
The Efficacy of Molecular Analysis in the Diagnosis of Bone and Soft Tissue Sarcoma: A 15-Year Mono-Institutional Study
 and
and
Abstract
1. Introduction
2. Results
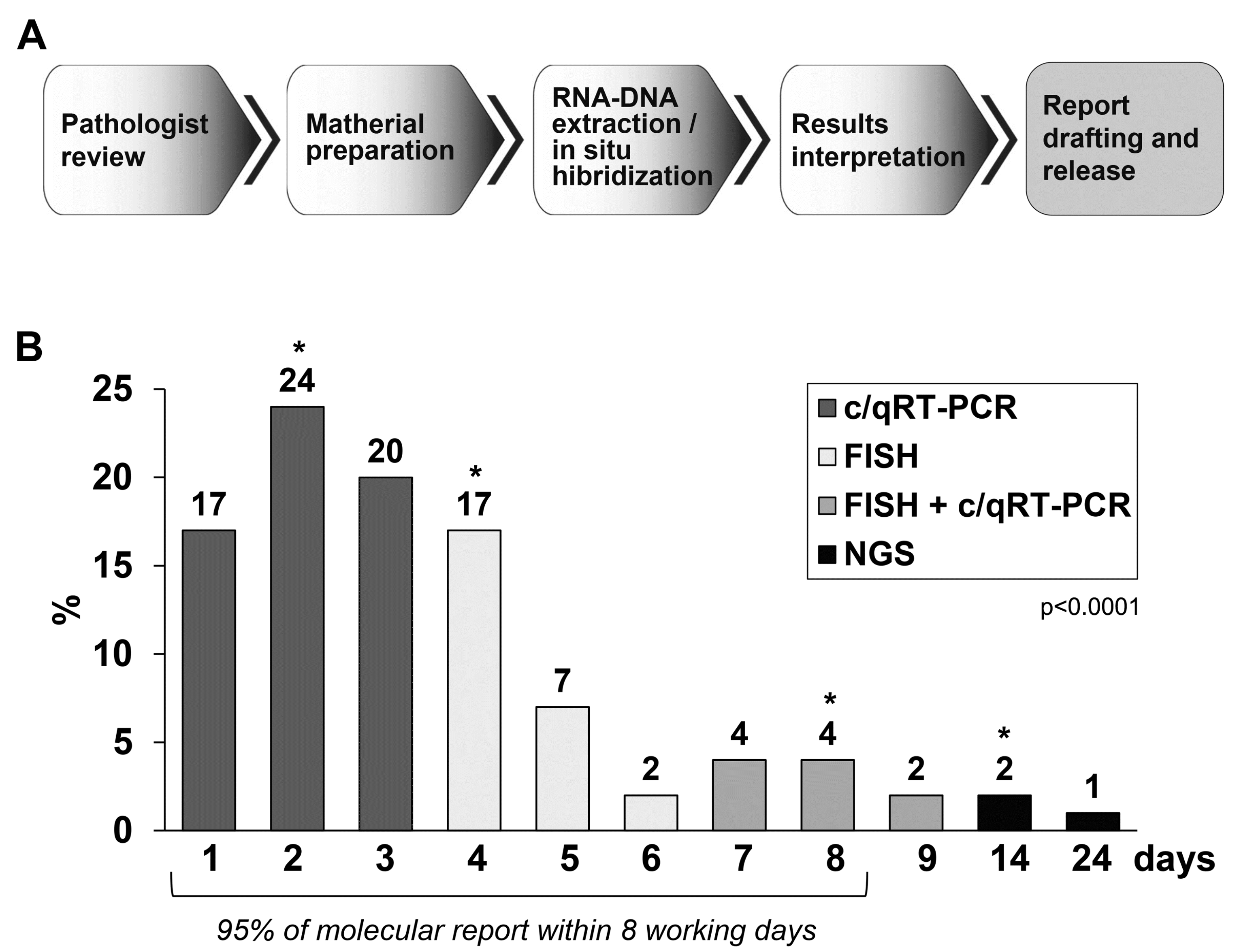
2.1. Molecular Methodology
2.2. Molecular Results
2.3. NGS Results
3. Discussion
4. Materials and Methods
4.1. Sample Collection
4.2. Molecular Testing
4.3. FISH Analysis
4.4. Anchored Multiplex PCR (AMP)-Based Targeted NGS
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antonescu, C.R.; Bridge, J.A.; Cunha, I.W. Soft tissue tumours. In WHO Classification of Tumours Editorial Board: Soft Tissue and Bone Tumours, 5th ed.; WHO Classification of Tumours Series; International Agency for Research on Cancer: Lyon, France, 2020. [Google Scholar]
- Bovée, J.V.M.G.; Flanagan, A.M.; Lazar, A.J.; Nielsen, G.P.; Yoshida, A. Bone tumours. In WHO Classification of Tumours Editorial Board: Soft Tissue and Bone Tumours, 5th ed.; WHO Classification of Tumours Series; International Agency for Research on Cancer: Lyon, France, 2020. [Google Scholar]
- Sbaraglia, M.; Bellan, E.; Tos, A.P.D. The 2020 WHO Classification of Soft Tissue Tumours: News and perspectives. Pathologica 2021, 113, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Antonescu, C.R.; Dal Cin, P. Promiscuous genes involved in recurrent chromosomal translocations in soft tissue tumours. Pathology 2014, 46, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Puls, F.; Niblett, A.J.; Mangham, D.C. Molecular pathology of bone tumours: Diagnostic implications. Histopathology 2014, 64, 461–476. [Google Scholar] [CrossRef]
- Lazar, A.; Abruzzo, L.V.; Pollock, R.E.; Lee, S.; Czerniak, B. Molecular Diagnosis of Sarcomas: Chromosomal Translocations in Sarcomas. Arch. Pathol. Lab. Med. 2006, 130, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, E.F.; Riegman, P.H.; Grizzle, W.E.; Watson, P. Factors that drive the increasing use of FFPE tissue in basic and translational cancer research. Biotech. Histochem. 2018, 93, 373–386. [Google Scholar] [CrossRef] [PubMed]
- van de Rijn, M.; Guo, X.; Sweeney, R.T.; Beck, A.H.; West, R.B. Molecular pathological analysis of sarcomas using paraffin-embedded tissue: Current limitations and future possibilities. Histopathology 2014, 64, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Asif, A.; Mushtaq, S.; Hassan, U.; Akhter, N.; Hussain, M.; Azam, M.; Qazi, R. Fluorescence in Situ Hybridization (FISH) for Differential Diagnosis of Soft Tissue Sarcomas. Asian Pac. J. Cancer Prev. 2018, 19, 655–660. [Google Scholar] [CrossRef]
- Scolnick, J.A.; Dimon, M.; Wang, I.-C.; Huelga, S.C.; Amorese, D.A. An Efficient Method for Identifying Gene Fusions by Targeted RNA Sequencing from Fresh Frozen and FFPE Samples. PLoS ONE 2015, 10, e0128916. [Google Scholar] [CrossRef]
- Miettinen, M.; Felisiak-Golabek, A.; Contreras, A.L.; Glod, J.; Kaplan, R.N.; Killian, J.K.; Lasota, J. New fusion sarcomas: Histopathology and clinical significance of selected entities. Hum. Pathol. 2019, 86, 57–65. [Google Scholar] [CrossRef]
- Benini, S.; Cocchi, S.; Gamberi, G.; Magagnoli, G.; Vogel, D.; Ghinelli, C.; Righi, A.; Picci, P.; Alberghini, M.; Gambarotti, M. Diagnostic Utility of Molecular Investigation in Extraskeletal Myxoid Chondrosarcoma. J. Mol. Diagn. 2014, 16, 314–323. [Google Scholar] [CrossRef]
- Zheng, Z.; Liebers, M.; Zhelyazkova, B.; Cao, Y.; Panditi, D.; Lynch, K.D.; Chen, J.; Robinson, H.E.; Shim, H.S.; Chmielecki, J.; et al. Anchored multiplex PCR for targeted next-generation sequencing. Nat. Med. 2014, 20, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.W.; Cleton-Jansen, A.-M.; Cleven, A.H.G.; Ruano, D.; van Wezel, T.; Szuhai, K.; Bovée, J.V.M.G. Molecular Analysis of Gene Fusions in Bone and Soft Tissue Tumors by Anchored Multiplex PCR–Based Targeted Next-Generation Sequencing. J. Mol. Diagn. 2018, 20, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Seager, M.; Aisner, D.L.; Davies, K.D. Oncogenic Gene Fusion Detection Using Anchored Multiplex Polymerase Chain Reaction Followed by Next Generation Sequencing. J. Vis. Exp. 2019, 149, e59895. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, S.; Gamberi, G.; Magagnoli, G.; Maioli, M.; Righi, A.; Frisoni, T.; Gambarotti, M.; Benini, S. CIC rearranged sarcomas: A single institution experience of the potential pitfalls in interpreting CIC FISH results. Pathol. Res. Pract. 2022, 231, 153773. [Google Scholar] [CrossRef]
- Di Novi, C.; Minniti, D.; Barbaro, S.; Zampirolo, M.G.; Cimino, A.; Bussolati, G. Vacuum-based preservation of surgical specimens: An environmentally-safe step towards a formalin-free hospital. Sci. Total Environ. 2010, 408, 3092–3095. [Google Scholar] [CrossRef]
- Benini, S.; Gamberi, G.; Cocchi, S.; Righi, A.; Frisoni, T.; Longhi, A.; Gambarotti, M. Identification of a novel fusion transcript EWSR1-VEZF1 by anchored multiplex PCR in malignant peripheral nerve sheath tumor. Pathol. Res. Pract. 2020, 216, 152760. [Google Scholar] [CrossRef]
- Thway, K.; Rockcliffe, S.; Gonzalez, D.; Swansbury, J.; Min, T.; Thompson, L.; Fisher, C. Utility of sarcoma-specific fusion gene analysis in paraffin-embedded material for routine diagnosis at a specialist centre. J. Clin. Pathol. 2010, 63, 508–512. [Google Scholar] [CrossRef]
- Neuville, A.; Ranchère-Vince, D.; Tos, A.D.; Montesco, M.; Hostein, I.; Toffolatti, L.; Chibon, F.; Pissaloux, D.; Alberti, L.; Decouvelaere, A.-V.; et al. Impact of Molecular Analysis on the Final Sarcoma Diagnosis. Am. J. Surg. Pathol. 2013, 37, 1259–1268. [Google Scholar] [CrossRef]
- Sbaraglia, M.; Tos, A.P.D. The pathology of soft tissue sarcomas. Radiol. Med. 2019, 124, 266–281. [Google Scholar] [CrossRef]
- Sbaraglia, M.; Righi, A.; Gambarotti, M.; Dei Tos, A.P. Ewing sarcoma and Ewing-like tumors. Virchows Arch. 2020, 476, 109–119. [Google Scholar] [CrossRef]
- Noujaim, J.; Jones, R.; Swansbury, J.; Gonzalez, D.; Benson, C.; Judson, I.; Fisher, C.; Thway, K. The spectrum of EWSR1-rearranged neoplasms at a tertiary sarcoma centre; assessing 772 tumour specimens and the value of current ancillary molecular diagnostic modalities. Br. J. Cancer 2017, 116, 669–678. [Google Scholar] [CrossRef]
- Vroobel, K.; Gonzalez, D.; Wren, D.; Thompson, L.; Swansbury, J.; Fisher, C.; Thway, K. Ancillary molecular analysis in the diagnosis of soft tissue tumours: Reassessment of its utility at a specialist centre. J. Clin. Pathol. 2016, 69, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Horn, H.; Allmanritter, J.; Doglioni, C.; Marx, A.; Müller, J.; Gattenlöhner, S.; Staiger, A.M.; Rosenwald, A.; Ott, G.; Ott, M.M. Fluorescence in situ analysis of soft tissue tumor associated genetic alterations in formalin-fixed paraffin-embedded tissue. Pathol. Res. Pract. 2014, 210, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Thway, K.; Wang, J.; Mubako, T.; Fisher, C. Histopathological Diagnostic Discrepancies in Soft Tissue Tumours Referred to a Specialist Centre: Reassessment in the Era of Ancillary Molecular Diagnosis. Sarcoma 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Kashofer, K.; Viertler, C.; Pichler, M.; Zatloukal, K. Quality Control of RNA Preservation and Extraction from Paraffin-Embedded Tissue: Implications for RT-PCR and Microarray Analysis. PLoS ONE 2013, 8, e70714. [Google Scholar] [CrossRef] [PubMed]
- Micke, P.; Ohshima, M.; Tahmasebpoor, S.; Ren, Z.-P.; Östman, A.; Pontén, F.; Botling, J. Biobanking of fresh frozen tissue: RNA is stable in nonfixed surgical specimens. Lab. Investig. 2006, 86, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Sun, R.; Hao, M.; Wang, Y.; Zhang, X.; Liu, Y.; Cong, X. Effect of Duration of Ex Vivo Ischemia Time and Storage Period on RNA Quality in Biobanked Human Renal Cell Carcinoma Tissue. Ann. Surg. Oncol. 2016, 23, 297–304. [Google Scholar] [CrossRef]
- Machado, I.; Noguera, R.; Pellin, A.; Lopez-Guerrero, J.A.; Piqueras, M.; Navarro, S.; Llombart-Bosch, A. Molecular Diagnosis of Ewing Sarcoma Family of Tumors: A comparative analysis of 560 cases with FISH and RT-PCR. Diagn. Mol. Pathol. 2009, 18, 189–199. [Google Scholar] [CrossRef]
- Srinivasan, M.; Sedmak, D.; Jewell, S. Effect of Fixatives and Tissue Processing on the Content and Integrity of Nucleic Acids. Am. J. Pathol. 2002, 161, 1961–1971. [Google Scholar] [CrossRef]
- Bussolati, G.; Annaratone, L.; Medico, E.; D’Armento, G.; Sapino, A. Formalin Fixation at Low Temperature Better Preserves Nucleic Acid Integrity. PLoS ONE 2011, 6, e21043. [Google Scholar] [CrossRef]
- Bussolati, G.; Chiusa, L.; Cimino, A.; D’Armento, G. Tissue transfer to pathology labs: Under vacuum is the safe alternative to formalin. Virchows Arch. 2008, 452, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, K.; Wang, Q.; Torres-Garcia, W.; Zheng, S.; Vegesna, R.; Kim, H.; Verhaak, R.G.W. The landscape and therapeutic relevance of cancer-associated transcript fusions. Oncogene 2015, 34, 4845–4854. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C. Soft tissue sarcomas with non-EWS translocations: Molecular genetic features and pathologic and clinical correlations. Virchows Arch. 2010, 456, 153–166. [Google Scholar] [CrossRef]
- Rupani, A.; Hallin, M.; Jones, R.L.; Fisher, C.; Thway, K.; Verhoef, C. Diagnostic Differences in Expert Second-Opinion Consultation Cases at a Tertiary Sarcoma Center. Sarcoma 2020, 2020, 9810170. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Q.; Goytain, A.; Dickson, B.C.; Nielsen, T.O. Advances in sarcoma molecular diagnostics. Genes, Chromosom. Cancer 2022, 61, 332–345. [Google Scholar] [CrossRef]
- Pei, J.; Zhao, X.; Patchefsky, A.S.; Flieder, D.B.; Talarchek, J.N.; Testa, J.R.; Wei, S. Clinical application of RNA sequencing in sarcoma diagnosis. Medicine 2019, 98, e16031. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumour Tested (Suspected Cases Based on Histology and IHC) | n. Cases Tested | n. c/qRT-PCR Tested | n. FISH Tested | n. c/qRT-PCR Positive | n. FISH Positive | n. c/qRT-PCR Failed | n. FISH Failed |
|---|---|---|---|---|---|---|---|
| Alveolar rhabdomyosarcoma | 47 | 30 | 25 | 23 | 6 | 6 | 7 |
| Alveolar soft part sarcoma | 17 | 14 | 5 | 14 | 2 | 1 | 0 |
| Aneurismal Bone cyst | 77 | 29 | 49 | 17 | 11 | 6 | 7 |
| Angiomatoid fibrous Histiocytoma | 8 | 6 | 5 | 4 | 2 | 2 | 0 |
| Cartilage-forming tumours (IDH1, IDH2) | 35 | 28 | n.a. | 17 | n.a. | 4 | n.a. |
| CIC-rearranged sarcoma | 35 | 21 | 25 | 18 | 13 | 6 | 2 |
| Clear cell sarcoma | 51 | 42 | 27 | 26 | 3 | 3 | 7 |
| Chondroblastoma (H3F3B) | 20 | 5 | n.a. | 9 | n.a. | 0 | n.a. |
| Dermatofibrosarcoma protuberans | 13 | 10 | 11 | 8 | 2 | 0 | 1 |
| Desmoplastic small round cell tumour | 9 | 6 | 6 | 5 | 2 | 0 | 0 |
| Epithelioid Haemangioendothelioma | 34 | 20 | 17 | 6 | 2 | 3 | 8 |
| Epithelioid Haemangioma | 10 | 9 | 2 | 2 | 0 | 1 | n.a. |
| Ewing sarcoma | 761 | 602 | 383 | 432 | 151 | 99 | 55 |
| Extraskeletal Myxoid Chondrosarcoma | 125 | 95 | 78 | 58 | 17 | 13 | 9 |
| Giant cell tumour of bone (H3F3A) | 71 | 71 | n.a. | 36 | n.a. | 2 | n.a. |
| Infantile sarcoma | 22 | 20 | 8 | 6 | 1 | 3 | 0 |
| Low-grade central osteosarcoma (MDM2) | 28 | n.a. | 28 | n.a. | 10 | n.a. | 5 |
| Low-grade fibromyxoid sarcoma | 9 | 8 | 1 | 8 | 1 | 0 | 0 |
| Mesenchymal Chondrosarcoma | 20 | 18 | 4 | 16 | 1 | 3 | 1 |
| Mixoid liposarcoma | 388 | 297 | 185 | 185 | 101 | 45 | 25 |
| Molecular counselling | 73 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Myoepithelial tumour | 13 | 5 | 13 | 0 | 3 | 5 | 1 |
| Parosteal osteosarcoma (MDM2) | 9 | n.a. | 9 | n.a. | 3 | n.a. | 2 |
| Pseudomyogenic Haemangioendothelioma | 3 | 3 | n.a. | 0 | n.a. | 3 | n.a. |
| Round cell sarcoma with EWSR1-non ETS fusions | 15 | 12 | 15 | 0 | 2 | 5 | 6 |
| Sarcoma with BCOR genetic alterations | 14 | 11 | 11 | 10 | 4 | 0 | 0 |
| Sclerosing Epithelioid Fibrosarcoma | 9 | 6 | 9 | 3 | 0 | 4 | 6 |
| Synovial sarcoma | 393 | 315 | 192 | 265 | 81 | 48 | 34 |
| Well/dedifferentiated liposarcoma MDM2 status | 396 | n.a. | 396 | n.a. | 156 | n.a. | 61 |
| BSTS Subtype | Molecular Test | Sensitivity | Specificity |
|---|---|---|---|
| Ewing sarcoma | c/qRT-PCR [t(11;22) t(t21;22)] | 94% | 100% |
| EWSR1 FISH | 85% | 94% | |
| Both test | 99% | 99% | |
| Synovial sarcoma | c/qRT-PCR t(X;18) | 95% | 100% |
| SS18 FISH | 75% | 100% | |
| Both test | 98% | 100% | |
| Mixoid liposarcoma | c/qRT-PCR [t(12;16) t(t12;22)] | 92% | 100% |
| DDIT3 FISH | 99% | 100% | |
| Both test | 99% | 100% | |
| Extraskeletal mixoid chondrosarcoma | c/qRT-PCR [t(9;22) t(t15;22) t(17;22)] | 88% | 100% |
| NR4A3 FISH | 94% | 100% | |
| Both test | 97% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benini, S.; Gamberi, G.; Cocchi, S.; Magagnoli, G.; Fortunato, A.R.; Sciulli, E.; Righi, A.; Gambarotti, M. The Efficacy of Molecular Analysis in the Diagnosis of Bone and Soft Tissue Sarcoma: A 15-Year Mono-Institutional Study. Int. J. Mol. Sci. 2023, 24, 632. https://doi.org/10.3390/ijms24010632
Benini S, Gamberi G, Cocchi S, Magagnoli G, Fortunato AR, Sciulli E, Righi A, Gambarotti M. The Efficacy of Molecular Analysis in the Diagnosis of Bone and Soft Tissue Sarcoma: A 15-Year Mono-Institutional Study. International Journal of Molecular Sciences. 2023; 24(1):632. https://doi.org/10.3390/ijms24010632
Chicago/Turabian StyleBenini, Stefania, Gabriella Gamberi, Stefania Cocchi, Giovanna Magagnoli, Angela Rosa Fortunato, Enrica Sciulli, Alberto Righi, and Marco Gambarotti. 2023. "The Efficacy of Molecular Analysis in the Diagnosis of Bone and Soft Tissue Sarcoma: A 15-Year Mono-Institutional Study" International Journal of Molecular Sciences 24, no. 1: 632. https://doi.org/10.3390/ijms24010632
APA StyleBenini, S., Gamberi, G., Cocchi, S., Magagnoli, G., Fortunato, A. R., Sciulli, E., Righi, A., & Gambarotti, M. (2023). The Efficacy of Molecular Analysis in the Diagnosis of Bone and Soft Tissue Sarcoma: A 15-Year Mono-Institutional Study. International Journal of Molecular Sciences, 24(1), 632. https://doi.org/10.3390/ijms24010632