
Nanomedicine-Based Delivery Strategies for Breast Cancer Treatment and Management

 ,
,  , , ,
, , ,  , ,
, ,
Abstract

1. Introduction
2. Nanomedicine: Evolving Demands for Breast Cancer Treatment
2.1. Liposomes
2.2. Dendrimers
2.3. Micelles
2.4. Carbon Nanotubes
2.5. Polymeric Nanoparticles
2.6. Solid Lipid Nanoparticles
2.7. Nanostructured Lipid Carriers (NLC)
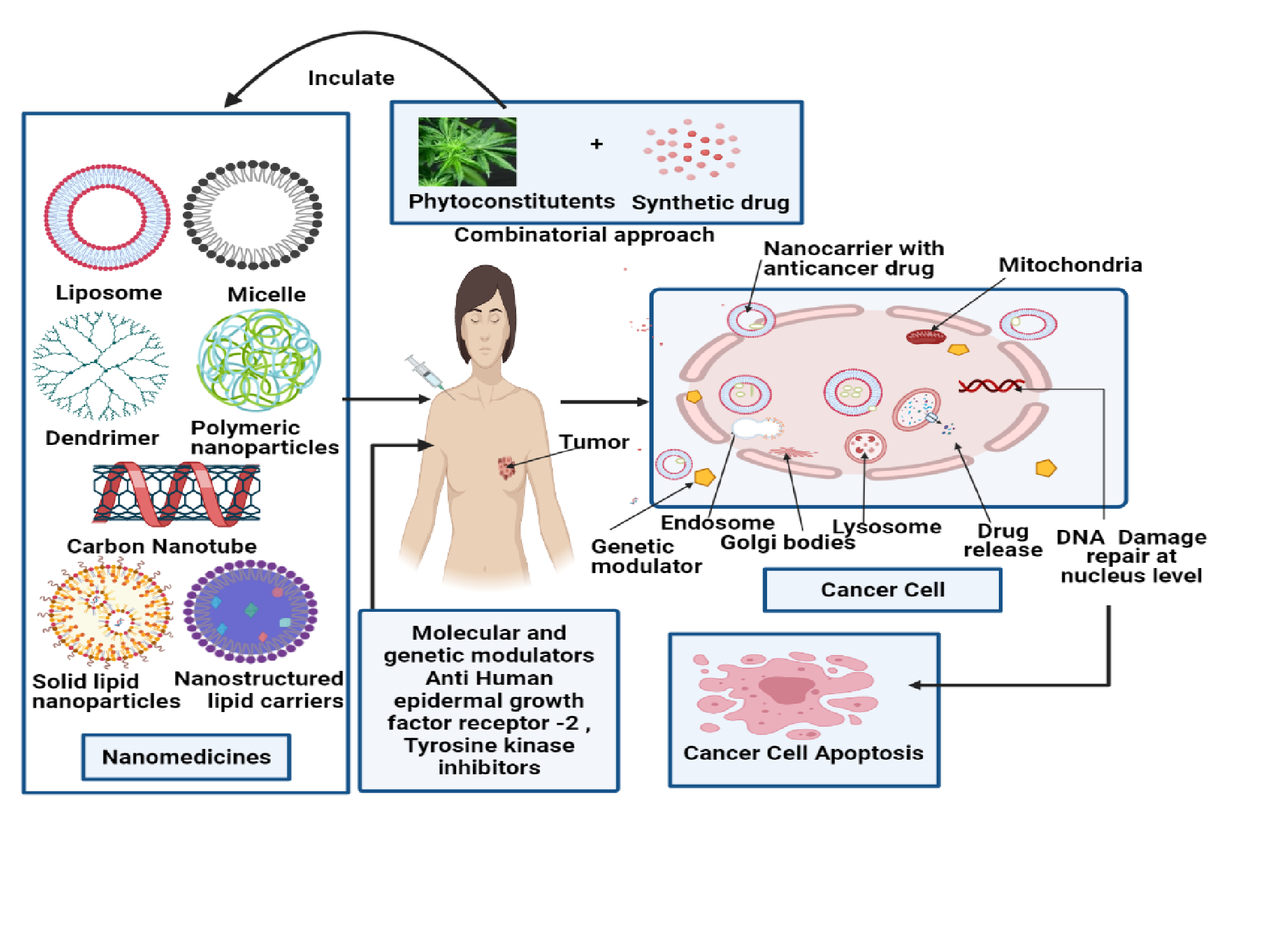
3. Combinatorial Nanocarrier-Based Drug Delivery for Anti-Tumor Agent Amalgamation in Breast Cancer
4. Perspective &Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tagde, P.; Kulkarni, G.T.; Mishra, D.K.; Kesharwani, P. Technology, Recent advances in folic acid engineered nanocarriers for treatment of breast cancer. J. Drug Deliv. Sci. Technol. 2020, 56, 101613. [Google Scholar] [CrossRef]
- Stevenson, J.; Farmer, R.D.T. HRT and breast cancer: A million women ride again. Climacteric 2020, 23, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer 2019, 11, 151. [Google Scholar] [CrossRef] [PubMed]
- McGhee, D.E.; Steele, J.R. Biomechanics of Breast Support for Active Women. Exerc. Sport Sci. Rev. 2020, 48, 99–109. [Google Scholar] [CrossRef]
- Adamson, K.; Rivedal, D.D.; Doren, E.L. Breast Reconstruction Following Breast Conserving Surgery: A Review. Curr. Surg. Rep. 2020, 8, 1–10. [Google Scholar] [CrossRef]
- Pyfer, B.J.; Jonczyk, M.; Jean, J.; Graham, R.A.; Chen, L.; Chatterjee, A. Analysis of Surgical Trends for Axillary Lymph Node Management in Patients with Ductal Carcinoma In Situ Using the NSQIP Database: Are We Following National Guidelines? Ann. Surg. Oncol. 2020, 27, 3448–3455. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-G.; Wang, J.; Lian, C.-L.; Lei, J.; Hua, L.; Lin, Q.; Chen, Y.-X.; He, Z.-Y. Evaluation of the 8th edition of the American joint committee on cancer’s pathological staging system in prognosis assessment and treatment decision making for stage T1-2N1 breast cancer after mastectomy. Breast 2020, 51, 2–10. [Google Scholar] [CrossRef]
- Chu, Q.D.; Li, T.; Hsieh, M.C.; Yi, Y.; Gibbs, J.F.; Lyons, J.M., III; Wu, X.C. Positive impact of the Patient Protection and Affordable Care Act Medicaid expansion on Louisiana women with breast cancer. Cancer 2021, 127, 688–699. [Google Scholar] [CrossRef] [PubMed]
- Colombage, U.N.; Lin, K.Y.; Soh, S.E.; Frawley, H.C.J.N. Urodynamics, Prevalence and impact of bladder and bowel disorders in women with breast cancer: A systematic review with meta-analysis. Neurourol. Urodyn. 2021, 40, 15–27. [Google Scholar] [CrossRef]
- Weedon-Fekjær, H.; Li, X.; Lee, S. Estimating the natural progression of non-invasive ductal carcinoma in situ breast cancer lesions using screening data. J. Med. Screen. 2020, 28, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.; Akolkar, D.; Patil, D.; Limaye, S.; Page, R.; Ranade, A.; Patil, R.; Patil, S.; Mhase, V.; Datta, V. Real-time non-invasive chemoresistance profiling of circulating tumor associated cells in breast cancers to determine resistance towards mitotic inhibitors. Eur. J. Cancer 2020, 138, S76–S77. [Google Scholar] [CrossRef]
- Magnuson, A.; Sedrak, M.S.; Gross, C.P.; Tew, W.P.; Klepin, H.D.; Wildes, T.M.; Muss, H.B.; Dotan, E.; Freedman, R.A.; O’Connor, T. Development and validation of a risk tool for predicting severe toxicity in older adults receiving chemotherapy for early-stage breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 608–618. [Google Scholar] [CrossRef] [PubMed]
- de Groot, S.; Lugtenberg, R.T.; Cohen, D.; Welters, M.J.; Ehsan, I.; Vreeswijk, M.P.; Smit, V.T.; de Graaf, H.; Heijns, J.B.; Portielje, J.E. Fasting mimicking diet as an adjunct to neoadjuvant chemotherapy for breast cancer in the multicentre randomized phase 2 DIRECT trial. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.X.; Suman, V.J.; Leitch, A.M.; Sanati, S.; Vij, K.R.; Unzeitig, G.W.; Hoog, J.; Watson, M.; Hahn, O.M.; Guenther, J.M. ALTERNATE: Neoadjuvant endocrine treatment (NET) approaches for clinical stage II or III estrogen receptor-positive HER2-negative breast cancer (ER+ HER2-BC) in postmenopausal (PM) women: Alliance A011106. Am. Soc. Clin. Oncol. JCO 2020, 38, 504. [Google Scholar] [CrossRef]
- Fouad, T.M.; Barrera, A.M.G.; Reuben, J.M.; Lucci, A.; Woodward, W.A.; Stauder, M.C.; Lim, B.; DeSnyder, S.M.; Arun, B.; Gildy, B. Inflammatory breast cancer: A proposed conceptual shift in the UICC–AJCC TNM staging system. Lancet Oncol. 2017, 18, e228–e232. [Google Scholar] [CrossRef]
- Azawi, S.; Liehr, T.; Rincic, M.; Manferrari, M. Molecular cytogenomic characterization of the murine breast cancer cell lines C-127I, EMT6/P and TA3 Hauschka. Int. J. Mol. Sci. 2020, 21, 4716. [Google Scholar] [CrossRef] [PubMed]
- Hills, N.; Leslie, M.; Davis, R.; Crowell, M.; Kameyama, H.; Rui, H.; Chervoneva, I.; Dooley, W.; Tanaka, T. Prolonged Time from Diagnosis to Breast-Conserving Surgery is Associated with Upstaging in Hormone Receptor-Positive Invasive Ductal Breast Carcinoma. Ann. Surg. Oncol. 2021, 28, 5895–5905. [Google Scholar] [CrossRef]
- Cominetti, M.R.; Altei, W.F.; Selistre-de-Araujo, H.S. Metastasis inhibition in breast cancer by targeting cancer cell extravasation. Breast CancerTargets Ther. 2019, 11, 165. [Google Scholar] [CrossRef]
- Available online: https://go.drugbank.com/drugs/DB00531 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB01248 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00990 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00675 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB01217 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00997 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00563 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00570 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB04572 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00947 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB01229 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00441 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB01006 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB09074 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB00445 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB08871 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB01101 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB04845 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB09073 (accessed on 20 February 2022).
- Available online: https://go.drugbank.com/drugs/DB11730 (accessed on 20 February 2022).
- Fraguas-Sánchez, A.I.; Martín-Sabroso, C.; Fernández-Carballido, A.; Torres-Suárez, A.I. Current status of nanomedicine in the chemotherapy of breast cancer. Cancer Chemother. Pharmacol. 2019, 84, 689–706. [Google Scholar] [CrossRef]
- Boucharaba, A.; Guillet, B.; Menaa, F.; Hneino, M.; van Wijnen, A.J.; Clézardin, P.; Peyruchaud, O. Bioactive lipids lysophosphatidic acid and sphingosine 1-phosphate mediate breast cancer cell biological functions through distinct mechanisms. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2009, 18, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Vanneman, M.; Dranoff, G. Combining immunotherapy and targeted therapies in cancer treatment. Nat. Rev. Cancer 2012, 12, 237–251. [Google Scholar] [CrossRef]
- Zhang, H.; Hu, H.; Zhang, H.; Dai, W.; Wang, X.; Wang, X.; Zhang, Q. Effects of PEGylated paclitaxel nanocrystals on breast cancer and its lung metastasis. Nanoscale 2015, 7, 10790–10800. [Google Scholar] [CrossRef] [PubMed]
- Tagde, P.; Tagde, P.; Islam, F.; Tagde, S.; Shah, M.; Hussain, Z.D.; Rahman, M.; Najda, A.; Alanazi, I.S.; Germoush, M.O. and Mohamed, H.R. The Multifaceted Role of Curcumin in Advanced Nanocurcumin Form in the Treatment and Management of Chronic Disorders. Molecules 2021, 26, 7109. [Google Scholar] [CrossRef] [PubMed]
- Dykman, L.A.; Khlebtsov, N.G. Uptake of engineered gold nanoparticles into mammalian cells. Chem. Rev. 2014, 114, 1258–1288. [Google Scholar] [CrossRef]
- Yang, M.; Gu, Y.; Tang, X.; Wang, T.; Liu, J. Advancement of lipid-based nanocarriers and combination application with physical penetration technique. Curr. Drug Deliv. 2019, 16, 312–324. [Google Scholar] [CrossRef]
- Plaza-Oliver, M.; Santander-Ortega, M.J.; Lozano, M.V. Current approaches in lipid-based nanocarriers for oral drug delivery. Drug Deliv. Transl. Res. 2021, 11, 471–497. [Google Scholar] [CrossRef]
- Tagde, P.; Tagde, S.; Bhattacharya, T.; Tagde, P.; Chopra, H.; Akter, R.; Kaushik, D.; Rahman, M. Blockchain and artificial intelligence technology in e-Health. Environ. Sci. Pollut. Res. 2021, 28, 52810–52831. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, E.J.; Langenhoven, L.; Grant, K.A.; van der Merwe, L.; Kotze, M. Clinical overestimation of HER2 positivity in early estrogen and progesterone receptor–positive breast cancer and the value of molecular subtyping using Blue Print. J. Glob. Oncol. 2017, 3, 314–322. [Google Scholar] [CrossRef]
- Day, E.S.; Bickford, L.R.; Slater, J.H.; Riggall, N.S.; Drezek, R.A.; West, J.L. Antibody-conjugated gold-gold sulfide nanoparticles as multifunctional agents for imaging and therapy of breast cancer. Int. J. Nanomed. 2010, 5, 445. [Google Scholar] [CrossRef]
- Cai, Z.; Chattopadhyay, N.; Yang, K.; Kwon, Y.L.; Yook, S.; Pignol, J.-P.; Reilly, R.M. 111In-labeled trastuzumab-modified gold nanoparticles are cytotoxic in vitro to HER2-positive breast cancer cells and arrest tumor growth in vivo in athymic mice after intratumoral injection. Nucl. Med. Biol. 2016, 43, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, P.; Vasaikar, S.; Wali, A. A landscape of nanomedicine innovations in India. Nanotechnol. Rev. 2018, 7, 131–148. [Google Scholar] [CrossRef]
- Patel, K.; Patel, K. Challenges and Recent Progress of Nano Sized Drug Delivery Systems for Lung Cancer Therapy: A Review. Himal. J. Health Sci. 2020, 5, 58–62. [Google Scholar]
- Fuhrhop, J.-H.; Wang, T. Bolaamphiphiles. Chem. Rev. 2004, 104, 2901–2938. [Google Scholar] [CrossRef] [PubMed]
- Tandel, H.; Bhatt, P.; Jain, K.; Shahiwala, A.; Misra, A. In-vitro and in-vivo tools in emerging drug delivery scenario: Challenges and updates. In In-Vitro and In-Vivo Tools in Drug Delivery Research for Optimum Clinical Outcomes; Mishra, A., shahiwala, A., Eds.; CRC Press, Tailor & Francis Group: Boca Raton, FL, USA, 2018; pp. 19–42. [Google Scholar]
- Wakaskar, R.R. General overview of lipid–polymer hybrid nanoparticles, dendrimers, micelles, liposomes, spongosomes and cubosomes. J. Drug Target. 2018, 26, 311–318. [Google Scholar] [CrossRef]
- Liao, Z.; Wong, S.W.; Yeo, H.L.; Zhao, Y. Nanocarriers for cancer treatment: Clinical impact and safety. NanoImpact 2020, 20, 100253. [Google Scholar] [CrossRef]
- Tagde, P.; Tagde, P.; Tagde, S.; Bhattacharya, T.; Garg, V.; Akter, R.; Rahman, M.H.; Najda, A.; Albadrani, G.M.; Sayed, A.A.; et al. Natural bioactive molecules: An alternative approach to the treatment and control of glioblastoma multiforme. Biomed. Pharmacother. 2021, 141, 111928. [Google Scholar] [CrossRef]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Solid lipid nanoparticles and nanostructured lipid carriers as novel drug delivery systems: Applications, advantages and disadvantages. Res. Pharm. Sci. 2018, 13, 288. [Google Scholar]
- Zhang, H.; Yu, N.; Chen, Y.; Yan, K.; Wang, X. Cationic liposome codelivering PI3K pathway regulator improves the response of BRCA1-deficient breast cancer cells to PARP1 inhibition. J. Cell. Biochem. 2019, 120, 13037–13045. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Hamidi, M. Passive and active targeting in cancer therapy by liposomes and lipid nanoparticles. Drug Metab. Pers. Ther. 2019, 34. [Google Scholar] [CrossRef]
- Zhao, M.; Ding, X.F.; Shen, J.Y.; Zhang, X.P.; Ding, X.W.; Xu, B. Use of liposomal doxorubicin for adjuvant chemotherapy of breast cancer in clinical practice. J. Zhejiang Univ.-SCIENCE B 2017, 18, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Yan, L.; Zhao, X.; Chen, X.; Li, A.; Zheng, D.; Zhou, X.; Dai, X.; Xu, F.-J. Versatile types of organic/inorganic nanohybrids: From strategic design to biomedical applications. Chem. Rev. 2018, 119, 1666–1762. [Google Scholar] [CrossRef]
- Yang, B.; Song, B.P.; Shankar, S.; Guller, A.; Deng, W. Recent advances in liposome formulations for breast cancer therapeutics. Cell. Mol. Life Sci. 2021, 78, 5225–5243. [Google Scholar] [CrossRef] [PubMed]
- Di Wu, M.S.; Xue, H.Y.; Wong, H.L. Nanomedicine applications in the treatment of breast cancer: Current state of the art. Int. J. Nanomed. 2017, 12, 5879–5892. [Google Scholar]
- Chowdhury, N.; Chaudhry, S.; Hall, N.; Olverson, G.; Zhang, Q.-J.; Mandal, T.; Dash, S.; Kundu, A. Targeted Delivery of Doxorubicin Liposomes for Her-2+ Breast Cancer Treatment. AAPS PharmSciTech 2020, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Abbasi, B.A.; Ahmad, R.; Mahmood, T.; Ali, B.; Khalil, A.T.; Kanwal, S.; Shah, S.A.; Alam, M.M.; Badshah, H.; et al. Nanomedicines for developing cancer nanotherapeutics: From benchtop to bedside and beyond. Appl. Microbiol. Biotechnol. 2018, 102, 9449–9470. [Google Scholar] [CrossRef] [PubMed]
- Rau, K.-M.; Lin, Y.-C.; Chen, Y.-Y.; Chen, J.-S.; Lee, K.-D.; Wang, C.-H.; Chang, H.-K. Pegylated liposomal doxorubicin (Lipo-Dox®) combined with cyclophosphamide and 5-fluorouracil is effective and safe as salvage chemotherapy in taxane-treated metastatic breast cancer: An open-label, multi-center, non-comparative phase II study. BMC Cancer 2015, 15, 1–8. [Google Scholar] [CrossRef]
- Burade, V.; Bhowmick, S.; Maiti, K.; Zalawadia, R.; Ruan, H.; Thennati, R. Lipodox®(generic doxorubicin hydrochloride liposome injection): In vivo efficacy and bioequivalence versus Caelyx®(doxorubicin hydrochloride liposome injection) in human mammary carcinoma (MX-1) xenograft and syngeneic fibrosarcoma (WEHI 164) mouse models. BMC Cancer 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Solinas, C.; Aiello, M.; Migliori, E.; Willard-Gallo, K.; Emens, L.A. Breast cancer vaccines: Heeding the lessons of the past to guide a path forward. Cancer Treat. Rev. 2020, 84, 101947. [Google Scholar] [CrossRef]
- Boulikas, T. Clinical overview on Lipoplatin™: A successful liposomal formulation of cisplatin. Expert Opin. Investig. Drugs 2009, 18, 1197–1218. [Google Scholar] [CrossRef]
- Awada, A.; Bondarenko, I.N.; Bonneterre, J.; Nowara, E.; Ferrero, J.M.; Bakshi, A.V.; Wilke, C.; Piccart, M.; CT4002 Study Group. A randomized controlled phase II trial of a novel composition of paclitaxel embedded into neutral and cationic lipids targeting tumor endothelial cells in advanced triple-negative breast cancer (TNBC). Ann. Oncol. 2014, 25, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Karkada, M.; Berinstein, N.L.; Mansour, M. Therapeutic vaccines and cancer: Focus on DPX-0907. Biol. Targets Ther. 2014, 8, 27. [Google Scholar] [CrossRef] [PubMed]
- Pilla, L.; Rivoltini, L.; Patuzzo, R.; Marrari, A.; Valdagni, R.; Parmiani, G. Multipeptide vaccination in cancer patients. Expert Opin. Biol. Ther. 2009, 9, 1043–1055. [Google Scholar] [CrossRef]
- Bulbake, U.; Doppalapudi, S.; Kommineni, N.; Khan, W. Liposomal formulations in clinical use: An updated review. Pharmaceutics 2017, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Henderson, I.C.; Allegra, J.; Woodcock, T.; Wolff, S.; Bryan, S.; Cartwright, K.; Dukart, G.; Henry, D. Randomized clinical trial comparing mitoxantrone with doxorubicin in previously treated patients with metastatic breast cancer. J. Clin. Oncol. 1989, 7, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Dickman, A. Integrated strategies for the successful management of breakthrough cancer pain. Curr. Opin. Supportive Palliat. Care 2011, 5, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Fishman, M.; Elsayed, Y.; Damjanov, N.; Steinberg, J.; Mahany, J.; Nieves, J.; Wanaski, S.; Dul, J.; Sherman, J. Phase I study of liposome entrapped paclitaxel (LEP-ETU) in patients with advanced cancer. J. Clin. Oncol. 2004, 22 (Suppl. 14), 2110. [Google Scholar] [CrossRef]
- May, J.P.; Li, S.-D. Hyperthermia-induced drug targeting. Expert Opin. Drug Deliv. 2013, 10, 511–527. [Google Scholar] [CrossRef]
- Espelin, C.W.; Leonard, S.C.; Geretti, E.; Wickham, T.J.; Hendriks, B.S. Dual HER2 targeting with trastuzumab and liposomal-encapsulated doxorubicin (MM-302) demonstrates synergistic antitumor activity in breast and gastric cancer. Cancer Res. 2016, 76, 1517–1527. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, Z.; Xie, C.; Zhao, Y. Dual-targeting liposome modified by glutamic hexapeptide and folic acid for bone metastatic breast cancer. Chem. Phys. Lipids 2020, 228, 104882. [Google Scholar] [CrossRef]
- Liang, Z.; Du, L.; Zhang, E.; Zhao, Y.; Wang, W.; Ma, P.; Dai, M.; Zhao, Q.; Xu, H.; Zhang, S.; et al. Targeted-delivery of siRNA via a polypeptide-modified liposome for the treatment of gp96 over-expressed breast cancer. Mater. Sci. Eng. C 2021, 121, 111847. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, M.; Ferraro, M.G.; Raucci, F.; Riccardi, C.; Saviano, A.; Russo Krauss, I.; Trifuoggi, M.; Caraglia, M.; Paduano, L.; Montesarchio, D.; et al. Safety and Efficacy Evaluation In Vivo of a Cationic Nucleolipid Nanosystem for the Nanodelivery of a Ruthenium (III) Complex with Superior Anticancer Bioactivity. Cancers 2021, 13, 5164. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, M.; Misso, G.; Ferraro, M.G.; Riccardi, C.; Capuozzo, A.; Zarone, M.R.; Maione, F.; Trifuoggi, M.; Stiuso, P.; D’Errico, G.; et al. Exploring cellular uptake, accumulation and mechanism of action of a cationic Ru-based nanosystem in human preclinical models of breast cancer. Sci. Rep. 2019, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.P.; da Silva Santos, S.; da Silva, J.V.; Parise-Filho, R.; Ferreira, E.I.; El Seoud, O.; Giarolla, J. Dendrimers in the context of nanomedicine. Int. J. Pharm. 2020, 573, 118814. [Google Scholar] [CrossRef]
- Narmani, A.; Mohammadnejad, J.; Yavari, K. Synthesis and evaluation of polyethylene glycol-and folic acid-conjugated polyamidoamine G4 dendrimer as nanocarrier. J. Drug Deliv. Sci. Technol. 2019, 50, 278–286. [Google Scholar] [CrossRef]
- Li, J.; Liang, H.; Liu, J.; Wang, Z. Poly (amidoamine)(PAMAM) dendrimer mediated delivery of drug and pDNA/siRNA for cancer therapy. Int. J. Pharm. 2018, 546, 215–225. [Google Scholar] [CrossRef]
- Janiszewska, J.; Posadas, I.; Játiva, P.; Bugaj-Zarebska, M.; Urbanczyk-Lipkowska, Z.; Ceña, V. Second generation amphiphilic poly-lysine dendrons inhibit glioblastoma cell proliferation without toxicity for neurons or astrocytes. PLoS ONE 2016, 11, e0165704. [Google Scholar]
- Alven, S.; Aderibigbe, B.A. The Therapeutic Efficacy of Dendrimer and Micelle Formulations for Breast Cancer Treatment. Pharmaceutics 2020, 12, 1212. [Google Scholar] [CrossRef]
- Mahmoudi, A.; Sadi, K.S.; Malaekeh-Nikouei, B. Surface engineered dendrimers as novel option for enhanced pharmaceutical and biomedical potential. In Dendrimer-Based Nanotherapeutics; Academic Press: Cambridge, MA, USA, 2021; pp. 225–252. [Google Scholar]
- Mehta, D.; Leong, N.; McLeod, V.M.; Kelly, B.D.; Pathak, R.; Owen, D.J.; Porter, C.J.; Kaminskas, L.M. Reducing dendrimer generation and PEG chain length increases drug release and promotes anticancer activity of PEGylated polylysine dendrimers conjugated with doxorubicin via a cathepsin-cleavable peptide linker. Mol. Pharm. 2018, 15, 4568–4576. [Google Scholar] [CrossRef]
- Aleanizy, F.S.; Alqahtani, F.Y.; Seto, S.; Al Khalil, N.; Aleshaiwi, L.; Alghamdi, M.; Alquadeib, B.; Alkahtani, H.; Aldarwesh, A.; Alqahtani, Q.H. Trastuzumab Targeted Neratinib Loaded Poly-Amidoamine Dendrimer Nanocapsules for Breast Cancer Therapy. Int. J. Nanomed. 2020, 15, 5433. [Google Scholar] [CrossRef]
- Deshmukh, A.S.; Chauhan, P.N.; Noolvi, M.N.; Chaturvedi, K.; Ganguly, K.; Shukla, S.S.; Nadagouda, M.N.; Aminabhavi, T.M. Polymeric micelles: Basic research to clinical practice. Int. J. Pharm. 2017, 532, 249–268. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Yamamoto, Y.; Yasunaga, M.; Koga, Y.; Kuroda, J.I.; Takigahira, M.; Harada, M.; Saito, H.; Hayashi, T.; Kato, Y. NC-6300, an epirubicin-incorporating micelle, extends the antitumor effect and reduces the cardiotoxicity of epirubicin. Cancer Sci. 2013, 104, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Danson, S.; Ferry, D.; Alakhov, V.; Margison, J.; Kerr, D.; Jowle, D.; Brampton, M.; Halbert, G.; Ranson, M. Phase I dose escalation and pharmacokinetic study of pluronic polymer-bound doxorubicin (SP1049C) in patients with advanced cancer. Br. J. Cancer 2004, 90, 2085–2091. [Google Scholar] [CrossRef] [PubMed]
- Venne, A.; Li, S.; Mandeville, R.; Kabanov, A.; Alakhov, V. Hypersensitizing effect of pluronic L61 on cytotoxic activity, transport, and subcellular distribution of doxorubicin in multiple drug-resistant cells. Cancer Res. 1996, 56, 3626–3629. [Google Scholar]
- Alakhov, V.; Klinski, E.; Li, S.; Pietrzynski, G.; Venne, A.; Batrakova, E.; Bronitch, T.; Kabanov, A. Block copolymer-based formulation of doxorubicin. From cell screen to clinical trials. Colloids Surf. BBiointerfaces 1999, 16, 113–134. [Google Scholar] [CrossRef]
- Sun, Y.; Zou, W.; Bian, S.; Huang, Y.; Tan, Y.; Liang, J.; Fan, Y.; Zhang, X. Bioreducible PAA-g-PEG graft micelles with high doxorubicin loading for targeted antitumor effect against mouse breast carcinoma. Biomaterials 2013, 34, 6818–6828. [Google Scholar] [CrossRef]
- Gener, P.; Gouveia, L.P.; Sabat, G.R.; de Sousa Rafael, D.F.; Fort, N.B.; Arranja, A.; Fernández, Y.; Prieto, R.M.; Ortega, J.S.; Arango, D. Biology; Medicine, Fluorescent CSC models evidence that targeted nanomedicines improve treatment sensitivity of breast and colon cancer stem cells. Nanomed. Nanotechnol. Biol. Med. 2015, 11, 1883–1892. [Google Scholar] [CrossRef]
- Lee, K.S.; Chung, H.C.; Im, S.A.; Park, Y.H.; Kim, C.S.; Kim, S.-B.; Rha, S.Y.; Lee, M.Y.; Ro, J. Multicenter phase II trial of Genexol-PM, a Cremophor-free, polymeric micelle formulation of paclitaxel, in patients with metastatic breast cancer. Breast Cancer Res. Treat. 2008, 108, 241–250. [Google Scholar] [CrossRef]
- Mukai, H.; Kogawa, T.; Matsubara, N.; Naito, Y.; Sasaki, M.; Hosono, A. A first-in-human Phase 1 study of epirubicin-conjugated polymer micelles (K-912/NC-6300) in patients with advanced or recurrent solid tumors. Investig. New Drugs 2017, 35, 307–314. [Google Scholar] [CrossRef]
- Matsumura, Y.; Hamaguchi, T.; Ura, T.; Muro, K.; Yamada, Y.; Shimada, Y.; Shirao, K.; Okusaka, T.; Ueno, H.; Ikeda, M.; et al. Phase I clinical trial and pharmacokinetic evaluation of NK911, a micelle-encapsulated doxorubicin. Br. J. Cancer 2004, 91, 1775–1781. [Google Scholar] [CrossRef]
- Kadokura, M.; Iwasa, S.; Honma, Y.; Kato, K.; Hamaguchi, T.; Yamada, Y.; Enomoto, N.; Shimada, Y. Weekly paclitaxel as second-line chemotherapy in Japanese patients with advanced gastric cancer. Anticancer. Res. 2013, 33, 4547–4552. [Google Scholar] [PubMed]
- Taurin, S.; Nehoff, H.; Diong, J.; Larsen, L.; Rosengren, R.J.; Greish, K. Curcumin-derivative nanomicelles for the treatment of triple negative breast cancer. J. Drug Target. 2013, 21, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Kutty, R.V.; Feng, S.-S. Cetuximab conjugated vitamin E TPGS micelles for targeted delivery of docetaxel for treatment of triple negative breast cancers. Biomaterials 2013, 34, 10160–10171. [Google Scholar] [CrossRef] [PubMed]
- Sargent, L.M.; Shvedova, A.; Hubbs, A.; Salisbury, J.; Benkovic, S.; Kashon, M.; Lowry, D.; Murray, A.; Kisin, E.; Friend, S.; et al. Induction of aneuploidy by single-walled carbon nanotubes. Environ. Mol. Mutagenesis 2009, 50, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Servant, A.; Jacobs, I.; Bussy, C.; Fabbro, C.; Da Ros, T.; Pach, E.; Ballesteros, B.; Prato, M.; Nicolay, K.; Kostarelos, K. Gadolinium-functionalised multi-walled carbon nanotubes as a T1 contrast agent for MRI cell labelling and tracking. Carbon 2016, 97, 126–133. [Google Scholar] [CrossRef]
- Hashemi, M.; Yadegari, A.; Yazdanpanah, G.; Omidi, M.; Jabbehdari, S.; Haghiralsadat, F.; Yazdian, F.; Tayebi, L. Normalization of doxorubicin release from graphene oxide: New approach for optimization of effective parameters on drug loading. Biotechnol. Appl. Biochem. 2017, 64, 433–442. [Google Scholar] [CrossRef]
- Huson, H.B.; Sanghani, M.V.; Mayra Lupe Llamas, C.; Leslie, E.; Botnick, M. Long-term community-based results of breast-conserving therapy in early-stage breast cancer. J. Community Supportive Oncol. 2016, 14, 249–254. [Google Scholar]
- Nasrollahi, F.; Varshosaz, J.; Khodadadi, A.A.; Lim, S.; Jahanian-Najafabadi, A. Targeted delivery of docetaxel by use of transferrin/poly (allylamine hydrochloride)-functionalized graphene oxide nanocarrier. ACS Appl. Mater. Interfaces 2016, 8, 13282–13293. [Google Scholar] [CrossRef]
- Shi, J.; Wang, B.; Wang, L.; Lu, T.; Fu, Y.; Zhang, H.; Zhang, Z. Fullerene (C60)-based tumor-targeting nanoparticles with “off-on” state for enhanced treatment of cancer. J. Control. Release 2016, 235, 245–258. [Google Scholar] [CrossRef]
- Jawahar, N.; De, A.; Jubee, S.; Reddy, E.S. Folic acid-conjugated raloxifene hydrochloride carbon nanotube for targeting breast cancer cells. Drug Dev. Res. 2020, 81, 305–314. [Google Scholar] [CrossRef]
- Akinoglu, E.; Ozbilgin, K.; Sonmez, P.K.; Ozkut, M.; Giersig, M.; Inan, S.; Gumustepe, E.; Kurtman, C. Biocompatibility of vertically aligned multi-walled carbon nanotube scaffolds for human breast cancer cell line MDA-MB-231. Prog. Biomater. 2017, 6, 189–196. [Google Scholar] [CrossRef]
- Crucho, C.I.; Barros, M.T. Polymeric nanoparticles: A study on the preparation variables and characterization methods. Mater. Sci. Eng. 2017, 80, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Cano, A.; Sánchez-López, E.; Ettcheto, M.; López-Machado, A.; Espina, M.; Souto, E.B.; Galindo, R.; Camins, A.; García, M.L.; Turowski, P. Current advances in the development of novel polymeric nanoparticles for the treatment of neurodegenerative diseases. Nanomedicine 2020, 15, 1239–1261. [Google Scholar] [CrossRef] [PubMed]
- Guterres, S.S.; Alves, M.P.; Pohlmann, A.R. Polymeric nanoparticles, nanospheres and nanocapsules, for cutaneous applications. Drug Target Insights 2007, 2, 117739280700200002. [Google Scholar] [CrossRef]
- Owens, D.E., III; Peppas, N.A. Opsonization, biodistribution, and pharmacokinetics of polymeric nanoparticles. Int. J. Pharm. 2006, 307, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Devulapally, R.; Sekar, N.M.; Sekar, T.V.; Foygel, K.; Massoud, T.F.; Willmann, J.K.; Paulmurugan, R. Polymer nanoparticles mediated codelivery of antimiR-10b and antimiR-21 for achieving triple negative breast cancer therapy. ACS Nano 2015, 9, 2290–2302. [Google Scholar] [CrossRef] [PubMed]
- Grewal, I.K.; Singh, S.; Arora, S.; Sharma, N. Polymeric nanoparticles for breast cancer therapy: A comprehensive review. Biointerface Res. Appl. Chem. 2020, 11, 11151–11171. [Google Scholar]
- Bahreyni, A.; Mohamud, Y.; Luo, H. Emerging nanomedicines for effective breast cancer immunotherapy. J. Nanobiotechnology 2020, 18, 1–14. [Google Scholar] [CrossRef]
- Hernandez-Aya, L.F.; Gao, F.; Goedegebuure, P.S.; Ma, C.X.; Ademuyiwa, F.O.; Park, H.; Peterson, L.L.; Bagegni, N.A.; Bose, R.; Gillanders, W.E. A randomized phase II study of nab-paclitaxel+ durvalumab+ neoantigen vaccine versus nab-paclitaxel+ durvalumab in metastatic triple-negative breast cancer (mTNBC). Am. Soc. Clin. Oncol. 2019, 37, 15_suppl. [Google Scholar] [CrossRef]
- Moreira, R.; Granja, A.; Pinheiro, M.; Reis, S. Nanomedicine Interventions in Clinical Trials for the Treatment of Metastatic Breast Cancer. Appl. Sci. 2021, 11, 1624. [Google Scholar] [CrossRef]
- Available online: https://clinicaltrials.gov/ct2/show/NCT00616967 (accessed on 20 February 2022).
- Andey, T.; Sudhakar, G.; Marepally, S.; Patel, A.; Banerjee, R.; Singh, M. Lipid nanocarriers of a lipid-conjugated estrogenic derivative inhibit tumor growth and enhance cisplatin activity against triple-negative breast cancer: Pharmacokinetic and efficacy evaluation. Mol. Pharm. 2015, 12, 1105–1120. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Pandit, J.; Sultana, Y.; Mishra, A.K.; Hazari, P.P.; Aqil, M. Optimization by design of etoposide loaded solid lipid nanoparticles for ocular delivery: Characterization, pharmacokinetic and deposition study. Mater. Sci. Eng. C 2019, 100, 959–970. [Google Scholar] [CrossRef] [PubMed]
- Aljaeid, B.M.; Hosny, K.M. Miconazole-loaded solid lipid nanoparticles: Formulation and evaluation of a novel formula with high bioavailability and antifungal activity. Int. J. Nanomed. 2016, 11, 441. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Bae, E.J.; Lee, M.-K. Enhanced anticancer activity and intracellular uptake of paclitaxel-containing solid lipid nanoparticles in multidrug-resistant breast cancer cells. Int. J. Nanomed. 2018, 13, 7549. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Mohammed, S. Breast cancer metastasis and the lymphatic system. Oncol. Lett. 2015, 10, 1233–1239. [Google Scholar] [CrossRef]
- Pindiprolu, S.K.S.; Chintamaneni, P.K.; Krishnamurthy, P.T.; Ratna Sree Ganapathineedi, K. Formulation-optimization of solid lipid nanocarrier system of STAT3 inhibitor to improve its activity in triple negative breast cancer cells. Drug Dev. Ind. Pharm. 2019, 45, 304–313. [Google Scholar] [CrossRef]
- Rompicharla, S.V.K.; Bhatt, H.; Shah, A.; Komanduri, N.; Vijayasarathy, D.; Ghosh, B.; Biswas, S. Formulation optimization, characterization, and evaluation of in vitro cytotoxic potential of curcumin loaded solid lipid nanoparticles for improved anticancer activity. Chem. Phys. Lipids 2017, 208, 10–18. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, L.; Chen, T.; Guo, W.; Bao, X.; Wang, D.; Ren, B.; Wang, H.; Li, Y.; Wang, Y. Anticancer effects of resveratrol-loaded solid lipid nanoparticles on human breast cancer cells. Molecules 2017, 22, 1814. [Google Scholar] [CrossRef]
- Sezer, C.V. An In Vitro Assessment of the Cytotoxic and Apoptotic Potency of Silymarin and Silymarin Loaded Solid Lipid Nanoparticles on Lung and Breast Cancer Cells. Pak. J. Zool. 2021, 53, 1407–1415. [Google Scholar] [CrossRef]
- Dawoud, M. Chitosan coated solid lipid nanoparticles as promising carriers for docetaxel. J. Drug Deliv. Sci. Technol. 2021, 62, 102409. [Google Scholar] [CrossRef]
- Yassemi, A.; Kashanian, S.; Zhaleh, H. Folic acid receptor-targeted solid lipid nanoparticles to enhance cytotoxicity of letrozole through induction of caspase-3 dependent-apoptosis for breast cancer treatment. Pharm. Dev. Technol. 2020, 25, 397–407. [Google Scholar] [CrossRef]
- Bhagwat, G.S.; Athawale, R.B.; Gude, R.P.; Md, S.; Alhakamy, N.A.; Fahmy, U.A.; Kesharwani, P. Formulation and Development of Transferrin Targeted Solid Lipid Nanoparticles for Breast Cancer Therapy. Front. Pharmacol. 2020, 11, 2064. [Google Scholar] [CrossRef] [PubMed]
- da Rocha, M.C.O.; da Silva, P.B.; Radicchi, M.A.; Andrade, B.Y.G.; de Oliveira, J.V.; Venus, T.; Merker, C.; Estrela-Lopis, I.; Longo, J.P.F.; Báo, S.N. Docetaxel-loaded solid lipid nanoparticles prevent tumor growth and lung metastasis of 4T1 murine mammary carcinoma cells. J. Nanobiotechnology 2020, 18, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, L.; Srivastava, S.; Panjeta, A.; Chaudhari, D.; Ghadi, R.; Kuche, K.; Malik, R.; Preet, S.; Jain, S.; Raza, K. Exploration of docetaxel palmitate and its solid lipid nanoparticles as a novel option for alleviating the rising concern of multi-drug resistance. Int. J. Pharm. 2020, 578, 119088. [Google Scholar] [CrossRef] [PubMed]
- Nayek, S.; Raghavendra, N.; Kumar, B.S. Development of novel S PC-3 gefitinib lipid nanoparticles for effective drug delivery in breast cancer. Tissue distribution studies and cell cytotoxicity analysis. J. Drug Deliv. Sci. Technol. 2021, 61, 102073. [Google Scholar] [CrossRef]
- Sabapati, M.; Palei, N.N.; Ashok Kumar, C.K.; Molakpogu, R.B. Solid lipid nanoparticles of Annona muricata fruit extract: Formulation, optimization and in vitro cytotoxicity studies. Drug Dev. Ind. Pharm. 2019, 45, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Zheng, M.; Yang, B.; Fu, H.; Li, Y. Pharmacotherapy, Improving breast cancer therapy using doxorubicin loaded solid lipid nanoparticles: Synthesis of a novel arginine-glycine-aspartic tripeptide conjugated, pH sensitive lipid and evaluation of the nanomedicine in vitro and in vivo. Biomed. Pharmacother. 2019, 116, 109006. [Google Scholar] [CrossRef]
- Wang, W.; Chen, T.; Xu, H.; Ren, B.; Cheng, X.; Qi, R.; Liu, H.; Wang, Y.; Yan, L.; Chen, S. Curcumin-loaded solid lipid nanoparticles enhanced anticancer efficiency in breast cancer. Molecules 2018, 23, 1578. [Google Scholar] [CrossRef]
- Badawi, N.M.; Teaima, M.H.; El-Say, K.M.; Attia, D.A.; El-Nabarawi, M.A.; Elmazar, M.M. Pomegranate extract-loaded solid lipid nanoparticles: Design, optimization, and in vitro cytotoxicity study. Int. J. Nanomed. 2018, 13, 1313. [Google Scholar] [CrossRef]
- Eskiler, G.G.; Cecener, G.; Egeli, U.; Tunca, B. Synthetically lethal BMN 673 (Talazoparib) loaded solid lipid nanoparticles for BRCA1 mutant triple negative breast cancer. Pharm. Res. 2018, 35, 1–20. [Google Scholar]
- Haider, M.; Abdin, S.M.; Kamal, L.; Orive, G. Nanostructured lipid carriers for delivery of chemotherapeutics: A review. Pharmaceutics 2020, 12, 288. [Google Scholar] [CrossRef] [PubMed]
- Müller, R.H.; Alexiev, U.; Sinambela, P.; Keck, C.M. Nanostructured lipid carriers (NLC): The second generation of solid lipid nanoparticles. In Percutaneous Penetration Enhancers Chemical Methods in Penetration Enhancement; Springer: Berlin/Heidelberg, Germany, 2016; pp. 161–185. [Google Scholar]
- Cortesi, R.; Valacchi, G.; Muresan, X.M.; Drechsler, M.; Contado, C.; Esposito, E.; Grandini, A.; Guerrini, A.; Forlani, G.; Sacchetti, G. Nanostructured lipid carriers (NLC) for the delivery of natural molecules with antimicrobial activity: Production, characterisation and in vitro studies. J. Microencapsul. 2017, 34, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Beloqui, A.; Solinís, M.Á.; Rodríguez-Gascón, A.; Almeida, A.J.; Préat, V. Nanostructured lipid carriers: Promising drug delivery systems for future clinics. Nanomed. Nanotechnol. Biol. Med. 2016, 12, 143–161. [Google Scholar] [CrossRef]
- Khosa, A.; Reddi, S.; Saha, R.N. Nanostructured lipid carriers for site-specific drug delivery. Biomed. Pharmacother. 2018, 103, 598–613. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Xu, X.; Zhao, Y.; Zhang, L.; Yu, Y.; Huang, F.; Yin, D.; Huang, H. Tumor targeted nanostructured lipid carrier co-delivering paclitaxel and indocyanine green for laser triggered synergetic therapy of cancer. RSC Adv. 2017, 7, 35086–35095. [Google Scholar] [CrossRef]
- Lin, M.; Teng, L.; Wang, Y.; Zhang, J.; Sun, X. Curcumin-guided nanotherapy: A lipid-based nanomedicine for targeted drug delivery in breast cancer therapy. Drug Deliv. 2016, 23, 1420–1425. [Google Scholar] [CrossRef]
- Chand, P.; Kumar, H.; Badduri, N.; Gupta, N.V.; Bettada, V.G.; Madhunapantula, S.V.; Kesharwani, S.S.; Dey, S.; Jain, V. Design and evaluation of cabazitaxel loaded NLCs against breast cancer cell lines. Colloids Surf. BBiointerfaces 2021, 199, 111535. [Google Scholar] [CrossRef]
- Gilani, S.J.; Bin-Jumah, M.; Rizwanullah, M.; Imam, S.S.; Imtiyaz, K.; Alshehri, S.; Rizvi, M.; Alam, M. Chitosan coated luteolin nanostructured lipid carriers: Optimization, in vitro-ex vivo assessments and cytotoxicity study in breast cancer cells. Coatings 2021, 11, 158. [Google Scholar] [CrossRef]
- Makeen, H.A.; Mohan, S.; Alkasim, M.A.; Sultan, M.H.; Albarraq, A.A.; Ahmed, R.A.; Alhazmi, H.A.; Alam, M.I. Preparation, Characterization and Anti-cancer Activity of Nanostructured Lipid Carriers Containing Imatinib. Pharmaceutics 2021, 13, 1086. [Google Scholar] [CrossRef]
- Soni, N.K.; Sonali, L.; Singh, A.; Mangla, B.; Neupane, Y.R.; Kohli, K.J.N. Nanostructured lipid carrier potentiated oral delivery of raloxifene for breast cancer treatment. Nanotechnology 2020, 31, 475101. [Google Scholar] [CrossRef]
- Karami, S.; Rostamizadeh, K.; Shademani, N.; Parsa, M. Synthesis and Investigation of the Curcumin-Loaded Magnetic Lipid Nanoparticles and Their Cytotoxicity Assessment on Human Breast Carcinoma Cell Line. Jundishapur J. Nat. Pharm. Prod. 2020, 15, 1–10. [Google Scholar] [CrossRef]
- Kamel, A.E.; Fadel, M.; Louis, D. Curcumin-loaded nanostructured lipid carriers prepared using Peceol™ and olive oil in photodynamic therapy: Development and application in breast cancer cell line. Int. J. Nanomed. 2019, 14, 5073. [Google Scholar] [CrossRef] [PubMed]
- Varshosaz, J.; Davoudi, M.A.; Rasoul-Amini, S. Docetaxel-loaded nanostructured lipid carriers functionalized with trastuzumab (Herceptin) for HER2-positive breast cancer cells. J. Liposome Res. 2018, 28, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Karim, R.; Palazzo, C.; Evrard, B.; Piel, G. Nanocarriers for the treatment of glioblastoma multiforme: Current state-of-the-art. J. Control. Release 2016, 227, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Quader, S.; Kataoka, K. Nanomaterial-enabled cancer therapy. Mol. Ther. 2017, 25, 1501–1513. [Google Scholar] [CrossRef]
- Teleanu, D.M.; Chircov, C.; Grumezescu, A.M.; Volceanov, A.; Teleanu, R.I. Blood-brain delivery methods using nanotechnology. Pharmaceutics 2018, 10, 269. [Google Scholar] [CrossRef] [PubMed]
- Elzoghby, A.O.; El-Lakany, S.A.; Helmy, M.W.; Abu-Serie, M.M.; Elgindy, N.A. Shell-crosslinked zein nanocapsules for oral codelivery of exemestane and resveratrol in breast cancer therapy. Nanomedicine 2017, 12, 2785–2805. [Google Scholar] [CrossRef]
- Tagde, P.; Tagde, S.; Tagde, P.; Bhattacharya, T.; Monzur, S.M.; Rahman, M.; Otrisal, P.; Behl, T.; Abdel-Daim, M.M.; Aleya, L.; et al. Nutraceuticals and Herbs in Reducing the Risk and Improving the Treatment of COVID-19 by Targeting SARS-CoV-2. Biomedicines 2021, 9, 1266. [Google Scholar] [CrossRef]
- Esfandiarpour-Boroujeni, S.; Bagheri-Khoulenjani, S.; Mirzadeh, H.; Amanpour, S. Fabrication and study of curcumin loaded nanoparticles based on folate-chitosan for breast cancer therapy application. Carbohydr. Polym. 2017, 168, 14–21. [Google Scholar] [CrossRef]
- Day, C.M.; Hickey, S.M.; Song, Y.; Plush, S.E.; Garg, S. Novel tamoxifen nanoformulations for improving breast cancer treatment: Old wine in new bottles. Molecules 2020, 25, 1182. [Google Scholar] [CrossRef]
- Guimarães, R.S.; Rodrigues, C.F.; Fernandes, N.; de Melo-Diogo, D.; Ferreira, P.; Correia, I.J.; Moreira, A.F. Combinatorial delivery of doxorubicin and acridine orange by gold core silica shell nanospheres functionalized with poly (ethylene glycol) and 4-methoxybenzamide for cancer targeted therapy. J. Inorg. Biochem. 2021, 219, 111433. [Google Scholar] [CrossRef]
- Khan, I.; Joshi, G.; Sarkar, B.; Nakhate, K.T.; Ajazuddin; Mantha, A.K.; Kumar, R.; Kaul, A.; Chaturvedi, S.; Mishra, A.K.; et al. Doxorubicin and crocin co-delivery by polymeric nanoparticles for enhanced anticancer potential in vitro and in vivo. ACS Appl. Bio Mater. 2020, 3, 7789–7799. [Google Scholar] [CrossRef]
- Mangla, B.; Neupane, Y.R.; Singh, A.; Kumar, P.; Shafi, S.; Kohli, K. Lipid-nanopotentiated combinatorial delivery of tamoxifen and sulforaphane: Ex vivo, in vivo and toxicity studies. Nanomedicine 2020, 15, 2563–2583. [Google Scholar] [CrossRef] [PubMed]
- Kunjiappan, S.; Sankaranarayanan, M.; Kumar, B.K.; Pavadai, P.; Babkiewicz, E.; Maszczyk, P.; Glodkowska-Mrowka, E.; Arunachalam, S.; Pandian, S.R.K.; Ravishankar, V.; et al. Capsaicin-loaded solid lipid nanoparticles: Design, biodistribution, in silico modeling and in vitro cytotoxicity evaluation. Nanotechnology 2020, 32, 095101. [Google Scholar] [CrossRef]
- Lerata, M.S.; D’Souza, S.; Sibuyi, N.R.; Dube, A.; Meyer, M.; Samaai, T.; Antunes, E.M.; Beukes, D.R. Encapsulation of variabilin in stearic acid solid lipid nanoparticles enhances its anticancer activity in vitro. Molecules 2020, 25, 830. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, R.; Pooja, D.; Kulhari, H.; Gudem, S.; Ravuri, H.G.; Bhargava, S.; Ramakrishna, S. Bombesin conjugated solid lipid nanoparticles for improved delivery of epigallocatechin gallate for breast cancer treatment. Chem. Phys. Lipids 2019, 224, 104770. [Google Scholar] [CrossRef]
- Ma, W.; Guo, Q.; Li, Y.; Wang, X.; Wang, J.; Tu, P. Co-assembly of doxorubicin and curcumin targeted micelles for synergistic delivery and improving anti-tumor efficacy. Eur. J. Pharm. Biopharm. 2017, 112, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Cai, Q.; Tang, Y.; Xu, Y.; Wang, Q.; Li, T.; Xu, H.; Wang, S.; Fan, K.; Liu, Z. PEGylated Lipid bilayer coated mesoporous silica nanoparticles for co-delivery of paclitaxel and curcumin: Design, characterization and its cytotoxic effect. Int. J. Pharm. 2018, 536, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Sun, N.; Cheng, R.; Zhao, C.; Liu, Z.; Li, X.; Liu, J.; Tian, Z. pH multistage responsive micellar system with charge-switch and PEG layer detachment for co-delivery of paclitaxel and curcumin to synergistically eliminate breast cancer stem cells. Biomaterials 2017, 147, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Ruttala, H.B.; Ko, Y.T. Liposomal co-delivery of curcumin and albumin/paclitaxel nanoparticle for enhanced synergistic antitumor efficacy. Colloids Surf. B Biointerfaces 2015, 128, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Aghazadeh, T.; Bakhtiari, N.; Rad, I.A.; Ramezani, F. Formulation of Kaempferol in Nanostructured Lipid Carriers (NLCs): A Delivery Platform to Sensitization of MDA-MB468 Breast Cancer Cells to Paclitaxel. Biointerface Res. Appl. Chem. 2021, 11, 14591–14601. [Google Scholar] [CrossRef]
- Li, X.; Jia, X.; Niu, H. Nanostructured lipid carriers co-delivering lapachone and doxorubicin for overcoming multidrug resistance in breast cancer therapy. Int. J. Nanomed. 2018, 13, 4107. [Google Scholar] [CrossRef] [PubMed]
- Lv, L.; Liu, C.; Chen, C.; Yu, X.; Chen, G.; Shi, Y.; Qin, F.; Ou, J.; Qiu, K.; Li, G. Quercetin and doxorubicin co-encapsulated biotin receptor-targeting nanoparticles for minimizing drug resistance in breast cancer. Oncotarget 2016, 7, 32184. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Indication | Treatment Approach |
|---|---|---|
| Stage 0 | Non-invasive breast cancers, such as ductal carcinoma in situ (DCIS) [11]. There is no sign of cancer cells or non-cancerous aberrant cells breaking out of the breast region where they began [12]. | |
| Stage I | Invasive breast cancers. The cancer either hasn’t spread beyond the breast or has spread in a very small amount to a lymph node [13]. | |
| Stage IA | Cancer has progressed to the fatty tissue of the breast. The tumor is no bigger than a shelled peanut. | Breast-conserving surgery or mastectomy may be used to treat these cancers. A sentinel lymph node biopsy (SLNB) or an axillary lymph node dissection will be required to examine the adjacent lymph nodes (ALND). Hormonal therapy is prescribed for people with hormone-receptor-positive cancer. Immunotherapy may be recommended before and after surgery if the cancer is triple-negative. Targeted therapy, such as trastuzumab (Herceptin), either alone or alongside chemotherapy recommended for HER2 positive [13]. |
| Stage IB | Cancer cells have been discovered in a few lymph nodes, but only in trace levels. | |
| Stage II | Cancer has grown or spreads [14]. | |
| Stage IIA | Indicates that the breast tumor, if present, is still tiny. It’s possible that there’s no cancer in the lymph nodes or that it’s spread to three or more. | Some systemic therapies may benefit in stage II and are given before surgery (neoadjuvant therapy), whereas others are given after (adjuvant therapy). The drugs utilized will be chosen by the woman’s age and tumor test findings, including Chemotherapy, Hormone therapy and HER2 targeted drugs [14]. |
| Stage IIB | Tumor is larger, ranging in size from a walnut to a lime. | |
| Stage III | Although cancer has not progressed to the bones or organs, it is considered advanced and more difficult to treat [15]. | |
| Stage IIIA | Indicates that cancer discovered in up to nine lymph nodes that run from your armpit to your collarbone in a chain. It may have spread to or swollen the nodules deep within your breast. There is a huge tumor in the breast in some cases, yet there is no tumor in others even if the tumor hasn’t migrated to the lymph nodes. | There are two main approaches to treating stage III breast cancer:Neoadjuvant chemotherapy (before surgery). Trastuzumab (Herceptin), a targeted medication for HER2-positive malignancies, is also used, sometimes with pertuzumab (Perjeta). This may cause the tumor to shrink to the point where a woman may receive breast-conserving surgery (BCS) [15]. A mastectomy is going to perform if the tumor does not shrink enough. Lymph nodes in the area will also need to be examined. For stage III malignancies, a sentinel lymph node biopsy (SLNB) is typically not an option. Instead, an ALND is usually performed. After surgery, radiation treatment is often required. Additional chemo may be administered following surgery in rare circumstances. Some women with HER2-positive malignancies will be treated for up to a year with trastuzumab (with or without pertuzumab) after surgery. Many women with HER2-positive malignancies will be treated with trastuzumab (with or without pertuzumab) for up to a year, followed by surgery and additional trastuzumab (with or without pertuzumab). If any residual cancer is identified at the time of surgery following neoadjuvant treatment, trastuzumab may be switched to a new medicine called ado-trastuzumab emtansine, which is given every three weeks for 14 doses [16]. If hormone receptor-positive cancer in lymph nodes and have finished a year of trastuzumab, in such condition doctor may propose therapy with neratinib, an oral medication. Adjuvant hormone treatment will be given to women with hormone receptor-positive (ER-positive or PR-positive) breast tumors, which may usually be administered simultaneously as trastuzumab. |
| Stage IIIB | Indicates that it has spread into the chest wall or skin around your breast. | |
| Stage IV | Breast cancer cells have gone beyond the breast and into the lymph nodes surrounding it. Skeletal bones, lungs, liver, and brain are the most prevalent locations. The term “metastatic” refers to the fact that cancer has moved beyond the part of the body where it has been initially discovered [16]. | Chemotherapy is a treatment for advanced-stage breast cancer that kills or damages as many cancer cells as possible. Chemotherapy is often used to treat advanced-stage breast cancer since it affects the whole body. Newer chemotherapy medications, such as Taxol (paclitaxel), Abraxane (albumin-bound or nab-paclitaxel), Taxotere (docetaxel), Adriamycin (doxorubicin), Ellence (epirubicin), and Halaven (erubilin), have been found to help women with advanced-stage breast cancer survive longer. Gemzar (chemical name: gemcitabine), Xeloda (chemical name: capecitabine), Navelbine (chemical name: vinorelbine), and Ixempra are some of the other chemotherapies utilized in metastatic breast cancer (chemical name: ixabepilone) [16,17]. |
| Molecular Sub Type | Indication | Other Condition | HarmoneTherapy | Chemotherapy | Anti-HER2 (Trastuzu-Mab) |
|---|---|---|---|---|---|
| Luminal A | The most prevalent molecular type, Luminal A tumors, develops at a slower pace than other cancers [18]. | Low tumor burden | Yes | No | No |
| High tumor burden * or grade 3 | Yes | Yes | No | ||
| Luminal B | More aggressive than luminal A cancer cells because they develop quicker. | HER2+ | Yes | Yes | Yes |
| HER2− | Yes | Yes | No | ||
| Triple-negative breast cancer (TNBC) | TNBC was more likely to occur in females with early menarche, larger waist-to-hip ratio, greater fecundity, shorter duration of breastfeeding, higher body mass index, and became more prevalent in premenopausal patients, according to several epidemiological studies. | Not applicable | No | Yes | No |
| HER2-positive | Cancers tend to grow faster than luminal cancers and can have a worse prognosis, but they are often success-fully treated with targeted therapies aimed at the HER2 protein. | Not applicable | No | Yes | Yes |
| Normal-like breast cancer | It closely matches luminal A (Breast cancer is a diverse disease at the molecular level, with activation of the HER2, stimulation of hormone receptors (estrogen receptor and progesterone receptor), and/or BRCA mutations being the most common molecular hallmarks.) Treatment options vary depending on the molecular subtype. Conventional cancer chemotherapies have limitations, such as drug resistance and non-differentiation between healthy and malignant cells, which leads to significant side effects and systemic toxicity [18]. | ||||
| Generic Name or Brand Name | Background | Molecular Structure | Stage | Dosage &Strength | Route | References |
|---|---|---|---|---|---|---|
| Trastuzumab (Herceptin) | Trastuzumab is a recombinant IgG1 kappa, humanized monoclonal antibody that selectively binds with high affinity in a cell-based assay (Kd = 5 nM) to the extracellular domain of the human epidermal growth factor receptor protein (HER2). | C6470H10012N1726O2013S42 | HER2+ | Powder, for solution (440 mg/ vial) | Iv | [13,14] |
| Injection, powder, for solution (150 mg, 150 mg/7.4 mL). | ||||||
| Injection, solution (600mg) | Sc | |||||
| Pertuzumab (Perjeta) | Pertuzumab is an antineoplastic agent used in the treatment of HER2-positive metastatic breast cancer in combination with other antineoplastic agents. | C17H27NO2 | Metastatic HER2+ in patients who have not been treated with hormone therapy or chemotherapy. | Injection, solution, concentrate (420 mg) | Iv | [15] |
| As neoadjuvant therapy in patients with locally advanced, inflammatory, or early-stage cancer; as adjuvant therapy in patients with early-stage cancer who have a high recurrence risk | Pertuzumab (420 mg/14 mL) + Trastuzumab (440 mg/vial),Powder, for solution; Solution. | Iv | ||||
| Pertuzumab (1200 mg) + Trastuzumab (600 mg), Injection, Solution. | Sc | |||||
| Pertuzumab (1200 mg/15 mL) + Hyaluronidase (human recombinant) (30,000 U/15 mL) + Trastuzumab (600 mg/15 mL), Injection, Solution. | Sc | |||||
| Ado-Trastuzumab Emtansine (Kadcyla) | Ado-Trastuzumab emtansine, is a first-in-class HER2 antibody drug conjugate (ADC) composed of Genentech’s trastuzumab antibody and ImmunoGen’s cell-killing chemical, DM1. | C6448H9948N1720O2012S44•(C47H62ClN4O13S)n | Used in patients with HER2-positive metastatic breast cancer who have previously received taxane and/or trastuzumab for metastatic cancer or who had a recurrence of their cancer within six months after adjuvant therapy. | Injection, powder, lyophilized, for solution (20 mg/1 mL, 100 mg) | Iv | [16,17,18] |
| Powder, for solution (160 mg/vial). | ||||||
| Abemaciclib (Verzenio) | Abemaciclib is an antitumor agent and dual inhibitor of cyclin-dependent kinases 4 (CDK4) and 6 (CDK6) that are involved in the cell cycle and promotion of cancer cell growth in case of unregulated activity. | C27H32F2N8 | As Monotherapy: Advanced or metastatic HR+ and HER2− | Starting dose:
| Oral | [18,19] |
| In combination with an aromatase inhibitor: Initial endocrine-based therapy for postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer | ||||||
| In combination with fulvestrant: For women with hormone receptor (HR)-positive, (HER2)-negative advanced or metastatic breast cancer with disease progression following endocrine therapy | ||||||
| Cyclophosphamide (Cytoxan, Endoxan, Cycloblastin, Neosar, Revimmune) | Precursor of the alkylating nitrogen mustard anticancer and immunosuppressive drug aldophosphamide, which must be activated in the liver to create the active aldophosphamide | C7H15Cl2N2O2P | Advanced or metastatic | Injection, powder, for solution (2 g/100 mL) | Iv; Oral | [19,20] |
| Tablet (25 mg/L) | Oral | |||||
| Capsule (25 mg/L) | Oral | |||||
| Docetaxel (Taxotere) | Docetaxel is a well-known anti-mitotic chemotherapy drug that is mostly used to treat breast, ovarian, and non-small cell lung cancer. Docetaxel binds to tubulin reversibly and with a high affinity in a 1:1 stoichiometric ratio. | C43H53NO14 | Metastatic cancer that has not gotten better with other chemotherapy or node positive cancer removed by surgery | Injection (10 mg/1 mL, 80 mg/4 mL, 160 mg/8 mL) | Iv | [19,21] |
| Injection, solution, concentrate(20 mg/1 mL) | ||||||
| Exemestane (Aromasin) | Exemestane is an oral steroidal aromatase inhibitor used in the adjuvant treatment of hormonally-responsive breast cancer in postmenopausal women. It irreversibly binds to the active site of the enzyme resulting in permanent inhibition. | C20H24O2 | Early stage, advanced or ER+. | Tablet (25 mg) | Oral | [19,22] |
| Tamoxifen Citrate | Tamoxifen is a selective estrogen receptor modulator used to treat estrogen receptor positive breast cancer, reduce the risk of invasive breast cancer following surgery, or reduce the risk of breast cancer in high risk women. | C26H29NO | Advanced or metastatic ER+ | Nolvadex:Tablet(20 mg/L, 10 mg/L) | Oral | [19,23] |
| Tamofen:Tablet (10 mg, 20 mg) | ||||||
| Soltamox:Liquid(20 mg/10 mL or 10 mg/5 mL) | ||||||
| Tamone:Tablet (10mg) | ||||||
| Anastrazole (Arimidex) | Anastrozole is a non-steroidal aromatase inhibitor (AI) comparable to letrozole that is used to treat postmenopausal women with estrogen-responsive breast cancer. | C17H19N5 | Early-stage, HR+ in women who have already received other treatment; HR+ locally advanced or metastatic breast cancer or hormone receptor unknown; advanced breast cancer that has gotten worse after treatment with tamoxifen citrate | Tablet, film coated (1 mg/mL) | Oral | [19,24] |
| Pellet Anastrozole (20 mg/L) + Testosterone (200 mg/L) | Oral | |||||
| Pellet, implantable Anastrozole (4 mg/L) + Testosterone (60 mg/L) | Sc | |||||
| Doxorubicin | Doxorubicin is a cytotoxic anthracycline antibiotic isolated from cultures of Streptomyces peucetius var. caesius. | C27H29NO11 | Node-positive cancer removed by surgery | Adriamycin: Solution (2 mg/mL) | Iv; Ives | [19,25] |
| Caelyx: Injection, solution, concentrate (2 mg/mL) | Iv | |||||
| Methotrexate (Rheumatrex, Trexall) | Methotrexate is a folate derivative that inhibits several enzymes responsible for nucleotide synthesis. This inhibition leads to suppression of inflammation as well as prevention of cell division. Because of these effects, methotrexate is often used to treat inflammation caused by arthritis or to control cell division in neoplastic diseases such as breast cancer and non-Hodgkin’s lymphoma | C20H22N8O5 | Advanced or metastatic | Tablet (2.5 mg/L) | Oral | [19,26] |
| Solution (25 mg/mL) | Im; Ia; Iv | |||||
| Vinblastine Sulfate (Velban) | Antitumor alkaloid isolated from Vinca rosea and used to treat breast cancer, testicular cancer, neuroblastoma, Hodgkin’s and non-Hodgkins lymphoma, mycosis fungoides, histiocytosis, and Kaposi’s sarcoma | C46H58N4O9 | Advanced or metastatic | Solution (1 mg/1 mL) | Iv | [19,27] |
| Thiotepa (Thioplex) | Alkalyting agent and is mostly used to treat breast cancer, ovarian cancer, and bladder cancer. It is also used as conditioning for bone marrow transplantation. Its main toxicity is myelosuppression. | C6H12N3PS | Advanced or metastatic | Injection, powder, for solution (100 mg; 15 mg; 30 mg) | Ic; Iv; Ives | [28] |
| Fulvestrant (Faslodex) | Fulvestrant is an estrogen receptor antagonist used to treat HR+ breast cancer that may also be HER2−. | C32H47F5O3S | HR+ and HER2− advanced cancer that has not been treated with hormone therapy; HR+ advanced cancer that got worse after treatment with hormone therapy or combined; used with palbociclib or abemaciclib in women with HR+ and HER2− advanced or metastatic cancer that got worse after treatment with hormone therapy | Injection, solution (50 mg/1 mL or 250 mg/5 mL) | Im | [29] |
| Paclitaxel (Abraxane) | Paclitaxel is a taxoid chemotherapeutic agent isolated from the bark of the Pacific yew tree, used as first-line and subsequent therapy for the treatment of advanced carcinoma of the ovary, and other various cancers including breast and lung cancer. | C47H51NO14 | Recurrent or metastatic | Injection, solution (6 mg/1 mL, 30 mg/5 mL, 300 mg/50 mL) | Iv | [16,17,30] |
| Gemcitabine Hydrochloride(Gemzar) | Gemcitabine is a nucleoside metabolic inhibitor used as adjunct therapy in the treatment of certain types of ovarian cancer, non-small cell lung carcinoma, metastatic breast cancer, and as a single agent for pancreatic cancer. | C9H11F2N3O4 | Combined with paclitaxel in cancer that has not gotten better with other chemotherapy | Injection, solution (38 mg/1 mL, 200 mg/vial, 1 g/vial, 2 g/vial) | Iv | [31] |
| Letrozole (Femara) | Letrozole is an aromatase inhibitor used to treat breast cancer in postmenopausal women. | C17H11N5 | Early-stage HR+ in women who have already received other treatment; early-stage cancer that has been treated with tamoxifen citrate for at least five years; locally, advanced or metastatic HER2+ and HR+ or HR−; advanced cancer that has gotten worse after anti-estrogen therapy. | Tablet, film coating (2.5 mg) | Oral | [32] |
| Letrozole (2.5 mg/L) + Ribociclib succinate (200 mg/L) | ||||||
| Olaparib (Lynparza) | Olaparib is a chemotherapeutic agent used to treat recurrent or advanced ovarian cancer and metastatic breast cancer in patients with specific mutations and prior history of chemotherapy. | C24H23FN4O3 | Metastatic HER2− with certain mutations in the BRCA1 or BRCA2 genes in patients who have been treated with chemotherapy given before or after surgery. | Tablet, film coated (100 mg, 100 mg/L, 150 mg, 150 mg/L) | Oral | [33] |
| Capsule (50 mg, 50 mg/L) | ||||||
| Epirubicin (Ellence) | Epirubicin is an anthracycline topoisomerase II inhibitor used as an adjuvant to treating axillary node metastases in patients who have undergone surgical resection of primary breast cancer. | C27H29NO11 | Node-positive breast cancer removed by surgery | Injection, solution (2 mg/1 mL) | Iv | [34] |
| Eribulin Mesylate (Halaven) | Eribulin is a microtubule inhibitor used to treat metastatic breast cancer and metastatic or unresectable liposarcoma. | C40H59NO11 | Patients who have been treated with anthracycline and taxane | Injection, solution (0.44 mg/mL, 0.5 mg/1 mL) | Iv | [35] |
| Capecitabine (Xeloda) | Capecitabine is an orally-administered chemotherapeutic agent used in the treatment of metastatic breast and colorectal cancers. Capecitabine is a prodrug, that is enzymatically converted to fluorouracil (antimetabolite) in the tumor, where it inhibits DNA synthesis and slows growth of tumor tissue. | C15H22FN3O6 | Metastatic cancer that has not gotten better with other chemotherapy | Tablet, film coated (150 mg, 500 mg) | Oral | [36] |
| Ixabepilone (Ixempra) | Ixabepilone is a microtubule inhibitor administered in combination with capecitabine or alone in the treatment of metastatic or locally advanced breast cancer that has shown inadequate response to taxanes and anthracyclines. | C27H42N2O5S | Locally advanced or metastatic cancer that has not gotten better with other chemotherapy | Kit (15 mg/15 mg, 45 mg/45 mg) | Iv | [37] |
| Palbociclib (Ibrance) | Palbociclib is an endocrine-based chemotherapeutic agent used in combination with other antineoplastic agents to treat HER2-negative and HR-positive advanced or metastatic breast cancer. | C24H29N7O2 | Recurrent or metastatic | Tablet, film coated (75 mg, 100 mg, 125 mg/L) | Oral | [38] |
| Capsule (75 mg, 75 mg/L, 125 mg/L) | ||||||
| Ribociclib (Kisqali) | Ribociclib is a kinase inhibitor used to treat HR+, HER2− advanced or metastatic breast cancer. | C23H30N8O | Recurrent or metastatic | Tablet, film coated (200 mg, 200 mg/L) | Oral | [39] |
| Challenges to Breast Cancer Drug Therapy | How Nanomedicine Can Help |
|---|---|
| 1.Low specificity for breast cancer | Nanomedicine uses passive and active targeting to enhance tumor medication levels while decreasing drug levels in noncancerous cells. |
| 2. Undesirable pharmacokinetics such as quick clearance and short half-life | Use of strategies such as PEGlyation to extend the circulation time. |
| 3. Anticancer drugs or excipients, such as surfactants and organic co-solvents, have dose-limiting toxicity. | Tumor progression selectivity; regulated medication release from nanocarrier; solvent- and surfactant-free nanoformulation. |
| 4. Drug resistance at cellular level, for example, increased drug efflux transport | Both passive and active targeting may improve endocytosis; some nanoformulations may block drug efflux processes; and co-delivery of medicines that target drug resistance mechanisms may improve endocytosis. |
| 5. Lower pH, hypoxia, cancer microenvironment interaction, and other factors contribute to drug resistance in the tumour microenvironment. | Targeting tumor microenvironment; use of stimulus-responsive nanoformulations such as pH-responsive devices. |
| 6. Difficulty in eradicating cancer stem cells | Targeting cancer stem cells. |
| Nanocarrier | Advantages | Disadvantages | Reference |
|---|---|---|---|
| Liposome | Uses for a wide variety of drugs and capable of increasing drug load while reducing unwanted drug activity. | Toxicity is caused by cationic lipids. The mononuclear phagocyte system degrades the nanocarriers quickly. | [56] |
| Dendrimer | It has higher loading capacity due to a variety of multifunctional surface groups and intracellular cavities, as well as it has high bioavailability. | Rapid clearance, organ accumulation, synthesis variability | [56] |
| Micelles | Reduction of toxicity and other adverse effects. | Use only for lipophilic drugs, low drug loading capacity | [56,57] |
| Carbon nanotube | To deliver chemotherapeutic and imaging agents, it must be capable of penetrating and localize at the cellular level. | Potential material toxicity | [57] |
| Polymeric nanoparticles | These are biocompatible, biodegradable, nontoxic, have a longer blood circulation time, less drug change, are less reactive to enzymatic degradation, and site-targeted administration. | Degradation of the carrier | [58] |
| Solid lipid nanoparticles (SLNs) | Due to its organic nature, it has a high solubility and bioavailability. | ||
| The kinetics of medication release can be better controlled. | Low drug loading capacities Possibly containing other colloidal structures and complex physical state | [59] | |
| Nanostructured lipid carrier (NLCs) | It is second generation SLNs having high drug loading and entrapment potential. | ||
| Long-term stability, prevent particles from coalescing, low toxicity, biodegradation, drug protection. | Gelation of lipid dispersion Polymorphic transition | [59] | |
| Biocompatible to a high degree. | |||
| Organic solvents may be avoided since the procedures are water-based. | |||
| Simple to scale-up and sterilize, and they are less costly than other materials. | |||
| Carriers based on polymers or surfactants. | |||
| Improve drug release control and/or target. | |||
| When compared to other NLCs, NLCs provide excellent and greater medication content. | |||
| NLCs may transport both lipophilic and hydrophilic molecules. Biodegradability of the majority of lipids. |
| Brand Name | Therapeutic Agent | Clinical Trial Phase | Company Name | Reference |
|---|---|---|---|---|
| Doxil | DOX | Approved | Sequus Pharmaceuticals Inc. | [68] |
| LipoDox | DOX | Approved | Sun Pharmaceutical Industries Ltd. | [69] |
| dHER2+AS15 | HER2 antigen | Phase 1/Phase 2 | GlaxoSmithKline | [75] |
| Lipoplatin | Cisplatin | Phase III | Regulon Inc. | [71] |
| EndoTAG1 | Paclitaxel | Completed | MediGene | [72] |
| DPX-0907 | Multicancer-associated antigens | Completed | ImmunoVaccine Technologies | [73,74] |
| LEM-ETU | Mitoxantrone | Phase I | NeoPharm Inc | [75,76] |
| Myocet™ | DOX | Approved | Elan Pharma | [77] |
| LEP-ETU | Paclitaxel | Phase II | NeoPharm Inc | [78] |
| ThermoDox™ | DOX | Phase III | Celsion | [79] |
| MM-302 | DOX | Phase 1 | Merrimack Pharmaceuticals | [80] |
| Brand Name | Therapeutic Agent | Clinical Trial Phase | Company Name | Reference |
|---|---|---|---|---|
| DEP® docetaxel | Docetaxel | Phase I | Starpharma | [90] |
| MAG-Tn3 | Vaccine composed of tri Tnglycotope | Phase I | Institute Pasteur | [85] |
| Brand Name | Therapeutic Agent | Clinical Trial Phase | Company Name | Reference |
|---|---|---|---|---|
| Genexol-PM™ | Paclitaxel | Phase II | Samyang | [100] |
| NC-6300 | Epirubicin | Phase I | Nanocarrier Co. | [101] |
| NK911 | Doxorubicin | Phase II | Nippon Kayaku Co. | [102] |
| NK105 | Paclitaxel | Phase III | Nippon Kayaku Co. | [103] |
| Brand Name | Therapeutic Agent | Clinical Trial Phase | Company Name | Reference |
|---|---|---|---|---|
| NCT00629499 P | Paclitaxel/Cyclophosphamide | Phase II | SCRI DevelopmentInnovations, LLC | [119] |
| NCT04249167 | Cryoablation, atezolizumab/nab-paclitaxel | Early Phase I | Mayo Clinic | [120] |
| NCT03606967 | Paclitaxel and durvalumab with or without neoantigen vaccine | Phase II | National Cancer Institute (NCI) | [121] |
| NCT00407888 | Doxorubicin hydrochloride, cyclophosphamide, and filgrastim followed by paclitaxel | Phase II | University of Washington | [122] |
| NCT00616967 | Carboplatin and nab-paclitaxel with or without vorinostat | Phase II | Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins | [123] |
| Lipid | Surfactant | HLB Value |
|---|---|---|
| Mixtures of mono-, di- and triglycerides Witeposol bases Glyceryl monostearate (Imwitor900), Glyceryl behenate (Compritol888ATO) and Glycerylpalmitosterate (PrecirolATO5) | Polysorbate80 | 15 |
| Sodium cholate | 18 | |
| Sodium glycocholate | 14.9 | |
| Cetylpyridiniumchloride | 15 | |
| Sodium dodecylsulphate | 40 | |
| Sodiumoleate | 18 | |
| Polyvinylalcohol | 15–19 | |
| CremophorEL | 12–14 | |
| Waxes Beeswax and Cetylpalmitate | Lecithin | 4–9 |
| Poloxamer188 | 29 | |
| Solid fatty acids Stearic acid, Palmitic acid and Behenic acid | Poloxamer407 | 21.5 |
| Tyloxapol | - | |
| Other lipids Miglyol812 and Paraffin | Polysorbate20 | 16.7 |
| Polysorbate60 | 14.9 |
| Cytotoxic Agents | Method of Preparation | Interventions | Reference |
|---|---|---|---|
| Silymarin | Hot homogenization method | Reduced A549 and MCF-7 cell proliferation induced apoptosis in both cells and increased bioavailability. In mammary carcinogenesis | [132] |
| Chitosan encapsulating Docetaxel | Hot homogenization method | Particle size was increased from 143 ± 2.5–225 nm ± 3.6, and the surface charge was reversed from 35 ± 3.3 to 25 mV± 2.1. Slower drug release, increased cytotoxicity in vitro, and tumor inhibition | [133] |
| Letrozole (Folic acid targeted) | Solvent emulsification evaporation | Enhanced biocompatibility and triggering apoptosis in a threat manner with low systemic adverse effects. In hormone-dependent breast cancer | [134] |
| Tamoxifen citrate (Transferrin targeted) | Hot emulsification method | Tamoxifen citrate increased targeting affinity towards breast cancer cells MCF-7 substantiated the developed SLN’s potential for breast cancer treatment. In ER+ breast cancers | [135] |
| Docetaxel | High-energy method | PS and PDI were 128 nm and 0.2 with a negative zeta potential with 86% encapsulation, 2% drug loading, and a regulated drug-release profile. In vivo investigations revealed that SLN-DTX had a greater anticancer activity by decreasing tumor volume. In Metastatic breast cancer | [136] |
| Docetaxel palmitate (DTX-PL) | Micro-emulsification technique | Oral bioavailability is improved, with a long biological half-life. The increased cytotoxicity in MDR cancer cells supports the promise of the novel lipophilic compound, which has improved the drug’s overall performance. In TNBC | [137] |
| Gefitinib | Modified hot homogenization method | SLNs were nanosized (90 percent) within 72 h, according to SEM images. The Higuchi model matches the kinetic analyses of GFT-SLNs (R2 = 0.935). The Higuchi model matches the kinetic analyses of GFT-SLNs (R2 = 0.935). In vitro assays of SLN showed significantly stronger antitumor activity (cell survival >65%) than free drug (p < 0.05). It has a high antitumor activity as well as improved drug dispersion in tissues. | [138] |
| Annona muricata fruit extract | High-pressure homogenization followed by ultrasonication method. | PS and percent EE were reported to be 134.8 nm and 83.26%, with a CDR of 79.83% after 48 h. It had an apoptotic impact and was more effective in killing MCF7 cancer cells. | [139] |
| Doxorubicin An arginine-glycine-aspartic (RGD) tripeptide modified, pH-sensitive (RGD-DOX-SLNs) | Emulsification and low-temperature solidification method | AUC –time curve was 5.58 times higher. T1/2 and Cmax were 10.85 h and 39.12 L/kg/h. in vitro and in vivo revealed that RGD-DOX-SLNs could be a potential new lipid carrier that might enhance breast cancer therapy. In Metastatic breast cancer | [140] |
| Curcumin | Emulsification evaporation-low temperature solidification method | Drug loading and encapsulation efficiency in SLNs were 23.38% and 72.47%. Greater cytotoxicity against SKBR3 cells. In an in vitro cellular uptake study, it found to have good absorption efficiency by SKBR3 cells. Cur-SLNs also produced higher apoptosis in SKBR3 cells. Decreased the manifestation of cyclin D1 and CDK4. These data suggest that Cur-SLNs might be a promising chemotherapeutic formulation for breast cancer therapy. | [141] |
| Pomegranate extract | Hot homogenization followed by the ultra-sonication technique | Improves bioefficacy, especially in MCF-7 breast cancer cells, where the IC50 was lowered by 47-fold from 49.2 to 1.05 g/mL and it has cytotoxicity in cancer cells vs normal cells Pomegranate extract has promising agent, especially for breast cancer. In Metastatic breast cancer | [142] |
| Talazoparib | Hot homogenization method | Talazoparib SLNs are more effective than talazoparib at suppressing MDR1, BCRP, and MRP1 genes and protein expression levels. Reverse MDR-mediated resistance in TNBC. | [143] |
| Resveratrol | Emulsification and low-temperature solidification method. | Res-SLNs were shown to be more effective at stopping MDA-MB-231 cells from proliferating andhad a considerably higher inhibitory impact on MDA-MB-231 cell invasion and migration. Res-SLNs increased the ratio Bax/Bcl-2 but lowered the expression of cyclinD1 and c-Myc, according to Western blot examination. Res–SLN has a lot of potential as a breast cancer therapy. | [131] |
| Lipid | Surfactant and Co-Surfactant | ||
|---|---|---|---|
| Solid Lipid | Liquid Lipid | ||
| Mixtues of mono, di andtriglycerides | Monoglycerides: Caprylate triglyceride, Caprate triglyceride, Glyceryl and tribehenate/Tribehenin. Diglycerides: Glyceryl palmitostearate and Glyceryl dibehenate. Triglycerides: Caprylate triglyceride, Caprate triglyceride, Glyceryl and tribehenate/Tribehenin. | Soya bean oil Oleic acid Medium chain triglycerides (MCT) caprylic- and capric triglycerides, αtocopherol Vitamin E Squalene Hydroxyoctacosanylhydroxystearate, Transcutol and Isopropyl myristate. | Poloxamer 188 Poloxamer 407 Soyabean phosphatidylcholin, Lecithin Tween 80 Cremophor® RH40, Sodium taurodeoxycholate, Sodium oleate Sodium dodecyl sulphure Butanol, Butyric acid |
| Waxes | Cetyl Palmitate, Carnauba, and wax Beeswax. | ||
| Fatty acids | Dodecanoic acid, Myristic acid, Palmitic acid and Stearic acid | ||
| Nanocarrier | Method of preparation | Interventions | Reference |
|---|---|---|---|
| Cabazitaxel (CBZ-loaded NLCs) | Hot homogenization method | NLCs containing CBZ induced a 6- and 2.5-fold increase in cytotoxicity, as well as an increase in apoptosis. In vitro cell culture assays, MDA-MB-468 and MCF-7 cells had reduced motility. In cells, NLC absorption was 2.5 to 2.1 times that of CBZ alone. For tumors that are resistant to drugs. | [151] |
| Luteolin (LTN)-encapsulated chitosan (CS) (LTN-CS-NLCs) | Melt emulsification ultrasonication technique | Mucoadhesion, gastro-intestinal stability, and intestinal penetration were all significantly improved in LTN-CS-NLCs. MDA-MB-231 and MCF-7 cells showed improved antioxidant activity as well as dose and time-dependent cytotoxicity. LTN-NLCs coated with chitosan show a lot of potential in the treatment of Breast cancer. | [152] |
| NLC loaded with Imatinib (NANIMA) | Hot homogenization method | The particle size of 104.63 ± 9.55 d.nm, PDI of 0.227 ± 0.06, and EE of 99.79 ± 0.03 and was sustained released. In cytotoxicity experiments on MCF-7 breast cancer cells, optimum NANIMA (IC50 = 6 M) was shown to be 8.75 times more effective than IMA alone (IC50 = 52.5 M). For the treatment of breast cancer, a lower dose of IMA-rich NLC will suffice rather than IMA alone. Furthermore, NANIMA has less adverse effects than IMA alone, leading in a satisfactory therapeutic outcome in the treatment of breast cancer. | [153] |
| Raloxifene | Ultrasonication method | In vitro, the RLN-NLCs were more cytotoxic to MCF-7 cells than the RLN solution. An ex vivo intestinal systemic absorption analysis revealed that the RLN-NLCs had better intestinal permeability. When RLN-NLCs were compared to RLN solution in an in vivo pharmacokinetic investigation in female Wistar rats, the oral bioavailability of RLN from RLN-NLCs increased 4.79-fold. One of the paths for a novel nanotherapeutic approach to the treatment of Breast cancer. | [154] |
| Curcumin-Loaded Magnetic Lipid Nanoparticles (CUR-NLC-SPIONs) | SPIONs by co-precipitation followed by CUR-NLC-SPIONs by homogenization technique | The average PS was 166.7 ± 14.20 nm, with a mean ZP- −27.6 ± 3.83 mv, PDI of 0.24 ± 0.14, EE was 99.95 ± 0.015%, and drug-loading capacity was 3.76 ± 0.005%. CUR-NLC-SPIONs had a more substantial cytotoxic effect against human breast cancer cells than free CUR. This new drug delivery technology, which uses superparamagnetic properties, might be utilized to create new biocompatible drug carriers and tailored cancer therapies. | [155] |
| Curcumin | High shear hot homogenization method | The small mean PS, spherical shape and negative ZP of NLCs assisted their internalization into cells. By regulating and suppressing P-gp expression, glyceryl monooleate enhanced the cytotoxic effects of CUR. | [156] |
| Docetaxel-loaded NLCs functionalized with trastuzumab (Herceptin) | Solvent extraction technique followed by probe sonication. | DTX added in chemically connected NLCs to Herceptin had more cytotoxic effects than physically coated nanoparticles. The Herceptin conjugated NLCs seem to have the potential for delivering DTX to HER2-positive breast cancer cells in a targeted way. | [157] |
| Combinatorial Approach | Nanocarrier | Interventions | Reference |
|---|---|---|---|
| DOX & Acridine orange (AO) | Gold core silica shell (AuMSS) nanosphere | AuMSS nanospheres have particle size of 192.6 ± 2.9 nm. AuMSS nanoparticles functionalization with the PANIS silane derivatives (TPANIS) promoted a slight increase in the nanoparticles size and colloidal stability. Additionally, both the DOX and AO were successfully encapsulated on the AuMSS-TPANIS nanospheres. Moreover, the AuMSS nanospheres functionalization with TPANIS significantly increased their internalization by MCF-7 cells resulting in an enhanced cytotoxic effect. | [165] |
| DOX and Crocin (carotenoid) | PLGA nanoparticles (PDCR NPs) | The PDCR NPs had a particle size of 174.2 ± 1.57 nm and showed a sustained and controlled release pattern. PDCR NPs cause apoptosis in breast cancer cells by reducing reactive oxygen species (ROS) and altering mitochondrial potential, resulting in cell-cycle arrest in the G2/M phase and death. In tumor-induced animal investigations, PDCR NPs showed decreased tumor volume when compared to control groups. In vitro and in vivo, the co-delivery of natural anticancer bioactive crocin with doxorubicin in PDCR NPs presents a feasible controlled-release nanoplatform for effective drug administration. | [166] |
| Tamoxifen (TAM) and sulforaphane (SFN) | TAM-SFN NLCs | TAM-SFN-NLCs exhibited a particle size of 121.9 ± 6.42 nm and zeta potential of −21.2 ± 2.91 mV. Oral bioavailability is improved. In vivo study revealed that SFN significantly reduced TAM-related toxicity. | [167] |
| Stearic acid loaded with capsaicin | SLNs | Synthesized SLNs were predominantly spherical, 80 nm diameter particles that proved to be biocompatible with good stability in aqueous conditions.In vivo biodistribution showed that 48h. The IC50 of capsaicin-loaded SLNs in HepG2 cells in vitrowas 21.36 μg× mL−1 and enhanced anticancer activity. | [168] |
| Variabilin Loaded Stearic Acid (Var-SLNs) | SLNs | Var-SLNs triggered apoptosis in HT-29, MCF-7, and PC-3 cells at rates of 47 percent (vs. 38% for variabilin), 48 percent (vs. 29% for variabilin), and 59% (vs. 29% for variabilin). An average size of 83.5 nm. Both variabilin and Var-SLN revealed comparable activity to Ceramide against the MCF-7 breast cancer cell line, revealing IC50 values of 34.8, 38.1 and 33.6 μM for variabilin, Var-SLN and Ceramide, respectively. Encapsulation into SLNs also has a “protective effect” on the non-tumorigenic epithelial cell line (MCF12A). Incorporating unstable or poorly soluble medicines into SLNs might save molecules that were previously thought to be druggable owing to poor physicochemical properties. | [169] |
| Epigallocatechin-gallate (EGCG) with Bombesin | SLNs | The bombesin-conjugated nanoparticles (EB-SLN) had a diameter of 163.4 ± 3.2 nm. IC50 values for EGCG, EGCG-SLN and EB-SLN in MDA-MB-231 were 65.4 ± 4.9 μg/mL, 6.9 ± 1.1 μg/mL and 3.2 ± 1.7 μg/mL, Similarly, these formulations were also more effective against B16F10 cells with IC50 values for EGCG, EGCG-SLN and EB-SLN found to be 59.3 ± 6.4 μg/mL,28.2 ± 1.9 μg/mL and 15.6 ± 1.3 μg/mL, respectively. It revealed that peptide-conjugated formulations had higher cytotoxicity against cancer cell lines than non-conjugated formulations. Furthermore, in-vivo investigations on C57/BL6 mice revealed that animals treated with the compound had a higher survival rate and had a smaller tumor volume. These findings support the system’s promise as a unique and effective drug delivery mechanism in breast cancer treatment. | [170] |
| DOX + CUR | Micelle | DOX + CUR-Micelles showed a consistent particle size, strong encapsulation effectiveness, a long-term release profile, and good colloidal stability. DOX + CUR-Micelles had the greatest cytotoxicity and cell apoptosis-inducing properties against DOX-resistant MCF-7/Adr cells in an in vitro cytotoxicity investigation. Furthermore, DOX + CUR-Micelles increased the cellular absorption of DOX through energy-dependent and caveolae-mediated endocytosis, and dramatically reversed MDR effects via CD44 targeted delivery and the synergic action of released CUR. In vivo data showed that DOX + CUR-Micelles not only had superior tumour accumulation and tumour targeting, and more effectively reduced tumour development in 4T1 tumor-bearing mice. In conclusion, this targeted combinational micellar delivery system including DOX and CUR might be a viable tumour therapeutic vehicle. | [171] |
| CUR and paclitaxel | PEGylated lipid bilayer coated mesoporous silica nanoparticles (PLMSNs) | MSNs with pore diameter of 2.754 nm and particle size of 115 ± 15 nm. In vitro release tests revealed that PLMSNs enhanced PTX dissolution when compared to PTX powder suspension and had a longer release time. PTX-CUR-PLMSNs showed a definite and long-lasting cytotoxic impact on canine breast cancer cells. This increased and extended activity of PTX-CUR-PLMSNs may contribute to the impact of sustained release. | [172] |
| Micelle | The obtained IC50 values of the mPEG-PBLA-PVIm triblock copolymer (PPBV). Micelles/PTX + CUR at pH 6.5 were 0.47 mg/mL (PTX) and 1.22 mg/mL (CUR), respectively. Tumor growth inhibition with no substantial recurrence. Furthermore, systemic administration of PPBV micelles/PTX+ CUR exhibited superior tumor inhibition activity and bCSCs-killing capacity in vivo. Consequently, collaborative therapy of PTX and CUR using pH multistage responsive PPBV micelles could be a potential strategy for inhibiting breast tumor growth by simultaneously eliminating bCSCs and non-CSCs. | [173] | |
| Nanoliposomes (CL-APNs) | The particle size of CL-APNs was found to be 252.13 ± 5.055nm. In vitro, drug-loaded nanoliposomes have a sustained drug release profile and relative ratio of migration was 37.64 ± 10.23 in B16F10 cells and 42.91 ± 9.54 in MCF-7 cells, the CL-APN remarkably inhibited cell migration compared to any other group in both the cell lines. The results of the cell migration assay were consistent with the cytotoxicity assay results and CL-APN could be potentially used in the treatment of multiple tumor malignancies. | [174] | |
| Folate (FA) and CUR | NLCs | FA-CUR-NLCs formulations exhibited small particle size of 127 nm. The IC50 (μmol/l) value of FA-CUR-NLCs (1.75 ± 0.29) was over 3.5-fold over CUR-NLCs (6.16 ± 0.67) in reducing viability of breast cancer cells, accounting for the highest anti-tumor activity. The effect of FA targeting and delivery ability of this NLCs formulation might be an effective tumor therapy strategy for treatment in breast carcinoma. | [150] |
| Kaempferol (KAE) and paclitaxel | NLCs | Particle size of 80 ± 3 nm for Kaempferol formulated into NLCs. The IC50 values for KAE and paclitaxel determined 44 ± 0.52 μM and 1.75 ± 0.36 nM, respectively. The moderated cell proliferation from 56 ± 26.8% to 44 ± 3.9% (p< 0.05) was demonstrated by KAE loaded NLCs. Paclitaxel cytotoxicity against MDA-MB 468 mice Breast cancer cells was increased by KAE-loaded NLCs. Synergistic anticancer activity was achieved by blocking apoptotic signaling and suppressing cancer cell cycle arrest in Sub G1 arrest, as well as down regulating anti-apoptotic Bcl-2 family gene levels. | [175] |
| β-lapachone plus DOX (LDNLC) | NLCs | The size distribution of LDNLC was approximately 100 nm with narrow distribution range, which was reflected by its relatively small PDI of 0.123 (<0.3). Compared to DOX mono-delivery NLC, in vitro cell studies in MCF-7 ADR cells revealed enhanced DOX retention (DNLC). In vivo anti-cancer studies on MCF-7 ADR tumor-bearing mice also demonstrated that LDNLC was substantially more effective than mono-delivery NLCs (DNLC and LNLC). The IC50 for MCF-7 ADR cells for LDNLC was calculated as 7.26 μM with a combination index of 0.31, thus indicating a remarkable synergism in the drug-resistant strain and could be a potential platform for overcoming MDR. | [176] |
| Quercetin and DOX | Biotin receptor-targeting nanoparticles (BNDQ) | Particle size of BNDQ were found to be 105.8 ± 1.4 nm and DOX tolerance in MCF-7/ADR cancer cells is reduced in vitro and in vivo. Quercetin decreased both the activity and the expression of P-gp in MCF-7/ADR cells could be a potential platform for overcoming MDR and It was found that the IC50 of BNDQ was 0.17 μg/mL significantly enhanced by the presence of free biotin compared to that in the absence of biotin in both MCF-7 and MCF-7/ADR cells. | [177] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tagde, P.; Najda, A.; Nagpal, K.; Kulkarni, G.T.; Shah, M.; Ullah, O.; Balant, S.; Rahman, M.H. Nanomedicine-Based Delivery Strategies for Breast Cancer Treatment and Management. Int. J. Mol. Sci. 2022, 23, 2856. https://doi.org/10.3390/ijms23052856
Tagde P, Najda A, Nagpal K, Kulkarni GT, Shah M, Ullah O, Balant S, Rahman MH. Nanomedicine-Based Delivery Strategies for Breast Cancer Treatment and Management. International Journal of Molecular Sciences. 2022; 23(5):2856. https://doi.org/10.3390/ijms23052856
Chicago/Turabian StyleTagde, Priti, Agnieszka Najda, Kalpana Nagpal, Giriraj T. Kulkarni, Muddaser Shah, Obaid Ullah, Sebastian Balant, and Md. Habibur Rahman. 2022. "Nanomedicine-Based Delivery Strategies for Breast Cancer Treatment and Management" International Journal of Molecular Sciences 23, no. 5: 2856. https://doi.org/10.3390/ijms23052856
APA StyleTagde, P., Najda, A., Nagpal, K., Kulkarni, G. T., Shah, M., Ullah, O., Balant, S., & Rahman, M. H. (2022). Nanomedicine-Based Delivery Strategies for Breast Cancer Treatment and Management. International Journal of Molecular Sciences, 23(5), 2856. https://doi.org/10.3390/ijms23052856