
Basophil Activation Test with Different Polyethylene Glycols in Patients with Suspected PEG Hypersensitivity Reactions

 ,
,  , ,
, ,  ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Skin Test Analyses
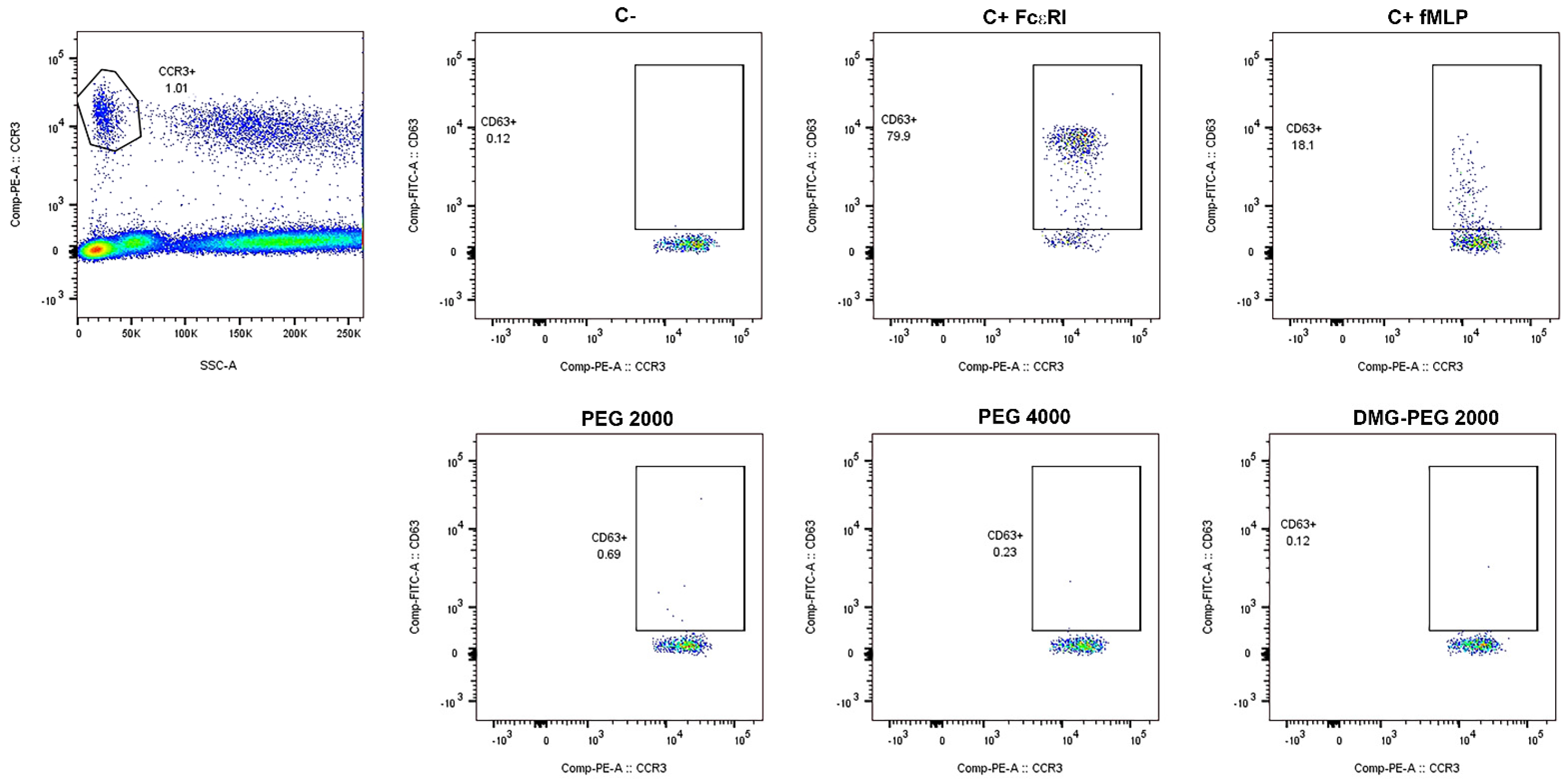
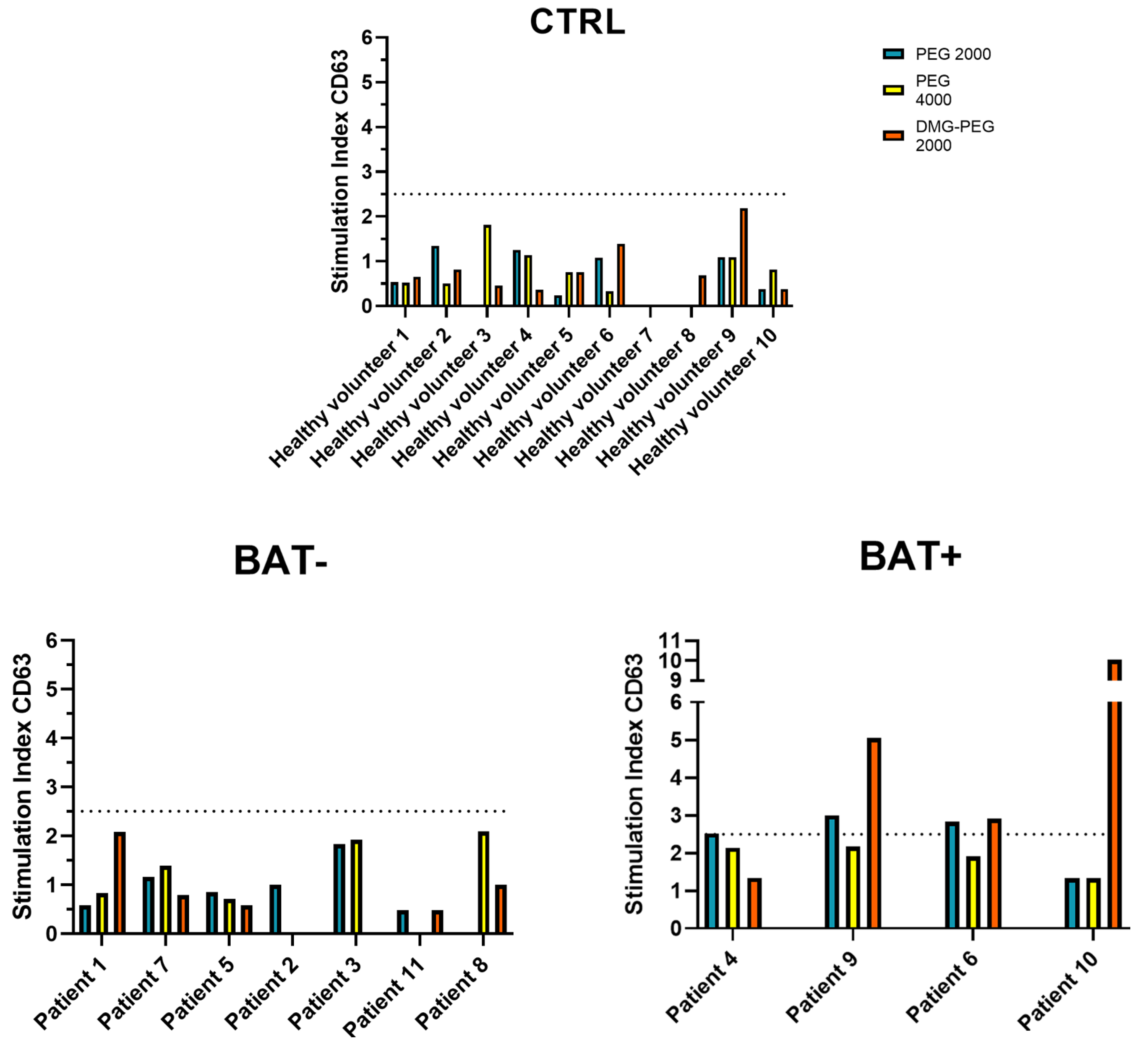
2.2. Basophil Activation Test Analyses
2.3. The Value of the Stimulation Index for the BAT Evaluation
2.4. Evaluation of Skin Test and BAT Analyses
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Skin Prick Tests and Intradermal Tests
4.3. Basophil Activation Test
4.4. Statistics
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sokolowska, M.; Lukasik, Z.M.; Agache, I.; Akdis, C.A.; Akdis, D.; Akdis, M.; Barcik, W.; Brough, H.A.; Eiwegger, T.; Eljaszewicz, A.; et al. Immunology of COVID-19: Mechanisms, Clinical Outcome, Diagnostics, and Perspectives—A Report of the European Academy of Allergy and Clinical Immunology (EAACI). Allergy 2020, 75, 2445–2476. [Google Scholar] [CrossRef]
- Castells, M.C.; Phillips, E.J. Maintaining Safety with SARS-CoV-2 Vaccines. N. Engl. J. Med. 2021, 384, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; Veen, W.; Brüggen, M.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune Response to SARS-CoV-2 and Mechanisms of Immunopathological Changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- Rossi, C.; Lanuti, P.; Cicalini, I.; De Bellis, D.; Pierdomenico, L.; Del Boccio, P.; Zucchelli, M.; Natale, L.; Sinjari, B.; Catitti, G.; et al. BNT162b2 MRNA Vaccination Leads to Long-Term Protection from COVID-19 Disease. Vaccines 2021, 9, 1164. [Google Scholar] [CrossRef] [PubMed]
- Lanuti, P.; Rossi, C.; Cicalini, I.; Pierdomenico, L.; Damiani, V.; Semeraro, D.; Verrocchio, S.; Del Boccio, P.; Evangelista, A.; Sarra, A.; et al. Picture of the Favourable Immune Profile Induced by Anti-SARS-CoV-2 Vaccination. Biomedicines 2021, 9, 1035. [Google Scholar] [CrossRef]
- Cicalini, I.; Rossi, C.; Natale, L.; Cufaro, M.C.; Catitti, G.; Vespa, S.; De Bellis, D.; Iannetti, G.; Lanuti, P.; Bucci, I.; et al. Passive Immunity to SARS-CoV-2 at Birth Induced by Vaccination in the First Trimester of Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 12789. [Google Scholar] [CrossRef] [PubMed]
- Vespa, S.; Simeone, P.; Catitti, G.; Buca, D.; De Bellis, D.; Pierdomenico, L.; Pieragostino, D.; Cicalini, I.; Del Boccio, P.; Natale, L.; et al. SARS-CoV-2 and Immunity: Natural Infection Compared with Vaccination. Int. J. Mol. Sci. 2022, 23, 8982. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Anastassopoulou, C.; Hatziantoniou, S.; Poland, G.A.; Tsakris, A. Anaphylaxis Rates Associated with COVID-19 Vaccines Are Comparable to Those of Other Vaccines. Vaccine 2022, 40, 183–186. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Robinson, L.B.; Camargo, C.A.; Shenoy, E.S.; Banerji, A.; Landman, A.B.; Wickner, P. Acute Allergic Reactions to MRNA COVID-19 Vaccines. JAMA 2021, 325, 1562. [Google Scholar] [CrossRef]
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and Allergic Reactions: The Past, the Current COVID-19 Pandemic, and Future Perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef]
- Wolfson, A.R.; Robinson, L.B.; Li, L.; McMahon, A.E.; Cogan, A.S.; Fu, X.; Wickner, P.; Samarakoon, U.; Saff, R.R.; Blumenthal, K.G.; et al. First-Dose MRNA COVID-19 Vaccine Allergic Reactions: Limited Role for Excipient Skin Testing. J. Allergy Clin. Immunol. Pract. 2021, 9, 3308–3320.e3. [Google Scholar] [CrossRef] [PubMed]
- Sellaturay, P.; Nasser, S.; Islam, S.; Gurugama, P.; Ewan, P.W. Polyethylene Glycol (PEG) Is a Cause of Anaphylaxis to the Pfizer/BioNTech MRNA COVID-19 Vaccine. Clin. Exp. Allergy 2021, 51, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Habran, M.; Vandebotermet, M.; Schrijvers, R. Polyethylene Glycol Allergy and Immediate-Type Hypersensitivity Reaction to COVID-19 Vaccination: Case Report. J. Investig. Allergol. Clin. Immunol. 2022, 32, 234–235. [Google Scholar] [CrossRef] [PubMed]
- Ieven, T.; Van Weyenbergh, T.; Vandebotermet, M.; Devolder, D.; Breynaert, C.; Schrijvers, R. Tolerability of Polysorbate 80-Containing COVID-19 Vaccines in Confirmed Polyethylene Glycol-Allergic Patients. J. Allergy Clin. Immunol. Pract. 2021, 9, 4470–4472.e1. [Google Scholar] [CrossRef] [PubMed]
- Garvey, L.H.; Nasser, S. Anaphylaxis to the First COVID-19 Vaccine: Is Polyethylene Glycol (PEG) the Culprit? Br. J. Anaesth. 2021, 126, e106–e108. [Google Scholar] [CrossRef] [PubMed]
- Sellaturay, P.; Nasser, S.; Ewan, P. Polyethylene Glycol-Induced Systemic Allergic Reactions (Anaphylaxis). J. Allergy Clin. Immunol. Pract. 2021, 9, 670–675. [Google Scholar] [CrossRef]
- Hsieh, M.-H.; Yamaguchi, Y. Immune Response in Regard to Hypersensitivity Reactions after COVID-19 Vaccination. Biomedicines 2022, 10, 1641. [Google Scholar] [CrossRef]
- Messengers of Hope. Nat. Biotechnol. 2021, 39, 1. [CrossRef]
- Cabanillas, B.; Novak, N.; Akdis, C.A. The Form of PEG Matters: PEG Conjugated with Lipids and Not PEG Alone Could Be the Specific Form Involved in Allergic Reactions to COVID-19 Vaccines. Allergy 2022, 77, 1658–1660. [Google Scholar] [CrossRef]
- Kumar, V.; Qin, J.; Jiang, Y.; Duncan, R.G.; Brigham, B.; Fishman, S.; Nair, J.K.; Akinc, A.; Barros, S.A.; Kasperkovitz, P.V. Shielding of Lipid Nanoparticles for SiRNA Delivery: Impact on Physicochemical Properties, Cytokine Induction, and Efficacy. Mol. Ther. Nucleic Acids 2014, 3, e210. [Google Scholar] [CrossRef]
- Hatziantoniou, S.; Maltezou, H.C.; Tsakris, A.; Poland, G.A.; Anastassopoulou, C. Anaphylactic Reactions to MRNA COVID-19 Vaccines: A Call for Further Study. Vaccine 2021, 39, 2605–2607. [Google Scholar] [CrossRef] [PubMed]
- Risma, K.A.; Edwards, K.M.; Hummell, D.S.; Little, F.F.; Norton, A.E.; Stallings, A.; Wood, R.A.; Milner, J.D. Potential Mechanisms of Anaphylaxis to COVID-19 MRNA Vaccines. J. Allergy Clin. Immunol. 2021, 147, 2075–2082.e2. [Google Scholar] [CrossRef] [PubMed]
- Klimek, L.; Jutel, M.; Akdis, C.A.; Bousquet, J.; Akdis, M.; Torres, M.J.; Agache, I.; Canonica, G.W.; Del Giacco, S.; O’Mahony, L.; et al. ARIA-EAACI Statement on Severe Allergic Reactions to COVID-19 Vaccines—An EAACI-ARIA Position Paper. Allergy 2021, 76, 1624–1628. [Google Scholar] [CrossRef]
- Mortz, C.G.; Kjaer, H.F.; Rasmussen, T.H.; Rasmussen, H.M.; Garvey, L.H.; Bindslev-Jensen, C. Allergy to Polyethylene Glycol and Polysorbates in a Patient Cohort: Diagnostic Work-up and Decision Points for Vaccination during the COVID-19 Pandemic. Clin. Transl. Allergy 2022, 12, e12111. [Google Scholar] [CrossRef]
- Eberlein, B.; Mathes, S.; Fischer, J.; Darsow, U.; Biedermann, T.; Brockow, K. Do Basophil Activation Tests Help Elucidate Allergic Reactions to the Ingredients in COVID-19 Vaccines? Allergy 2022, 77, 2924–2936. [Google Scholar] [CrossRef]
- Lim, X.R.; Tan, J.W.L.; Chan, G.Y.L.; Hou, J.; Xie, L.; Goh, V.H.L.; Boon, J.; Lee, S.S.M.; Teo, C.M.-L.; Tan, S.C.; et al. Evaluation of Patients with Vaccine Allergies Prior to MRNA-Based COVID-19 Vaccination. Vaccines 2022, 10, 1025. [Google Scholar] [CrossRef]
- Brockow, K.; Mathes, S.; Fischer, J.; Volc, S.; Darsow, U.; Eberlein, B.; Biedermann, T. Experience with Polyethylene Glycol Allergy-Guided Risk Management for COVID-19 Vaccine Anaphylaxis. Allergy 2022, 77, 2200–2210. [Google Scholar] [CrossRef]
- Labella, M.; Céspedes, J.A.; Doña, I.; Shamji, M.H.; Agache, I.; Mayorga, C.; Torres, M.J. The Value of the Basophil Activation Test in the Evaluation of Patients Reporting Allergic Reactions to the BNT162b2 MRNA COVID-19 Vaccine. Allergy 2022, 77, 2067–2079. [Google Scholar] [CrossRef]
- Kleine-Tebbe, J.; Erdmann, S.; Knol, E.F.; MacGlashan, D.W.; Poulsen, L.K.; Gibbs, B.F. Diagnostic Tests Based on Human Basophils: Potentials, Pitfalls and Perspectives. Int. Arch. Allergy Immunol. 2006, 141, 79–90. [Google Scholar] [CrossRef]
- Santos, A.F.; Alpan, O.; Hoffmann, H.-J. Basophil Activation Test: Mechanisms and Considerations for Use in Clinical Trials and Clinical Practice. Allergy 2021, 76, 2420–2432. [Google Scholar] [CrossRef]
- Balzer, L.; Pennino, D.; Blank, S.; Seismann, H.; Darsow, U.; Schnedler, M.; McIntyre, M.; Ollert, M.W.; Durham, S.R.; Spillner, E.; et al. Basophil Activation Test Using Recombinant Allergens: Highly Specific Diagnostic Method Complementing Routine Tests in Wasp Venom Allergy. PLoS ONE 2014, 9, e108619. [Google Scholar] [CrossRef] [PubMed]
- Hagau, N.; Gherman-Ionica, N.; Sfichi, M.; Petrisor, C. Threshold for Basophil Activation Test Positivity in Neuromuscular Blocking Agents Hypersensitivity Reactions. Allergy Asthma Clin. Immunol. 2013, 9, 42. [Google Scholar] [CrossRef] [Green Version]
- Restivo, V.; Candore, G.; Barrale, M.; Caravello, E.; Graziano, G.; Onida, R.; Raineri, M.; Tiralongo, S.; Brusca, I. Allergy to Polyethilenglicole of Anti-SARS CoV2 Vaccine Recipient: A Case Report of Young Adult Recipient and the Management of Future Exposure to SARS-CoV2. Vaccines 2021, 9, 412. [Google Scholar] [CrossRef] [PubMed]
- Barbaud, A.; Garvey, L.H.; Arcolaci, A.; Brockow, K.; Mori, F.; Mayorga, C.; Bonadonna, P.; Atanaskovic-Markovic, M.; Moral, L.; Zanoni, G.; et al. Allergies and COVID-19 Vaccines: An ENDA/EAACI Position Paper. Allergy 2022, 77, 2292–2312. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.G.A. Clinical Features and Severity Grading of Anaphylaxis. J. Allergy Clin. Immunol. 2004, 114, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Marchisio, M.; Simeone, P.; Bologna, G.; Ercolino, E.; Pierdomenico, L.; Pieragostino, D.; Ventrella, A.; Antonini, F.; Del Zotto, G.; Vergara, D.; et al. Flow Cytometry Analysis of Circulating Extracellular Vesicle Subtypes from Fresh Peripheral Blood Samples. Int. J. Mol. Sci. 2020, 22, 48. [Google Scholar] [CrossRef] [PubMed]
- Lanuti, P.; Ciccocioppo, F.; Bonanni, L.; Marchisio, M.; Lachmann, R.; Tabet, N.; Pierdomenico, L.; Santavenere, E.; Catinella, V.; Iacone, A.; et al. Amyloid-Specific T-Cells Differentiate Alzheimer’s Disease from Lewy Body Dementia. Neurobiol. Aging 2012, 33, 2599–2611. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients | Sex | Age | Skin Test | BAT |
|---|---|---|---|---|
| Patient 1 | F | 35 | − | − |
| Patient 2 | F | 55 | * | − |
| Patient 3 | M | 69 | − | − |
| Patient 4 | M | 32 | + | − (SI > 2.5) |
| Patient 5 | F | 52 | − | − |
| Patient 6 | F | 50 | − | − (SI > 2.5) |
| Patient 7 | F | 54 | − | − |
| Patient 8 | M | 50 | − | − |
| Patient 9 | F | 53 | * | − (SI > 2.5) |
| Patient 10 | M | 36 | − | − (SI > 2.5) |
| Patient 11 | M | 60 | + | − |
| Patient 12 | F | 51 | − | NR |
| Patient 13 | F | 54 | − | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vespa, S.; Del Biondo, P.; Simeone, P.; Cavallucci, E.; Catitti, G.; Auciello, R.; De Bellis, D.; Altomare, I.; Pierdomenico, L.; Canonico, B.; et al. Basophil Activation Test with Different Polyethylene Glycols in Patients with Suspected PEG Hypersensitivity Reactions. Int. J. Mol. Sci. 2022, 23, 14592. https://doi.org/10.3390/ijms232314592
Vespa S, Del Biondo P, Simeone P, Cavallucci E, Catitti G, Auciello R, De Bellis D, Altomare I, Pierdomenico L, Canonico B, et al. Basophil Activation Test with Different Polyethylene Glycols in Patients with Suspected PEG Hypersensitivity Reactions. International Journal of Molecular Sciences. 2022; 23(23):14592. https://doi.org/10.3390/ijms232314592
Chicago/Turabian StyleVespa, Simone, Pietro Del Biondo, Pasquale Simeone, Enrico Cavallucci, Giulia Catitti, Raffaella Auciello, Domenico De Bellis, Isotta Altomare, Laura Pierdomenico, Barbara Canonico, and et al. 2022. "Basophil Activation Test with Different Polyethylene Glycols in Patients with Suspected PEG Hypersensitivity Reactions" International Journal of Molecular Sciences 23, no. 23: 14592. https://doi.org/10.3390/ijms232314592
APA StyleVespa, S., Del Biondo, P., Simeone, P., Cavallucci, E., Catitti, G., Auciello, R., De Bellis, D., Altomare, I., Pierdomenico, L., Canonico, B., Cicalini, I., Angilletta, I., Del Boccio, P., Pieragostino, D., Santilli, F., Urbani, A., De Laurenzi, V., Stuppia, L., & Lanuti, P. (2022). Basophil Activation Test with Different Polyethylene Glycols in Patients with Suspected PEG Hypersensitivity Reactions. International Journal of Molecular Sciences, 23(23), 14592. https://doi.org/10.3390/ijms232314592