
Visualization of Murine Vascular Remodeling and Blood Flow Dynamics by Ultra-High-Frequency Ultrasound Imaging





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
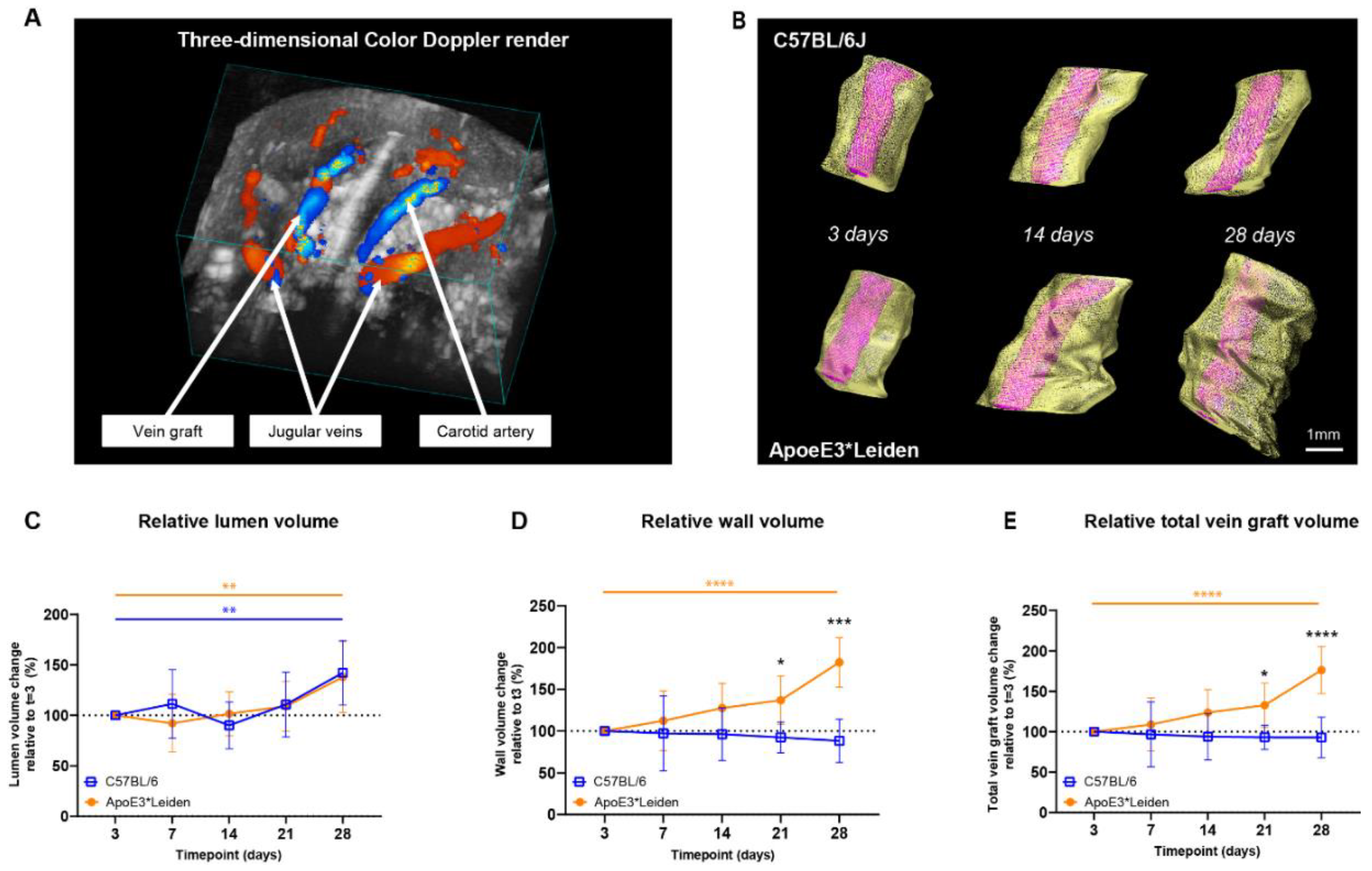
2.1. Area and Volume Ultrasound Measurements of Vein Grafts of C57BL/6J and ApoE3*Leiden Mice Can Be Quantified over Time
2.1.1. Two-Dimensional Morphological Analysis
2.1.2. Three-Dimensional Reconstructions for Volume Measurements
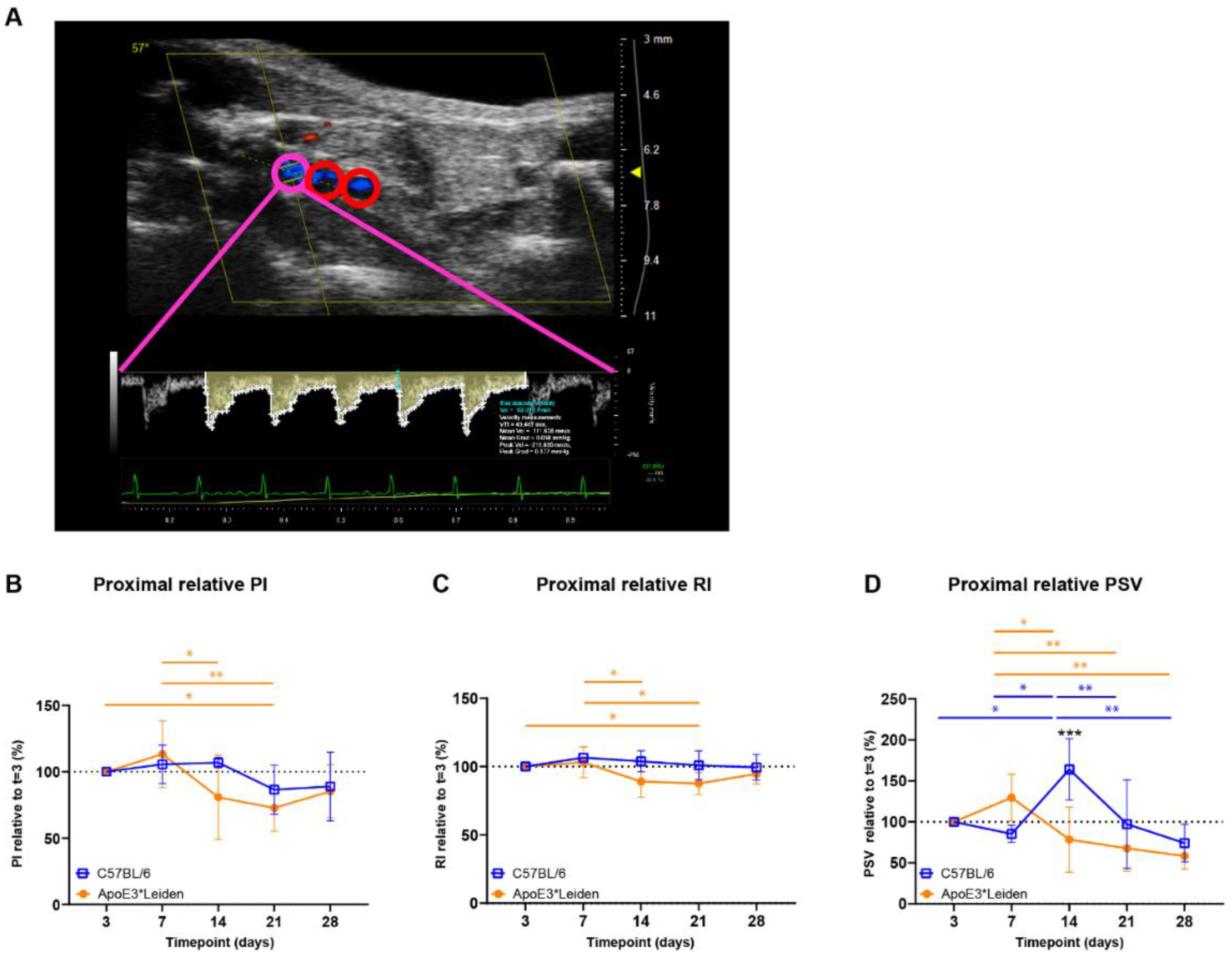
2.2. Clinically Relevant Ultrasound Velocity Measurements and Derivatives Can Be Quantified at Three Distinct Sites in Vein Grafted C57BL/6J and ApoE3*Leiden Mice over Time
2.3. Systolic Acceleration Measurements in Vein Grafts of C57BL/6J and ApoE3*Leiden Mice over Time
2.4. Longitudinal Characterization of Flow Patterns in Murine AVFs
2.4.1. Blood Flow Rate Measurements Can Distinguish between Matured and Non-Matured AVFs in C57BL/6J Mice
2.4.2. Blood Flow Pattern and Velocity Measurements Can Be Used to Quantify the Blood Flow in AVFs in C57BL/6J Mice over Time
3. Discussion
4. Materials and Methods
4.1. Animals and Surgery
4.2. Ultrasound Imaging
4.3. Ultrasound Data Analyses
4.3.1. Morphological Quantification of Vein Graft
4.3.2. Hemodynamic Quantification
4.4. Statistics and Software
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACCmax | Maximum systolic acceleration |
| ACCsys | Mean systolic acceleration |
| AVF | Arteriovenous fistula |
| B-mode | Brightness mode |
| EDV | End-diastolic velocity |
| RI | Resistive index |
| PI | Pulsatility index |
| PSV | Peak systolic velocity |
| PW | Pulsed wave |
| SBI | Spectral broadening index |
References
- de Vries, M.R.; Quax, P.H.A. Inflammation in Vein Graft Disease. Front. Cardiovasc. Med. 2018, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Gasper, W.J.; Owens, C.D.; Kim, J.M.; Hills, N.; Belkin, M.; Creager, M.A.; Conte, M.S. Thirty-day vein remodeling is predictive of midterm graft patency after lower extremity bypass. J. Vasc. Surg. 2013, 57, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Bezhaeva, T.; de Vries, M.R.; Geelhoed, W.J.; van der Veer, E.P.; Versteeg, S.; van Alem, C.M.A.; Voorzaat, B.M.; Eijkelkamp, N.; van der Bogt, K.E.; Agoulnik, A.I.; et al. Relaxin receptor deficiency promotes vascular inflammation and impairs outward remodeling in arteriovenous fistulas. FASEB J. 2018, 32, 6293–6304. [Google Scholar] [CrossRef] [PubMed]
- de Vries, M.R.; Simons, K.H.; Jukema, J.W.; Braun, J.; Quax, P.H. Vein graft failure: From pathophysiology to clinical outcomes. Nat. Rev. Cardiol. 2016, 13, 451–470. [Google Scholar] [CrossRef] [PubMed]
- Korshunov, V.A.; Schwartz, S.M.; Berk, B.C. Vascular remodeling: Hemodynamic and biochemical mechanisms underlying Glagov’s phenomenon. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1722–1728. [Google Scholar] [CrossRef]
- Lardenoye, J.H.; de Vries, M.R.; Lowik, C.W.; Xu, Q.; Dhore, C.R.; Cleutjens, J.P.; van Hinsbergh, V.W.; van Bockel, J.H.; Quax, P.H. Accelerated atherosclerosis and calcification in vein grafts: A study in APOE*3 Leiden transgenic mice. Circ. Res. 2002, 91, 577–584. [Google Scholar] [CrossRef]
- Schinstock, C.A.; Albright, R.C.; Williams, A.W.; Dillon, J.J.; Bergstralh, E.J.; Jenson, B.M.; McCarthy, J.T.; Nath, K.A. Outcomes of arteriovenous fistula creation after the Fistula First Initiative. Clin. J. Am. Soc. Nephrol. 2011, 6, 1996–2002. [Google Scholar] [CrossRef]
- Shiu, Y.T.; Rotmans, J.I.; Geelhoed, W.J.; Pike, D.B.; Lee, T. Arteriovenous conduits for hemodialysis: How to better modulate the pathophysiological vascular response to optimize vascular access durability. Am. J. Physiol. Renal Physiol. 2019, 316, F794–F806. [Google Scholar] [CrossRef]
- Rothuizen, T.C.; Wong, C.; Quax, P.H.; van Zonneveld, A.J.; Rabelink, T.J.; Rotmans, J.I. Arteriovenous access failure: More than just intimal hyperplasia? Nephrol. Dial. Transplant. 2013, 28, 1085–1092. [Google Scholar] [CrossRef]
- Wong, C.Y.; de Vries, M.R.; Wang, Y.; van der Vorst, J.R.; Vahrmeijer, A.L.; van Zonneveld, A.J.; Hamming, J.F.; Roy-Chaudhury, P.; Rabelink, T.J.; Quax, P.H.; et al. A Novel Murine Model of Arteriovenous Fistula Failure: The Surgical Procedure in Detail. J. Vis. Exp. 2016, 108, e53294. [Google Scholar] [CrossRef]
- Moran, C.M.; Thomson, A.J.W. Preclinical Ultrasound Imaging—A Review of Techniques and Imaging Applications. Front. Phys. 2020, 8. [Google Scholar] [CrossRef]
- Petersen, L.J.; Petersen, J.R.; Ladefoged, S.D.; Mehlsen, J.; Jensen, H.A. The pulsatility index and the resistive index in renal arteries in patients with hypertension and chronic renal failure. Nephrol. Dial. Transplant. 1995, 10, 2060–2064. [Google Scholar] [PubMed]
- Irace, C.; Gnasso, A.; Cirillo, F.; Leonardo, G.; Ciamei, M.; Crivaro, A.; Renzulli, A.; Cotrufo, M. Arterial remodeling of the common carotid artery after aortic valve replacement in patients with aortic stenosis. Stroke 2002, 33, 2446–2450. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, M.; Wyttenbach, R.; Corti, R.; Staub, D.; Gallino, A. The Growing Field of Imaging of Atherosclerosis in Peripheral Arteries. Angiology 2019, 70, 20–34. [Google Scholar] [CrossRef]
- Matsuo, Y.; Takumi, T.; Mathew, V.; Chung, W.Y.; Barsness, G.W.; Rihal, C.S.; Gulati, R.; McCue, E.T.; Holmes, D.R.; Eeckhout, E.; et al. Plaque characteristics and arterial remodeling in coronary and peripheral arterial systems. Atherosclerosis 2012, 223, 365–371. [Google Scholar] [CrossRef]
- Iwakoshi, S.; Hirai, T.; Kichikawa, K. Updates on Ultrasonography Imaging in Abdominal Aortic Aneurysm. Ann. Vasc. Dis. 2019, 12, 319–322. [Google Scholar] [CrossRef]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef]
- Sier, V.Q.; van der Vorst, J.R.; Quax, P.H.A.; de Vries, M.R.; Zonoobi, E.; Vahrmeijer, A.L.; Dekkers, I.A.; de Geus-Oei, L.F.; Smits, A.M.; Cai, W.; et al. Endoglin/CD105-Based Imaging of Cancer and Cardiovascular Diseases: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 4804. [Google Scholar] [CrossRef]
- Mallery, J.A.; Tobis, J.M.; Griffith, J.; Gessert, J.; McRae, M.; Moussabeck, O.; Bessen, M.; Moriuchi, M.; Henry, W.L. Assessment of normal and atherosclerotic arterial wall thickness with an intravascular ultrasound imaging catheter. Am. Heart J. 1990, 119, 1392–1400. [Google Scholar] [CrossRef][Green Version]
- de Jong, A.; Sier, V.Q.; Peters, H.A.B.; Schilder, N.K.M.; Jukema, J.W.; Goumans, M.J.T.H.; Quax, P.H.A.; de Vries, M.R. Interfering in the ALK1 Pathway Results in Macrophage-Driven Outward Remodeling of Murine Vein Grafts. Front. Cardiovasc. Med. 2022, 8, 784980. [Google Scholar] [CrossRef]
- Eberth, J.F.; Popovic, N.; Gresham, V.C.; Wilson, E.; Humphrey, J.D. Time course of carotid artery growth and remodeling in response to altered pulsatility. Am. J. Physiol. Heart Circ. Physiol. 2010, 299, H1875–H1883. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brouwers, J.; Jiang, J.F.Y.; Feld, R.T.; van Doorn, L.P.; van Wissen, R.C.; van Walderveen, M.A.A.; Hamming, J.F.; Schepers, A. A New Doppler-Derived Parameter to Quantify Internal Carotid Artery Stenosis: Maximal Systolic Acceleration. Ann. Vasc. Surg. 2022, 81, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Bardelli, M.; Veglio, F.; Arosio, E.; Cataliotti, A.; Valvo, E.; Morganti, A.; Italian Group for the Study of Renovascular Hypertension. New intrarenal echo-Doppler velocimetric indices for the diagnosis of renal artery stenosis. Kidney Int. 2006, 69, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Van Tongeren, R.B.; Bastiaansen, A.J.; Van Wissen, R.C.; Le Cessie, S.; Hamming, J.F.; Van Bockel, J.H. A comparison of the Doppler-derived maximal systolic acceleration versus the ankle-brachial pressure index or detecting and quantifying peripheral arterial occlusive disease in diabetic patients. J. Cardiovasc. Surg. 2010, 51, 391–398. [Google Scholar]
- Brouwers, J.; van Doorn, L.P.; van Wissen, R.C.; Putter, H.; Hamming, J.F. Using maximal systolic acceleration to diagnose and assess the severity of peripheral artery disease in a flow model study. J. Vasc. Surg. 2020, 71, 242–249. [Google Scholar] [CrossRef]
- Lomonte, C.; Casucci, F.; Antonelli, M.; Giammaria, B.; Losurdo, N.; Marchio, G.; Basile, C. Is there a place for duplex screening of the brachial artery in the maturation of arteriovenous fistulas? Semin. Dial. 2005, 18, 243–246. [Google Scholar] [CrossRef]
- Dixon, B.S. Why don’t fistulas mature? Kidney Int. 2006, 70, 1413–1422. [Google Scholar] [CrossRef]
- Frauchiger, B.; Schmid, H.P.; Roedel, C.; Moosmann, P.; Staub, D. Comparison of carotid arterial resistive indices with intima-media thickness as sonographic markers of atherosclerosis. Stroke 2001, 32, 836–841. [Google Scholar] [CrossRef]
- Heyer, E.J.; Mergeche, J.L.; Connolly, E.S., Jr. Middle cerebral artery pulsatility index and cognitive improvement after carotid endarterectomy for symptomatic stenosis. J. Neurosurg. 2014, 120, 126–131. [Google Scholar] [CrossRef]
- Buschmann, E.E.; Li, L.; Brix, M.; Zietzer, A.; Hillmeister, P.; Busjahn, A.; Bramlage, P.; Buschmann, I. A novel computer-aided diagnostic approach for detecting peripheral arterial disease in patients with diabetes. PLoS ONE 2018, 13, e0199374. [Google Scholar] [CrossRef]
- Hoeks, A.P.G.; Reneman, R.S. Flow patterns and arterial wall dynamics. In Cerebrovascular Ultrasound: Theory, Practice and Future Developments; Hennerici, M.G., Meairs, S.P., Eds.; Cambridge University Press: Cambridge, UK, 2001; pp. 77–87. [Google Scholar]
- Sprynger, M.; Rigo, F.; Moonen, M.; Aboyans, V.; Edvardsen, T.; de Alcantara, M.L.; Brodmann, M.; Naka, K.K.; Kownator, S.; Simova, I.; et al. Focus on echovascular imaging assessment of arterial disease: Complement to the ESC guidelines (PARTIM 1) in collaboration with the Working Group on Aorta and Peripheral Vascular Diseases. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1195–1221. [Google Scholar] [CrossRef] [PubMed]
- Zieman, S.J.; Melenovsky, V.; Kass, D.A. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, S.; Amirian, J.H.; Litovsky, S.H.; Smalling, R.W.; Emelianov, S.Y. Ex vivo Characterization of Atherosclerosis using Intravascular Photoacoustic Imaging. Opt. Express 2007, 15, 16657–16666. [Google Scholar] [CrossRef] [PubMed]
- Watase, H.; Sun, J.; Hippe, D.S.; Balu, N.; Li, F.; Zhao, X.; Mani, V.; Fayad, Z.A.; Fuster, V.; Hatsukami, T.S.; et al. Carotid Artery Remodeling Is Segment Specific: An In Vivo Study by Vessel Wall Magnetic Resonance Imaging. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.I.; Khalil, R.M.; Obuchowski, N.A.; Baus, L.K. Common carotid artery: Variability of Doppler US velocity measurements. Radiology 1997, 204, 339–341. [Google Scholar] [CrossRef]
- Lee, V.S.; Hertzberg, B.S.; Workman, M.J.; Smith, T.P.; Kliewer, M.A.; DeLong, D.M.; Carroll, B.A. Variability of Doppler US measurements along the common carotid artery: Effects on estimates of internal carotid arterial stenosis in patients with angiographically proved disease. Radiology 2000, 214, 387–392. [Google Scholar] [CrossRef]
- Tremoleda, J.L.; Kerton, A.; Gsell, W. Anaesthesia and physiological monitoring during in vivo imaging of laboratory rodents: Considerations on experimental outcomes and animal welfare. EJNMMI Res. 2012, 2, 44. [Google Scholar] [CrossRef]
- Hartley, C.J.; Reddy, A.K.; Madala, S.; Michael, L.H.; Entman, M.L.; Taffet, G.E. Effects of isoflurane on coronary blood flow velocity in young, old and ApoE−/− mice measured by Doppler ultrasound. Ultrasound Med. Biol. 2007, 33, 512–521. [Google Scholar] [CrossRef]
- Sawada, H.; Chen, J.Z.; Wright, B.C.; Moorleghen, J.J.; Lu, H.S.; Daugherty, A. Ultrasound Imaging of the Thoracic and Abdominal Aorta in Mice to Determine Aneurysm Dimensions. J. Vis. Exp. 2019, 145, e59013. [Google Scholar] [CrossRef]
- AIUM Practice Parameter for the Performance of Vascular Ultrasound Examinations for Postoperative Assessment of Hemodialysis Access. J. Ultrasound Med. 2020, 39, E39–E48. [CrossRef]
- Zamboli, P.; Fiorini, F.; D’Amelio, A.; Fatuzzo, P.; Granata, A. Color Doppler ultrasound and arteriovenous fistulas for hemodialysis. J. Ultrasound 2014, 17, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.Y.; de Vries, M.R.; Wang, Y.; van der Vorst, J.R.; Vahrmeijer, A.L.; van Zonneveld, A.J.; Roy-Chaudhury, P.; Rabelink, T.J.; Quax, P.H.; Rotmans, J.I. Vascular remodeling and intimal hyperplasia in a novel murine model of arteriovenous fistula failure. J. Vasc. Surg. 2014, 59, 192–201.e1. [Google Scholar] [CrossRef]
- Wong, C.; Bezhaeva, T.; Rothuizen, T.C.; Metselaar, J.M.; de Vries, M.R.; Verbeek, F.P.; Vahrmeijer, A.L.; Wezel, A.; van Zonneveld, A.J.; Rabelink, T.J.; et al. Liposomal prednisolone inhibits vascular inflammation and enhances venous outward remodeling in a murine arteriovenous fistula model. Sci. Rep. 2016, 6, 30439. [Google Scholar] [CrossRef] [PubMed]
- Bezhaeva, T.; Wong, C.; de Vries, M.R.; van der Veer, E.P.; van Alem, C.M.A.; Que, I.; Lalai, R.A.; van Zonneveld, A.J.; Rotmans, J.I.; Quax, P.H.A. Deficiency of TLR4 homologue RP105 aggravates outward remodeling in a murine model of arteriovenous fistula failure. Sci. Rep. 2017, 7, 10269. [Google Scholar] [CrossRef] [PubMed]
- de Jong, A.; de Jong, R.C.M.; Peters, E.A.; Arens, R.; Jukema, J.W.; de Vries, M.R.; Quax, P.H.A. P300/CBP Associated Factor (PCAF) Deficiency Enhances Diet-Induced Atherosclerosis in ApoE3*Leiden Mice via Systemic Inhibition of Regulatory T Cells. Front. Cardiovasc. Med. 2020, 7, 604821. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sier, V.Q.; de Jong, A.; Quax, P.H.A.; de Vries, M.R. Visualization of Murine Vascular Remodeling and Blood Flow Dynamics by Ultra-High-Frequency Ultrasound Imaging. Int. J. Mol. Sci. 2022, 23, 13298. https://doi.org/10.3390/ijms232113298
Sier VQ, de Jong A, Quax PHA, de Vries MR. Visualization of Murine Vascular Remodeling and Blood Flow Dynamics by Ultra-High-Frequency Ultrasound Imaging. International Journal of Molecular Sciences. 2022; 23(21):13298. https://doi.org/10.3390/ijms232113298
Chicago/Turabian StyleSier, Vincent Q., Alwin de Jong, Paul H. A. Quax, and Margreet R. de Vries. 2022. "Visualization of Murine Vascular Remodeling and Blood Flow Dynamics by Ultra-High-Frequency Ultrasound Imaging" International Journal of Molecular Sciences 23, no. 21: 13298. https://doi.org/10.3390/ijms232113298
APA StyleSier, V. Q., de Jong, A., Quax, P. H. A., & de Vries, M. R. (2022). Visualization of Murine Vascular Remodeling and Blood Flow Dynamics by Ultra-High-Frequency Ultrasound Imaging. International Journal of Molecular Sciences, 23(21), 13298. https://doi.org/10.3390/ijms232113298