
Celiac Disease and the Risk of Cardiovascular Diseases

 , ,
, , 
Abstract
1. Introduction
2. Clinical Presentation and Diagnosis
3. Pathophysiology of Celiac Disease
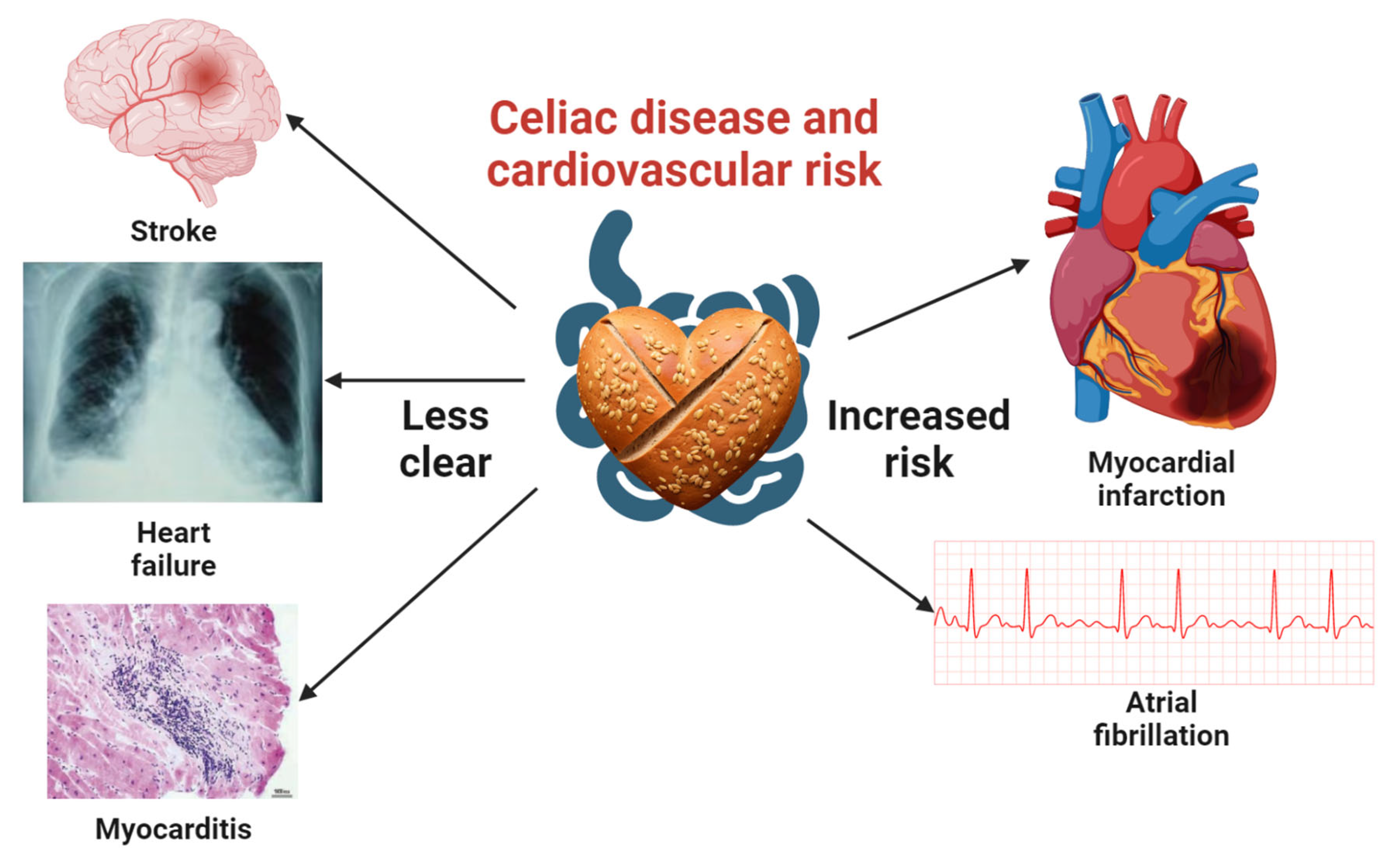
4. Association between Celiac Disease and Cardiovascular Diseases
4.1. CD and CVD Risk Factors
4.2. Celiac Disease and CVD
4.3. CD and Myocardial Infarction
4.4. CD and Stroke
4.5. CD and Cardiomyopathy/Heart Failure
4.6. CD and Cardiac Arrhythmias
4.7. Celiac Disease and Myopericarditis
5. Mechanism and Prevention of CVD
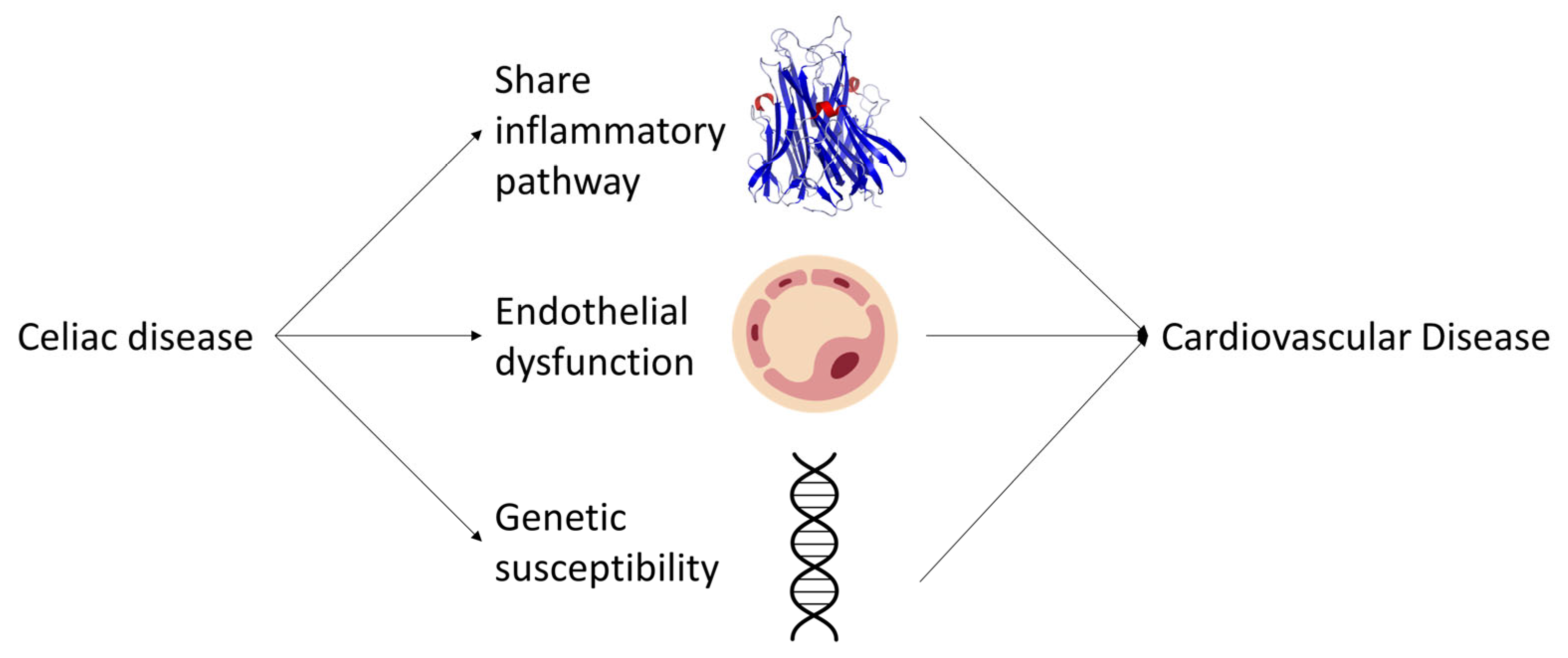
6. Molecular Mechanisms Linking CD and CVD
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e2. [Google Scholar] [CrossRef]
- Wei, L.; Spiers, E.; Reynolds, N.; Walsh, S.; Fahey, T.; Macdonald, T.M. The association between coeliac disease and cardiovascular disease. Aliment. Pharmacol. Ther. 2008, 27, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Green, P.H.R.; Söderling, J.; Roelstraete, B.; Ludvigsson, J.F. Association Between Celiac Disease and Mortality Risk in a Swedish Population. JAMA 2020, 323, 1277–1285. [Google Scholar] [CrossRef]
- Kaukinen, K. Updates on systemic consequences of coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sanchez, M.I.; Silvester, J.A.; Lebwohl, B.; Leffler, D.A.; Anderson, R.P.; Therrien, A.; Kelly, C.P.; Verdu, E.F. Society for the Study of Celiac Disease position statement on gaps and opportunities in coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 875–884. [Google Scholar] [CrossRef]
- Ciaccio, E.J.; Lewis, S.K.; Biviano, A.B.; Iyer, V.; Garan, H.; Green, P.H. Cardiovascular involvement in celiac disease. World J. Cardiol. 2017, 9, 652–666. [Google Scholar] [CrossRef]
- Catassi, C.; Verdu, E.F.; Bai, J.C.; Lionetti, E. Coeliac disease. Lancet 2022, 399, 2413–2426. [Google Scholar] [CrossRef]
- Leffler, D.A.; Green, P.H.R.; Fasano, A. Extraintestinal manifestations of coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 561–571. [Google Scholar] [CrossRef]
- Husby, S.; Murray, J.A.; Katzka, D.A. AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease—Changing Utility of Serology and Histologic Measures: Expert Review. Gastroenterology 2019, 156, 885–889. [Google Scholar] [CrossRef]
- Nellikkal, S.S.; Hafed, Y.; Larson, J.J.; Murray, J.A.; Absah, I. High Prevalence of Celiac Disease Among Screened First-Degree Relatives. Mayo Clin. Proc. 2019, 94, 1807–1813. [Google Scholar] [CrossRef]
- Leonard, M.M.; Sapone, A.; Catassi, C.; Fasano, A. Celiac Disease and Nonceliac Gluten Sensitivity: A Review. JAMA 2017, 318, 647–656. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef]
- Sollid, L.M.; Qiao, S.-W.; Anderson, R.P.; Gianfrani, C.; Koning, F. Nomenclature and listing of celiac disease relevant gluten T-cell epitopes restricted by HLA-DQ molecules. Immunogenetics 2012, 64, 455–460. [Google Scholar] [CrossRef]
- Jones, E.Y.; Fugger, L.; Strominger, J.L.; Siebold, C. MHC class II proteins and disease: A structural perspective. Nat. Rev. Immunol. 2006, 6, 271–282. [Google Scholar] [CrossRef]
- Targan, S.R.; Kagnoff, M.F.; Brogan, M.D.; Shanahan, F. Immunologic Mechanisms in Intestinal Diseases. Ann. Intern. Med. 1987, 106, 853–870. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Sanders, D.S.; Grünewald, R.A.; Woodroofe, N.; Boscolo, S.; Aeschlimann, D. Gluten sensitivity: From gut to brain. Lancet Neurol. 2010, 9, 318–330. [Google Scholar] [CrossRef]
- Emilsson, L.; Carlsson, R.; Holmqvist, M.; James, S.; Ludvigsson, J.F. The characterisation and risk factors of ischaemic heart disease in patients with coeliac disease. Aliment. Pharmacol. Ther. 2013, 37, 905–914. [Google Scholar] [CrossRef]
- Conroy, M.; Allen, N.; Lacey, B.; Soilleux, E.; Littlejohns, T. Association between coeliac disease and cardiovascular disease: Prospective analysis of UK Biobank data. BMJ Med. 2023, 2, e000371. [Google Scholar] [CrossRef]
- Kim, S.; Chang, Y.; Cho, J.; Hong, Y.S.; Zhao, D.; Kang, J.; Jung, H.-S.; Yun, K.E.; Guallar, E.; Ryu, S.; et al. Life’s Simple 7 Cardiovascular Health Metrics and Progression of Coronary Artery Calcium in a Low-Risk Population. Arter. Thromb. Vasc. Biol. 2019, 39, 826–833. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Logan, R.F.A.; Card, T.; Smith, C.; Hubbard, R. Risk of vascular disease in adults with diagnosed coeliac disease: A population-based study. Aliment. Pharmacol. Ther. 2004, 20, 73–79. [Google Scholar] [CrossRef]
- Korkmaz, H.; Sozen, M.; Kebapcilar, L. Increased arterial stiffness and its relationship with inflammation, insulin, and insulin resistance in celiac disease. Eur. J. Gastroenterol. Hepatol. 2015, 27, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Sari, C.; Bayram, N.A.; Doğan, F.E.A.; Bastug, S.; Bolat, A.D.; Sarı, S.; Ersoy, O.; Bozkurt, E. The Evaluation of Endothelial Functions in Patients with Celiac Disease. Echocardiography 2012, 29, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, Z.; Demircioglu, K.; Sayar, S.; Kahraman, R.; Caklili, O.; Ozcan, F.B.; Kostek, O.; Baycan, O.F.; Doganay, H.L.; Caliskan, M. Lipid profile atherogenic indeces and their relation of epicardial fat thickness and carotid intima media thickness in Celiac disease. North Clin. Istanb. 2019, 6, 242–247. [Google Scholar] [CrossRef]
- Brar, P.; Kwon, G.Y.; Holleran, S.; Bai, D.; Tall, A.R.; Ramakrishnan, R.; Green, P.H. Change in Lipid Profile in Celiac Disease: Beneficial Effect of Gluten-Free Diet. Am. J. Med. 2006, 119, 786–790. [Google Scholar] [CrossRef]
- Pauschinger, M.; Noutsias, M.; Lassner, D.; Schultheiss, H.P.; Kuehl, U. Inflammation, ECG changes and pericardial effusion: Whom to biopsy in suspected myocarditis? Clin. Res. Cardiol. 2006, 95, 569–583. [Google Scholar] [CrossRef]
- Ran, H.H.; Zhang, R.; Lu, X.C.; Yang, B.; Fan, H.; Zhu, H.L. Imatinib-induced decompensated heart failure in an elderly patient with chronic myeloid leukemia: Case report and literature review. J. Geriatr. Cardiol. 2012, 9, 411–414. [Google Scholar] [CrossRef][Green Version]
- Heikkilä, K.; Koskinen, O.; Agarwal, A.; Tikkinen, K.; Mäki, M.; Kaukinen, K. Associations of coeliac disease with coronary heart disease and cerebrovascular disease: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 816–831. [Google Scholar] [CrossRef]
- Emilsson, L.; Lebwohl, B.; Sundstrom, J.; Ludvigsson, J.F. Cardiovascular disease in patients with coeliac disease: A systematic review and meta-analysis. Dig. Liver Dis. 2015, 47, 847–852. [Google Scholar] [CrossRef]
- Hervonen, K.; Alakoski, A.; Salmi, T.; Helakorpi, S.; Kautiainen, H.; Kaukinen, K.; Pukkala, E.; Collin, P.; Reunala, T. Reduced mortality in dermatitis herpetiformis: A population—Based study of 476 patients. Br. J. Dermatol. 2012, 167, 1331–1337. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; West, J.; Card, T.; Appelros, P. Risk of Stroke in 28,000 Patients with Celiac Disease: A Nationwide Cohort Study in Sweden. J. Stroke Cerebrovasc. Dis. 2012, 21, 860–867. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; James, S.; Askling, J.; Stenestrand, U.; Ingelsson, E. Nationwide Cohort Study of Risk of Ischemic Heart Disease in Patients with Celiac Disease. Circulation 2011, 123, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Grainge, M.J.; West, J.; Card, T.R.; Holmes, G.K.T. Causes of Death in People with Celiac Disease Spanning the Pre- and Post-Serology Era: A Population-Based Cohort Study from Derby, UK. Am. J. Gastroenterol. 2011, 106, 933–939. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; De Faire, U.; Ekbom, A.; Montgomery, S.M. Vascular disease in a population-based cohort of individuals hospitalised with coeliac disease. Heart 2007, 93, 1111–1115. [Google Scholar] [CrossRef]
- Solaymani-Dodaran, M.; West, J.; Logan, R.F. Long-Term Mortality in People with Celiac Disease Diagnosed in Childhood Compared with Adulthood: A Population-Based Cohort Study. Am. J. Gastroenterol. 2007, 102, 864–870. [Google Scholar] [CrossRef]
- Viljamaa, M.; Kaukinen, K.; Pukkala, E.; Hervonen, K.; Reunala, T.; Collin, P. Malignancies and mortality in patients with coeliac disease and dermatitis herpetiformis: 30-year population-based study. Dig. Liver Dis. 2006, 38, 374–380. [Google Scholar] [CrossRef]
- Peters, U.; Askling, J.; Gridley, G.; Ekbom, A.; Linet, M. Causes of Death in Patients Celiac Disease in a Population-Based Swedish Cohort. Arch. Intern. Med. 2003, 163, 1566–1572. [Google Scholar] [CrossRef]
- Corrao, G.; Corazza, G.R.; Bagnardi, V.; Brusco, G.; Ciacci, C.; Cottone, M.; Guidetti, C.S.; Usai, P.; Cesari, P.; Pelli, M.A.; et al. Mortality in patients with coeliac disease and their relatives: A cohort study. Lancet 2001, 358, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, A.; Whittaker, S.; Carpenter, L.; English, J. Mortality and cancer incidence in patients with dermatitis herpetiformis: A cohort study. Br. J. Dermatol. 1993, 129, 140–144. [Google Scholar] [CrossRef]
- Whorwell, P.; Alderson, M.; Foster, K.; Wright, R. Death from ischæmic heart-disease and malignancy in adult patients with cœliac disease. Lancet 1976, 308, 113–114. [Google Scholar] [CrossRef]
- Logan, R.F.; Rifkind, E.A.; Turner, I.D.; Ferguson, A. Mortality in celiac disease. Gastroenterology 1989, 97, 265–271. [Google Scholar] [CrossRef]
- Anderson, L.A.; McMillan, S.A.; Watson, R.G.P.; Monaghan, P.; Gavin, A.T.; Fox, C.; Murray, L.J. Malignancy and mortality in a population-based cohort of patients with coeliac disease or ‘gluten sensitivity’. World J. Gastroenterol. 2007, 13, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Conrad, N.; Verbeke, G.; Molenberghs, G.; Goetschalckx, L.; Callender, T.; Cambridge, G.; Mason, J.C.; Rahimi, K.; McMurray, J.J.V.; Verbakel, J.Y. Autoimmune diseases and cardiovascular risk: A population-based study on 19 autoimmune diseases and 12 cardiovascular diseases in 22 million individuals in the UK. Lancet 2022, 400, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Naaraayan, A.; Nimkar, A.; Jesmajian, S.; Gitler, B.; Acharya, P. Atherosclerotic Cardiovascular Disease Prevalence Among Patients with Celiac Disease in the United States: An Observational Study. Mayo Clin. Proc. 2021, 96, 666–676. [Google Scholar] [CrossRef] [PubMed]
- Curione, M.; Barbato, M.; De Biase, L.; Viola, F.; Russo, L.L.; Cardi, E. Prevalence of coeliac disease in idiopathic dilated cardiomyopathy. Lancet 1999, 354, 222–223. [Google Scholar] [CrossRef]
- Corazza, G.R.; Andreani, M.L.; Biagi, F.; Corrao, G.; Pretolani, S.; Giulianelli, G.; Ghironzi, G.; Gasbarrini, G. The Smaller Size of the ‘Coeliac Iceberg’ in Adults. Scand. J. Gastroenterol. 1997, 32, 917–919. [Google Scholar] [CrossRef]
- Fonager, K.; Sørensen, H.T.; Nørgård, B.; Thulstrup, A.M. Cardiomyopathy in Danish patients with coeliac disease. Lancet 1999, 354, 1561. [Google Scholar] [CrossRef]
- Bolia, R.; Srivastava, A.; Kapoor, A.; Yachha, S.K.; Poddar, U. Children with untreated coeliac disease have sub-clinical cardiac dysfunction: A longitudinal observational analysis. Scand. J. Gastroenterol. 2018, 53, 803–808. [Google Scholar] [CrossRef]
- Elfström, P.; Hamsten, A.; Montgomery, S.M.; Ekbom, A.; Ludvigsson, J.F. Cardiomyopathy, pericarditis and myocarditis in a population-based cohort of inpatients with coeliac disease. J. Intern. Med. 2007, 262, 545–554. [Google Scholar] [CrossRef]
- Gawałko, M.; Balsam, P.; Lodziński, P.; Grabowski, M.; Krzowski, B.; Opolski, G.; Kosiuk, J. Cardiac Arrhythmias in Autoimmune Diseases. Circ. J. 2020, 84, 685–694. [Google Scholar] [CrossRef]
- Emilsson, L.; Smith, J.G.; West, J.; Melander, O.; Ludvigsson, J.F. Increased risk of atrial fibrillation in patients with coeliac disease: A nationwide cohort study. Eur. Heart J. 2011, 32, 2430–2437. [Google Scholar] [CrossRef] [PubMed]
- Frustaci, A.; Cuoco, L.; Chimenti, C.; Pieroni, M.; Fioravanti, G.; Gentiloni, N.; Maseri, A.; Gasbarrini, G. Celiac disease associated with autoimmune myocarditis. Circulation 2002, 105, 2611–2618. [Google Scholar] [CrossRef] [PubMed]
- Corazza, G.R.; Frisoni, M.; Filipponi, C.; Gullo, L.; Poggi, V.M.; Gasbarrini, G. Investigation of QT interval in adult coeliac disease. BMJ 1992, 304, 1285. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Samy, L.; Barkun, A.; Huynh, T. Cardiac syncope in a woman with undiagnosed celiac disease. Can. Med. Assoc. J. 2017, 189, E365–E367. [Google Scholar] [CrossRef] [PubMed]
- Rubio, J.L.C.; Ortego, N.; Diez-Ruiz, A.; Guilarte, J.; De la Higuera-Iorres, J. Celiac Disease Presenting as Chronic Anemia Associated with Heart Block. Am. J. Gastroenterol. 1998, 93, 1391–1392. [Google Scholar] [CrossRef]
- Mah, M.W.; Priel, I.E.; Humen, D.P.; Brown, N.E.; Sproule, B.J. Idiopathic pulmonary hemosiderosis, complete heart block and celiac disease. Can. J. Cardiol. 1989, 5, 191–194. [Google Scholar]
- Mannarino, S.; Santacesaria, S.; Raso, I.; Fini, G.; Pozzi, E.; Cocuccio, C.; Calcaterra, V.; Zuccotti, G. Atrioventricular Block in Celiac Disease: An Unusual Clinical Presentation in a Child. A Case-Based Review. Children 2022, 9, 1627. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K.; Leducq Transatlantic Network on Atherothrombosis. Inflammation in Atherosclerosis: From Pathophysiology to Practice. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef]
- Lebwohl, B.; Cao, Y.; Zong, G.; Hu, F.B.; Green, P.H.R.; Neugut, A.I.; Rimm, E.B.; Sampson, L.; Dougherty, L.W.; Giovannucci, E.; et al. Long term gluten consumption in adults without celiac disease and risk of coronary heart disease: Prospective cohort study. BMJ 2017, 357, j1892. [Google Scholar] [CrossRef]
- Fry, L.; Madden, A.M.; Fallaize, R. An investigation into the nutritional composition and cost of gluten-free versus regular food products in the UK. J. Hum. Nutr. Diet. 2018, 31, 108–120. [Google Scholar] [CrossRef]
- Potter, M.D.E.; Brienesse, S.C.; Walker, M.M.; Boyle, A.; Talley, N.J. Effect of the gluten-free diet on cardiovascular risk factors in patients with coeliac disease: A systematic review. J. Gastroenterol. Hepatol. 2018, 33, 781–791. [Google Scholar] [CrossRef]
- Wang, Y.; Cao, Y.; Lebwohl, B.; Song, M.; Sun, Q.; Green, P.H.; Giovannucci, E.L.; Willett, W.C.; Chan, A.T. Gluten Intake and Risk of Digestive System Cancers in 3 Large Prospective Cohort Studies. Clin. Gastroenterol. Hepatol. 2022, 20, 1986–1996.e11. [Google Scholar] [CrossRef]
- Wang, Y.; Lebwohl, B.; Mehta, R.; Cao, Y.; Green, P.H.R.; Grodstein, F.; Jovani, M.; Lochhead, P.; Okereke, O.I.; Sampson, L.; et al. Long-term Intake of Gluten and Cognitive Function Among US Women. JAMA Netw. Open 2021, 4, e2113020. [Google Scholar] [CrossRef]
- Zong, G.; Lebwohl, B.; Hu, F.B.; Sampson, L.; Dougherty, L.W.; Willett, W.C.; Chan, A.T.; Sun, Q. Gluten intake and risk of type 2 diabetes in three large prospective cohort studies of US men and women. Diabetologia 2018, 61, 2164–2173. [Google Scholar] [CrossRef]
- Sapone, A.; Lammers, K.M.; Casolaro, V.; Cammarota, M.; Giuliano, M.T.; De Rosa, M.; Stefanile, R.; Mazzarella, G.; Tolone, C.; Russo, M.I.; et al. Divergence of gut permeability and mucosal immune gene expression in two gluten-associated conditions: Celiac disease and gluten sensitivity. BMC Med. 2011, 9, 23. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in Atherosclerosis. Arter. Thromb. Vasc. Biol. 2012, 32, 2045–2051. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Lerman, L.O.; Lerman, A. Endothelial Dysfunction: A Marker of Atherosclerotic Risk. Arter. Thromb. Vasc. Biol. 2003, 23, 168–175. [Google Scholar] [CrossRef]
- De Marchi, S.; Chiarioni, G.; Prior, M.; Arosio, E. Young adults with coeliac disease may be at increased risk of early atherosclerosis. Aliment. Pharmacol. Ther. 2013, 38, 162–169. [Google Scholar] [CrossRef]
- Zhernakova, A.; Elbers, C.C.; Ferwerda, B.; Romanos, J.; Trynka, G.; Dubois, P.C.; De Kovel, C.G.; Franke, L.; Oosting, M.; Barisani, D.; et al. Evolutionary and Functional Analysis of Celiac Risk Loci Reveals SH2B3 as a Protective Factor against Bacterial Infection. Am. J. Hum. Genet. 2010, 86, 970–977. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author | Publication Year | Type of Study | Method Used to Identify Celiac Disease | Study Duration | Patients, n | Country | Cardiovascular Disease-Related Outcomes | Effect Size | Adjusted Variables |
|---|---|---|---|---|---|---|---|---|---|
| Conroy | 2023 | Prospective cohort | Combination of self-report with verbal interview and hospital inpatient diagnosis | Patient enrolled from 2006 to 2010, with a median follow-up of 12.4 years | 2083 celiac disease, 467,012 without celiac disease | UK | Composite cardiovascular disease incidents (ischemic heart disease, myocardial infarction, and stroke) identified by diagnostic codes from hospital inpatient and death records. Primary outcome of this study. | Adjusted HR: 1.44 (1.26–1.65) | Sex, Townsend score, education, region, year of birth, year of recruitment, ethnicity, smoking, alcohol consumption, physical activity, family history of CVD, total cholesterol, glucose, antihypertensive use, cholesterol-lowering medication use, and diabetes |
| Conrad | 2022 | Retrospective cohort | Various diagnostic codes | Celiac disease was diagnosed between 2020 and 2017. Median follow-up 6.2 years (IQR 2.7–10.8) | 24,895 celiac disease, 1:5 matched to general population | UK | Composite cardiovascular disease incidents (aortic aneurysm, atrial fibrillation and flutter, supraventricular arrhythmias, conduction system disease, myocarditis and pericarditis of non-infectious origin, peripheral arterial disease, infective endocarditis, stroke (ischemic and hemorrhagic) or TIA, valve disorders (excluding congenital and rheumatic), and venous thromboembolism. Celiac disease belongs to a subgroup analysis of this study on 19 autoimmune diseases. | HR: 1.50 (1.33–1.69) | Matched by age, sex, socioeconomic status, region, and calendar year. No further adjustment of comorbidities |
| Naaraayan | 2021 | Cross-sectional | ICD-9 diagnostic codes | Hospitalization with diagnosis of celiac disease from 2005 to 2014. No follow-up (cross-sectional) | 227,172 adult hospitalizations with celiac disease, 1:5 matched to hospitalizations without celiac disease | US | ICD-9 identified atherosclerotic cardiovascular disease presence in hospital inpatient records. | Adjusted OR on matched groups: 0.98 (0.95–1.01) | Matched by age, sex, race, and calendar year to hospitalizations. Further adjusted to hypertension, diabetes, hyperlipidemia, obesity, chronic kidney disease, and smoking status |
| Lebwohl | 2020 | Retrospective cohort | Histopathologically diagnosed | Patients were diagnosed from 1969 to 2017, with a median follow-up of 12.5 years | 49,829 celiac disease, 1:5 matched to general population | Sweden | ICD-identified cardiovascular disease caused death. Secondary outcome of this study. | Matched and unadjusted HR:1.08 (1.02–1.13) Matched and adjusted HR: 1.03 (0.98–1.08) | Groups matched by age, sex, county, and calendar period. Further adjustment including education, Nordic country of birth, and medical comorbidities (type 1 diabetes, autoimmune thyroid disease, rheumatoid arthritis, and inflammatory bowel disease) |
| Ludvigsson | 2012 | Cohort, possibly mixture of retrospective and prospective | Serology-positive | Patients were diagnosed from 1969 to 2008. follow-up median and range 9 (0–40) years, mean and SD 10.4 (6.4) | 46,330 patients with positive celiac disease serology who underwent biopsy (regardless of biopsy results), up to 1:5 matched on age and sex to general population | Sweden | ICD-identified stroke (ischemic and hemorrhagic incidents. Primary outcome of this study. | Matched and unadjusted HR: 1.10 (1.01–1.19) Matched and adjusted HR: 1.11 (0.96–1.29) | Groups matched by age and sex. Further adjustments included type 1 diabetes, rheumatoid arthritis, use of hypertensive medication, and lipid-lowering therapy |
| Ludvigsson | 2011 | Cohort, possibly a mixture of retrospective and prospective | Small intestinal histopathology | Patients were diagnosed from 1969 to 2008. follow-up median and range 8 (0–39) years | 28,190 patients with biopsy-proven CD, up to 1:5, matched on age, sex, county, and calendar year to general population | Sweden | ICD-identified composite incident ischemic heart disease (myocardial infarction and angina pectoris) from hospital inpatient and death records. Primary outcome of this study. | Matched HR 1.19 (1.11–1.28) | Matched by age, sex, county, and calendar year |
| Grainge | 2011 | Prospective cohort | Biopsy-proven | Followed-up from 1978 until death or 2006. Median and IQR 6.2 (3.2–12.9) years | 1092 CD patients with at least 2 years of follow-up | Derby, UK | Cardiovascular disease caused death based on ICD-10 codes (I00-I99) assigned on death certificates. Secondary outcome of this study. | SMR 1.12 (0.82–1.50) | SMR generated using rates of cohorts stratified by 5-year age category, sex, and calendar year |
| Wei | 2008 | Community-based cohort, likely retrospective | Serology-positive or biopsy-proven | Average follow-up of 3.7 years | 367 CD patients and 5537 antiendomysial antibody negative comparators | Tayside, Scotland, UK | ICD-identified composite incident cardiovascular disease (ischemic heart disease, heart failure, cerebrovascular disease, or cardiovascular death) from hospital inpatient and death records. Primary outcome of this study. | Unadjusted HR: 1.10 (0.62–1.92) Adjusted HR for gluten-free prescriptions: 2.4 (1.32–4.42) | Multiple univariate adjustments (not listed in this table), including age, sex, deprivation, diabetes, previous cardiovascular hospitalization, cardiovascular drugs, allopurinol, glucocorticoids, NSAIDs, and folic acid, all of which have statistically insignificant results |
| Ludvigsson | 2007 | Prospective cohort | ICD diagnostic codes | Unclear, patients with <1 year of follow-up were excluded | 13,358 CD patients and 64,118 age- and sex-matched controls | Sweden | Hospital-based ICD-defined incident vascular diseases, including myocardial infarction, angina pectoris, heart failure, brain hemorrhage, and ischemic stroke. Primary outcome of this study. | Unadjusted HR and adjusted HR ranges from 1.24 to 1.46 for different cardiovascular diseases, all statistically significant | Matched by age and sex. Further adjustment for diabetes |
| Solaymani Dodaran | 2007 | Population-based cohort, likely retrospective | Biopsy-proven | Mean 26, median 28 | 285 children and 340 adults were diagnosed with CD. Mortality compared to regional expected populational mortality rates | Lothian, Scotland, UK | Cerebrovascular disease and ischemic heart disease caused deaths. ICD-defined cause of death from death registry. Secondary outcome of this study. | SMR 1.38 (0.84–2.13) and 1.20 (0.84–1.67) for cerebrovascular disease and ischemic heart disease in adults | None |
| West | 2004 | Population-based retrospective cohort | Recorded diagnosis | Unclear, 0–10 years based on Kaplan–Meier curve | 3790 CD patients and 17,925 age- and sex-matched controls | UK | Incident myocardial infarction and stroke identified using recorded diagnosis. | Unadjusted HR for stroke 1.29 (0.98–1.70), for myocardial infarction 0.85 (0.63–1.13) | BMI, hypertension, and smoking were adjusted but not systemically reported |
| Corrao | 2001 | Prospective cohort | Biopsy-proven | Patients were diagnosed from 1962 to 1994. Mean follow-up 6.0 years (SD 4.9) | 1072 adult patients in patient cohort: 862 patients’ parents; 862 patients’ siblings | Italy | ICD-9 identified circulatory system diseases caused deaths. Secondary outcome of this study. | SMR in celiac disease cohort 0.7 (0.3–1.5) | Standardized for age, sex, and calendar year |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Chen, B.; Ciaccio, E.J.; Jneid, H.; Virani, S.S.; Lavie, C.J.; Lebovits, J.; Green, P.H.R.; Krittanawong, C. Celiac Disease and the Risk of Cardiovascular Diseases. Int. J. Mol. Sci. 2023, 24, 9974. https://doi.org/10.3390/ijms24129974
Wang Y, Chen B, Ciaccio EJ, Jneid H, Virani SS, Lavie CJ, Lebovits J, Green PHR, Krittanawong C. Celiac Disease and the Risk of Cardiovascular Diseases. International Journal of Molecular Sciences. 2023; 24(12):9974. https://doi.org/10.3390/ijms24129974
Chicago/Turabian StyleWang, Yichen, Bing Chen, Edward J. Ciaccio, Hani Jneid, Salim S. Virani, Carl J. Lavie, Jessica Lebovits, Peter H. R. Green, and Chayakrit Krittanawong. 2023. "Celiac Disease and the Risk of Cardiovascular Diseases" International Journal of Molecular Sciences 24, no. 12: 9974. https://doi.org/10.3390/ijms24129974
APA StyleWang, Y., Chen, B., Ciaccio, E. J., Jneid, H., Virani, S. S., Lavie, C. J., Lebovits, J., Green, P. H. R., & Krittanawong, C. (2023). Celiac Disease and the Risk of Cardiovascular Diseases. International Journal of Molecular Sciences, 24(12), 9974. https://doi.org/10.3390/ijms24129974