
Dual Oxidase 2 (DUOX2) as a Proteomic Biomarker for Predicting Treatment Response to Chemoradiation Therapy for Locally Advanced Rectal Cancer: Using High-Throughput Proteomic Analysis and Machine Learning Algorithm

 , , , and
, , , and
Abstract
1. Introduction
2. Results
2.1. Overall Protein Identification and Quantification
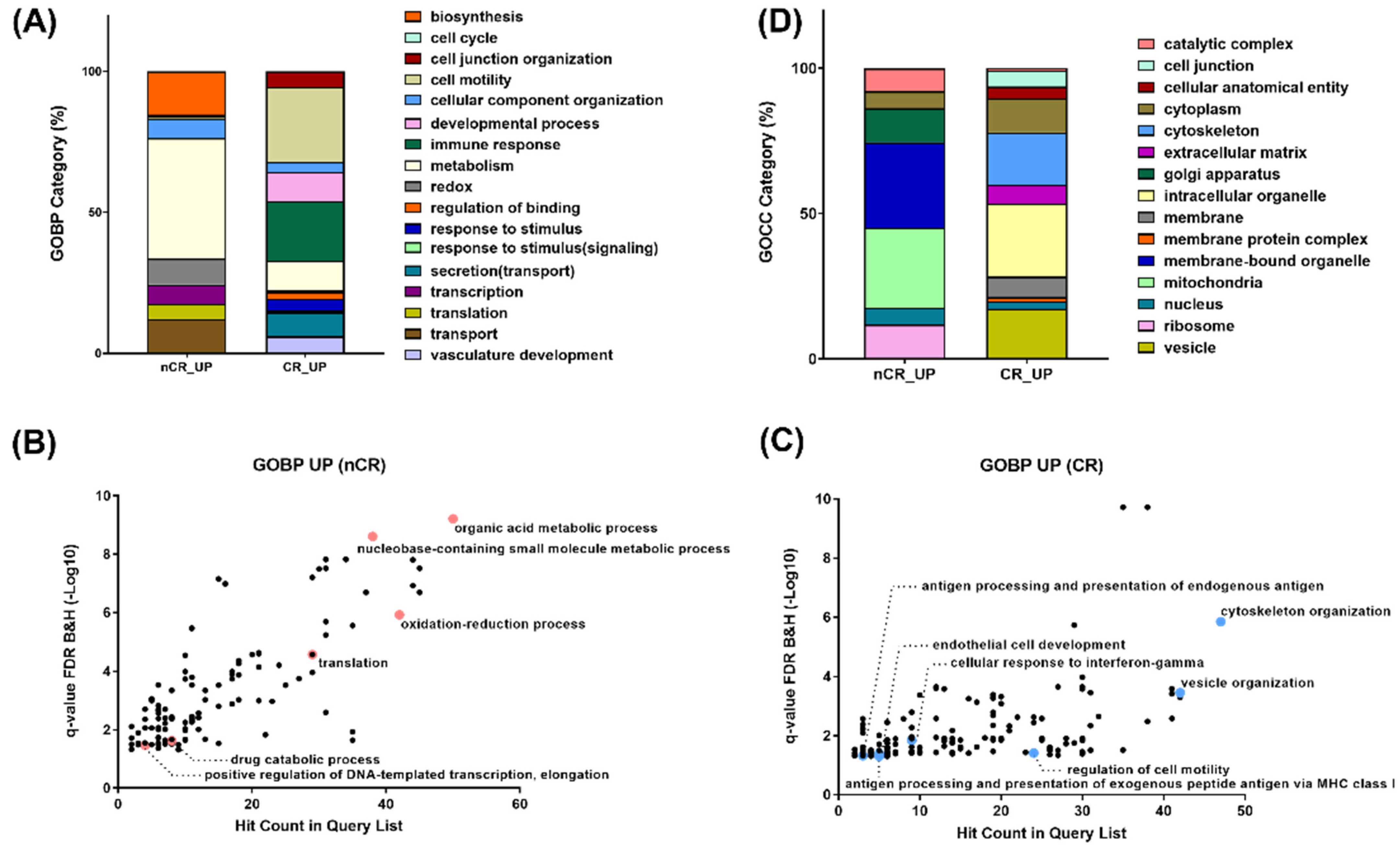
2.2. Characterization of Enriched Pathways Based on CCRT Response
2.3. Machine Learning Approach for Selecting Protein Biomarkers to Predict Treatment Response
2.4. Immunohistochemical Validation of the Predictive Value of DUOX2
3. Discussion
4. Materials and Methods
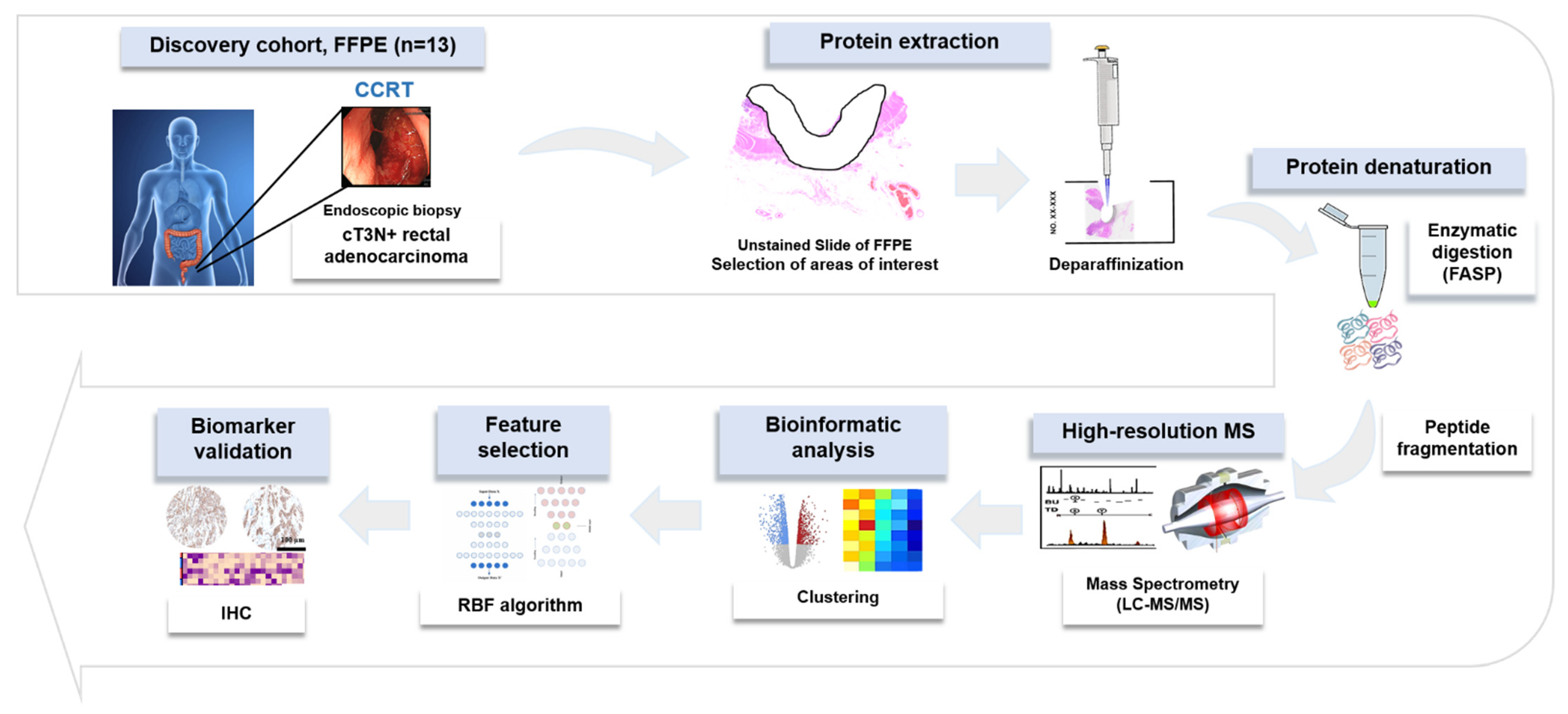
4.1. Sample Collection
4.2. LC-MS/MS Proteomics Analysis
4.3. Data Analysis and Peptide Identification, Label-Free Quantification
4.4. Machine Learning Analysis for Prioritizing Predictive Biomarkers
4.5. Immunohistochemistry for Validation of Selected Biomarker
4.6. Bioinformatics and Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; van Krieken, J.H.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Roh, M.S.; Colangelo, L.H.; O’Connell, M.J.; Yothers, G.; Deutsch, M.; Allegra, C.J.; Kahlenberg, M.S.; Baez-Diaz, L.; Ursiny, C.S.; Petrelli, N.J.; et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J. Clin. Oncol. 2009, 27, 5124–5130. [Google Scholar] [CrossRef] [PubMed]
- Peeters, K.C.; van de Velde, C.J.; Leer, J.W.; Martijn, H.; Junggeburt, J.M.; Kranenbarg, E.K.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Marijnen, C.A. Late side effects of short-course preoperative radiotherapy combined with total mesorectal excision for rectal cancer: Increased bowel dysfunction in irradiated patients--a Dutch colorectal cancer group study. J. Clin. Oncol. 2005, 23, 6199–6206. [Google Scholar] [CrossRef]
- Paun, B.C.; Cassie, S.; MacLean, A.R.; Dixon, E.; Buie, W.D. Postoperative complications following surgery for rectal cancer. Ann. Surg. 2010, 251, 807–818. [Google Scholar] [CrossRef]
- Maas, M.; Nelemans, P.J.; Valentini, V.; Das, P.; Rodel, C.; Kuo, L.J.; Calvo, F.A.; Garcia-Aguilar, J.; Glynne-Jones, R.; Haustermans, K.; et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: A pooled analysis of individual patient data. Lancet Oncol. 2010, 11, 835–844. [Google Scholar] [CrossRef]
- Fokas, E.; Liersch, T.; Fietkau, R.; Hohenberger, W.; Beissbarth, T.; Hess, C.; Becker, H.; Ghadimi, M.; Mrak, K.; Merkel, S.; et al. Tumor regression grading after preoperative chemoradiotherapy for locally advanced rectal carcinoma revisited: Updated results of the CAO/ARO/AIO-94 trial. J. Clin. Oncol. 2014, 32, 1554–1562. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Perez, R.O.; Nadalin, W.; Sabbaga, J.; Ribeiro, U., Jr.; Silva e Sousa, A.H., Jr.; Campos, F.G.; Kiss, D.R.; Gama-Rodrigues, J. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: Long-term results. Ann. Surg. 2004, 240, 711–717. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Gama-Rodrigues, J.; Sao Juliao, G.P.; Proscurshim, I.; Sabbagh, C.; Lynn, P.B.; Perez, R.O. Local recurrence after complete clinical response and watch and wait in rectal cancer after neoadjuvant chemoradiation: Impact of salvage therapy on local disease control. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 822–828. [Google Scholar] [CrossRef]
- Renehan, A.G.; Malcomson, L.; Emsley, R.; Gollins, S.; Maw, A.; Myint, A.S.; Rooney, P.S.; Susnerwala, S.; Blower, A.; Saunders, M.P.; et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): A propensity-score matched cohort analysis. Lancet Oncol. 2016, 17, 174–183. [Google Scholar] [CrossRef]
- Kuremsky, J.G.; Tepper, J.E.; McLeod, H.L. Biomarkers for response to neoadjuvant chemoradiation for rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 673–688. [Google Scholar] [CrossRef]
- Machackova, T.; Prochazka, V.; Kala, Z.; Slaby, O. Translational Potential of MicroRNAs for Preoperative Staging and Prediction of Chemoradiotherapy Response in Rectal Cancer. Cancers 2019, 11, 1545. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.W.; Li, M.; Guo, Z.W.; Zhang, R.; Xi, S.Y.; Zhang, X.G.; Li, Y.; Wu, D.Q.; Ren, Y.F.; Pang, X.L.; et al. A Genotype Signature for Predicting Pathologic Complete Response in Locally Advanced Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Tyanova, S.; Albrechtsen, R.; Kronqvist, P.; Cox, J.; Mann, M.; Geiger, T. Proteomic maps of breast cancer subtypes. Nat. Commun. 2016, 7, 10259. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.S.; Huang, T.; Zhong, X.M.; Zhang, H.W.; Cong, X.L.; Xu, H.; Lu, G.X.; Yu, F.; Xue, S.B.; Lv, Z.W.; et al. Proteogenomic characterization and comprehensive integrative genomic analysis of human colorectal cancer liver metastasis. Mol. Cancer 2018, 17, 139. [Google Scholar] [CrossRef]
- Hu, T.; Wu, X.; Li, K.; Li, Y.; He, P.; Wu, Z.; Fan, J.; Liu, W.; Guan, M. AKAP12 Endogenous Transcripts Suppress The Proliferation, Migration And Invasion Of Colorectal Cancer Cells By Directly Targeting oncomiR-183-5p. Onco-Targets Ther. 2019, 12, 8301–8310. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, X.; Liang, Q.; Wang, S.; Liao, X.; Li, D.; Pan, F. Prognostic Value of Dynactin mRNA Expression in Cutaneous Melanoma. Med. Sci. Monit. 2018, 24, 3752–3763. [Google Scholar] [CrossRef]
- Bertz, M.; Kuhn, K.; Koeberle, S.C.; Muller, M.F.; Hoelzer, D.; Thies, K.; Deubel, S.; Thierbach, R.; Kipp, A.P. Selenoprotein H controls cell cycle progression and proliferation of human colorectal cancer cells. Free Radic. Biol. Med. 2018, 127, 98–107. [Google Scholar] [CrossRef]
- Zhang, X.; Han, J.; Feng, L.; Zhi, L.; Jiang, D.; Yu, B.; Zhang, Z.; Gao, B.; Zhang, C.; Li, M.; et al. DUOX2 promotes the progression of colorectal cancer cells by regulating the AKT pathway and interacting with RPL3. Carcinogenesis 2020, 42, 105–117. [Google Scholar] [CrossRef]
- Kang, K.A.; Ryu, Y.S.; Piao, M.J.; Shilnikova, K.; Kang, H.K.; Yi, J.M.; Boulanger, M.; Paolillo, R.; Bossis, G.; Yoon, S.Y.; et al. DUOX2-mediated production of reactive oxygen species induces epithelial mesenchymal transition in 5-fluorouracil resistant human colon cancer cells. Redox Biol. 2018, 17, 224–235. [Google Scholar] [CrossRef]
- Logtenberg, M.E.W.; Jansen, J.H.M.; Raaben, M.; Toebes, M.; Franke, K.; Brandsma, A.M.; Matlung, H.L.; Fauster, A.; Gomez-Eerland, R.; Bakker, N.A.M.; et al. Glutaminyl cyclase is an enzymatic modifier of the CD47- SIRPalpha axis and a target for cancer immunotherapy. Nat. Med. 2019, 25, 612–619. [Google Scholar] [CrossRef]
- Cheng, Y.; Wu, J.; Qin, B.; Zou, B.C.; Wang, Y.H.; Li, Y. CREB1-induced lncRNA LEF1-AS1 contributes to colorectal cancer progression via the miR-489/DIAPH1 axis. Biochem. Biophys. Res. Commun. 2020, 526, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Zhu, J.; Dong, Y.; He, C.; Hu, X. Suppressor of Ty homolog-5, a novel tumor-specific human telomerase reverse transcriptase promoter-binding protein and activator in colon cancer cells. Oncotarget 2015, 6, 32841–32855. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.H.; Wong, K.Y.; Seim, I.; Wang, R.; He, Y.; Wu, A.; Patrick, M.; Lourie, R.; Schreiber, V.; Giri, R.; et al. MUC13 promotes the development of colitis-associated colorectal tumors via beta-catenin activity. Oncogene 2019, 38, 7294–7310. [Google Scholar] [CrossRef] [PubMed]
- Pabla, S.; Seager, R.J.; Van Roey, E.; Gao, S.; Hoefer, C.; Nesline, M.K.; DePietro, P.; Burgher, B.; Andreas, J.; Giamo, V.; et al. Integration of tumor inflammation, cell proliferation, and traditional biomarkers improves prediction of immunotherapy resistance and response. Biomark. Res. 2021, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.T.; Yang, C.M. Role of NADPH oxidase/ROS in pro-inflammatory mediators-induced airway and pulmonary diseases. Biochem. Pharmacol. 2012, 84, 581–590. [Google Scholar] [CrossRef]
- Geiszt, M.; Witta, J.; Baffi, J.; Lekstrom, K.; Leto, T.L. Dual oxidases represent novel hydrogen peroxide sources supporting mucosal surface host defense. FASEB J. 2003, 17, 1502–1504. [Google Scholar] [CrossRef]
- Rigutto, S.; Hoste, C.; Grasberger, H.; Milenkovic, M.; Communi, D.; Dumont, J.E.; Corvilain, B.; Miot, F.; De Deken, X. Activation of dual oxidases Duox1 and Duox2: Differential regulation mediated by camp-dependent protein kinase and protein kinase C-dependent phosphorylation. J. Biol. Chem. 2009, 284, 6725–6734. [Google Scholar] [CrossRef]
- Landry, W.D.; Cotter, T.G. ROS signalling, NADPH oxidases and cancer. Biochem. Soc. Trans. 2014, 42, 934–938. [Google Scholar] [CrossRef]
- Chu, F.F.; Esworthy, R.S.; Doroshow, J.H. Role of Se-dependent glutathione peroxidases in gastrointestinal inflammation and cancer. Free Radic. Biol. Med. 2004, 36, 1481–1495. [Google Scholar] [CrossRef]
- Wu, Y.; Konate, M.M.; Lu, J.; Makhlouf, H.; Chuaqui, R.; Antony, S.; Meitzler, J.L.; Difilippantonio, M.J.; Liu, H.; Juhasz, A.; et al. IL-4 and IL-17A Cooperatively Promote Hydrogen Peroxide Production, Oxidative DNA Damage, and Upregulation of Dual Oxidase 2 in Human Colon and Pancreatic Cancer Cells. J. Immunol. 2019, 203, 2532–2544. [Google Scholar] [CrossRef]
- Lin, S.C.; Chang, I.W.; Hsieh, P.L.; Lin, C.Y.; Sun, D.P.; Sheu, M.J.; Yang, C.C.; Lin, L.C.; He, H.L.; Tian, Y.F. High Immunoreactivity of DUOX2 Is Associated With Poor Response to Preoperative Chemoradiation Therapy and Worse Prognosis in Rectal Cancers. J. Cancer 2017, 8, 2756–2764. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Moon, S.; Kim, Y.; Kim, J.; Jin, J.; Kim, Y. In-depth proteomic analysis of mouse microglia using a combination of FASP and StageTip-based, high pH, reversed-phase fractionation. Proteomics 2013, 13, 2984–2988. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Jin, J.; Woo, J.; Min, H.; Kim, Y. Proteomic analysis of mouse astrocytes and their secretome by a combination of FASP and StageTip-based, high pH, reversed-phase fractionation. Proteomics 2014, 14, 1604–1609. [Google Scholar] [CrossRef]
- Tyanova, S.; Temu, T.; Cox, J. The MaxQuant computational platform for mass spectrometry-based shotgun proteomics. Nat. Protoc. 2016, 11, 2301–2319. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.; Neuhauser, N.; Michalski, A.; Scheltema, R.A.; Olsen, J.V.; Mann, M. Andromeda: A peptide search engine integrated into the MaxQuant environment. J. Proteome. Res. 2011, 10, 1794–1805. [Google Scholar] [CrossRef] [PubMed]
- Schwanhausser, B.; Busse, D.; Li, N.; Dittmar, G.; Schuchhardt, J.; Wolf, J.; Chen, W.; Selbach, M. Global quantification of mammalian gene expression control. Nature 2011, 473, 337–342. [Google Scholar] [CrossRef]
- Tyanova, S.; Temu, T.; Sinitcyn, P.; Carlson, A.; Hein, M.Y.; Geiger, T.; Mann, M.; Cox, J. The Perseus computational platform for comprehensive analysis of (prote)omics data. Nat. Methods 2016, 13, 731–740. [Google Scholar] [CrossRef]
- Hirsch, F.R.; Varella-Garcia, M.; Bunn, P.A., Jr.; Di Maria, M.V.; Veve, R.; Bremmes, R.M.; Baron, A.E.; Zeng, C.; Franklin, W.A. Epidermal growth factor receptor in non-small-cell lung carcinomas: Correlation between gene copy number and protein expression and impact on prognosis. J. Clin. Oncol. 2003, 21, 3798–3807. [Google Scholar] [CrossRef]
- Chen, J.; Xu, H.; Aronow, B.J.; Jegga, A.G. Improved human disease candidate gene prioritization using mouse phenotype. BMC Bioinform. 2007, 8, 392. [Google Scholar] [CrossRef]
- Baker, P.R.; Chalkley, R.J. MS-viewer: A web-based spectral viewer for proteomics results. Mol. Cell Proteom. 2014, 13, 1392–1396. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set (n = 13) | Validation Set (n = 79) | ||||||
|---|---|---|---|---|---|---|---|
| Characteristics | CR (n = 5), n (%) | Non-CR (n = 8), n (%) | p-Value | CR (n = 17), n (%) | Non-CR (n = 62), n (%) | p-Value | |
| Age | ≤60 years | 2 (40.0%) | 2 (25.0%) | 0.569 | 10 (58.8%) | 34 (54.8%) | 0.770 |
| >60 years | 3 (60.0%) | 6 (75.0%) | 7 (41.2%) | 28 (45.2%) | |||
| Gender | Male | 3 (60.0%) | 6 (75.0%) | 0.569 | 11 (64.7%) | 44 (71.0%) | 0.619 |
| Female | 2 (40.0%) | 2 (25.0%) | 6 (35.3%) | 18 (29.0%) | |||
| Distance from anal verge | ≤5 cm | 4 (80.0%) | 6 (75.0%) | 0.835 | 12 (70.6%) | 45 (72.6%) | 0.871 |
| >5 cm | 1 (20.0%) | 2 (25.0%) | 5 (29.4%) | 17 (27.4%) | |||
| Initial CEA level | ≤3.0 ng/mL | 1 (20.0%) | 3 (37.5%) | 0.506 | 14 (82.4%) | 26 (41.9%) | 0.003 |
| >3.0 ng/mL | 4 (80.0%) | 5 (62.5%) | 3 (17.6%) | 36 (58.1%) | |||
| Type of Surgery | LAR | 5 (38.5%) | 8 (61.5%) | N/A | 16 (94.1%) | 60 (96.8%) | 0.612 |
| APR | – | – | 1 (5.9%) | 2 (3.2%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Ryu, H.S.; Park, H.C.; Yu, J.I.; Yoo, G.S.; Choi, C.; Nam, H.; Lee, J.J.B.; Do, I.-G.; Han, D.; et al. Dual Oxidase 2 (DUOX2) as a Proteomic Biomarker for Predicting Treatment Response to Chemoradiation Therapy for Locally Advanced Rectal Cancer: Using High-Throughput Proteomic Analysis and Machine Learning Algorithm. Int. J. Mol. Sci. 2022, 23, 12923. https://doi.org/10.3390/ijms232112923
Lee H, Ryu HS, Park HC, Yu JI, Yoo GS, Choi C, Nam H, Lee JJB, Do I-G, Han D, et al. Dual Oxidase 2 (DUOX2) as a Proteomic Biomarker for Predicting Treatment Response to Chemoradiation Therapy for Locally Advanced Rectal Cancer: Using High-Throughput Proteomic Analysis and Machine Learning Algorithm. International Journal of Molecular Sciences. 2022; 23(21):12923. https://doi.org/10.3390/ijms232112923
Chicago/Turabian StyleLee, Hyebin, Han Suk Ryu, Hee Chul Park, Jeong Il Yu, Gyu Sang Yoo, Changhoon Choi, Heerim Nam, Jason Joon Bock Lee, In-Gu Do, Dohyun Han, and et al. 2022. "Dual Oxidase 2 (DUOX2) as a Proteomic Biomarker for Predicting Treatment Response to Chemoradiation Therapy for Locally Advanced Rectal Cancer: Using High-Throughput Proteomic Analysis and Machine Learning Algorithm" International Journal of Molecular Sciences 23, no. 21: 12923. https://doi.org/10.3390/ijms232112923
APA StyleLee, H., Ryu, H. S., Park, H. C., Yu, J. I., Yoo, G. S., Choi, C., Nam, H., Lee, J. J. B., Do, I.-G., Han, D., & Ha, S. Y. (2022). Dual Oxidase 2 (DUOX2) as a Proteomic Biomarker for Predicting Treatment Response to Chemoradiation Therapy for Locally Advanced Rectal Cancer: Using High-Throughput Proteomic Analysis and Machine Learning Algorithm. International Journal of Molecular Sciences, 23(21), 12923. https://doi.org/10.3390/ijms232112923