
Anti-β2-glycoprotein I/HLA-DR Antibody and Adverse Obstetric Outcomes

 ,
,
Abstract
1. Introduction
2. Results
2.1. Anti-β2GPI/HLA-DR Antibody in Women with RPL
2.2. Anti-β2GPI/HLA-DR Antibody in Women with FGR
2.3. Anti-β2GPI/HLA-DR Antibody in Women with HDP
2.4. Anti-β2GPI/HLA-DR Antibody in Women with PD before 34 GWs
2.5. Associations between Anti-β2GPI/HLA-DR Antibody and Adverse Obstetric Outcomes
3. Discussion
4. Materials and Methods
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jiang, Y.; Arase, N.; Kohyama, M.; Hirayasu, K.; Suenaga, T.; Jin, H.; Matsumoto, M.; Shida, K.; Lanier, L.L.; Saito, T.; et al. Transport of misfolded endoplasmic reticulum proteins to the cell surface by MHC class II molecules. Int. Immunol. 2013, 25, 235–246. [Google Scholar] [CrossRef]
- Jin, H.; Arase, N.; Hirayasu, K.; Kohyama, M.; Suenaga, T.; Saito, F.; Tanimura, K.; Matsuoka, S.; Ebina, K.; Shi, K.; et al. Autoantibodies to IgG/HLA class II complexes are associated with rheumatoid arthritis susceptibility. Proc. Natl. Acad. Sci. USA 2014, 111, 3787–3792. [Google Scholar] [CrossRef]
- Hiwa, R.; Ohmura, K.; Arase, N.; Jin, H.; Hirayasu, K.; Kohyama, M.; Suenaga, T.; Saito, F.; Terao, C.; Atsumi, T.; et al. Myeloperoxidase/HLA Class II Complexes Recognized by Autoantibodies in Microscopic Polyangiitis. Arthritis Rheumatol. 2017, 69, 2069–2080. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Kishida, K.; Arase, N.; Matsuoka, S.; Nakai, W.; Kohyama, M.; Suenaga, T.; Yamamoto, K.; Sasazuki, T.; Arase, H. Abrogation of self-tolerance by misfolded self-antigens complexed with MHC class II molecules. Sci. Adv. 2022, 8, eabj9867. [Google Scholar] [CrossRef]
- Tsuji, H.; Ohmura, K.; Jin, H.; Naito, R.; Arase, N.; Kohyama, M.; Suenaga, T.; Sakakibara, S.; Kochi, Y.; Okada, Y.; et al. Anti-Double-Stranded DNA Antibodies Recognize DNA Presented on HLA Class II Molecules of Systemic Lupus Erythematosus Risk Alleles. Arthritis Rheumatol. 2022, 74, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.W.M.; De Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- McNeil, H.P.; Simpson, R.J.; Chesterman, C.N.; Krilis, S.A. Anti-phospholipid antibodies are directed against a complex antigen that includes a lipid-binding inhibitor of coagulation: b2-glycoprotein I (apolipoprotein H). Proc. Natl. Acad. Sci. USA 1990, 87, 4120–4124. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Barbui, T.; Zwaal, R.F.; Comfurius, P.; Bevers, E.M. Antiphospholipid antibodies: Involvement of protein cofactors. Haematologica 1993, 78, 1–4. [Google Scholar]
- Matsuura, E.; Igarashi, Y.; Yasuda, T.; Triplett, D.A.; Koike, T. Anticardiolipin antibodies recognize b2-glycoprotein I structure altered by interacting with an oxygen modified solid phase surface. J. Exp. Med. 1994, 179, 457–462. [Google Scholar] [CrossRef]
- Schwarzenbacher, R.; Zeth, K.; Diederichs, K.; Gries, A.; Kostner, G.M.; Laggner, P.; Prassl, R. Crystal structure of human b2-glycoprotein I: Implications for phospholipid binding and the antiphospholipid syndrome. EMBO J. 1999, 18, 6228–6239. [Google Scholar] [CrossRef]
- Tanimura, K.; Jin, H.; Suenaga, T.; Morikami, S.; Arase, N.; Kishida, K.; Hirayasu, K.; Kohyama, M.; Ebina, Y.; Yasuda, S.; et al. b2-Glycoprotein I/HLA class II complexes are novel autoantigens in antiphospholipid syndrome. Blood 2015, 125, 2835–2844. [Google Scholar] [CrossRef]
- Tanimura, K.; Saito, S.; Nakatsuka, M.; Nagamatsu, T.; Fujii, T.; Fukui, A.; Deguchi, M.; Sasagawa, Y.; Arase, N.; Arase, H.; et al. The b2-Glycoprotein I/HLA-DR Complex as a Major Autoantibody Target in Obstetric Antiphospholipid Syndrome. Arthritis Rheumatol. 2020, 72, 1882–1891. [Google Scholar] [CrossRef] [PubMed]
- Soderberg, O.; Gullberg, M.; Jarvius, M.; Ridderstrale, K.; Leuchowius, K.J.; Jarvius, J.; Wester, K.; Hydbring, P.; Bahram, F.; Larsson, L.G.; et al. Direct observation of individual endogenous protein complexes in situ by proximity ligation. Nat. Methods 2006, 3, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, K.; Khamashta, M.A.; Koike, T.; Matsuura, E.; Hughes, G.R. b2-Glycoprotein I reactivity of monoclonal anticardiolipin antibodies from patients with the antiphospholipid syndrome. Arthritis Rheum. 1994, 37, 1453–1461. [Google Scholar] [CrossRef]
- Stepan, H.; Hund, M.; Andraczek, T. Combining Biomarkers to Predict Pregnancy Complications and Redefine Preeclampsia: The Angiogenic-Placental Syndrome. Hypertension 2020, 75, 918–926. [Google Scholar] [CrossRef]
- Wang, A.; Rana, S.; Karumanchi, S.A. Preeclampsia: The role of angiogenic factors in its pathogenesis. Physiology 2009, 24, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.F. Infection in the prediction and antibiotics in the prevention of spontaneous preterm labour and preterm birth. BJOG 2003, 110 (Suppl. 2), 71–75. [Google Scholar] [CrossRef]
- Lockwood, C.J. Predicting premature delivery—No easy task. N. Engl. J. Med. 2002, 346, 282–284. [Google Scholar] [CrossRef]
- Arase, N.; Tanimura, K.; Jin, H.; Yamaoka, T.; Kishibe, M.; Nishioka, M.; Kiyohara, E.; Tani, M.; Matsuoka, S.; Ohmura, K.; et al. Novel autoantibody against the b2-glycoprotein I/human leucocyte antigen-DR complex in patients with refractory cutaneous ulcers. Br. J. Dermatol. 2018, 178, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Agar, C.; van Os, G.M.; Morgelin, M.; Sprenger, R.R.; Marquart, J.A.; Urbanus, R.T.; Derksen, R.H.; Meijers, J.C.; de Groot, P.G. b2-glycoprotein I can exist in 2 conformations: Implications for our understanding of the antiphospholipid syndrome. Blood 2010, 116, 1336–1343. [Google Scholar] [CrossRef]
- Atik, R.B.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Mcheik, S.; Peramo, B.; Quenby, S.; Nielsen, H.S.; et al. ESHRE guideline: Recurrent pregnancy loss: An update in 2022. Hum. Reprod. Open. 2022, 2023, hoad002. [Google Scholar]
- ACOG Committee Opinion No. 743: Low-Dose Aspirin Use During Pregnancy. Obstet. Gynecol. 2018, 132, e44–e52. [CrossRef]
- ACOG Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obstet. Gynecol. 2019, 133, 1.
- Ono, Y.; Wada, S.; Ota, H.; Fukushi, Y.; Tanimura, K.; Yoshino, O.; Arase, H.; Yamada, H. Anti-b2-glycoprotein I/HLA-DR antibody in fertility. J. Reprod. Immunol. 2023, 158, 103955. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2020, 113, 533–535. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| RPL n = 462 | Control n = 488 | p-Value | |
|---|---|---|---|
| Age (years) | 35.5 ± 4.7 | 33.6 ± 5.3 | <0.001 |
| BMI (kg/m2) | 21.5 ± 3.5 | 22.5 ± 4.4 | <0.001 |
| Gravidity (no) | 3.7 ± 1.7 | 1.9 ± 1.0 | <0.001 |
| Parity (no) | 0.5 ± 0.7 | 0.8 ± 0.8 | <0.001 |
| History of spontaneous miscarriages (no) | 2.8 ± 1.4 | 0.1 ± 0.3 | <0.001 |
| History of stillbirths at 22 GWs or later (no) | 0.05 ± 0.3 | 0.01 ± 0.09 | <0.001 |
| History of thrombosis | 4 (0.9%) | 0 (0%) | 0.06 |
| Autoimmune diseases | 34 (7.4%) | 0 (0%) | <0.001 |
| Use of immunosuppressive drugs | 9 (1.9%) | 0 (0%) | <0.01 |
| Chronic hypertension | 2 (0.4%) | 0 (0%) | 0.2 |
| Smoking habit | 41 (8.9%) | 40 (8.2%) | 0.8 |
| Anti-β2GPI/HLA-DR antibody positive | 78 (16.9%) | 27 (5.5%) | <0.001 |
| Total n = 462 | Anti-β2GPI/HLA-DR–Positive Women with RPL n = 78 | Anti-β2GPI/HLA-DR–Negative Women with RPL n = 384 | p-Value | |
|---|---|---|---|---|
| Age (years) | 35.5 ± 4.7 | 34.9 ± 4.9 | 35.7 ± 4.6 | 0.2 |
| BMI (kg/m2) | 21.5 ± 3.5 | 22.2 ± 3.9 | 21.4 ± 3.4 | 0.08 |
| Gravidity (no) | 3.7 ± 1.7 | 3.4 ± 1.4 | 3.7 ± 1.7 | 0.1 |
| Parity (no) | 0.5 ± 0.7 | 0.4 ± 0.6 | 0.5 ± 0.7 | 0.3 |
| History of spontaneous miscarriages (no) | 2.8 ± 1.4 | 2.5 ± 1.3 | 2.8 ± 1.4 | 0.06 |
| History of stillbirths at 22 GWs or later (no) | 0.1 ± 0.3 | 0.1 ± 0.4 | 0.0 ± 0.2 | 0.2 |
| History of thrombosis | 4 (0.9%) | 2 (2.6%) | 2 (0.5%) | 0.1 |
| Autoimmune diseases | 34 (7.4%) | 15 (19.2%) | 19 (4.9%) | <0.001 |
| Use of immunosuppressive drugs | 9 (1.9%) | 4 (5.1%) | 5 (1.3%) | <0.05 |
| Chronic hypertension | 2 (0.4%) | 0 (0%) | 2 (0.5%) | 1.0 |
| Smoking habit | 41 (8.9%) | 8 (10.3%) | 33 (8.6%) | 0.6 |
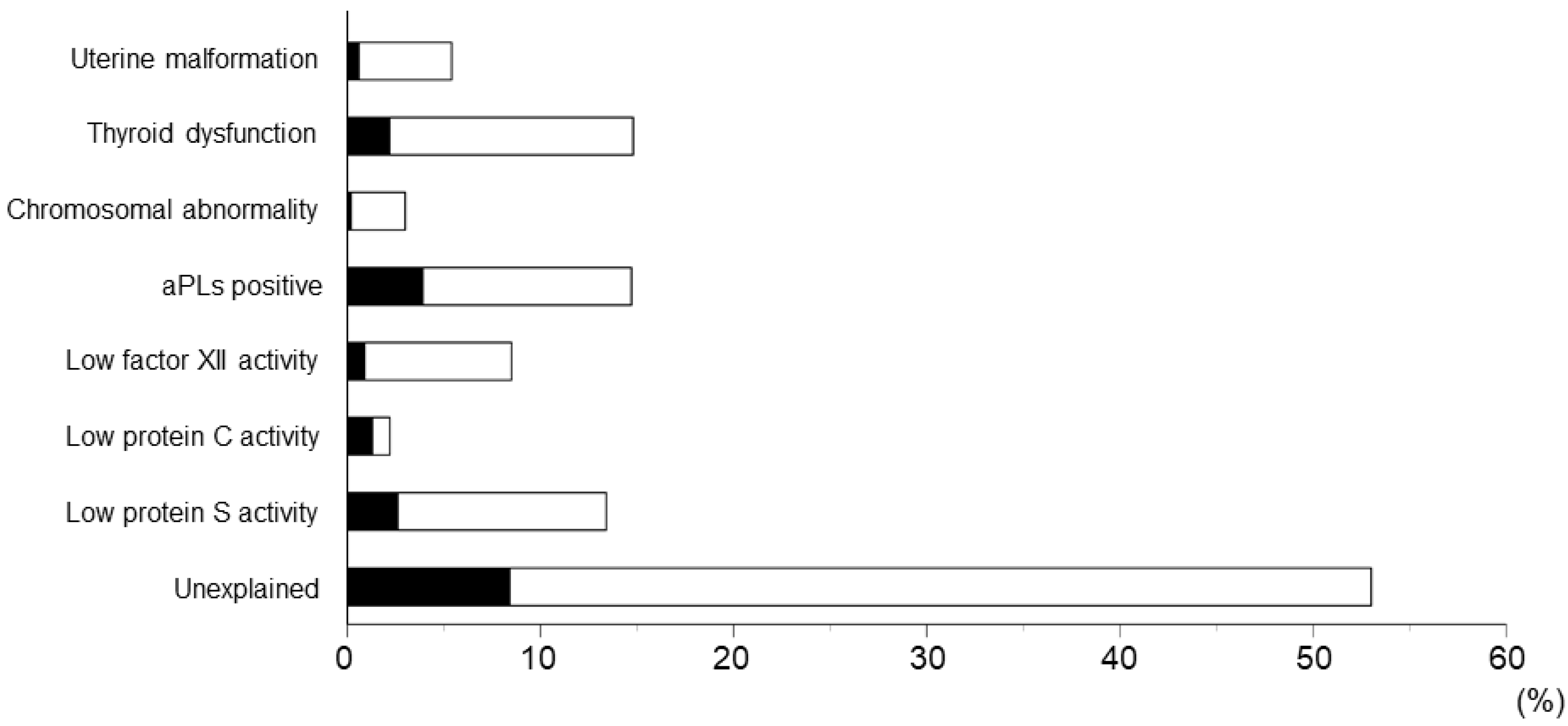
| Uterine malformation | 25 (5.4%) | 3 (3.8%) | 22 (5.7%) | 0.8 |
| Thyroid dysfunction | 68 (14.7%) | 10 (12.8%) | 58 (15.1%) | 0.7 |
| Chromosomal abnormality | 14 (3.0%) | 1 (1.3%) | 13 (3.4%) | 0.5 |
| aPL positive | 68 (14.7%) | 18 (23.1%) | 50 (13.0%) | <0.05 |
| Low factor XII activity | 39 (8.4%) | 4 (5.1%) | 35 (9.1%) | 0.4 |
| Low protein C activity | 10 (2.2%) | 6 (7.7%) | 4 (1.0%) | 0.4 |
| Low protein S activity | 62 (13.4%) | 12 (15.4%) | 50 (13.0%) | 0.7 |
| Unexplained | 245 (53.0%) | 39 (50.0%) | 206 (53.6%) | 0.6 |
| FGR | Control n = 488 | |||
|---|---|---|---|---|
| Previous n = 49 | Current n = 83 | All n = 124 | ||
| Age (years) | 33.6 ± 4.1 | 31.6 ± 5.2 ** | 32.4 ± 5.0 * | 33.6 ± 5.3 |
| BMI (kg/m2) | 22.3 ± 4.4 | 23.3 ± 5.0 | 22.8 ± 4.6 | 22.5 ± 4.4 |
| Gravidity (no) | 2.7 ± 1.2 ** | 2.1 ± 1.2 | 2.3 ± 1.3 ** | 1.9 ± 1.0 |
| Parity (no) | 1.2 ± 0.8 ** | 0.7 ± 0.9 | 0.9 ± 0.9 | 0.8 ± 0.8 |
| History of spontaneous miscarriages (no) | 0.4 ± 0.8 ** | 0.3 ± 0.7 ** | 0.3 ± 0.7 ** | 0.1 ± 0.3 |
| History of stillbirths at 22 GWs or later (no) | 0.1 ± 0.3 * | 0 | 0.05 ± 0.2 | 0.01 ± 0.09 |
| History of thrombosis | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Autoimmune diseases | 5 (10.2%) ** | 4 (4.8%) ** | 7 (5.7%) ** | 0 (0%) |
| Use of immunosuppressive drugs | 1 (2.0%) | 2 (2.4%) * | 2 (1.6%) * | 0 (0%) |
| Chronic hypertension | 2 (4.0%) ** | 2 (2.4%) * | 3 (2.4%) ** | 0 (0%) |
| Smoking habit | 1 (2.0%) | 6 (7.2%) | 7 (5.7%) | 40 (8.2%) |
| Pregnancy following ART | 7 (14.3%) | 8 (9.6%) | 13 (10.5%) | 75 (15.3%) |
| Anti-β2GPI/HLA-DR antibody positive | 9 (18.4%) ** | 12 (14.5%) ** | 19 (15.3%) ** | 27 (5.5%) |
| HDP | Control n = 488 | |||
|---|---|---|---|---|
| Previous n = 64 | Current n = 79 | All n = 138 | ||
| Age (years) | 35.4 ± 4.3 ** | 35.0 ± 5.6 * | 35.1 ± 5.0 ** | 33.6 ± 5.3 |
| BMI (kg/m2) | 23.2 ± 4.7 | 24.8 ± 6.5 ** | 24.0 ± 5.9 * | 22.5 ± 4.4 |
| Gravidity (no) | 2.3 ± 1.2 * | 1.9 ± 1.0 | 2.0 ± 1.1 | 1.9 ± 1.0 |
| Parity (no) | 1.0 ± 0.8 | 0.6 ± 0.7 | 0.8 ± 0.8 | 0.8 ± 0.8 |
| History of spontaneous miscarriages (no) | 0.4 ± 0.8 ** | 0.3 ± 0.6 * | 0.3 ± 0.7 ** | 0.1 ± 0.3 |
| History of stillbirths at 22 GWs or later (no) | 0.06 ± 0.2 | 0.02 ± 0.1 | 0.04 ± 0.2 | 0.01 ± 0.09 |
| History of thrombosis | 1 (1.6%) | 0 (0%) | 1 (0.7%) | 0 (0%) |
| Autoimmune diseases | 3 (4.7%) ** | 6 (7.6%) ** | 9 (6.5%) ** | 0 (0%) |
| Use of immunosuppressive drugs | 1 (1.6%) | 3 (3.8%) ** | 4 (2.9%) ** | 0 (0%) |
| Chronic hypertension | 10 (15.6%) ** | 17 (21.5%) ** | 24 (17.4%) ** | 0 (0%) |
| Smoking habit | 1 (1.6%) | 13 (16.5%) * | 14 (10.1%) | 40 (8.2%) |
| Pregnancy following ART | 16 (25.0%) | 14 (17.7%) | 28 (20.3%) | 75 (15.3%) |
| Anti-β2GPI/HLA-DR antibody positive | 12 (18.8%) ** | 13 (16.5%) ** | 24 (17.4%) ** | 27 (5.5%) |
| Preterm Delivery ≤ 34 GW | Control n = 488 | |||
|---|---|---|---|---|
| Prior n = 35 | Current n = 39 | All n = 71 | ||
| Age (years) | 35.3 ± 4.3 * | 34.4 ± 4.8 | 34.9 ± 4.6 * | 33.6 ± 5.3 |
| BMI (kg/m2) | 21.7 ± 2.7 | 22.7 ± 2.9 | 22.2 ± 2.9 | 22.5 ± 4.4 |
| Gravidity (no) | 2.7 ± 1.3 ** | 2.3 ± 1.0 ** | 2.5 ± 1.2 ** | 1.9 ± 1.0 |
| Parity (no) | 1.3 ± 0.8 ** | 1.0 ± 0.8 | 1.1 ± 0.8 ** | 0.8 ± 0.8 |
| History of spontaneous miscarriages (no) | 0.5 ± 1.1 | 0.4 ± 0.8 * | 0.5 ± 0.9 ** | 0.1 ± 0.3 |
| History of stillbirths at 22 GWs or later (no) | 0.1 ± 0.3 | 0.03 ± 0.2 | 0.07 ± 0.3 | 0.01 ± 0.09 |
| History of thrombosis | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Autoimmune diseases | 3 (8.6%) ** | 2 (5.1%) ** | 5 (7.0%) ** | 0 (0%) |
| Use of immunosuppressive drugs | 2 (5.7%) ** | 0 (0%) | 2 (2.8%) * | 0 (0%) |
| Chronic hypertension | 3 (8.6%) ** | 1 (2.6%) | 4 (5.6%) ** | 0 (0%) |
| Smoking habit | 5 (14.3%) | 5 (12.8%) | 10 (14.1%) | 40 (8.2%) |
| Pregnancy following ART | 5 (14.3%) | 5 (12.8%) | 10 (14.1%) | 75 (15.3%) |
| Anti-β2GPI/HLA-DR antibody positive | 5 (14.3%) | 3 (7.7%) | 8 (11.3%) | 27 (5.5%) |
| Adverse Obstetric Outcome | Crude OR | 95% CI | p-Value | Adjusted OR * | 95% CI | p-Value | |
|---|---|---|---|---|---|---|---|
| RPL | n = 462 | 3.5 | 2.2–5.5 | <0.001 | 3.3 | 1.9–5.6 | <0.001 |
| FGR | |||||||
| Previous | n = 49 | 3.8 | 1.7–8.7 | <0.005 | 3.1 | 1.2–8.0 | <0.05 |
| Current | n = 83 | 2.9 | 1.4–6.0 | <0.005 | 2.6 | 1.2–5.6 | <0.05 |
| All | n = 124 | 3.1 | 1.7–5.8 | <0.001 | 2.7 | 1.3–5.3 | <0.01 |
| HDP | |||||||
| Previous | n = 64 | 3.9 | 1.9–8.2 | <0.001 | 2.5 | 1.01–6.2 | <0.05 |
| Current | n = 79 | 3.4 | 1.7–6.8 | <0.001 | 2.7 | 1.2–6.0 | <0.05 |
| All | n = 138 | 3.6 | 2.0–6.5 | <0.001 | 2.7 | 1.4–5.3 | <0.01 |
| PD ≤ 34 GWs | |||||||
| Previous | n = 35 | 2.8 | 1.02–7.9 | <0.05 | 2.9 | 0.9–9.2 | 0.08 |
| Current | n = 39 | 1.4 | 0.4–5.0 | 0.6 | 1.7 | 0.5–6.0 | 0.4 |
| All | n = 71 | 2.2 | 0.9–5.0 | 0.07 | 2.3 | 0.9–5.7 | 0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanimura, K.; Saito, S.; Tsuda, S.; Ono, Y.; Ota, H.; Wada, S.; Deguchi, M.; Nakatsuka, M.; Nagamatsu, T.; Fujii, T.; et al. Anti-β2-glycoprotein I/HLA-DR Antibody and Adverse Obstetric Outcomes. Int. J. Mol. Sci. 2023, 24, 10958. https://doi.org/10.3390/ijms241310958
Tanimura K, Saito S, Tsuda S, Ono Y, Ota H, Wada S, Deguchi M, Nakatsuka M, Nagamatsu T, Fujii T, et al. Anti-β2-glycoprotein I/HLA-DR Antibody and Adverse Obstetric Outcomes. International Journal of Molecular Sciences. 2023; 24(13):10958. https://doi.org/10.3390/ijms241310958
Chicago/Turabian StyleTanimura, Kenji, Shigeru Saito, Sayaka Tsuda, Yosuke Ono, Hajime Ota, Shinichiro Wada, Masashi Deguchi, Mikiya Nakatsuka, Takeshi Nagamatsu, Tomoyuki Fujii, and et al. 2023. "Anti-β2-glycoprotein I/HLA-DR Antibody and Adverse Obstetric Outcomes" International Journal of Molecular Sciences 24, no. 13: 10958. https://doi.org/10.3390/ijms241310958
APA StyleTanimura, K., Saito, S., Tsuda, S., Ono, Y., Ota, H., Wada, S., Deguchi, M., Nakatsuka, M., Nagamatsu, T., Fujii, T., Kobashi, G., Arase, H., & Yamada, H. (2023). Anti-β2-glycoprotein I/HLA-DR Antibody and Adverse Obstetric Outcomes. International Journal of Molecular Sciences, 24(13), 10958. https://doi.org/10.3390/ijms241310958