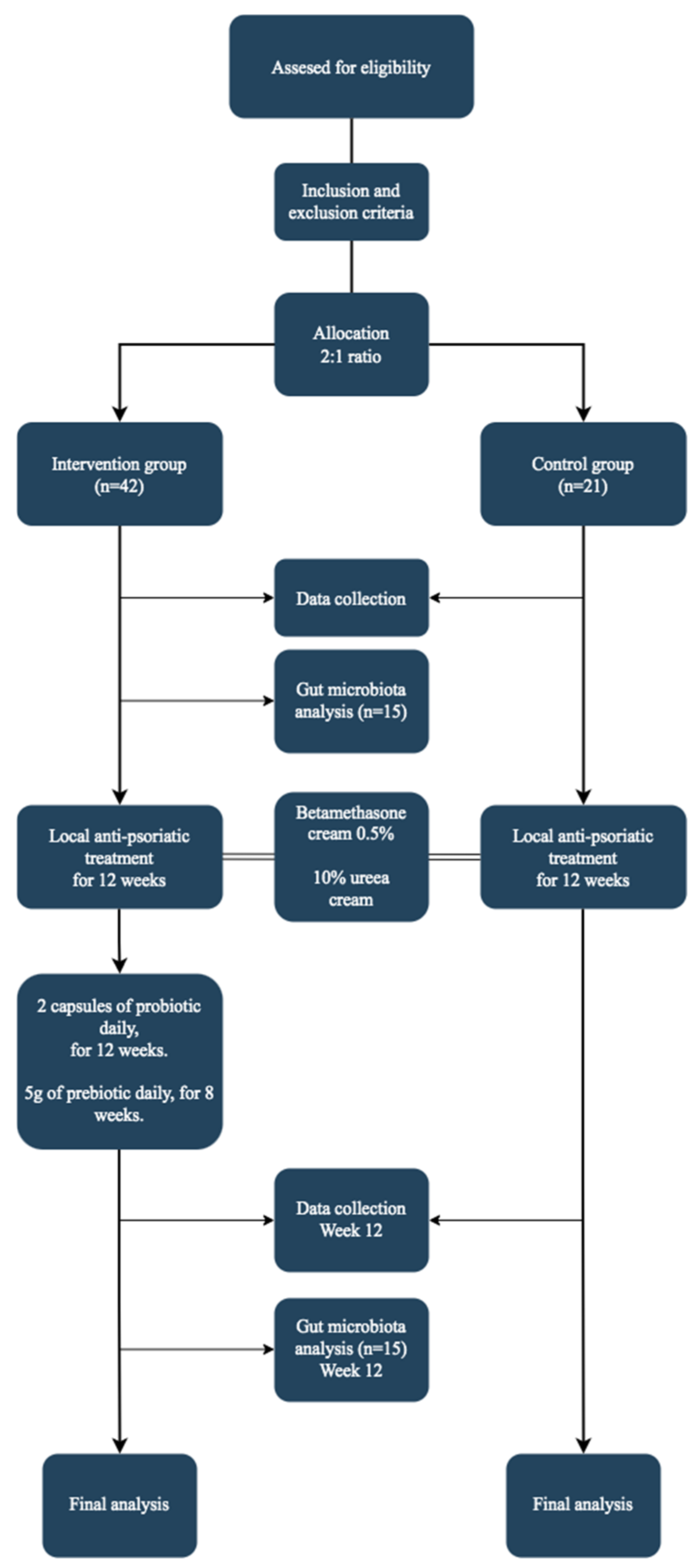
3.2. Study Design and Population
3.3. Data Collection
3.4. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M. National, Regional, and Worldwide Epidemiology of Psoriasis: Systematic Analysis and Modelling Study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, G.W.; Lebwohl, M. Psoriasis: Overview and Diagnosis. In Evidence-Based Psoriasis. Updates in Clinical Dermatology; Bhutani, T., Liao, W., Nakamura, M., Eds.; Springer: Cham, Switzerland, 2018; pp. 1–16. [Google Scholar] [CrossRef]
- Zhou, X.; Chen, Y.; Cui, L.; Shi, Y.; Guo, C. Advances in the Pathogenesis of Psoriasis: From Keratinocyte Perspective. Cell Death Dis. 2022, 13, 81. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Zheng, W.; Dong, Y.; Wang, J.; Garstka, M.A.; Li, R.; An, J.; Ma, H. Serum Levels of Adipokines and Cytokines in Psoriasis Patients: A Systematic Review and Meta-Analysis. Oncotarget 2017, 9, 1266–1278. [Google Scholar] [CrossRef] [PubMed]
- Arican, O.; Aral, M.; Sasmaz, S.; Ciragil, P. Serum Levels of TNF-α, IFN-γ, IL-6, IL-8, IL-12, IL-17, and IL-18 in Patients with Active Psoriasis and Correlation with Disease Severity. Mediators Inflamm. 2005, 2005, 273–279. [Google Scholar] [CrossRef]
- Catinean, A.; Neag, M.A.; Mitre, A.O.; Bocsan, C.I.; Buzoianu, A.D. Microbiota and Immune-Mediated Skin Diseases-An Overview. Microorganisms 2019, 7, 279. [Google Scholar] [CrossRef]
- Buhaș, M.C.; Gavrilaș, L.I.; Candrea, R.; Cătinean, A.; Mocan, A.; Miere, D.; Tătaru, A. Gut Microbiota in Psoriasis. Nutrients 2022, 14, 2970. [Google Scholar] [CrossRef]
- Hidalgo-Cantabrana, C.; Gómez, J.; Delgado, S.; Requena-López, S.; Queiro-Silva, R.; Margolles, A.; Coto, E.; Sánchez, B.; Coto-Segura, P. Gut Microbiota Dysbiosis in a Cohort of Patients with Psoriasis. Br. J. Dermatol. 2019, 181, 1287–1295. [Google Scholar] [CrossRef]
- Zhang, X.; Shi, L.; Sun, T.; Guo, K.; Geng, S. Dysbiosis of Gut Microbiota and Its Correlation with Dysregulation of Cytokines in Psoriasis Patients. BMC Microbiol. 2021, 21, 78. [Google Scholar] [CrossRef]
- Schade, L.; Mesa, D.; Faria, A.R.; Santamaria, J.R.; Xavier, C.A.; Ribeiro, D.; Hajar, F.N.; Azevedo, V.F. The Gut Microbiota Profile in Psoriasis: A Brazilian Case-control Study. Lett. Appl. Microbiol. 2021, 74, 498–504. [Google Scholar] [CrossRef]
- Lin, C.; Zeng, T.; Deng, Y.; Yang, W.; Xiong, J. Treatment of Psoriasis Vulgaris Using Bacteroides Fragilis BF839: A Single-Arm, Open Preliminary Clinical Study. Chin. J. Biotechnol. 2021, 37, 3828–3835. [Google Scholar] [CrossRef]
- Moludi, J.; Fathollahi, P.; Khedmatgozar, H.; Pourteymour Fard Tabrizi, F.; Ghareaghaj Zare, A.; Razmi, H.; Amirpour, M. Probiotics Supplementation Improves Quality of Life, Clinical Symptoms, and Inflammatory Status in Patients with Psoriasis. J. Drugs Dermatol. 2022, 21, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Deng, Y.; Fang, Z.; Zhai, Q.; Cui, S.; Zhao, J.; Chen, W.; Zhang, H. Potential Role of Probiotics in Ameliorating Psoriasis by Modulating Gut Microbiota in Imiquimod-Induced Psoriasis-Like Mice. Nutrients 2021, 13, 2010. [Google Scholar] [CrossRef] [PubMed]
- Bader, J.; Albin, A.; Stahl, U. Spore-forming bacteria and their utilisation as probiotics. Benef. Microbes 2012, 3, 67–75. [Google Scholar] [CrossRef]
- Casula, G.; Cutting, S.M. Bacillus probiotics: Spore germination in the gastrointestinal tract. Appl. Environ. Microbiol. 2002, 68, 2344–2352. [Google Scholar] [CrossRef] [PubMed]
- Hoa, T.T.; Duc, L.H.; Isticato, R.; Baccigalupi, L.; Ricca, E.; Van, P.H.; Cutting, S.M. Fate and dissemination of Bacillus subtilis spores in a murine model. Appl. Environ. Microbiol. 2001, 67, 3819–3823. [Google Scholar] [CrossRef]
- Gu, M.J.; Song, S.K.; Park, S.M.; Lee, I.K.; Yun, C.H. Bacillus subtilis Protects Porcine Intestinal Barrier from Deoxynivalenol via Improved Zonula Occludens-1 Expression. Asian-Australas J. Anim. Sci. 2014, 27, 580–586. [Google Scholar] [CrossRef]
- Marzorati, M.; Abbeele, P.; Bubeck, S.S.; Bayne, T.; Krishnan, K.; Young, A.; Mehta, D.; DeSouza, A. Bacillus subtilis HU58 and Bacillus coagulans SC208 Probiotics Reduced the Effects of Antibiotic-Induced Gut Microbiome Dysbiosis in an M-SHIME® Model. Microorganisms 2020, 8, 1028. [Google Scholar] [CrossRef]
- Marzorati, M.; Van den Abbeele, P.; Bubeck, S.; Bayne, T.; Krishnan, K.; Young, A. Treatment with a spore-based probiotic containing five strains of Bacillus induced changes in the metabolic activity and community composition of the gut microbiota in a SHIME(R) model of the human gastrointestinal system. Food Res. Int. 2021, 149, 110676. [Google Scholar] [CrossRef]
- McFarlin, B.K.; Henning, A.L.; Bowman, E.M.; Gary, M.A.; Carbajal, K.M. Oral spore-based probiotic supplementation was associated with reduced incidence of post-prandial dietary endotoxin, triglycerides, and disease risk biomarkers. World J. Gastrointest. Pathophysiol. 2017, 8, 117–126. [Google Scholar] [CrossRef]
- Hejdysz, M.; Kaczmarek, S.A.; Kubiś, M.; Wiśniewska, Z.; Peris, S.; Budnik, S.; Rutkowski, A. The effect of protease and Bacillus licheniformis on nutritional value of pea, faba bean, yellow lupin and narrow-leaved lupin in broiler chicken diets. Br. Poult. Sci. 2020, 61, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Vajaranant, K.; Fields, M.L. The Production of Vitamin B6 by Microorganisms in Corn Meal 1. J. Food Prot. 1989, 52, 827–828. [Google Scholar] [CrossRef]
- Khaneja, R.; Perez-Fons, L.; Fakhry, S.; Baccigalupi, L.; Steiger, S.; To, E.; Sandmann, G.; Dong, T.C.; Ricca, E.; Fraser, P.D.; et al. Carotenoids found in Bacillus. J. Appl. Microbiol. 2010, 108, 1889–1902. [Google Scholar] [CrossRef] [PubMed]
- Sy, C.; Caris-Veyrat, C.; Dufour, C.; Boutaleb, M.; Borel, P.; Dangles, O. Inhibition of iron-induced lipid peroxidation by newly identified bacterial carotenoids in model gastric conditions: Comparison with common carotenoids. Food Funct. 2013, 4, 698–712. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Yamada, Y.; Ohtani, Y.; Mitsui, N.; Murasawa, H.; Araki, S. Production of menaquinone (vitamin K2)-7 by Bacillus subtilis. J. Biosci. Bioeng. 2001, 91, 16–20. [Google Scholar] [CrossRef]
- Lopetuso, L.R.; Scaldaferri, F.; Franceschi, F.; Gasbarrini, A. Bacillus clausii and gut homeostasis: State of the art and future perspectives. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Fu, R.; Liang, C.; Chen, D.; Yan, H.; Tian, G.; Zheng, P.; He, J.; Yu, J.; Mao, X.; Huang, Z.; et al. Effects of dietary Bacillus coagulans and yeast hydrolysate supplementation on growth performance, immune response and intestinal barrier function in weaned piglets. J. Anim. Physiol. Anim. Nutr. 2021, 105, 898–907. [Google Scholar] [CrossRef]
- Neu, A.K.; Pleissner, D.; Mehlmann, K.; Schneider, R.; Puerta-Quintero, G.I.; Venus, J. Fermentative utilization of coffee mucilage using Bacillus coagulans and investigation of down-stream processing of fermentation broth for optically pure l(+)-lactic acid production. Bioresour. Technol. 2016, 211, 398–405. [Google Scholar] [CrossRef]
- Duysburgh, C.; Van den Abbeele, P.; Krishnan, K.; Bayne, T.F.; Marzorati, M. A synbiotic concept containing spore-forming Bacillus strains and a prebiotic fiber blend consistently enhanced metabolic activity by modulation of the gut microbiome in vitro. Int. J. Pharm. X 2019, 1, 100021. [Google Scholar] [CrossRef]
- Krumbeck, J.A.; Rasmussen, H.E.; Hutkins, R.W.; Clarke, J.; Shawron, K.; Keshavarzian, A.; Walter, J. Probiotic Bifidobacterium strains and galactooligosaccharides improve intestinal barrier function in obese adults but show no synergism when used together as synbiotics. Microbiome. 2018, 6, 121. [Google Scholar] [CrossRef]
- Dou, Y.; Yu, X.; Luo, Y.; Chen, B.; Ma, D.; Zhu, J. Effect of Fructooligosaccharides Supplementation on the Gut Microbiota in Human: A Systematic Review and Meta-Analysis. Nutrients. 2022, 14, 3298. [Google Scholar] [CrossRef] [PubMed]
- Yan, F.; Tian, S.; Du, K.; Xue, X.; Gao, P.; Chen, Z. Preparation and nutritional properties of xylooligosaccharide from agricultural and forestry byproducts: A comprehensive review. Front. Nutr. 2022, 9, 977548. [Google Scholar] [CrossRef] [PubMed]
- Mattei, P.L.; Corey, K.C.; Kimball, A.B. Psoriasis Area Severity Index (PASI) and the Dermatology Life Quality Index (DLQI): The Correlation between Disease Severity and Psychological Burden in Patients Treated with Biological Therapies. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 333–337. [Google Scholar] [CrossRef]
- Moludi, J.; Khedmatgozar, H.; Saiedi, S.; Razmi, H.; Alizadeh, M.; Ebrahimi, B. Probiotic Supplementation Improves Clinical Outcomes and Quality of Life Indicators in Patients with Plaque Psoriasis: A Randomized Double-Blind Clinical Trial. Clin. Nutr. ESPEN 2021, 46, 33–39. [Google Scholar] [CrossRef]
- Akbarzadeh, A.; Alirezaei, P.; Doosti-Irani, A.; Mehrpooya, M.; Nouri, F. The Efficacy of Lactocare® Synbiotic on the Clinical Symptoms in Patients with Psoriasis: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Dermatol. Res. Pract. 2022, 2022, 4549134. [Google Scholar] [CrossRef]
- Bhosle, M.J.; Kulkarni, A.; Feldman, S.R.; Balkrishnan, R. Quality of Life in Patients with Psoriasis. Health Qual. Life Outcomes 2006, 4, 35. [Google Scholar] [CrossRef] [PubMed]
- Wiciński, M.; Gębalski, J.; Gołębiewski, J.; Malinowski, B. Probiotics for the Treatment of Overweight and Obesity in Humans—A Review of Clinical Trials. Microorganisms 2020, 8, 1148. [Google Scholar] [CrossRef] [PubMed]
- Ovcina-Kurtovic, N.; Kasumagic-Halilovic, E. Serum Levels of Tumor Necrosis Factor-alpha in Patients with Psoriasis. Mater. Sociomed. 2022, 34, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Michalak-Stoma, A.; Bartosińska, J.; Kowal, M.; Raczkiewicz, D.; Krasowska, D.; Chodorowska, G. IL-17A in the Psoriatic Patients’ Serum and Plaque Scales as Potential Marker of the Diseases Severity and Obesity. Mediators Inflamm. 2020, 2020, 7420823. [Google Scholar] [CrossRef]
- Kim, H.O.; Kim, H.S.; Youn, J.C.; Shin, E.C.; Park, S. Serum cytokine profiles in healthy young and elderly population assessed using multiplexed bead-based immunoassays. J. Transl. Med. 2011, 9, 113. [Google Scholar] [CrossRef]
- Li, Y.; Golden, J.B.; Camhi, M.I.; Zhang, X.; Fritz, Y.; Diaconu, D.; Ivanco, T.L.; Simon, D.I.; Kikly, K.; McCormick, T.S.; et al. Protection from Psoriasis-Related Thrombosis after Inhibition of IL-23 or IL-17A. J. Invest. Dermatol. 2018, 138, 310–315. [Google Scholar] [CrossRef]
- Meephansan, J.; Subpayasarn, U.; Komine, M.; Ohtsuki, M. Pathogenic Role of Cytokines and Effect of Their Inhibition in Psoriasis. In An Interdisciplinary Approach to Psoriasis; InTech: London, UK, 2017; Available online: https://www.intechopen.com/chapters/54988 (accessed on 29 June 2023).
- Asadullah, K.; Sterry, W.; Volk, H.D. Interleukin-10 and Psoriasis. Available online: https://www.ncbi.nlm.nih.gov/books/NBK6507/ (accessed on 20 March 2023).
- Zeng, L.; Yu, G.; Wu, Y.; Hao, W.; Zeng, L. The Effectiveness and Safety of Probiotic Supplements for Psoriasis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Preclinical Trials. J. Immunol. Res. 2021, 2021, 7552546. [Google Scholar] [CrossRef]
- Chen, Y.H.; Wu, C.S.; Chao, Y.H.; Lin, C.C.; Tsai, H.Y.; Li, Y.R.; Chen, Y.Z.; Tsai, W.H.; Chen, Y.K. Lactobacillus Pentosus GMNL-77 Inhibits Skin Lesions in Imiquimod-Induced Psoriasis-like Mice. J. Food Drug Anal. 2017, 25, 559–566. [Google Scholar] [CrossRef]
- Groeger, D.; O’Mahony, L.; Murphy, E.F.; Bourke, J.F.; Dinan, T.G.; Kiely, B.; Shanahan, F.; Quigley, E.M.M. Bifidobacterium Infantis 35624 Modulates Host Inflammatory Processes beyond the Gut. Gut Microbes 2013, 4, 325–339. [Google Scholar] [CrossRef]
- Ooi, L.G.; Liong, M.T. Cholesterol-Lowering Effects of Probiotics and Prebiotics: A Review of in Vivo and in Vitro Findings. Int. J. Mol. Sci. 2010, 11, 2499–2522. [Google Scholar] [CrossRef]
- Sivamaruthi, B.S.; Bharathi, M.; Kesika, P.; Suganthy, N.; Chaiyasut, C. The Administration of Probiotics against Hypercholesterolemia: A Systematic Review. Appl. Sci. 2021, 11, 6913. [Google Scholar] [CrossRef]
- Miao, C.; Li, J.; Li, Y.; Zhang, X. Obesity and Dyslipidemia in Patients with Psoriasis: A Case–Control Study. Medicine 2019, 98, e16323. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P. Hyperuricemia in Patients with Chronic Plaque Psoriasis. Drug Dev. Res. 2014, 75, S70–S72. [Google Scholar] [CrossRef] [PubMed]
- Tripolino, C.; Ciaffi, J.; Ruscitti, P.; Giacomelli, R.; Meliconi, R.; Ursini, F. Hyperuricemia in Psoriatic Arthritis: Epidemiology, Pathophysiology, and Clinical Implications. Front. Med. 2021, 8, 1–11. [Google Scholar] [CrossRef]
- Widawski, L.; Fabacher, T.; Spielmann, L.; Gottenberg, J.; Sibilia, J.; Duret, P.; Messer, L.; Felten, R. Psoriatic Arthritis with Hyperuricemia: More Peripheral, Destructive, and Challenging to Treat. Clin. Rheumatol. 2022, 41, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.Q.; Zheng, Q.X.; Jiang, X.M.; Chen, X.Q.; Zhang, X.Y.; Wu, J.L. Probiotic Supplements Improve Blood Glucose and Insulin Resistance/Sensitivity among Healthy and GDM Pregnant Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based. Complement. Alternat. Med. 2021, 2021, 9830200. [Google Scholar] [CrossRef]
- Ruan, Y.; Sun, J.; He, J.; Chen, F.; Chen, R.; Chen, H. Effect of Probiotics on Glycemic Control: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. PLoS ONE 2015, 10, 1–15. [Google Scholar] [CrossRef]
- Nicolescu, A.C.; Ionescu, S.; Ancuta, I.; Popa, V.-T.; Lupu, M.; Soare, C.; Cozma, E.-C.; Voiculescu, V.-M. Subepidermal Low-Echogenic Band—Its Utility in Clinical Practice: A Systematic Review. Diagnostics 2023, 13, 970. [Google Scholar] [CrossRef]
- El Gammal, S.; El Gammal, C.; Kaspar, K.; Pieck, C.; Altmeyer, P.; Vogt, M.; Ermert, H. Sonography of the Skin at 100 MHz Enables in Vivo Visualization of Stratum Corneum and Viable Epidermis in Palmar Skin and Psoriatic Plaques. J. Invest. Dermatol. 1999, 113, 821–829. [Google Scholar] [CrossRef]
- Marina, M.E.; Jid, C.B.; Roman, I.I.; Mihu, C.M.; Tătaru, A.D. Ultrasonography in Psoriatic Disease. Med. Ultrason. 2015, 17, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Jwo, J.Y.; Chang, Y.T.; Huang, Y.C. Effects of Probiotics Supplementation on Skin Photoaging and Skin Barrier Function: A Systematic Review and Meta-Analysis. Photodermatol. Photoimmunol. Photomed. 2022, 39, 122–131. [Google Scholar] [CrossRef]
- Yin, L.; Wan, Y.D.; Pan, X.T.; Zhou, C.Y.; Lin, N.; Ma, C.T.; Yao, J.; Su, Z.; Wan, C.; Yu, Y.W.; et al. Association Between Gut Bacterial Diversity and Mortality in Septic Shock Patients: A Cohort Study. Med. Sci. Monit. 2019, 25, 7376–7382. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.R.; Shin, J.; Guevarra, R.B.; Lee, J.H.; Kim, D.W.; Seol, K.H.; Lee, J.H.; Kim, H.B.; Isaacson, R.E. Deciphering Diversity Indices for a Better Understanding of Microbial Communities. J. Microbiol. Biotechnol. 2017, 27, 2089–2093. [Google Scholar] [CrossRef]
- Navarro-López, V.; Martínez-Andrés, A.; Ramírez-Boscà, A.; Ruzafa-Costas, B.; Núñez-Delegido, E.; Carrión-Gutiérrez, M.A.; Prieto-Merino, D.; Codoñer-Cortés, F.; Ramón-Vidal, D.; Genovés-Martínez, S.; et al. Efficacy and Safety of Oral Administration of a Mixture of Probiotic Strains in Patients with Psoriasis: A Randomized Controlled Clinical Trial. Acta Derm. Venereol. 2019, 99, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Scher, J.U.; Ubeda, C.; Artacho, A.; Attur, M.; Isaac, S.; Reddy, S.M.; Marmon, S.; Neimann, A.; Brusca, S.; Patel, T.; et al. Decreased Bacterial Diversity Characterizes the Altered Gut Microbiota in Patients with Psoriatic Arthritis, Resembling Dysbiosis in Inflammatory Bowel Disease. Arthritis Rheumatol. 2015, 67, 128–139. [Google Scholar] [CrossRef]
- Stojanov, S.; Berlec, A.; Štrukelj, B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel Disease. Microorganism 2020, 8, 1715. [Google Scholar] [CrossRef]
- Dei-Cas, I.; Giliberto, F.; Luce, L.; Dopazo, H.; Penas-Steinhardt, A. Metagenomic Analysis of Gut Microbiota in Non-Treated Plaque Psoriasis Patients Stratified by Disease Severity: Development of a New Psoriasis-Microbiome Index. Sci. Reports 2020, 10, 12754. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.; Cohen, N.A.; Shalev, V.; Uzan, A.; Koren, O.; Maharshak, N. Psoriatic Patients Have a Distinct Structural and Functional Fecal Microbiota Compared with Controls. J. Dermatol. 2019, 46, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.R.; Zhao, S.; Zhu, W.; Wu, L.; Li, J.; Shen, M.X.; Lei, L.; Chen, X.; Peng, C. The Akkermansia Muciniphila Is a Gut Microbiota Signature in Psoriasis. Exp. Dermatol. 2017, 27, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Li, L.F.; Dai, T.Y.; Qi, X.; Wang, Y.; Zheng, T.Z.; Gao, X.Y.; Zhang, Y.J.; Ai, Y.; Ma, L.; et al. Short-Chain Fatty Acids Produced by Ruminococcaceae Mediate α-Linolenic Acid Promote Intestinal Stem Cells Proliferation. Mol. Nutr. Food Res. 2021, 66, 2100408. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, V.F.; Elias-Oliveira, J.; Pereira, Í.S.; Pereira, J.A.; Barbosa, S.C.; Machado, M.S.G.; Carlos, D. Akkermansia Muciniphila and Gut Immune System: A Good Friendship That Attenuates Inflammatory Bowel Disease, Obesity, and Diabetes. Front. Immunol. 2022, 13, 1–8. [Google Scholar] [CrossRef]
- Șomlea, M.; Boca, A.; Pop, A.; Ilieș, R.; Vesa, S.; Buzoianu, A.; Tătaru, A. High-Frequency Ultrasonography of Psoriatic Skin: A Non-Invasive Technique in the Evaluation of the Entire Skin of Patients with Psoriasis: A Pilot Study. Exp. Ther. Med. 2019, 18, 4981–4986. [Google Scholar] [CrossRef]
- Microbiom in Materii Fecale—Detalii Analiza|Bioclinica. Available online: https://bioclinica.ro/analize/genetica-moleculara/microbiom-in-materii-fecale-1 (accessed on 14 March 2023).
- Das Intestinale Mikrobiom|Adipositas, Diabetes Und Arteriosklerose. Available online: https://www.ganzimmun.de/labor/wichtige-laborinformationen/das-intestinale-mikrobiom (accessed on 14 March 2023).



{kind=link}
{kind=link}
| Variable | Intervention (n = 42) | Control (n = 21) | p-Value |
|---|---|---|---|
| Sex, n (%) | |||
| Male Female | 18.0 (42.9) 24.0 (57.1) | 12.0 (57.1) 9.0 (42.9) | 0.29 * |
| Age (years), mean (SD) | |||
| 34.0 (10.0) | 42.9 (7.7) | <0.001 ** | |
| Smoking status, n (%) | |||
| No Yes | 27.0 (64.3) 15.0 (35.7) | 15.0 (71.4) 6.0 (28.6) | 0.57 * |
| Family history of psoriasis, n (%) | |||
| No Yes | 20.0 (47.6) 22.0 (52.4) | 8.0 (38.1) 13.0 (61.9) | 0.47 * |
| Psoriasis severity, n (%) | |||
| Mild (PASI < 10) Severe (PASI > 10) | 20.0 (47.6) 22.0 (52.4) | 18.0 (85.7) 3.0 (14.3) | 0.006 * |
| Nail psoriasis, n (%) | |||
| No Yes | 22.0 (52.4) 20.0 (47.6) | 17.0 (81.0) 4.0 (19.0) | 0.03 * |
| Psoriatic arthritis, n (%) | |||
| No Yes | 24.0 (57.1) 18.0 (42.9) | 21.0 (100.0) 0.0 | <0.001 * |
| Inflammatory bowel disease, n (%) | |||
| No Yes | 17.0 (40.5) 25.0 (59.5) | 10.0 (47.6) 11.0 (52.4) | 0.59 * |
| Pruritus, n (%) | |||
| No Yes | 5.0 (11.9) 37.0 (88.1) | 5.0 (23.8) 16.0 (76.2) | 0.22 * |
| Previous corticosteroid treatment, n (%) | |||
| No Yes | 11.0 (26.2) 31.0 (73.8) | 12.0 (57.1) 9.0 (42.9) | 0.016 * |
| Variable | Intervention (n = 42) | Control (n = 21) | p-Value *** | p-Adjusted 1 (Change in Intervention Versus Change in Control Group) |
|---|---|---|---|---|
| PASI, mean (SD) | ||||
| Baseline | 10.0 (1.8) | 8.6 (1.2) | ||
| End of study | 8.1 (2.4) | 8.7 (1.6) | ||
| Change | 1.9 (1.4) | −0.2 (0.6) | <0.001 | |
| p-value * (baseline versus end of trial) | <0.001 | 0.23 | ||
| Adjusted mean | 7.6 | 9.8 | <0.001 | |
| DLQI, mean (SD) | ||||
| Baseline | 7.2 (2.9) | 7.7 (2.9) | ||
| End of study | 5.8 (2.9) | 8.4 (4.1) | ||
| Change | 1.4 (1.0) | −0.7 (2.3) | <0.001 | |
| p-value * (baseline versus end of trial) | <0.001 | 0.19 | ||
| Adjusted mean | 6.0 | 7.9 | <0.001 |
| Variable | Intervention (n = 42) | Control (n = 21) | p-Value **** (Change in Intervention versus Change in Control Group) |
|---|---|---|---|
| BMI (kg/m2), median (IQR) | |||
| Baseline | 24.5 (7.9) | 21.6 (4.1) | |
| End of study | 24.5 (8.4) | 21.8 (4.0) | |
| Change | 0.2 (0.6) | −0.2 (1.0) | 0.025 |
| p-value ** (baseline versus end of trial) | 0.019 | 0.17 | |
| Fat mass (%), median (IQR) | |||
| Baseline | 29.4 (19.4) | 22.7 (5.2) | |
| End of study | 26.4 (22.6) | 22.4 (5.4) | |
| Change | 0.4 (2.5) | −0.1 (1.7) | 0.32 |
| p-value ** (baseline versus end of trial) | 0.22 | 0.92 | |
| Free fat mass (%), mean (SD) | |||
| Baseline | 52.6 (10.3) | 46.3 (9.0) | |
| End of study | 50.3 (10.2) | 46.7 (9.1) | |
| Change | 2.4 (5.4) | −0.4 (1.6) | 0.004 |
| p-value * (baseline versus end of trial) | 0.007 | 0.27 |
| Variable | Intervention (n = 42) | Control (n = 21) | p-Value (Change in Intervention versus Change in Control Group) |
|---|---|---|---|
| TNF-α (pg/mL), median (IQR) | |||
| Baseline | 50.0 (41.4) | 7.3 (54.7) | |
| End of study | 15.1 (36.2) | 11.0 (12.7) | |
| Change | 19.5 (42.0) | –1.5 (22.8) | 0.040 **** |
| p-value ** (baseline versus end of trial) | 0.002 | 0.82 | |
| IL-17A (pg/mL), median (IQR) | |||
| Baseline | 19.0 (89.5) | 3.5 (6.6) | |
| End of study | 27.9 (51.8) | 12.5 (80.4) | |
| Change | –1.2 (46.3) | –3.8 (16.9) | 0.66 **** |
| p-value ** (baseline versus end of trial) | 0.55 | 0.006 | |
| IL-6 (pg/mL), median (IQR) | |||
| Baseline | 21.0 (20.5) | 3.8 (1.2) | |
| End of study | 16.2 (16.6) | 21.3 (17.8) | |
| Change | 3.1 (10.0) | –2.4 (18.4) | 0.002 **** |
| p-value ** (baseline versus end of trial) | 0.05 | 0.26 | |
| IFN-γ (pg/mL), median (IQR) | |||
| Baseline | 7.4 (21.3) | 5.3 (9.8) | |
| End of study | 5.9 (16.2) | 6.0 (4.0) | |
| Change | 1.3 (6.7) | −0.3 (5.8) | 0.040 **** |
| p-value ** (baseline versus end of trial) | 0.14 | 0.27 | |
| IL-10 (pg/mL), median (IQR) | |||
| Baseline | 4.4 (3.6) | 4.4 (11.8) | |
| End of study | 9.0 (16.2) | 3.2 (4.3) | |
| Change | –3.6 (5.4) | 0.2 (3.7) | <0.001 **** |
| p-value ** (baseline versus end of trial) | <0.001 | 0.005 |
| Parameter | Intervention (n = 42) | Control (n = 21) | p-Value (Change in Intervention versus Change in Control Group) | p-Adjusted |
|---|---|---|---|---|
| Total cholesterol (mg/dL), mean (SD) | ||||
| Baseline | 195.5 (31.8) | 190.5 (64.1) | ||
| End of study | 192.8 (29.0) | 203.8 (61.5) | ||
| Change | 2.7 (14.0) | –3.3 (43.5) | 0.12 *** | |
| p-value * (baseline versus end of trial) | 0.23 | 0.11 | ||
| Adjusted mean | 188.7 | 211.9 | 0.003 | |
| LDL-C (mg/dL), mean (SD) | ||||
| Baseline | 126.4 (28.4) | 135.0 (137.2) | ||
| End of study | 119.4 (29.6) | 149.6 (132) | 0.001 *** | |
| Change | 7.0 (15.0) | –14.6 (36.4) | ||
| p-value * (baseline versus end of trial) | 0.004 | 0.08 | ||
| Adjusted mean | 119.5 | 149.3 | <0.001 | |
| HDL-C (mg/dL), mean (SD) | ||||
| Baseline | 52.7 (9.0) | 58.4 (11.2) | ||
| End of study | 56.6 (10.7) | 58.6 (13.6) | ||
| Change | –3.9 (5.4) | −0.3 (8) | 0.07 *** | |
| p-value * (baseline versus end of trial) | <0.001 | 0.88 | ||
| Adjusted mean | 58.8 | 54.2 | 0.027 | |
| Triglyceride (mg/dL), median (IQR) | ||||
| Baseline | 83.0 (42.0) | 62.0 (70.5) | ||
| End of study | 75.5 (47.0) | 65.0 (95.0) | ||
| Change | 5.5 (15.0) | –2.0 (19.0) | 0.024 **** | |
| p-value ** (baseline versus end of trial) | 0.017 | 0.36 | ||
| Uric acid (mg/dL), median (IQR) | ||||
| Baseline | 4.5 (1.6) | 3.6 (3.1) | ||
| End of study | 3.6 (0.9) | 4.4 (3.4) | ||
| Change | 0.6 (0.8) | −0.2 (4.3) | 0.32 **** | |
| p-value ** (baseline versus end of trial) | 0.001 | 0.64 | ||
| Blood sugar (mmol/L), median (IQR) | ||||
| Baseline | 90.0 (19.0) | 79.0 (46.0) | ||
| End of study | 100.0 (24.0) | 82.0 (20.0) | ||
| Change | –7.5 (21.0) | –2.0 (29.0) | 0.53 **** | |
| p-value ** (baseline versus end of trial) | 0.001 | 0.16 | ||
| Insulin (mcU/mL), median (IQR) | ||||
| Baseline | 17.1 (17.5) | 14.3 (22.5) | ||
| End of study | 25.7 (18.8) | 15.2 (13.0) | ||
| Change | –2.9 (9.4) | −0.9 (6.0) | 0.42 **** | |
| p-value ** (baseline versus end of trial) | 0.001 | 0.66 |
| Parameter | Intervention (n = 42) | Control (n = 21) | p-Value (Change in Intervention versus Change in Control Group) |
|---|---|---|---|
| Psoriasis plaque hydration (μS), median (IQR) | |||
| Baseline | 20.1 (13.4) | 61.0 (19.0) | |
| End of trial | 90.0 (31.5) | 74.0 (14.0) | |
| Change | –60.1 (30.8) | –18.0 (23.0) | <0.001 ** |
| p-value * (baseline versus end of trial) | <0.001 | <0.001 | |
| Perilesional area hydration (μS), median (IQR) | |||
| Baseline | 131.0 (74.5) | 134.0 (23.0) | |
| End of trial | 168.0 (90.0) | 157.0 (38.0) | |
| Change | –52.1 (30.5) | –22.0 (21.0) | 0.003 ** |
| p-value * (baseline versus end of trial) | <0.001 | <0.001 | |
| SLEB (µm), median (IQR) | |||
| Baseline | 261.5 (95.0) | 224.0 (100.0) | |
| End of trial | 159.0 (53.0) | 186.0 (80.0) | |
| Change | 109.0 (91.0) | 40.0 (72.0) | <0.001 ** |
| p-value * (baseline versus end of trial) | <0.001 | 0.009 | |
| Skin thickness (µm), median (IQR) | |||
| Baseline | 1168.0 (521.0) | 1245.0 (1399.0) | |
| End of trial | 997.0 (150.0) | 1302.0 (506.0) | |
| Change | 237.5 (276.0) | 20.0 (167.0) | <0.001 ** |
| p-value * (baseline versus end of trial) | <0.001 | 0.82 |
| Parameter | Baseline Mean (SD) | End of Study Mean (SD) | Change Mean (SD) | p-Value * |
|---|---|---|---|---|
| Shannon index | 2.820 (0.317) | 2.990 (0.291) | −0.169 (0.222) | 0.011 |
| Firmicutes/Bacteroidetes ratio | 1.206 (0.433) | 1.620 (0.334) | −0.413 (0.294) | <0.001 |
| Acetate/propionate production | 15.660 (9.023) | 20.346 (10.035) | –4.686 (6.531) | 0.015 |
| Prevotella/Bacteroidetes ratio | 3.200 (1.107) | 2.280 (1.435) | 0.920 (1.425) | 0.025 |
| LPS-positive bacteria | 3.465 (1.817) | 2.421 (1.310) | 1.044 (1.531) | 0.019 |
| Bacteroidetes | 40.572 (8.160) | 30.097 (5.168) | 10.475 (6.499) | <0.001 |
| Prevotella spp. | 19.660 (12.244) | 10.523 (7.951) | 9.136 (10.118) | 0.004 |
| Prevotella copri | 19.028 (12.358) | 8.488 (7.532) | 10.540 (9.934) | 0.001 |
| Ruminococcus spp. | 2.479 (1.081) | 3.446 (1.497) | −0.967 (1.688) | 0.044 |
| Parameter | Baseline Median (IQR) | End of Study Median (IQR) | Change Median (IQR) | p-Value * |
|---|---|---|---|---|
| Verrucomicrobia | 0.543 (1.451) | 0.592 (2.115) | −0.199 (0.491) | 0.031 |
| Akkermansia muciniphila | 0.051 (0.526) | 0.189 (0.678) | −0.068 (0.238) | 0.030 |
| Clostridium difficile | 0.006 (0.011) | 0.002 (0.006) | 0.004 (0.006) | 0.040 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buhaș, M.C.; Candrea, R.; Gavrilaș, L.I.; Miere, D.; Tătaru, A.; Boca, A.; Cătinean, A. Transforming Psoriasis Care: Probiotics and Prebiotics as Novel Therapeutic Approaches. Int. J. Mol. Sci. 2023, 24, 11225. https://doi.org/10.3390/ijms241311225
Buhaș MC, Candrea R, Gavrilaș LI, Miere D, Tătaru A, Boca A, Cătinean A. Transforming Psoriasis Care: Probiotics and Prebiotics as Novel Therapeutic Approaches. International Journal of Molecular Sciences. 2023; 24(13):11225. https://doi.org/10.3390/ijms241311225
Chicago/Turabian StyleBuhaș, Mihaela Cristina, Rareș Candrea, Laura Ioana Gavrilaș, Doina Miere, Alexandru Tătaru, Andreea Boca, and Adrian Cătinean. 2023. "Transforming Psoriasis Care: Probiotics and Prebiotics as Novel Therapeutic Approaches" International Journal of Molecular Sciences 24, no. 13: 11225. https://doi.org/10.3390/ijms241311225
APA StyleBuhaș, M. C., Candrea, R., Gavrilaș, L. I., Miere, D., Tătaru, A., Boca, A., & Cătinean, A. (2023). Transforming Psoriasis Care: Probiotics and Prebiotics as Novel Therapeutic Approaches. International Journal of Molecular Sciences, 24(13), 11225. https://doi.org/10.3390/ijms241311225