
The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis

 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
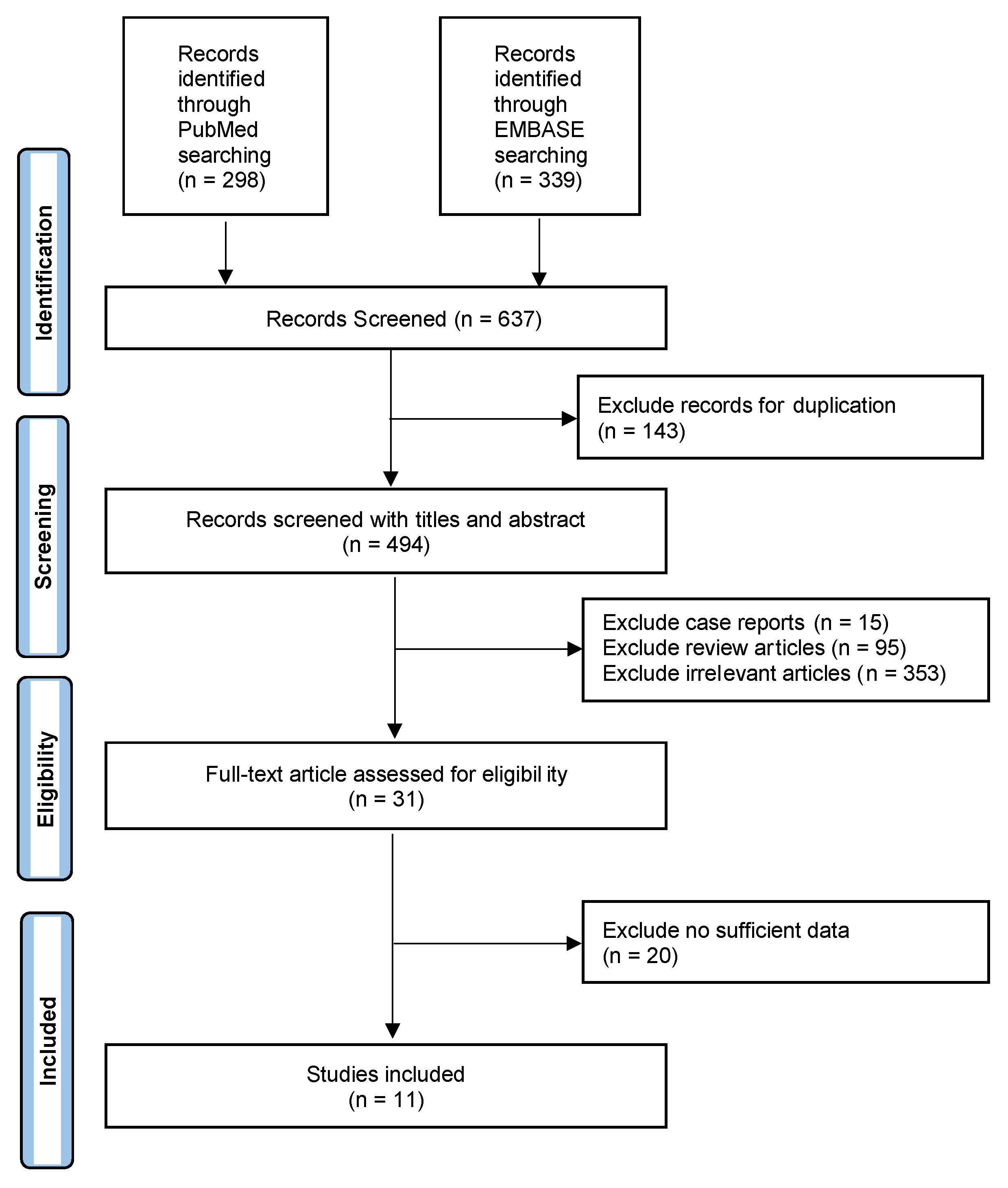
2.1. Search Strategy
2.2. Study Selection
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
3.1. Literature Search & Study Population
3.2. Detection of Extrathyroidal Extension by Ultrasound
3.3. Detection of Extrathyroidal Extension Sub-Group Analyses & Meta-regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Powers, A.E.; Marcadis, A.R.; Lee, M.; Morris, L.G.T.; Marti, J.L. Changes in Trends in Thyroid Cancer Incidence in the United States, 1992 to 2016. JAMA 2019, 322, 2440–2441. [Google Scholar] [CrossRef] [PubMed]
- Shaha, A.R. Implications of Prognostic Factors and Risk Groups in the Management of Differentiated Thyroid Cancer. Laryngoscope 2004, 114, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Sundram, F.; Robinson, B.G.; Kung, A.; Lim-Abrahan, M.A.; Bay, N.Q.; Chuan, L.K.; Chung, J.H.; Huang, S.-M.; Hsu, L.-C.; Kamaruddin, N. Well-Differentiated Epithelial Thyroid Cancer Management in the Asia Pacific Region: A Report and Clinical Practice Guideline. Thyroid 2006, 16, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Fligor, S.C.; Lopez, B.; Uppal, N.; Lubitz, C.C.; James, B.C. Time to Surgery and Thyroid Cancer Survival in the United States. Ann. Surg. Oncol. 2021, 28, 3556–3565. [Google Scholar] [CrossRef]
- Baloch, Z.W.; LiVolsi, V.A.; Asa, S.L.; Rosai, J.; Merino, M.J.; Randolph, G.; Vielh, P.; DeMay, R.M.; Sidawy, M.K.; Frable, W.J. Diagnostic Terminology and Morphologic Criteria for Cytologic Diagnosis of Thyroid Lesions: A Synopsis of the National Cancer Institute Thyroid Fine-Needle Aspiration State of the Science Conference. Diagn. Cytopathol. 2008, 36, 425–437. [Google Scholar] [CrossRef]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M. Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Hu, S.; Zhang, H.; Sun, Z.; Ge, Y.; Li, J.; Yu, C.; Deng, Z.; Dou, W.; Wang, X. Preoperative Assessment of Extrathyroidal Extension of Papillary Thyroid Carcinomas by Ultrasound and Magnetic Resonance Imaging: A Comparative Study. Radiol. Med. 2020, 125, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Ramundo, V.; Di Gioia, C.R.T.; Falcone, R.; Lamartina, L.; Biffoni, M.; Giacomelli, L.; Filetti, S.; Durante, C.; Grani, G. Diagnostic Performance of Neck Ultrasonography in the Preoperative Evaluation for Extrathyroidal Extension of Suspicious Thyroid Nodules. World J. Surg. 2020, 44, 2669–2674. [Google Scholar] [CrossRef] [PubMed]
- Jiao, W.-P.; Zhang, L. Using Ultrasonography to Evaluate the Relationship between Capsular Invasion or Extracapsular Extension and Lymph Node Metastasis in Papillary Thyroid Carcinomas. Chin. Med. J. 2017, 130, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.S.; Kim, S.S.; Kim, W.J.; Bae, M.J.; Kang, J.H.; Choi, B.G.; Jeon, Y.K.; Kim, B.H.; Lee, B.J.; Wang, S.G.; et al. Comparison of Two- and Three-Dimensional Sonography for the Prediction of the Extrathyroidal Extension of Papillary Thyroid Carcinomas. Korean J. Intern. Med. 2016, 31, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Kamaya, A.; Tahvildari, A.M.; Patel, B.N.; Willmann, J.K.; Jeffrey, R.B.; Desser, T.S. Sonographic Detection of Extracapsular Extension in Papillary Thyroid Cancer. J. Ultrasound Med. 2015, 34, 2225–2230. [Google Scholar] [CrossRef]
- Choi, J.S.; Lee, H.S.; Kim, E.-K.; Moon, H.J.; Kwak, J.Y. The Influence of Body Mass Index on the Diagnostic Performance of Pre-Operative Staging Ultrasound in Papillary Thyroid Carcinoma. Clin. Endocrinol. 2015, 83, 550–555. [Google Scholar] [CrossRef]
- Gweon, H.M.; Son, E.J.; Youk, J.H.; Kim, J.-A.; Park, C.S. Preoperative Assessment of Extrathyroidal Extension of Papillary Thyroid Carcinoma. J. Ultrasound Med. 2014, 33, 819–825. [Google Scholar] [CrossRef]
- Lee, C.Y.; Kim, S.J.; Ko, K.R.; Chung, K.-W.; Lee, J.-H. Predictive Factors for Extrathyroidal Extension of Papillary Thyroid Carcinoma Based on Preoperative Sonography. J. Ultrasound Med. 2014, 33, 231–238. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kwon, T.-K.; Sung, M.-W.; Kim, K.H.; Hah, J.H. Prediction of Extrathyroidal Extension Using Ultrasonography and Computed Tomography. Int. J. Endocrinol. 2014, 2014, 351058. [Google Scholar] [CrossRef]
- Wei, X.; Li, Y.; Zhang, S.; Gao, M. Prediction of Thyroid Extracapsular Extension with Cervical Lymph Node Metastases (ECE-LN) by CEUS and BRAF Expression in Papillary Thyroid Carcinoma. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2014, 35, 8559–8564. [Google Scholar] [CrossRef]
- Wada, N.; Nakayama, H.; Suganuma, N.; Masudo, Y.; Rino, Y.; Masuda, M.; Imada, T. Prognostic Value of the Sixth Edition AJCC/UICC TNM Classification for Differentiated Thyroid Carcinoma with Extrathyroid Extension. J. Clin. Endocrinol. Metab. 2007, 92, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Youngwirth, L.M.; Adam, M.A.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Extrathyroidal Extension Is Associated with Compromised Survival in Patients with Thyroid Cancer. Thyroid 2017, 27, 626–631. [Google Scholar] [CrossRef]
- Kwak, J.Y.; Kim, E.-K.; Youk, J.H.; Kim, M.J.; Son, E.J.; Choi, S.H.; Oh, K.K. Extrathyroid Extension of Well-Differentiated Papillary Thyroid Microcarcinoma on US. Thyroid 2008, 18, 609–614. [Google Scholar] [CrossRef]
- Liu, L.; Oh, C.; Heo, J.H.; Park, H.S.; Lee, K.; Chang, J.W.; Jung, S.-N.; Koo, B.S. Clinical Significance of Extrathyroidal Extension According to Primary Tumor Size in Papillary Thyroid Carcinoma. Eur. J. Surg. Oncol. 2018, 44, 1754–1759. [Google Scholar] [CrossRef] [PubMed]
- Sipos, J.A. Advances in Ultrasound for the Diagnosis and Management of Thyroid Cancer. Thyroid 2009, 19, 1363–1372. [Google Scholar] [CrossRef] [PubMed]
- Omar, M.; Attia, A.S.; Issa, P.P.; Christensen, B.R.; Sugumar, K.; Alnahla, A.; Hadedeya, D.; Shalaby, H.; Gupta, N.; Shama, M. Diagnostic Accuracy of Ultrasound in Predicting Extrathyroidal Extension and Its Relation to Body Mass Index in a North American Population. Biomedicines 2022, 10, 2408. [Google Scholar] [CrossRef] [PubMed]
- Issa, P.P.; Mueller, L.; Hussein, M.; Albuck, A.; Shama, M.; Toraih, E.; Kandil, E. Radiologist Versus Non-Radiologist Detection of Lymph Node Metastasis in Papillary Thyroid Carcinoma by Ultrasound: A Meta-Analysis. Biomedicines 2022, 10, 2575. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Bidault, S.; Hadoux, J.; Guerlain, J.; Girard, E.; Breuskin, I.; Attard, M.; Suciu, V.; Baudin, E.; Al Ghuzlan, A. Can Preoperative Ultrasound Predict Extrathyroidal Extension of Differentiated Thyroid Cancer? Eur. J. Endocrinol. 2021, 185, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Reiners, C.; Wegscheider, K.; Schicha, H.; Theissen, P.; Vaupel, R.; Wrbitzky, R.; Schumm-Draeger, P.-M. Prevalence of Thyroid Disorders in the Working Population of Germany: Ultrasonography Screening in 96,278 Unselected Employees. Thyroid 2004, 14, 926–932. [Google Scholar] [CrossRef]
- Guth, S.; Theune, U.; Aberle, J.; Galach, A.; Bamberger, C. Very High Prevalence of Thyroid Nodules Detected by High Frequency (13 MHz) Ultrasound Examination. Eur. J. Clin. Investig. 2009, 39, 699–706. [Google Scholar] [CrossRef]
- Hwang, H.S.; Orloff, L.A. Efficacy of Preoperative Neck Ultrasound in the Detection of Cervical Lymph Node Metastasis from Thyroid Cancer. Laryngoscope 2011, 121, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Eun, N.L.; Son, E.J.; Kim, J.-A.; Gweon, H.M.; Kang, J.-H.; Youk, J.H. Comparison of the Diagnostic Performances of Ultrasonography, CT and Fine Needle Aspiration Cytology for the Prediction of Lymph Node Metastasis in Patients with Lymph Node Dissection of Papillary Thyroid Carcinoma: A Retrospective Cohort Study. Int. J. Surg. 2018, 51, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Keutgen, X.M.; Li, H.; Memeh, K.; Busch, J.C.; Williams, J.; Lan, L.; Sarne, D.; Finnerty, B.; Angelos, P.; Fahey, T.J. A Machine-Learning Algorithm for Distinguishing Malignant from Benign Indeterminate Thyroid Nodules Using Ultrasound Radiomic Features. J. Med. Imaging 2022, 9, 034501. [Google Scholar] [CrossRef]
- Jiang, M.; Li, C.; Tang, S.; Lv, W.; Yi, A.; Wang, B.; Yu, S.; Cui, X.; Dietrich, C.F. Nomogram Based on Shear-Wave Elastography Radiomics Can Improve Preoperative Cervical Lymph Node Staging for Papillary Thyroid Carcinoma. Thyroid 2020, 30, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.-R.; Shin, J.; Park, H.; Cho, H.; Hahn, S.; Park, K. Radiomics Study of Thyroid Ultrasound for Predicting BRAF Mutation in Papillary Thyroid Carcinoma: Preliminary Results. Am. J. Neuroradiol. 2020, 41, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Agyekum, E.A.; Ren, Y.; Zhang, J.; Zhang, Q.; Sun, H.; Zhang, G.; Xu, F.; Bo, X.; Lv, W. A Radiomic Nomogram for the Ultrasound-Based Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma. Front. Oncol. 2021, 11, 625646. [Google Scholar] [CrossRef]
- Lee, D.; Ji, Y.; Sung, E.; Park, J.; Lee, Y.; Park, D.; Tae, K. Roles of Ultrasonography and Computed Tomography in the Surgical Management of Cervical Lymph Node Metastases in Papillary Thyroid Carcinoma. Eur. J. Surg. Oncol. EJSO 2013, 39, 191–196. [Google Scholar] [CrossRef]
- Hu, S.; Zhang, H.; Zhong, Y.; Agyekum, E.A.; Sun, Z.; Ge, Y.; Li, J.; Dou, W.; He, J.; Xiang, H. Assessing Diagnostic Value of Combining Ultrasound and MRI in Extrathyroidal Extension of Papillary Thyroid Carcinoma. Cancer Manag. Res. 2022, 14, 1285. [Google Scholar] [CrossRef]
- Attia, A.S.; Hussein, M.; Issa, P.P.; Elnahla, A.; Farhoud, A.; Magazine, B.M.; Youssef, M.R.; Aboueisha, M.; Shama, M.; Toraih, E.; et al. Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies. Int. J. Mol. Sci. 2022, 23, 15626. [Google Scholar] [CrossRef]
- Kebebew, E.; Weng, J.; Bauer, J.; Ranvier, G.; Clark, O.H.; Duh, Q.-Y.; Shibru, D.; Bastian, B.; Griffin, A. The Prevalence and Prognostic Value of BRAF Mutation in Thyroid Cancer. Ann. Surg. 2007, 246, 466. [Google Scholar] [CrossRef]
- Li, C.; Lee, K.C.; Schneider, E.B.; Zeiger, M.A. BRAF V600E Mutation and Its Association with Clinicopathological Features of Papillary Thyroid Cancer: A Meta-Analysis. J. Clin. Endocrinol. Metab. 2012, 97, 4559–4570. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, E.H.; Greider, C.W.; Szostak, J.W. Telomeres and Telomerase: The Path from Maize, Tetrahymena and Yeast to Human Cancer and Aging. Nat. Med. 2006, 12, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, Z.; Chen, T.; Zeng, W.; Guo, Y.; Huang, T. TERT Promoter Mutation and Its Association with Clinicopathological Features and Prognosis of Papillary Thyroid Cancer: A Meta-Analysis. Sci. Rep. 2016, 6, 36990. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Song, Y.S.; Kim, Y.A.; Lim, J.A.; Cho, S.W.; Moon, J.H.; Hahn, S.; Park, D.J.; Park, Y.J. Effects of Coexistent BRAFV600E and TERT Promoter Mutations on Poor Clinical Outcomes in Papillary Thyroid Cancer: A Meta-Analysis. Thyroid 2017, 27, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wang, L.; Jia, X.; Hu, X.; Pang, P.; Zhao, S.; Wang, Y.; Wang, J.; Zhang, Y.; Lyu, Z. The Coexistence of Genetic Mutations in Thyroid Carcinoma Predicts Histopathological Factors Associated with a Poor Prognosis: A Systematic Review and Network Meta-Analysis. Front. Oncol. 2020, 10, 540238. [Google Scholar] [CrossRef]
- Park, J.Y.; Yi, J.W.; Park, C.H.; Lim, Y.; Lee, K.H.; Lee, K.E.; Kim, J.H. Role of BRAF and RAS Mutations in Extrathyroidal Extension in Papillary Thyroid Cancer. Cancer Genom. Proteom. 2016, 13, 171–181. [Google Scholar]
- Rivera, M.; Ricarte-Filho, J.; Tuttle, R.M.; Ganly, I.; Shaha, A.; Knauf, J.; Fagin, J.; Ghossein, R. Molecular, Morphologic, and Outcome Analysis of Thyroid Carcinomas According to Degree of Extrathyroid Extension. Thyroid 2010, 20, 1085–1093. [Google Scholar] [CrossRef]
- Park, Y.M.; Wang, S.-G.; Goh, J.Y.; Shin, D.H.; Kim, I.-J.; Lee, B.-J. Intraoperative Frozen Section for the Evaluation of Extrathyroidal Extension in Papillary Thyroid Cancer. World J. Surg. 2015, 39, 187–193. [Google Scholar] [CrossRef]
- Ji, Y.B.; Lee, D.W.; Song, C.M.; Kim, K.R.; Park, C.W.; Tae, K. Accuracy of Intraoperative Determination of Central Node Metastasis by the Surgeon in Papillary Thyroid Carcinoma. Otolaryngol. Head Neck Surg. 2014, 150, 542–547. [Google Scholar] [CrossRef]
- Scherl, S.; Mehra, S.; Clain, J.; Dos Reis, L.L.; Persky, M.; Turk, A.; Wenig, B.; Husaini, H.; Urken, M.L. The Effect of Surgeon Experience on the Detection of Metastatic Lymph Nodes in the Central Compartment and the Pathologic Features of Clinically Unapparent Metastatic Lymph Nodes: What Are We Missing When We Don’t Perform a Prophylactic Dissection of Central Compartment Lymph Nodes in Papillary Thyroid Cancer? Thyroid 2014, 24, 1282–1288. [Google Scholar]


{kind=link}
| Study | Year | Study Period | Country | Study Design | Patients |
|---|---|---|---|---|---|
| Hu, 2020 [11] | 2020 | 05.2014–12.2018 | China | Retrospective | 225 |
| Ramundo, 2020 [12] | 2020 | 11.2015–05.2019 | Italy | Retrospective | 128 |
| Jiao & Zhang, 2017 [13] | 2017 | 10.2011–07.2014 | China | Retrospective | 166 |
| Yi, 2016 [14] | 2016 | 05.2011–12.2011 | Korea | Prospective | 61 |
| Kamaya, 2015 [15] | 2015 | USA | Retrospective | 129 | |
| Choi, 2014 [16] | 2014 | 12.2012–04.2013 | Korea | Prospective | 625 |
| Gweon, 2014 [17] | 2014 | Korea | Prospective | 79 | |
| Kim, 2014 [17] | 2014 | 01.2011–05.2012 | USA | Retrospective | 75 |
| Lee, 2014 [18] | 2014 | 05.2009–12.2010 | Korea | Retrospective | 568 |
| Lee, 2014 [19] | 2014 | 01.2006–12.2012 | Korea | Retrospective | 252 |
| Wei, 2014 [20] | 2014 | China | Prospective | 317 |
| Estimate [95% CI] | |
|---|---|
| Sensitivity | 76.4% [74.3–78.5%] |
| Specificity | 51.2% [48.6–53.8%] |
| DOR | 5.317 [2.538; 11.139] |
| AUC | 0.6874 ± 0.0841 |
| Sub-Group | Estimate | 95%CI Lower | 95%CI Upper | ||
|---|---|---|---|---|---|
| Year of Publication | Sensitivity | <2015 | 78.9% | 76.5% | 81.2% |
| ≥2015 | 69.7% | 65.2% | 74.0% | ||
| Specificity | <2015 | 53.9% | 50.9% | 56.8% | |
| ≥2015 | 41.6% | 36.2% | 47.2% | ||
| DOR | <2015 | 5.569 | 2.305 | 13.455 | |
| ≥2015 | 5.077 | 1.182 | 21.812 | ||
| Study design | Sensitivity | Retrospective | 89.2% | 86.9% | 91.3% |
| Prospective | 63.9% | 60.5% | 67.2% | ||
| Specificity | Retrospective | 50.8% | 47.3% | 54.2% | |
| Prospective | 51.8% | 47.8% | 55.7% | ||
| DOR | Retrospective | 10.423 | 5.074 | 21.41 | |
| Prospective | 1.917 | 0.735 | 5.004 | ||
| Country | Sensitivity | China | 67.7% | 63.2% | 71.9% |
| Korea | 75.3% | 72.1% | 78.4% | ||
| USA | 87.2% | 83.2% | 90.4% | ||
| Specificity | China | 62.7% | 57.2% | 67.9% | |
| Korea | 41.6% | 37.9% | 45.4% | ||
| USA | 63.1% | 57.8% | 68.2% | ||
| DOR | China | 5.043 | 0.838 | 30.368 | |
| Korea | 2.452 | 0.946 | 6.356 | ||
| USA | 18.695 | 4.207 | 83.078 | ||
| Variable | Coefficient | SE | p-Value | DOR | 95%CI Lower | 95%CI Upper | |
|---|---|---|---|---|---|---|---|
| Study design | Prospective vs. Retrospective | −1.543 | 0.806 | 0.1 | 0.21 | 0.03 | 1.54 |
| Year of Publication | ≥2015 vs. <2015 | −0.505 | 0.782 | 0.54 | 0.6 | 0.09 | 4.1 |
| Country | USA vs. Asia | −0.098 | 0.165 | 0.58 | 0.91 | 0.57 | 1.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issa, P.P.; Albuck, A.L.; Hossam, E.; Hussein, M.; Aboueisha, M.; Attia, A.S.; Omar, M.; Abdelrahman, S.; Naser, G.; Clark, R.D.E.; et al. The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 371. https://doi.org/10.3390/ijms24010371
Issa PP, Albuck AL, Hossam E, Hussein M, Aboueisha M, Attia AS, Omar M, Abdelrahman S, Naser G, Clark RDE, et al. The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(1):371. https://doi.org/10.3390/ijms24010371
Chicago/Turabian StyleIssa, Peter P., Aaron L. Albuck, Eslam Hossam, Mohammad Hussein, Mohamed Aboueisha, Abdallah S. Attia, Mahmoud Omar, Seif Abdelrahman, Gehad Naser, Robert D. E. Clark, and et al. 2023. "The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 24, no. 1: 371. https://doi.org/10.3390/ijms24010371
APA StyleIssa, P. P., Albuck, A. L., Hossam, E., Hussein, M., Aboueisha, M., Attia, A. S., Omar, M., Abdelrahman, S., Naser, G., Clark, R. D. E., Toraih, E., & Kandil, E. (2023). The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 24(1), 371. https://doi.org/10.3390/ijms24010371