
Annoying Psoriasis and Atopic Dermatitis: A Narrative Review

Abstract
:1. Morbidity and Clinical Classification
1.1. Morbidity and Clinical Classification of Psoriasis
1.2. Morbidity and Clinical Classification of Atopic Dermatitis
1.2.1. Morbidity of Atopic Dermatitis
1.2.2. Clinical Classification of Atopic Dermatitis
- A.
- Lichenoid atopic dermatitisIn general, the clinical manifestations of Lichenoid atopic dermatitis include thickening, raised and uneven skin, because of continuous itch and long-term friction, it will show a leather-like appearance [21].
- B.
- Juvenile plantar dermatosisJuvenile plantar dermatosis mainly occurs on the soles of children and adolescents. Different from athlete’s foot caused by a fungal infection, the typical expressions are extremely itchy, shiny appearance, and erythema on the surface of the first toe and sole [22]. Wearing plastic shoes easily exacerbates disease
- C.
- Nummular-type atopic dermatitisNummular-type atopic dermatitis is a chronic disease. Clinically, multiple coin-shaped lesions can be seen on the skin [22], these lesions are itchy and well-defined. This kind of dermatitis often occurs after skin injuries, such as burns, and contusions, most of which can be successfully treated with steroids.
- D.
- Follicular atopic dermatitisThe clinical presentations of follicular atopic dermatitis are mostly single papules, and the lesions often involve the hair follicles and surrounding dermis [20]. In children, the lesions often include the entire chest, back, abdomen, and proximal limbs. Doctors usually recommend topical steroids for 2 to 4 weeks [22].
- E.
- Eczema coxsackiumEczema coxsackium is a specific term for Coxsackie virus infection. This type of dermatitis is caused by Coxsackie infection in children with AD [22].Pustules and oral ulcers occur in the anterior elbow and popliteal fossa [23]. Therefore, it is recommended to supplement the lost water and electrolytes in clinical practice, and treat the symptoms of the patient.
- F.
- Psoriasiform atopic dermatitisPsoriasis and atopic dermatitis are the two different diagnoses, and psoriasiform atopic dermatitis, as the name suggests, is atopic dermatitis with a tissue type similar to psoriasis, which simultaneously manifests the characteristics of two diseases, such as itching and desquamation [24]. The use of traditional steroids was found to be ineffective and phototherapy was necessary to improve lesions [22].
2. Molecular Mechanisms
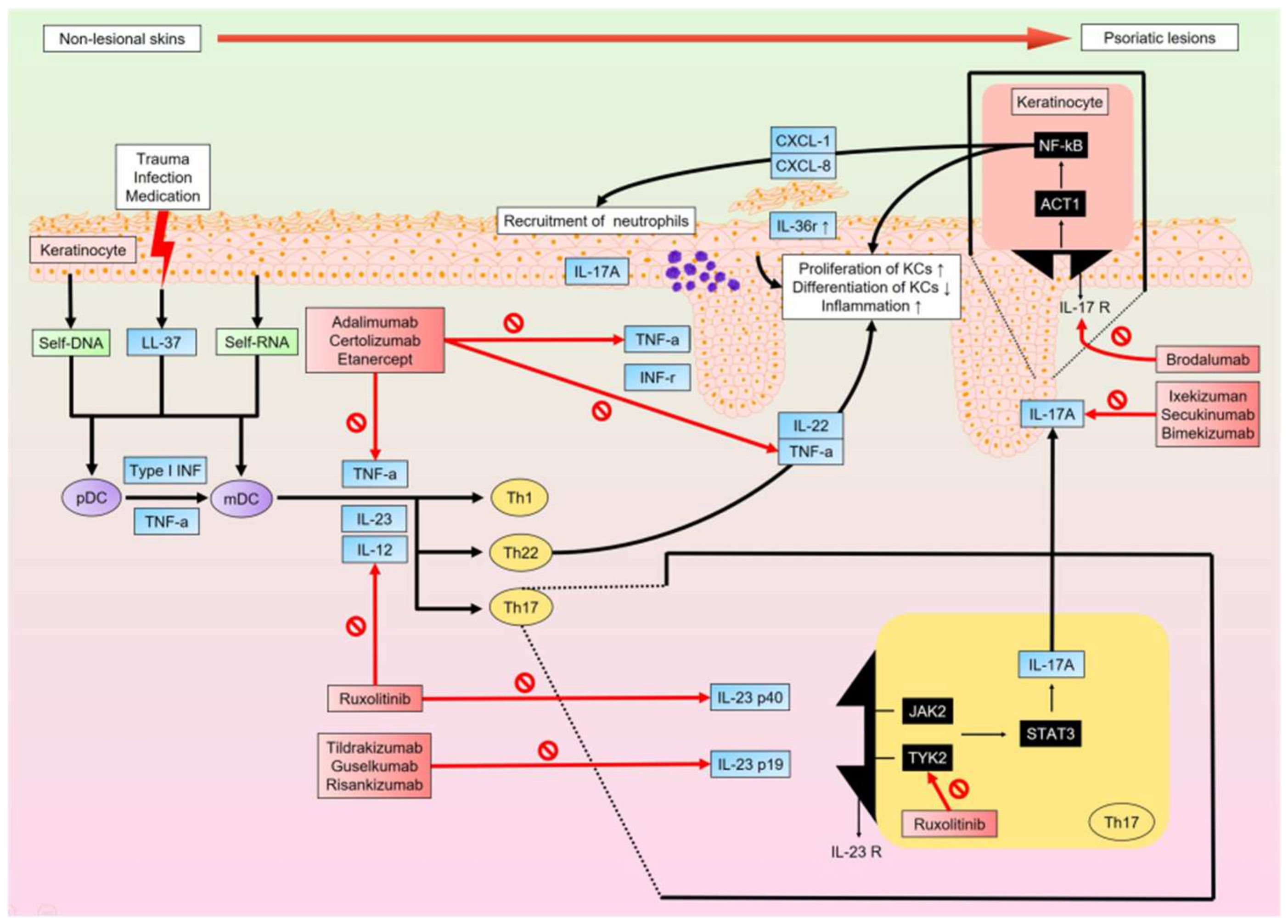
2.1. Pathological Molecular Mechanisms of Psoriasis
2.2. Pathological Molecular Mechanisms of Atopic Dermatitis
3. Management
3.1. Treatment Options for Psoriasis
3.1.1. Interleukin 23-Targeted Therapies
3.1.2. Interleukin 17-Targeted Therapies
3.1.3. Tumor Necrosis Factor-Targeted Therapies
3.2. Treatment Options for Atopic Dermatitis
3.2.1. Topical Medication
3.2.2. Systemic Therapeutics
3.2.3. Emerging Therapies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACT1 | actin-1 |
| ACH | acrodermatitis continua of Hallopeau |
| AD | atopic dermatitis |
| Alpha-NAC | alpha chain of the nascent polypeptide-associated complex |
| AMPs | antimicrobial peptides |
| cAMP | cyclic adenosine monophosphate |
| CARD | caspase recruitment domain |
| CCL17/TARC | C-C motif chemokine ligand 17/thymus- and activation-regulated chemokine |
| CXCL | chemokine (C-X-C motif) ligand |
| E | eosinphil |
| EL | excimer laser |
| FLG | fliaggrin |
| FKBP | FK506 binding protein |
| FSL | full-spectrum light |
| GM-CSF | granulocyte/monocyte colony-stimulating factor |
| HIV | human immunodeficiency virus |
| HLA-Cw6 | human leukocyte antigen-Cw6 |
| IFN | interferon |
| Ig | immunoglobulin |
| IL | interleukin |
| ISAAC | International Study of Asthma and Allergies in Childhood |
| JAK2/TYK2 | Janus kinase 2/Tyrosine kinase 2 |
| KCs | keratinocytes |
| KLK | Kallikrein-like peptidase |
| LC | Langerhan cell |
| lncRNA | long noncoding RNA |
| M | mast cell |
| mDC | myeloid dendritic cell |
| MHC | major histocompatibility complex |
| miRNA | microRNA |
| NB UVA/UVB | narrow band UVA/UVB |
| NF-κB | nuclear factor-kappa-light-chain-enhancer of activated B cells |
| PASI | psoriasis area severity index |
| PAR2 | protease-activated receptor 2 |
| pDC | plasmacytoid dendritic cell |
| PDE4 | Phosphodiesterase-4 |
| PPP | palmoplantar pustulosis |
| PRINS | psoriasis associated RNA induced by stress |
| PSORS1 | psoriasis susceptibility gene 1 |
| PUVA | psoralen and ultraviolet A |
| PWAR6 | Prader Willi/Angelman region RNA 6 |
| RCT | randomized controlled trial |
| S. aureus | Staphylococcus aureus |
| SCORAD | scoring atopic dermatitis |
| SPINK5 | Serine protease inhibitor Kazal type 5 |
| STAT | signal transducers and activators of transcription |
| S100A8/A9 | S100 calcium-binding protein A8/A9 |
| TCIs | topical calcineurin inhibitors |
| TCSs | topical corticosteroids |
| TEWL | trans epidermal water loss |
| Th | T helper |
| TNF-α | tumor necrosis factor-α |
| TSLP | thymic stromal lymphopoietin |
| UVR | ultraviolet radiation |
References
- Kapila, S.; Hong, E.; Fischer, G. A comparative study of childhood psoriasis and atopic dermatitis and greater understanding of the overlapping condition, psoriasis-dermatitis. Australas. J. Dermatol. 2012, 53, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Krueger, J.G.; Lebwohl, M.G. Systemic immune mechanisms in atopic dermatitis and psoriasis with implications for treatment. Exp. Dermatol. 2018, 27, 409–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufman, B.P.; Alexis, A.F. Psoriasis in Skin of Color: Insights into the Epidemiology, Clinical Presentation, Genetics, Quality-of-Life Impact, and Treatment of Psoriasis in Non-White Racial/Ethnic Groups. Am. J. Clin. Dermatol. 2018, 19, 405–423. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Schon, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Helmick, C.G.; Lee-Han, H.; Hirsch, S.C.; Baird, T.L.; Bartlett, C.L. Prevalence of psoriasis among adults in the U.S.: 2003-2006 and 2009-2010 National Health and Nutrition Examination Surveys. Am. J. Prev. Med. 2014, 47, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Merola, J.F.; Li, T.; Li, W.Q.; Cho, E.; Qureshi, A.A. Prevalence of psoriasis phenotypes among men and women in the USA. Clin. Exp. Dermatol. 2016, 41, 486–489. [Google Scholar] [CrossRef]
- Romiti, R.; Amone, M.; Menter, A.; Miot, H.A. Prevalence of psoriasis in Brazil—A geographical survey. Int. J. Dermatol. 2017, 56, e167–e168. [Google Scholar] [CrossRef]
- Springate, D.A.; Parisi, R.; Kontopantelis, E.; Reeves, D.; Griffiths, C.E.; Ashcroft, D.M. Incidence, prevalence and mortality of patients with psoriasis: A U.K. population-based cohort study. Br. J. Dermatol. 2017, 176, 650–658. [Google Scholar] [CrossRef]
- Prignano, F.; Rogai, V.; Cavallucci, E.; Bitossi, A.; Hammen, V.; Cantini, F. Epidemiology of Psoriasis and Psoriatic Arthritis in Italy-a Systematic Review. Curr. Rheumatol. Rep. 2018, 20, 43. [Google Scholar] [CrossRef]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Alexander, H.; Nestle, F.O. Pathogenesis and immunotherapy in cutaneous psoriasis: What can rheumatologists learn? Curr. Opin. Rheumatol. 2017, 29, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Sarac, G.; Koca, T.T.; Baglan, T. A brief summary of clinical types of psoriasis. N. Clin. Istanb. 2016, 3, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Haider, S.; Colicino, S.; Murray, C.S.; Holloway, J.; Simpson, A.; Cullinan, P.; Custovic, A.; Investigators, S. Different definitions of atopic dermatitis: Impact on prevalence estimates and associated risk factors. Br. J. Dermatol. 2019, 181, 1272–1279. [Google Scholar] [CrossRef] [PubMed]
- Flohr, C. Recent perspectives on the global epidemiology of childhood eczema. Allergol. Immunopathol. 2011, 39, 174–182. [Google Scholar] [CrossRef]
- Nutten, S. Atopic dermatitis: Global epidemiology and risk factors. Ann. Nutr. Metab. 2015, 66 (Suppl. S1), 8–16. [Google Scholar] [CrossRef]
- Odhiambo, J.A.; Williams, H.C.; Clayton, T.O.; Robertson, C.F.; Asher, M.I.; Group, I.P.T.S. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J. Allergy Clin. Immunol. 2009, 124, 1251–1258 e1223. [Google Scholar] [CrossRef]
- Shaw, T.E.; Currie, G.P.; Koudelka, C.W.; Simpson, E.L. Eczema prevalence in the United States: Data from the 2003 National Survey of Children’s Health. J. Investig. Dermatol. 2011, 131, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Li, P.; Tang, J.; Han, X.; Zou, X.; Xu, G.; Xu, Z.; Wei, F.; Liu, Q.; Wang, M.; et al. Prevalence of Atopic Dermatitis in Chinese Children aged 1–7 ys. Sci. Rep. 2016, 6, 29751. [Google Scholar] [CrossRef]
- Abuabara, K.; Yu, A.M.; Okhovat, J.P.; Allen, I.E.; Langan, S.M. The prevalence of atopic dermatitis beyond childhood: A systematic review and meta-analysis of longitudinal studies. Allergy 2018, 73, 696–704. [Google Scholar] [CrossRef]
- Silverberg, N.B. Typical and atypical clinical appearance of atopic dermatitis. Clin. Dermatol. 2017, 35, 354–359. [Google Scholar] [CrossRef]
- Allen, H.B.; Jones, N.P.; Bowen, S.E. Lichenoid and other clinical presentations of atopic dermatitis in an inner city practice. J. Am. Acad. Dermatol. 2008, 58, 503–504. [Google Scholar] [CrossRef] [PubMed]
- Wallach, D.; Taieb, A. Atopic dermatitis/atopic eczema. Chem. Immunol. Allergy 2014, 100, 81–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horsten, H.H.; Fisker, N.; Bygum, A. Eczema Coxsackium Caused by Coxsackievirus A6. Pediatr. Dermatol. 2016, 33, e230–e231. [Google Scholar] [CrossRef] [PubMed]
- Tirumalae, R. Psoriasiform dermatoses: Microscopic approach. Indian J. Dermatol. 2013, 58, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Mahil, S.K.; Capon, F.; Barker, J.N. Update on psoriasis immunopathogenesis and targeted immunotherapy. Semin. Immunopathol. 2016, 38, 11–27. [Google Scholar] [CrossRef] [Green Version]
- Rendon, A.; Schakel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [Green Version]
- von Csiky-Sessoms, S.; Lebwohl, M. What’s New in Psoriasis. Dermatol. Clin. 2019, 37, 129–136. [Google Scholar] [CrossRef]
- Morizane, S.; Gallo, R.L. Antimicrobial peptides in the pathogenesis of psoriasis. J. Dermatol. 2012, 39, 225–230. [Google Scholar] [CrossRef]
- Prinz, I.; Sandrock, I.; Mrowietz, U. Interleukin-17 cytokines: Effectors and targets in psoriasis-A breakthrough in understanding and treatment. J. Exp. Med. 2020, 217, e20191397. [Google Scholar] [CrossRef]
- Girolomoni, G.; Strohal, R.; Puig, L.; Bachelez, H.; Barker, J.; Boehncke, W.H.; Prinz, J.C. The role of IL-23 and the IL-23/TH 17 immune axis in the pathogenesis and treatment of psoriasis. J. Eur. Acad Dermatol. Venereol. 2017, 31, 1616–1626. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Du, J.; Han, Y.; Wei, Z. Correlation analysis between IL-35, IL-36gamma, CCL27 and psoriasis vulgaris. J. Dermatol.og Treat 2019, 32, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Kadono, T. Psoriasis: Behind the scenes. J. Dermatol. 2016, 43, 4–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furue, K.; Yamamura, K.; Tsuji, G.; Mitoma, C.; Uchi, H.; Nakahara, T.; Kido-Nakahara, M.; Kadono, T.; Furue, M. Highlighting Interleukin-36 Signalling in Plaque Psoriasis and Pustular Psoriasis. Acta Derm. Venereol. 2018, 98, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, M.; Huang, Y.; Zhu, X.; Lin, X.; Luo, D. miR125bmediated regulation of cell proliferation through the Jagged1/Notch signaling pathway by inhibiting BRD4 expression in psoriasis. Mol. Med. Rep. 2019, 19, 5227–5236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Xue, H.; Gao, T.; Gao, M.; Zhang, Y. Notch1 Signaling Regulates the Th17/Treg Immune Imbalance in Patients with Psoriasis Vulgaris. Mediat. Inflamm. 2018, 2018, 3069521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, D.J.; Chan, W.H.; Hinojosa, T.; Hsu, S.; Feldman, S.R. Mechanisms of microbial pathogenesis and the role of the skin microbiome in psoriasis: A review. Clin. Dermatol. 2019, 37, 160–166. [Google Scholar] [CrossRef]
- Thio, H.B. The Microbiome in Psoriasis and Psoriatic Arthritis: The Skin Perspective. J. Rheumatol. Suppl. 2018, 94, 30–31. [Google Scholar] [CrossRef]
- Chang, H.W.; Yan, D.; Singh, R.; Liu, J.; Lu, X.; Ucmak, D.; Lee, K.; Afifi, L.; Fadrosh, D.; Leech, J.; et al. Alteration of the cutaneous microbiome in psoriasis and potential role in Th17 polarization. Microbiome 2018, 6, 154. [Google Scholar] [CrossRef]
- Peng, W.; Novak, N. Pathogenesis of atopic dermatitis. Clin. Exp. Allergy 2015, 45, 566–574. [Google Scholar] [CrossRef]
- Cabanillas, B.; Novak, N. Atopic dermatitis and filaggrin. Curr. Opin. Immunol. 2016, 42, 1–8. [Google Scholar] [CrossRef]
- Dezman, K.; Korosec, P.; Rupnik, H.; Rijavec, M. SPINK5 is associated with early-onset and CHI3L1 with late-onset atopic dermatitis. Int. J. Immunogenet. 2017, 44, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Gittler, J.K.; Shemer, A.; Suarez-Farinas, M.; Fuentes-Duculan, J.; Gulewicz, K.J.; Wang, C.Q.; Mitsui, H.; Cardinale, I.; de Guzman Strong, C.; Krueger, J.G.; et al. Progressive activation of T(H)2/T(H)22 cytokines and selective epidermal proteins characterizes acute and chronic atopic dermatitis. J. Allergy Clin. Immunol. 2012, 130, 1344–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martel, B.C.; Litman, T.; Hald, A.; Norsgaard, H.; Lovato, P.; Dyring-Andersen, B.; Skov, L.; Thestrup-Pedersen, K.; Skov, S.; Skak, K.; et al. Distinct molecular signatures of mild extrinsic and intrinsic atopic dermatitis. Exp. Dermatol. 2016, 25, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Aeberhard, C.; Erdemoglu, Y.; Simon, H.U. Th17 cells and tissue remodeling in atopic and contact dermatitis. Allergy 2014, 69, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, S.; Park, C.O.; Shin, J.U.; Noh, J.Y.; Lee, Y.S.; Lee, N.R.; Kim, H.R.; Noh, S.; Lee, Y.; Lee, J.H.; et al. DAMP molecules S100A9 and S100A8 activated by IL-17A and house-dust mites are increased in atopic dermatitis. Exp. Dermatol. 2014, 23, 938–941. [Google Scholar] [CrossRef] [PubMed]
- Cevikbas, F.; Wang, X.; Akiyama, T.; Kempkes, C.; Savinko, T.; Antal, A.; Kukova, G.; Buhl, T.; Ikoma, A.; Buddenkotte, J.; et al. A sensory neuron-expressed IL-31 receptor mediates T helper cell-dependent itch: Involvement of TRPV1 and TRPA1. J. Allergy Clin. Immunol. 2014, 133, 448–460. [Google Scholar] [CrossRef] [Green Version]
- van de Kerkhof, P.C. An update on topical therapies for mild-moderate psoriasis. Dermatol. Clin. 2015, 33, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wu, M.X. A clinical review of phototherapy for psoriasis. Lasers Med. Sci. 2018, 33, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Golbari, N.M.; Porter, M.L.; Kimball, A.B. Current guidelines for psoriasis treatment: A work in progress. Cutis 2018, 101, 10–12. [Google Scholar]
- Sinclair, R.; Thirthar Palanivelu, V. Tildrakizumab for the treatment of psoriasis. Expert. Rev. Clin. Immunol. 2019, 15, 5–12. [Google Scholar] [CrossRef]
- Reich, K.; Papp, K.A.; Blauvelt, A.; Tyring, S.K.; Sinclair, R.; Thaci, D.; Nograles, K.; Mehta, A.; Cichanowitz, N.; Li, Q.; et al. Tildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): Results from two randomised controlled, phase 3 trials. Lancet 2017, 390, 276–288. [Google Scholar] [CrossRef]
- Nakamura, M.; Lee, K.; Jeon, C.; Sekhon, S.; Afifi, L.; Yan, D.; Lee, K.; Bhutani, T. Guselkumab for the Treatment of Psoriasis: A Review of Phase III Trials. Dermatol. Ther. 2017, 7, 281–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langley, R.G.; Lebwohl, M.; Krueger, G.G.; Szapary, P.O.; Wasfi, Y.; Chan, D.; Hsu, M.C.; You, Y.; Poulin, Y.; Korman, N.; et al. Long-term efficacy and safety of ustekinumab, with and without dosing adjustment, in patients with moderate-to-severe psoriasis: Results from the PHOENIX 2 study through 5 years of follow-up. Br. J. Dermatol. 2015, 172, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Rouse, N.C.; Farhangian, M.E.; Wehausen, B.; Feldman, S.R. The cost-effectiveness of ustekinumab for moderate-to-severe psoriasis. Expert Rev. Pharmacoecon. Outcomes Res. 2015, 15, 877–884. [Google Scholar] [CrossRef]
- Gordon, K.B.; Strober, B.; Lebwohl, M.; Augustin, M.; Blauvelt, A.; Poulin, Y.; Papp, K.A.; Sofen, H.; Puig, L.; Foley, P.; et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): Results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet 2018, 392, 650–661. [Google Scholar] [CrossRef]
- Bauer, E.; Lucier, J.; Furst, D.E. Brodalumab-an IL-17RA monoclonal antibody for psoriasis and psoriatic arthritis. Expert Opin. Biol. Ther. 2015, 15, 883–893. [Google Scholar] [CrossRef]
- Griffiths, C.E.; Reich, K.; Lebwohl, M.; van de Kerkhof, P.; Paul, C.; Menter, A.; Cameron, G.S.; Erickson, J.; Zhang, L.; Secrest, R.J.; et al. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): Results from two phase 3 randomised trials. Lancet 2015, 386, 541–551. [Google Scholar] [CrossRef]
- Morita, K.; Tokushige, C.; Maeda, S.; Kiyose, H.; Noura, M.; Iwai, A.; Yamada, M.; Kashiwazaki, G.; Taniguchi, J.; Bando, T.; et al. RUNX transcription factors potentially control E-selectin expression in the bone marrow vascular niche in mice. Blood Adv. 2018, 2, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Natsis, N.E.; Gottlieb, A.B. Bimekizumab for the treatment of psoriatic disease. Expert Opin. Biol. Ther. 2018, 18, 1193–1197. [Google Scholar] [CrossRef]
- Glatt, S.; Helmer, E.; Haier, B.; Strimenopoulou, F.; Price, G.; Vajjah, P.; Harari, O.A.; Lambert, J.; Shaw, S. First-in-human randomized study of bimekizumab, a humanized monoclonal antibody and selective dual inhibitor of IL-17A and IL-17F, in mild psoriasis. Br. J. Clin. Pharmacol. 2017, 83, 991–1001. [Google Scholar] [CrossRef]
- Burness, C.B.; McKeage, K. Adalimumab: A Review in Chronic Plaque Psoriasis. Drugs 2015, 75, 2119–2130. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, A.B.; Blauvelt, A.; Thaci, D.; Leonardi, C.L.; Poulin, Y.; Drew, J.; Peterson, L.; Arendt, C.; Burge, D.; Reich, K. Certolizumab pegol for the treatment of chronic plaque psoriasis: Results through 48 weeks from 2 phase 3, multicenter, randomized, double-blinded, placebo-controlled studies (CIMPASI-1 and CIMPASI-2). J. Am. Acad Dermatol. 2018, 79, 302–314 e306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papp, K.A.; Poulin, Y.; Bissonnette, R.; Bourcier, M.; Toth, D.; Rosoph, L.; Poulin-Costello, M.; Setterfield, M.; Syrotuik, J. Assessment of the long-term safety and effectiveness of etanercept for the treatment of psoriasis in an adult population. J. Am. Acad Dermatol. 2012, 66, e33–e45. [Google Scholar] [CrossRef] [PubMed]
- Ara, M.; Gracia, T.; Pastushenko, E. Etanercept combined with systemic drugs or phototherapy for treatment of psoriasis. Actas. Dermosifiliogr. 2015, 106, 180–188. [Google Scholar] [CrossRef]
- Bai, F.; Li, G.G.; Liu, Q.; Niu, X.; Li, R.; Ma, H. Short-Term Efficacy and Safety of IL-17, IL-12/23, and IL-23 Inhibitors Brodalumab, Secukinumab, Ixekizumab, Ustekinumab, Guselkumab, Tildrakizumab, and Risankizumab for the Treatment of Moderate to Severe Plaque Psoriasis: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. J. Immunol. Res. 2019, 2019, 2546161. [Google Scholar] [CrossRef] [Green Version]
- Sbidian, E.; Chaimani, A.; Garcia-Doval, I.; Do, G.; Hua, C.; Mazaud, C.; Droitcourt, C.; Hughes, C.; Ingram, J.R.; Naldi, L.; et al. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 12, CD011535. [Google Scholar] [CrossRef]
- Imaizumi, A.; Kawakami, T.; Murakami, F.; Soma, Y.; Mizoguchi, M. Effective treatment of pruritus in atopic dermatitis using H1 antihistamines (second-generation antihistamines): Changes in blood histamine and tryptase levels. J. Dermatol. Sci. 2003, 33, 23–29. [Google Scholar] [CrossRef]
- Sidbury, R.; Kodama, S. Atopic dermatitis guidelines: Diagnosis, systemic therapy, and adjunctive care. Clin. Dermatol. 2018, 36, 648–652. [Google Scholar] [CrossRef]
- Hamilton, J.D.; Suarez-Farinas, M.; Dhingra, N.; Cardinale, I.; Li, X.; Kostic, A.; Ming, J.E.; Radin, A.R.; Krueger, J.G.; Graham, N.; et al. Dupilumab improves the molecular signature in skin of patients with moderate-to-severe atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 1293–1300. [Google Scholar] [CrossRef] [Green Version]
- Wollenberg, A.; Howell, M.D.; Guttman-Yassky, E.; Silverberg, J.I.; Kell, C.; Ranade, K.; Moate, R.; van der Merwe, R. Treatment of atopic dermatitis with tralokinumab, an anti-IL-13 mAb. J. Allergy Clin. Immunol. 2019, 143, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Kabashima, K.; Furue, M.; Hanifin, J.M.; Pulka, G.; Wollenberg, A.; Galus, R.; Etoh, T.; Mihara, R.; Nakano, M.; Ruzicka, T. Nemolizumab in patients with moderate-to-severe atopic dermatitis: Randomized, phase II, long-term extension study. J. Allergy Clin. Immunol. 2018, 142, 1121–1130.e7. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Brunner, P.M.; Neumann, A.U.; Khattri, S.; Pavel, A.B.; Malik, K.; Singer, G.K.; Baum, D.; Gilleaudeau, P.; Sullivan-Whalen, M.; et al. Efficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by conventional treatments: A randomized, double-blind, phase 2a trial. J. Am. Acad Dermatol. 2018, 78, 872–881.e876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, M.; Marasca, C.; Fabbrocini, G.; Patruno, C. Adult atopic dermatitis: New and emerging therapies. Expert Rev. Clin. Pharmacol. 2018, 11, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Papp, K.A.; Poulin, Y.; Gooderham, M.; Raman, M.; Mallbris, L.; Wang, C.; Purohit, V.; Mamolo, C.; Papacharalambous, J.; et al. Topical tofacitinib for atopic dermatitis: A phase IIa randomized trial. Br. J. Dermatol. 2016, 175, 902–911. [Google Scholar] [CrossRef]
- Mayba, J.N.; Gooderham, M.J. Review of Atopic Dermatitis and Topical Therapies. J. Cutan. Med. Surg. 2017, 21, 227–236. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Tom, W.L.; Berger, T.G.; Krol, A.; Paller, A.S.; Schwarzenberger, K.; Bergman, J.N.; Chamlin, S.L.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of care for the management of atopic dermatitis: Section 2. Management and treatment of atopic dermatitis with topical therapies. J. Am. Acad Dermatol. 2014, 71, 116–132. [Google Scholar] [CrossRef] [Green Version]
- Gutfreund, K.; Bienias, W.; Szewczyk, A.; Kaszuba, A. Topical calcineurin inhibitors in dermatology. Part I: Properties, method and effectiveness of drug use. Postepy Dermatol. Alergol. 2013, 30, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Abedz, N.; Pawliczak, R. Efficacy and safety of topical calcineurin inhibitors for the treatment of atopic dermatitis: Meta-analysis of randomized clinical trials. Postepy Dermatol. Alergol. 2019, 36, 752–759. [Google Scholar] [CrossRef]
- Yang, E.J.; Sekhon, S.; Sanchez, I.M.; Beck, K.M.; Bhutani, T. Recent Developments in Atopic Dermatitis. Pediatrics 2018, 142, e20181102. [Google Scholar] [CrossRef] [Green Version]
- Kawashima, M.; Tango, T.; Noguchi, T.; Inagi, M.; Nakagawa, H.; Harada, S. Addition of fexofenadine to a topical corticosteroid reduces the pruritus associated with atopic dermatitis in a 1-week randomized, multicentre, double-blind, placebo-controlled, parallel-group study. Br. J. Dermatol. 2003, 148, 1212–1221. [Google Scholar] [CrossRef]
- Ortiz-Salvador, J.M.; Perez-Ferriols, A. Phototherapy in Atopic Dermatitis. Adv. Exp. Med. Biol. 2017, 996, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Choi, J.Y.; Shin, J.W.; Huh, C.H.; Park, K.C.; Du, M.H.; Yoon, S.; Na, J.I. Changes in Lesional and Non-lesional Skin Microbiome During Treatment of Atopic Dermatitis. Acta Derm. Venereol. 2019, 99, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vakeva, L.; Niemela, S.; Lauha, M.; Pasternack, R.; Hannuksela-Svahn, A.; Hjerppe, A.; Joensuu, A.; Soronen, M.; Ylianttila, L.; Pastila, R.; et al. Narrowband ultraviolet B phototherapy improves quality of life of psoriasis and atopic dermatitis patients up to 3 months: Results from an observational multicenter study. Photodermatol. Photoimmunol. Photomed. 2019, 35, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ferriols, A.; Aranegui, B.; Pujol-Montcusi, J.A.; Martin-Gorgojo, A.; Campos-Dominguez, M.; Feltes, R.A.; Gilaberte, Y.; Echeverria-Garcia, B.; Alvarez-Perez, A.; Garcia-Doval, I. Phototherapy in atopic dermatitis: A systematic review of the literature. Actas Dermosifiliogr. 2015, 106, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Patrizi, A.; Raone, B.; Ravaioli, G.M. Management of atopic dermatitis: Safety and efficacy of phototherapy. Clin. Cosmet. Investig. Dermatol. 2015, 8, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Simpson, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.P.; et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. N. Engl. J. Med. 2016, 375, 2335–2348. [Google Scholar] [CrossRef]
- Blauvelt, A.; de Bruin-Weller, M.; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.; Rubel, D.; et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): A 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 2017, 389, 2287–2303. [Google Scholar] [CrossRef]
- Simpson, E.L.; Flohr, C.; Eichenfield, L.F.; Bieber, T.; Sofen, H.; Taieb, A.; Owen, R.; Putnam, W.; Castro, M.; DeBusk, K.; et al. Efficacy and safety of lebrikizumab (an anti-IL-13 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by topical corticosteroids: A randomized, placebo-controlled phase II trial (TREBLE). J. Am. Acad Dermatol. 2018, 78, 863–871.e11. [Google Scholar] [CrossRef] [Green Version]
- Saleem, M.D.; Oussedik, E.; D’Amber, V.; Feldman, S.R. Interleukin-31 pathway and its role in atopic dermatitis: A systematic review. J. Dermatolog. Treat. 2017, 28, 591–599. [Google Scholar] [CrossRef]
- Mihara, R.; Kabashima, K.; Furue, M.; Nakano, M.; Ruzicka, T. Nemolizumab in moderate to severe atopic dermatitis: An exploratory analysis of work productivity and activity impairment in a randomized phase II study. J. Dermatol. 2019, 46, 662–671. [Google Scholar] [CrossRef]
- Werfel, T.; Allam, J.P.; Biedermann, T.; Eyerich, K.; Gilles, S.; Guttman-Yassky, E.; Hoetzenecker, W.; Knol, E.; Simon, H.U.; Wollenberg, A.; et al. Cellular and molecular immunologic mechanisms in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2016, 138, 336–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Im, D.D.; Ross, P.A.; Hotz, J.; Newth, C.J.L. Evaluating the Practice of Repositioning Endotracheal Tubes in Neonates and Children Based on Radiographic Location. Pediatr. Crit. Care Med. 2019, 20, 1057–1060. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Tom, W.L.; Lebwohl, M.G.; Blumenthal, R.L.; Boguniewicz, M.; Call, R.S.; Eichenfield, L.F.; Forsha, D.W.; Rees, W.C.; Simpson, E.L.; et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults. J. Am. Acad Dermatol. 2016, 75, 494–503.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichenfield, L.F.; Call, R.S.; Forsha, D.W.; Fowler, J., Jr.; Hebert, A.A.; Spellman, M.; Stein Gold, L.F.; Van Syoc, M.; Zane, L.T.; Tschen, E. Long-term safety of crisaborole ointment 2% in children and adults with mild to moderate atopic dermatitis. J. Am. Acad Dermatol. 2017, 77, 641–649.e5. [Google Scholar] [CrossRef] [Green Version]
- He, H.; Guttman-Yassky, E. JAK Inhibitors for Atopic Dermatitis: An Update. Am. J. Clin. Dermatol. 2019, 20, 181–192. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Disease and Treatment | Target or Gene | Reference |
|---|---|---|
| Psoriasis | ||
| Interleukin 23-targeted therapies | ||
| Tildrakizumab | IL23 p19 | [51] |
| Guselkumab | IL23 p19 | [52] |
| Ustekinumab | p40 | [54] |
| Risankizumab | IL23 p19 | [55] |
| Interleukin 17-targeted therapies | ||
| Brodalumab | IL17 | [56] |
| Xekizumab | IL17A | [57] |
| Secukinumab | IL17A | [58] |
| Bimekizumab | IL17A, IL17F | [59] |
| Tumor necrosis factor-targeted therapies | ||
| Adalimumab | p55, p75 | [61] |
| Certolizumab | TNF-α | [62] |
| Etanercept | TNF-α | [64] |
| Atopic dermatitis | ||
| Anti-histamine | [67] | |
| Immunosuppressive drug | ||
| Cyclosporine | ||
| Methotrexate | ||
| Azathioprine | ||
| Mcophenylate mofetil | [68] | |
| Emerging therapies | ||
| Dupilumab | IL4, IL13. | [69] |
| Tralokinumab, Lebrikizumab | IL13 | [70] |
| Nemolizumab | IL31 | [71] |
| Fezakinumab | IL22 | [72] |
| Secukinumab | IL17A | [73] |
| Baricitinib | JAK1, JAK2 | [74] |
| Upadacitinib | JAK | [74] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.-Y.; Chen, S.-C.; Hsu, S.-Y.; Lin, Y.-A.; Shih, C.-M.; Huang, C.-Y.; Wang, K.-H.; Lee, A.-W. Annoying Psoriasis and Atopic Dermatitis: A Narrative Review. Int. J. Mol. Sci. 2022, 23, 4898. https://doi.org/10.3390/ijms23094898
Chen W-Y, Chen S-C, Hsu S-Y, Lin Y-A, Shih C-M, Huang C-Y, Wang K-H, Lee A-W. Annoying Psoriasis and Atopic Dermatitis: A Narrative Review. International Journal of Molecular Sciences. 2022; 23(9):4898. https://doi.org/10.3390/ijms23094898
Chicago/Turabian StyleChen, Wei-Yu, Shao-Chuan Chen, Shou-Yi Hsu, Yu-An Lin, Chun-Ming Shih, Chun-Yao Huang, Kuo-Hsien Wang, and Ai-Wei Lee. 2022. "Annoying Psoriasis and Atopic Dermatitis: A Narrative Review" International Journal of Molecular Sciences 23, no. 9: 4898. https://doi.org/10.3390/ijms23094898
APA StyleChen, W.-Y., Chen, S.-C., Hsu, S.-Y., Lin, Y.-A., Shih, C.-M., Huang, C.-Y., Wang, K.-H., & Lee, A.-W. (2022). Annoying Psoriasis and Atopic Dermatitis: A Narrative Review. International Journal of Molecular Sciences, 23(9), 4898. https://doi.org/10.3390/ijms23094898