
Circulating Levels of Ferritin, RDW, PTLs as Predictive Biomarkers of Postoperative Atrial Fibrillation Risk after Cardiac Surgery in Extracorporeal Circulation


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Postoperative Monitoring
2.3. Electrocardiographic and Echocardiographic Parameters in the Groups 0 and 1
2.4. Laboratory Analysis
2.5. Statistical Analysis
3. Results
3.1. Demographic and Basal Clinical Characteristics of Patients Enrolled in the Study
3.2. Evaluation of Circulating Ferritin Levels and Other Haemato-Chemical Biomarkers in POAF vs. No POAF Cases
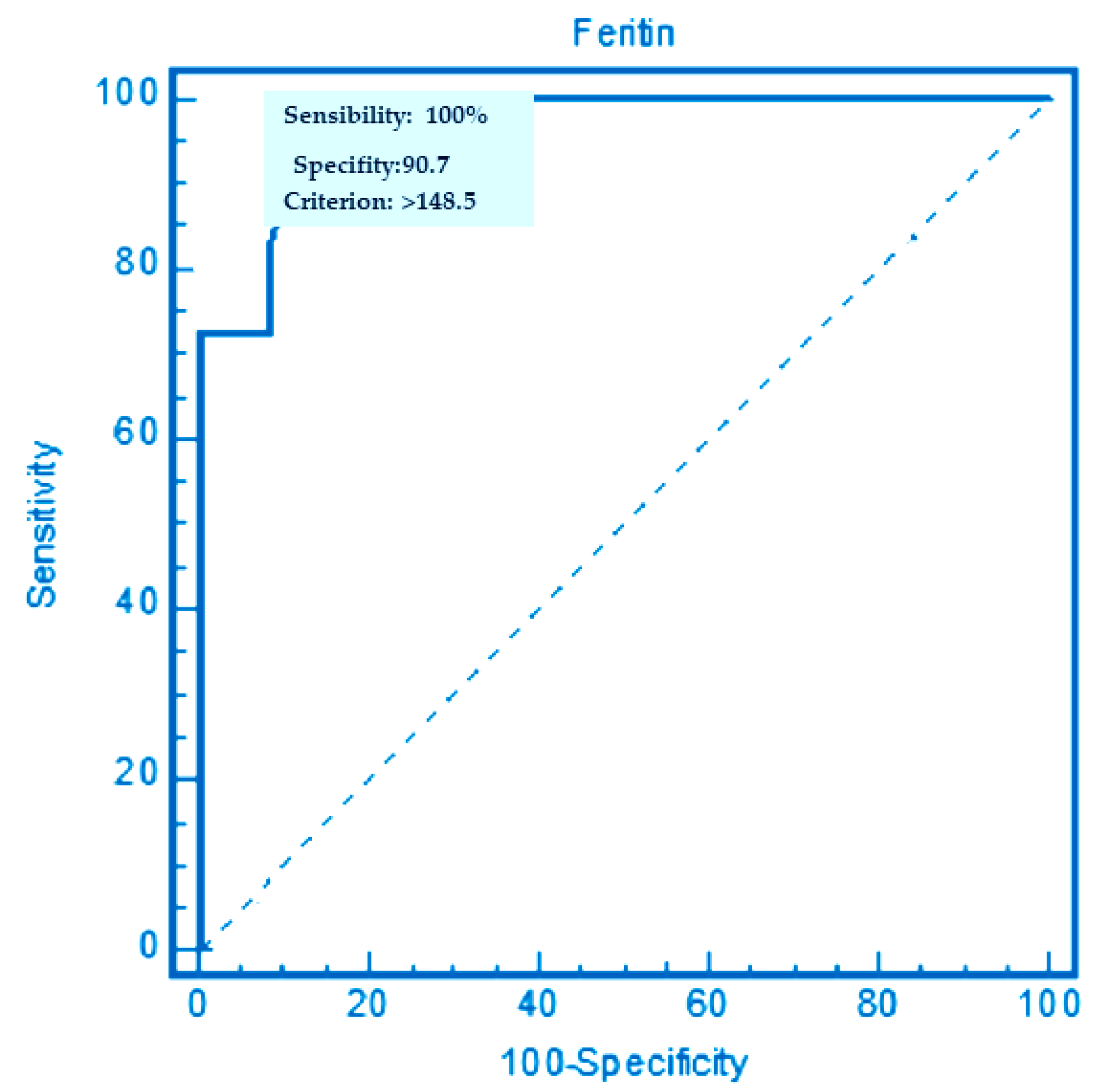
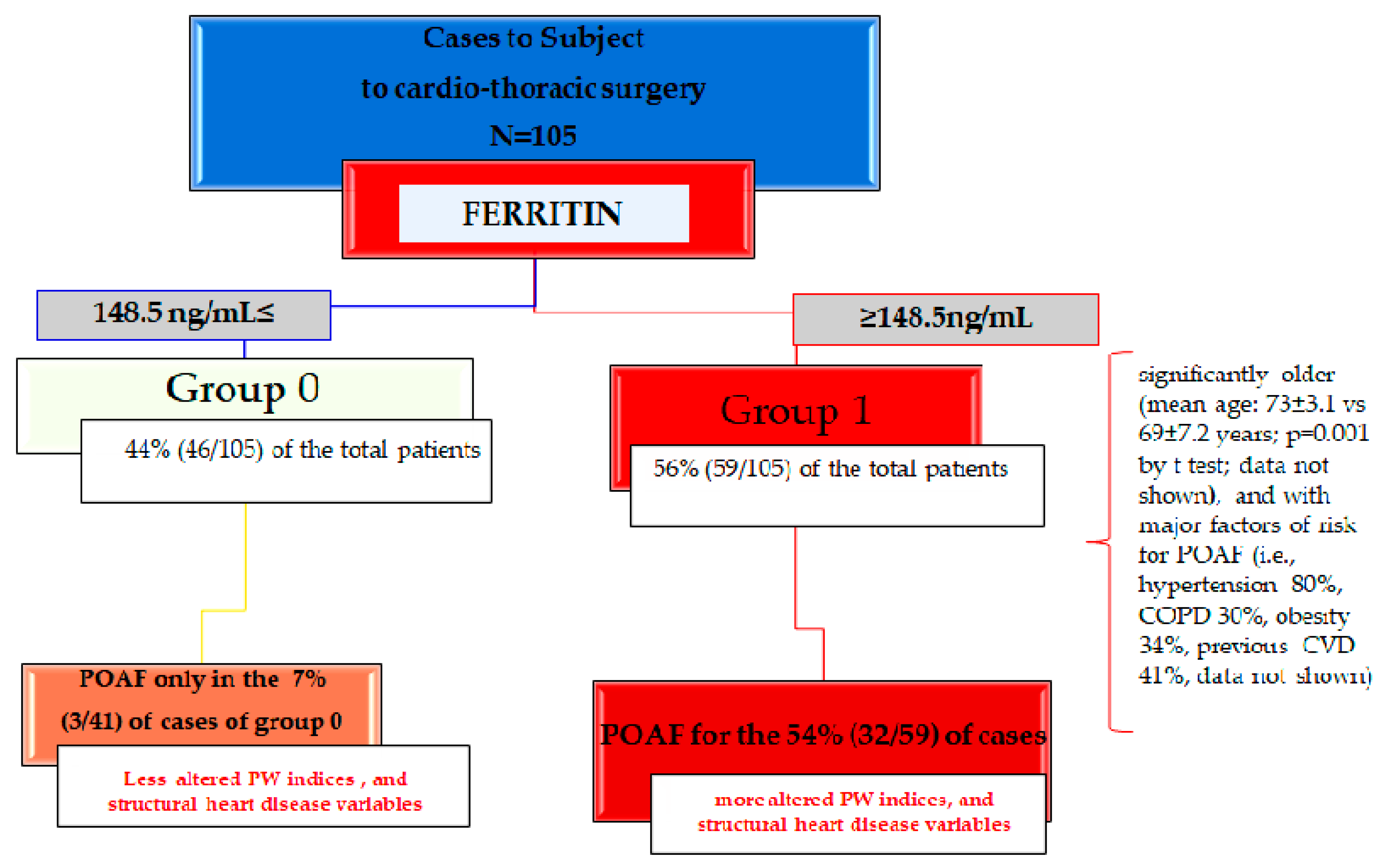
3.3. Cut-Off Values of Mean Serun Ferritin Levels for Predicting the Occurrence of POAF in the 105 Patients Enrolled
3.4. Major Prevalence of Risk POAF Factors in the Group 1 vs. Group 0
3.5. Significant Correlation between PWd, P-min, and P-max with Mean Serum Ferritin Levels and the Percentage of RDW in the Case Group 1 vs. Group 0
3.6. The Association of PW Indices with Structural Heart Disease Variables in the Group 1 after Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dobrev, D.; Aguilar, M.; Heijman, J.; Guichard, J.-B.; Nattel, S. Postoperative atrial fibrillation: Mechanisms, manifestations and management. Nat. Rev. Cardiol. 2019, 16, 417–436. [Google Scholar] [CrossRef] [PubMed]
- Tzoumas, A.; Nagraj, S.; Tasoudis, P.; Arfaras-Melainis, A.; Palaiodimos, L.; Kokkinidis, D.G.; Kampaktsis, P.N. Atrial Fibrillation Following Coronary Artery Bypass Graft: Where Do We Stand? Cardiovasc. Revasc. Med. 2021, 40, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Bessissow, A.; Khan, J.; Devereaux, P.; Alvarez-Garcia, J.; Alonso-Coello, P. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: An overview. J. Thromb. Haemost. 2015, 13 (Suppl. 1), S304–S312. [Google Scholar] [CrossRef] [PubMed]
- Helgadottir, S.; Sigurdsson, M.I.; Ingvarsdottir, I.L.; Arnar, D.O.; Gudbjartsson, T. Atrial fibrillation following cardiac surgery: Risk analysis and long-term survival. J. Cardiothorac. Surg. 2012, 7, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Quon, M.J.; Behlouli, H.; Pilote, L. Anticoagulant Use and Risk of Ischemic Stroke and Bleeding in Patients With Secondary Atrial Fibrillation Associated With Acute Coronary Syndromes, Acute Pulmonary Disease, or Sepsis. JACC Clin. Electrophysiol. 2018, 4, 386–393. [Google Scholar] [CrossRef]
- Lubitz, S.A.; Yin, X.; Rienstra, M.; Schnabel, R.B.; Walkey, A.; Magnani, J.W.; Rahman, F.; McManus, D.D.; Tadros, T.M.; Levy, D.; et al. Long-Term Outcomes of Secondary Atrial Fibrillation in the Community. Circulation 2015, 131, 1648–1655. [Google Scholar] [CrossRef] [Green Version]
- Ghurram, A.; Krishna, N.; Bhaskaran, R.; Kumaraswamy, N.; Jayant, A.; Varma, P.K. Patients who develop post-operative atrial fibrillation have reduced survival after off-pump coronary artery bypass grafting. Indian J. Thorac. Cardiovasc. Surg. 2020, 36, 6–13. [Google Scholar] [CrossRef]
- Greenberg, J.W.; Lancaster, T.; Schuessler, R.B.; Melby, S.J. Postoperative atrial fibrillation following cardiac surgery: A persistent complication. Eur. J. Cardio-Thorac. Surg. 2017, 52, 665–672. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, Y.; Peighambari, M.M.; Naghshbandi, S.; Samiei, N.; Ghavidel, A.A.; Dehghani, M.R.; Haghjoo, M.; Hosseini, S. Postoperative Atrial Fibrillation Following Cardiac Surgery: From Pathogenesis to Potential Therapies. Am. J. Cardiovasc. Drugs 2020, 20, 19–49. [Google Scholar] [CrossRef]
- Korkmaz, U.; Ucaroglu, E. Aortic knob width as a novel predictor of postoperative atrial fibrillation following off-pump coronary artery bypass grafting. Med. Sci. 2021, 10, 1145. [Google Scholar] [CrossRef]
- Gaudino, M.; Andreotti, F.; Zamparelli, R.; Di Castelnuovo, A.; Nasso, G.; Burzotta, F.; Iacoviello, L.; Donati, M.B.; Schiavello, R.; Maseri, A.; et al. The −174G/C Interleukin-6 Polymorphism Influences Postoperative Interleukin-6 Levels and Postoperative Atrial Fibrillation. Is Atrial Fibrillation an Inflammatory Complication? Circulation 2003, 108 (Suppl. 1), II195-9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hak, Ł.; Myśliwska, J.; Wieckiewicz, J.; Szyndler, K.; Siebert, J.; Rogowski, J. Interleukin-2 as a Predictor of Early Postoperative Atrial Fibrillation After Cardiopulmonary Bypass Graft (CABG). J. Interf. Cytokine Res. 2009, 29, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Girerd, N.; Pibarot, P.; Fournier, D.; Daleau, P.; Voisine, P.; O’Hara, G.; Després, J.-P.; Mathieu, P. Middle-aged men with increased waist circumference and elevated C-reactive protein level are at higher risk for postoperative atrial fibrillation following coronary artery bypass grafting surgery. Eur. Heart J. 2009, 30, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Jacob, K.A.; Nathoe, H.M.; Dieleman, J.; van Osch, D.; Kluin, J.; Van Dijk, D. Inflammation in new-onset atrial fibrillation after cardiac surgery: A systematic review. Eur. J. Clin. Investig. 2014, 44, 402–428. [Google Scholar] [CrossRef] [Green Version]
- Iscan, S.; Eygi, B.; Besir, Y.; Yurekli, I.; Cakir, H.; Yilik, L.; Gokalp, O.; Gurbuz, A. Inflammation, Atrial Fibrillation and Cardiac Surgery: Current Medical and Invasive Approaches for the Treatment of Atrial Fibrillation. Curr. Pharm. Des. 2018, 24, 310–322. [Google Scholar] [CrossRef]
- Topal, D.; Korkmaz, U.T.K.; Velioglu, Y.; Yuksel, A.; Donmez, I.; Uçaroğlu, E.R.; Kayis, S.A. Systemic immune-inflammation index as a novel predictor of atrial fibrillation after off-pump coronary artery bypass grafting. Rev. Assoc. Med. Bras. 2022, 68, 1240–1246. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Kelesoglu, S.; Elcik, D.; Ozmen, R.; Kalay, N. Predictive Values of Systemic Immune-Inflammation Index in New-Onset Atrial Fibrillation Following Coronary Artery Bypass Grafting. Braz. J. Cardiovasc. Surg. 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Cacoub, P.; Choukroun, G.; Cohen-Solal, A.; Luporsi, E.; Peyrin-Biroulet, L.; Peoc’H, K.; Andrieu, V.; Lasocki, S.; Puy, H.; Trochu, J. Iron deficiency screening is a key issue in chronic inflammatory diseases: A call to action. J. Intern. Med. 2022, 292, 542–556. [Google Scholar] [CrossRef]
- Mikkelsen, L.F.; Nordestgaard, B.G.; Schnohr, P.; Ellervik, C. Increased Ferritin Concentration and Risk of Atrial Fibrillation and Heart Failure in Men and Women: Three Studies of the Danish General Population Including 35,799 Individuals. Clin. Chem. 2019, 65, 180–188. [Google Scholar] [CrossRef]
- Sokal, A.; Wójcik, S.; Pruszkowska, P.; Kowalski, O.; Lenarczyk, R.; Liberska, A.; Mazurek, M.; Pluta, S.; Kalarus, Z. Ferritin as a potential biomarker of efficacy of treatment of atrial fibrillation—Preliminary report. Postepy. Hig. Med. Dosw. 2017, 71, 876–880. [Google Scholar] [CrossRef]
- Chen, L.Y.; Ribeiro, A.L.P.; Platonov, P.G.; Cygankiewicz, I.; Soliman, E.Z.; Gorenek, B.; Ikeda, T.; Vassilikos, V.P.; Steinberg, J.S.; Varma, N.; et al. P Wave Parameters, and Indices: A Critical Appraisal of Clinical Utility, Challenges, and Future Research-A Consensus Document Endorsed by the International Society of Electrocardiology and the International Society for Holter and Noninvasive Electrocardiology. Circ. Arrhythm. Electrophysiol. 2022, 15, e010435. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.; Tse, G.; Martinez-Selles, M.; Baranchuk, A. Atrial Conduction Disorders. Curr. Cardiol. Rev. 2021, 17, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, A.; Hung, C.-L.; Claggett, B.; Nochioka, K.; Cheng, S.; Kitzman, D.W.; Shah, A.M.; Solomon, S.D. Left Atrial Structure and Function Across the Spectrum of Cardiovascular Risk in the Elderly: The Atherosclerosis Risk in Communities study. Circ. Cardiovasc. Imaging 2016, 9, e004010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.M.; Cheng, S.; Skali, H.; Wu, J.; Mangion, J.R.; Kitzman, D.; Matsushita, K.; Konety, S.; Butler, K.R.; Fox, E.R.; et al. Rationale and Design of a Multicenter Echocardiographic Study to Assess the Relationship Between Cardiac Structure and Function and Heart Failure Risk in a Biracial Cohort of Community-Dwelling Elderly Persons: The Atherosclerosis Risk in Communities study. Circ. Cardiovasc. Imaging 2014, 7, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetz, L.H.; Schork, N.J. Personalized medicine: Motivation, challenges, and progress. Fertil. Steril. 2018, 109, 952–963. [Google Scholar] [CrossRef] [PubMed]
- Balistreri, C.R. Promising Strategies for Preserving Adult Endothelium Health and Reversing Its Dysfunction: From Liquid Biopsy to New Omics Technologies and Noninvasive Circulating Biomarkers. Int. J. Mol. Sci. 2022, 23, 7548. [Google Scholar] [CrossRef]
- Malesza, I.J.; Bartkowiak-Wieczorek, J.; Winkler-Galicki, J.; Nowicka, A.; Dzięciołowska, D.; Błaszczyk, M.; Gajniak, P.; Słowińska, K.; Niepolski, L.; Walkowiak, J.; et al. The Dark Side of Iron: The Relationship between Iron, Inflammation and Gut Microbiota in Selected Diseases Associated with Iron Deficiency Anaemia—A Narrative Review. Nutrients 2022, 14, 3478. [Google Scholar] [CrossRef]
- Savarese, G.; von Haehling, S.; Butler, J.; Cleland, J.G.; Ponikowski, P.; Anker, S.D. Iron deficiency and cardiovascular disease. Eur. Heart J. 2022; ehac569, Epub ahead of print. [Google Scholar] [CrossRef]
- Chen, Y.; Guo, T.L. Dietary advanced glycation end-products elicit toxicological effects by disrupting gut microbiome and immune homeostasis. J. Immunotoxicol. 2021, 18, 93–104. [Google Scholar] [CrossRef]
- Adamsson Eryd, S.; Borné, Y.; Melander, O.; Persson, M.; Smith, J.G.; Hedblad, B.; Engström, G. Red blood cell distribution width is associated with incidence of atrial fibrillation. J. Intern. Med. 2014, 275, 84–92. [Google Scholar] [CrossRef]
- Gurses, K.M.; Yalcin, M.U.; Kocyigit, D.; Evranos, B.; Ates, A.H.; Yorgun, H.; Sahiner, M.L.; Kaya, E.B.; Ozer, N.; Oto, M.A.; et al. Red blood cell distribution width predicts outcome of cryoballoon--based atrial fibrillation ablation. J. Interv. Card. Electrophysiol. 2015, 42, 51–58. [Google Scholar] [CrossRef]
- Poz, D.; De Falco, E.; Pisano, C.; Madonna, R.; Ferdinandy, P.; Balistreri, C.R. Diagnostic and Prognostic Relevance of Red Blood Cell Distribution Width for Vascular Aging and Cardiovascular Diseases. Rejuvenation Res. 2019, 22, 146–162. [Google Scholar] [CrossRef] [PubMed]
- Balistreri, C.R.; Pisano, C.; Bertoldo, F.; Massoud, R.; Dolci, S.; Ruvolo, G. Red Blood Cell Distribution Width, Vascular Aging Biomarkers, and Endothelial Progenitor Cells for Predicting Vascular Aging and Diagnosing/Prognosing Age-Related Degenerative Arterial Diseases. Rejuvenation Res. 2019, 22, 399–408. [Google Scholar] [CrossRef]
- Sayın, M.R.; Özderya, A.; Konuş, A.H.; Yerlikaya, M.G.; Maz, M.A.; Çırakoğlu, F.; Uzun, G.; Kara, F. The use of systemic immune-inflammation index to predict new onset atrial fibrillation in the context of acute coronary syndrome. Kardiologiia 2022, 62, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Guzelburc, O.; Zengin, A.; Karatas, M.B.; Erdogan, S.B.; Emre, A. Relationship between platelet mass index and postoperative atrial fibrillation after elective coronary artery bypass surgery: A retrospective study. Herz, 2022; 1–7, Epub ahead of print. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498, Erratum in: Eur. Heart J. 2021, 42, 507. Erratum in: Eur. Heart J. 2021, 42, 546–547. Erratum in: Eur. Heart J. 2021, 42, 4194. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, A.; Norby, F.L.; Roetker, N.S.; Soliman, E.Z.; Koene, R.J.; Rooney, M.R.; O’Neal, W.T.; Shah, A.M.; Claggett, B.L.; Solomon, S.D.; et al. Refining Prediction of Atrial Fibrillation–Related Stroke Using the P2-CHA2DS2-VASc Score. Circulation 2019, 139, 180–191. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall | Without POAF | With POAF | p-Value |
|---|---|---|---|---|
| N = 105 | N = 70 (67.0) | N = 35 (33.0) | ||
| Gender, n (%), n (%): | ||||
| F | 35 (33.0) | 21 (30.0) | 11 (31.0) | 0.79 † |
| M | 70 (67.0) | 49 (70.0) | 24 (69.0) | |
| Age (mean ± SD) | 70.1 ± 7.1 | 67 ± 6.8 | 73.3 ± 7.6 | 0.005 ^ |
| Body surface area (BSA), (mean ± SD) | 1.81 ± 4.8 | 1.82 ± 4.6 | 1.92 ± 4.8 | 0.44 ^ |
| HYPERTENSION, n (%), n (%): | 0.06 § | |||
| No | 18 (17.0) | 21(30.0) | 3 (9.6) | |
| YES | 87 (83.0) | 49 (70.0) | 32 (91.4) | |
| Smoking, n (%): | 0.84 † | |||
| Ex | 22 (21.0) | 14 (20.0) | 8 (23.0) | |
| No | 27 (26.0) | 18 (26.0) | 9 (26.0) | |
| YES | 56 (53.0) | 38 (54.0) | 18 (51.0) | |
| DIABETES, n (%): | 0.45 § | |||
| No | 82 (78.0) | 55 (78.0) | 27 (77.0) | |
| YES | 23 (22.0) | 15 (22.0) | 8 (23.0) | |
| DYSLIPIDEMIA, n (%): | 0.12 § | |||
| No | 73 (69.0) | 50 (71.0) | 23 (66.0) | |
| YES | 32 (31.0) | 20 (29.0) | 12 (34.0) | |
| Chronic obstructive pulmonary disease (COPD), n (%): | 0.001 § | |||
| No | 80 (78.0) | 63 (90.0) | 17 (48.5) | |
| YES | 25 (22.0) | 7 (10.0) | 18 (51.5) | |
| OBESITY, n (%): | 0.003 § | |||
| No | 73 (70.0) | 58 (83.0) | 15 (43.0) | |
| YES | 32 (30.0) | 12 (17.0) | 20 (57.0) | |
| Previous cardiovascular diseases (CVD), n (%): | 0.003 § | |||
| No | 73 (70.0) | 56 (80.0) | 17 (48.5) | |
| YES | 32 (30.0) | 14 (20.0) | 18 (51.5) | |
| Amiodarone., n (%): | 0.29 § | |||
| No | 87 (83.0) | 61 (87.0) | 26 (74.0) | |
| YES | 18 (17.0) | 9 (13.0) | 9 (26.0) | |
| ACE-INHIBITORS., n (%): | 0.497 † | |||
| No | 73 (70.0) | 45 (64.0) | 28 (80.0) | |
| YES | 32 (30.0) | 25 (36.0) | 7 (20.0) |
| Variables | Overall | Without POAF | With POAF | p-Value ^ (POAF Cases vs. Cases without POAF) |
|---|---|---|---|---|
| N = 105 | N = 70 | N = 35 | ||
| Hemoglobin, HB (g/dL) (mean ± SD) | 13.1 ± 4.2 | 12.8 ± 5.6 | 10.4 ± 3.6 | 0.024 |
| PLT 103/µL | 227.3 ± 1058 | 230 ± 5.7 | 251 ± 5.6 | <0.0001 |
| CREATININE (mg/dL) | 1.30 ± 7.2 | 0.97 ± 7.2 | 1.48 ± 8.2 | 0.36 |
| International normalized ratio (INR) | 1.12 ± 0.8 | 1.12 ± 2.9 | 1.21 ± 5.5 | 0.42 |
| Mg (mg/dL) | 2.11 ± 2.4 | 1.92 ± 1.9 | 1.9 ± 1.9 | 0.40 |
| K (mEq/L) | 4.28 ± 2.5 | 4.20 ± 2.5 | 4.18 ± 2.8 | 0.41 |
| RDW (%) | 13.9. ± 3.1 | 12.5 ± 3.5 | 16 ± 4.1 | 0.0003 |
| FERRITIN (ng/mL) | 216.2 ± 3.5 | 232.5 ± 6.2 | 286 ± 2.7 | <0.0001 |
| SIDERAEMIA | 82 ± 2.8 | 81 ± 3.2 | 75 ± 4.6 | 0.04 |
| Variables | Group 0 | Group 1 | p-Value ^ |
|---|---|---|---|
| Hemoglobin, HB (g/dL) (mean ± SD) | 13.5 ± 4.1 | 11.5 ± 2.6 | 0.01 |
| PLT 103/µL | 20 ± 4.9 | 24 ± 6.1 | <0.0001 |
| CREATININE (mg/dL) | 1.02 ± 5.6 | 1.14 ± 5.6 | 0.49 |
| International normalized ratio (INR) | 1.03 ± 1.5 | 1.11 ± 3.2 | 0.48 |
| Mg (mg/dL) | 1.83 ± 1.8 | 1.8 ± 4.1 | 0.48 |
| K (mEq/L) | 4.10 ± 1.5 | 4.08 ± 2.4 | 0.49 |
| RDW (%) | 13.2 ± 3.1 | 16.0 ± 4.2 | 0.04 |
| SIDERAEMIA | 86 ± 6.1 | 80 ± 3.1 | <0.0001 |
| Variables | Group 1 | Group 0 | ||||
|---|---|---|---|---|---|---|
| Mean serum ferritin | PWd | P-max | P-min | Pwd | P-max | P-min |
| Pearson correlation | 0.89 | 0.88 | 0.83 | 0.66 | 0.41 | 0.38 |
| p value | 0.0001 | 0.0001 | 0.0001 | 0.046 | 0.059 | 0.061 |
| RDW (%) | ||||||
| Pearson correlation | 0.79 | 0.77 | 0.71 | 0.51 | 0.40 | 0.37 |
| p value | 0.0002 | 0.0002 | 0.0002 | 0.06 | 0.06 | 0.07 |
| Structural Heart Disease Variables * | ||||
|---|---|---|---|---|
| Left atrial volume index >34 mL/m2 | PWd 1.49 (1.36–1.76) § | P-max 1.45 (1.29–1.74) § | P-min 1.29 (1.29–1.74) § | IAB 1.29 (1.29–1.74) § |
| Left ventricular mass index >115 g/m2 for men, >95 g/m2 for women | 1.61 (1.42–1.88) § | 1.09 (1.01–1.41) ‡ | 1.06 (1.74–2.43) ‡ | 1.02 (1.01–1.14) ‡ |
| Left ventricular end diastolic diameter >5.8 cm for men, >5.2 cm for women | 2.25 (1.65–3.22) § | 1.52 (1.24–2.18) § | 1.39 (1.24–2.08) § | 1.19 (1.01–1.64) § |
| Left ventricular ejection fraction <52% for men, <54% for female | 1.36 (1.16–1.69) § | 1.18 (1.05–1.27) ‡ | 1.12(1.10–1.34) ‡ | 0.29 (1.29–1.74) § |
| LAGLS %, difference (95% CI) | −1.59 (−2.33, −0.77) § | −1.19 (−1.86, −0.33)§ | −1.10 (−1.86, −0.33) § | −1.29 (1.29–1.74) § |
| LAEF %, difference (95% CI) | −2.79 (−3.29, −1.60) § | −1.17 (−3.01, −0.30) ‡ | −0.06 (−1.48, 1.32) | −1.97 (−4.85, 2.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altieri, C.; Pisano, C.; Vincenzo, L.; Ferrante, M.S.; Pellerito, V.; Nardi, P.; Bassano, C.; Buioni, D.; Greco, E.; Ruvolo, G.; et al. Circulating Levels of Ferritin, RDW, PTLs as Predictive Biomarkers of Postoperative Atrial Fibrillation Risk after Cardiac Surgery in Extracorporeal Circulation. Int. J. Mol. Sci. 2022, 23, 14800. https://doi.org/10.3390/ijms232314800
Altieri C, Pisano C, Vincenzo L, Ferrante MS, Pellerito V, Nardi P, Bassano C, Buioni D, Greco E, Ruvolo G, et al. Circulating Levels of Ferritin, RDW, PTLs as Predictive Biomarkers of Postoperative Atrial Fibrillation Risk after Cardiac Surgery in Extracorporeal Circulation. International Journal of Molecular Sciences. 2022; 23(23):14800. https://doi.org/10.3390/ijms232314800
Chicago/Turabian StyleAltieri, Claudia, Calogera Pisano, Labriola Vincenzo, Maria Sabrina Ferrante, Valentina Pellerito, Paolo Nardi, Carlo Bassano, Dario Buioni, Ernesto Greco, Giovanni Ruvolo, and et al. 2022. "Circulating Levels of Ferritin, RDW, PTLs as Predictive Biomarkers of Postoperative Atrial Fibrillation Risk after Cardiac Surgery in Extracorporeal Circulation" International Journal of Molecular Sciences 23, no. 23: 14800. https://doi.org/10.3390/ijms232314800
APA StyleAltieri, C., Pisano, C., Vincenzo, L., Ferrante, M. S., Pellerito, V., Nardi, P., Bassano, C., Buioni, D., Greco, E., Ruvolo, G., & Balistreri, C. R. (2022). Circulating Levels of Ferritin, RDW, PTLs as Predictive Biomarkers of Postoperative Atrial Fibrillation Risk after Cardiac Surgery in Extracorporeal Circulation. International Journal of Molecular Sciences, 23(23), 14800. https://doi.org/10.3390/ijms232314800