
The Genetic Basis for the Increased Prevalence of Metabolic Syndrome among Post-Traumatic Stress Disorder Patients

 , and
, and
Abstract
1. Introduction
2. Results
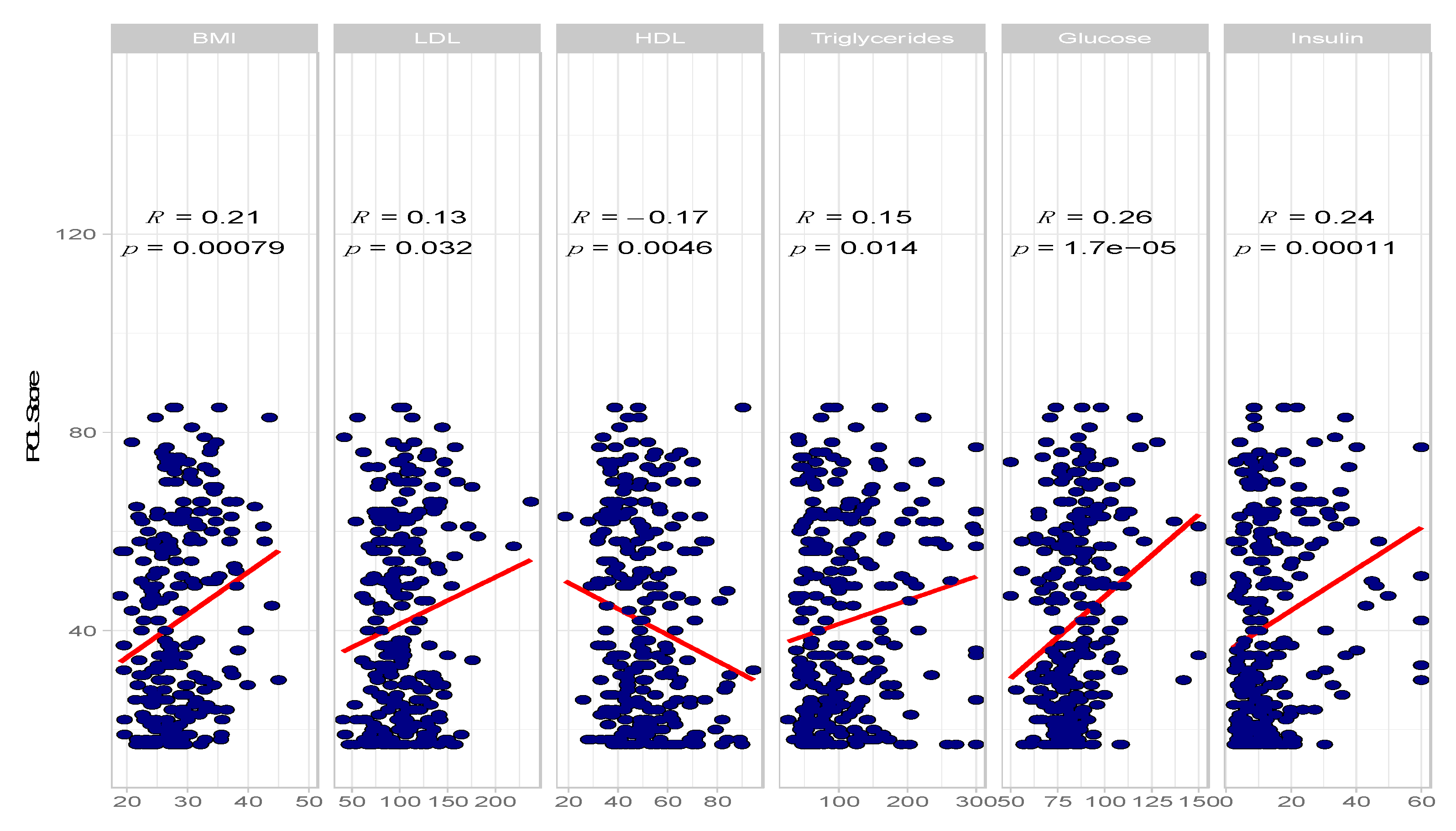
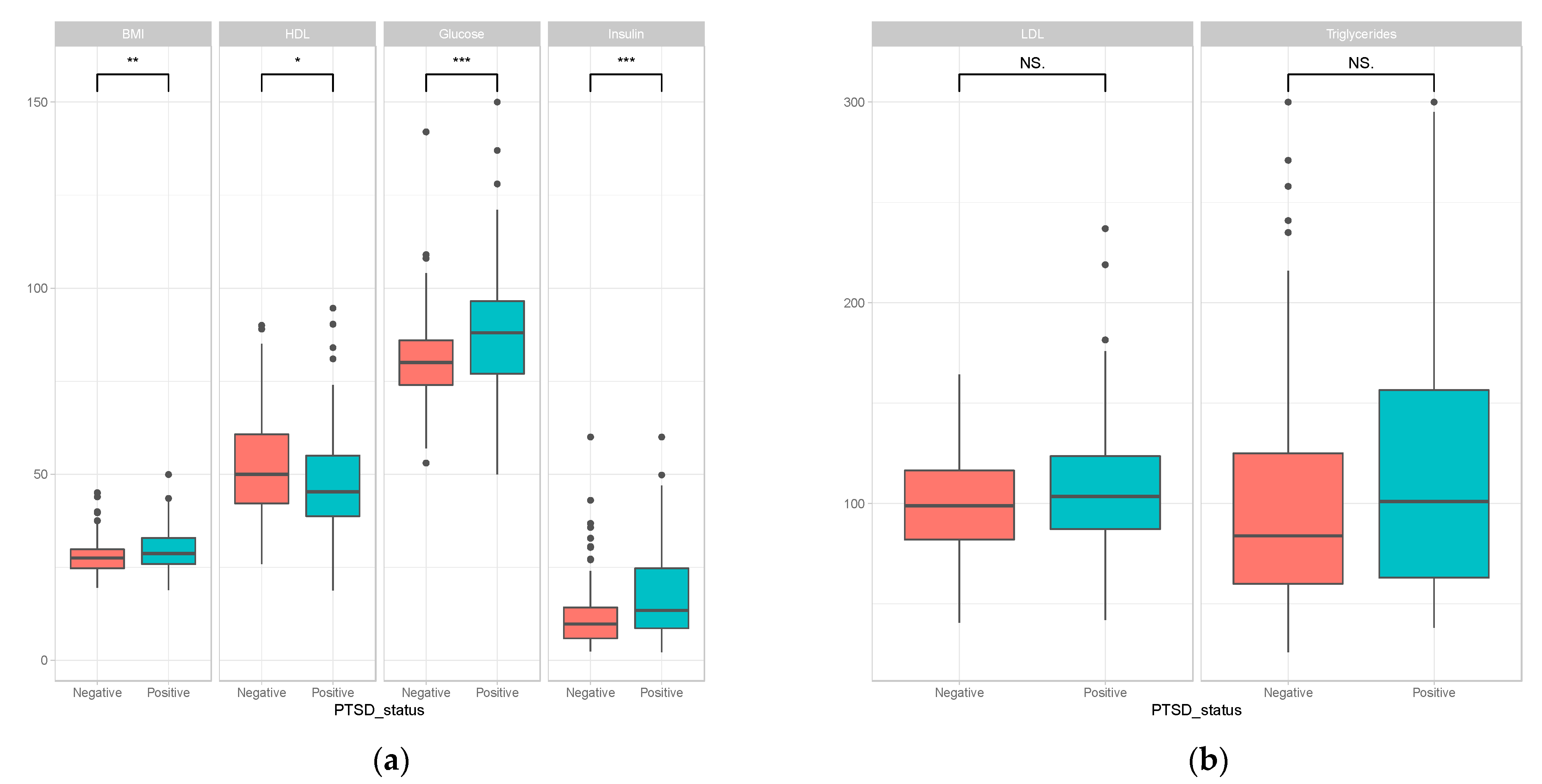
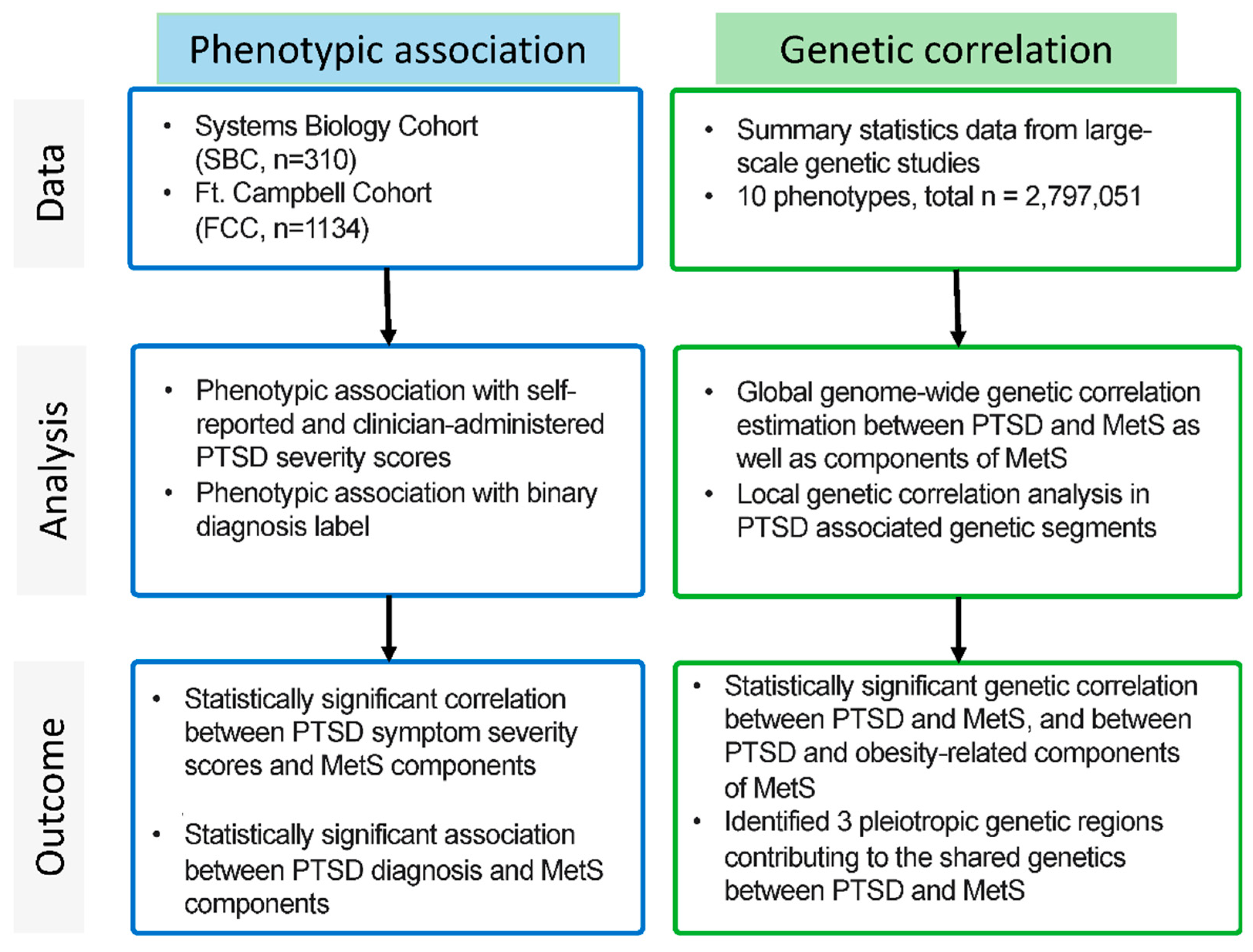
2.1. Association between PTSD Phenotypes and Components of Metabolic Syndrome
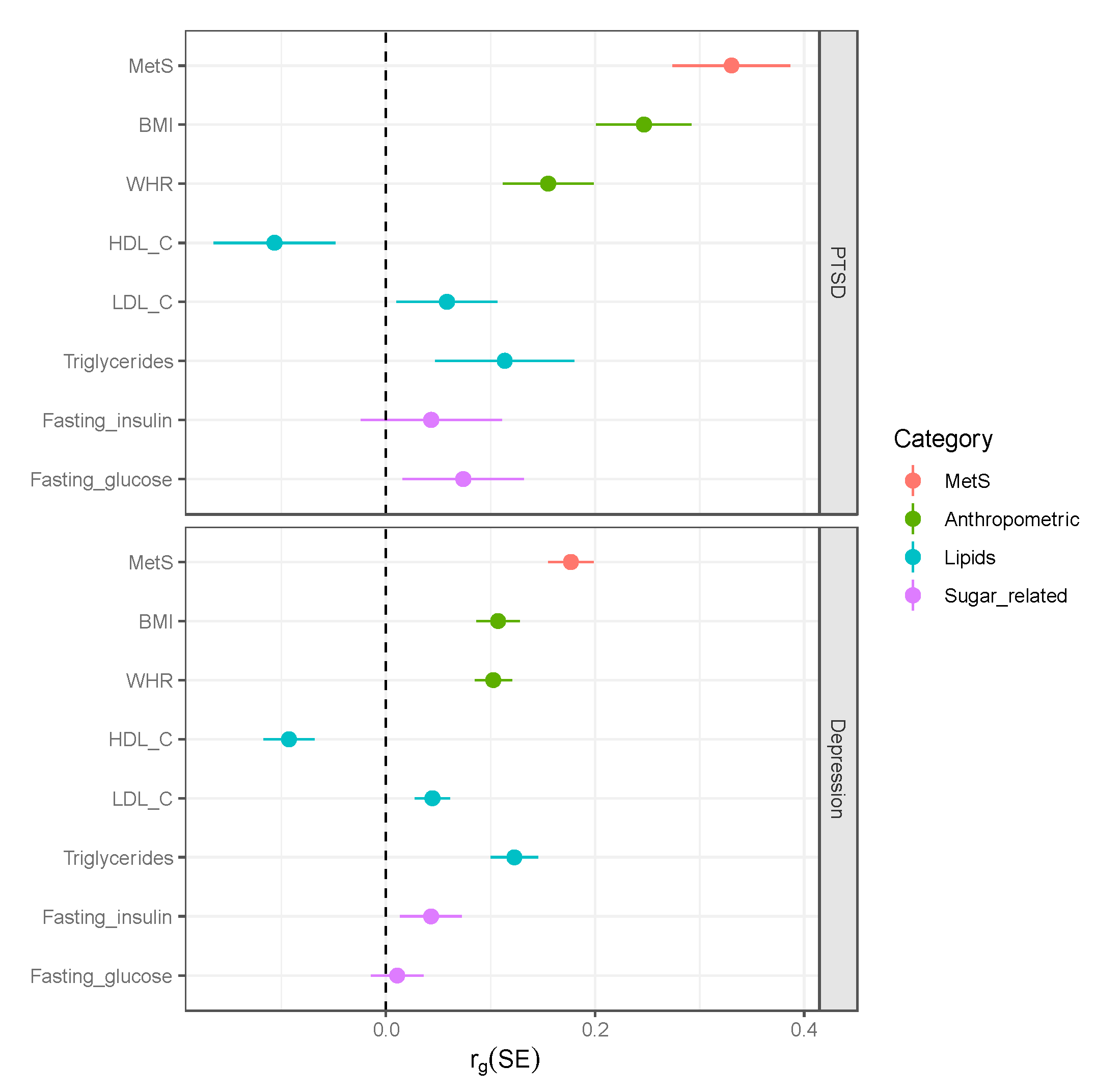
2.2. Genome-Wide Genetic Correlations between PTSD and Metabolic Traits
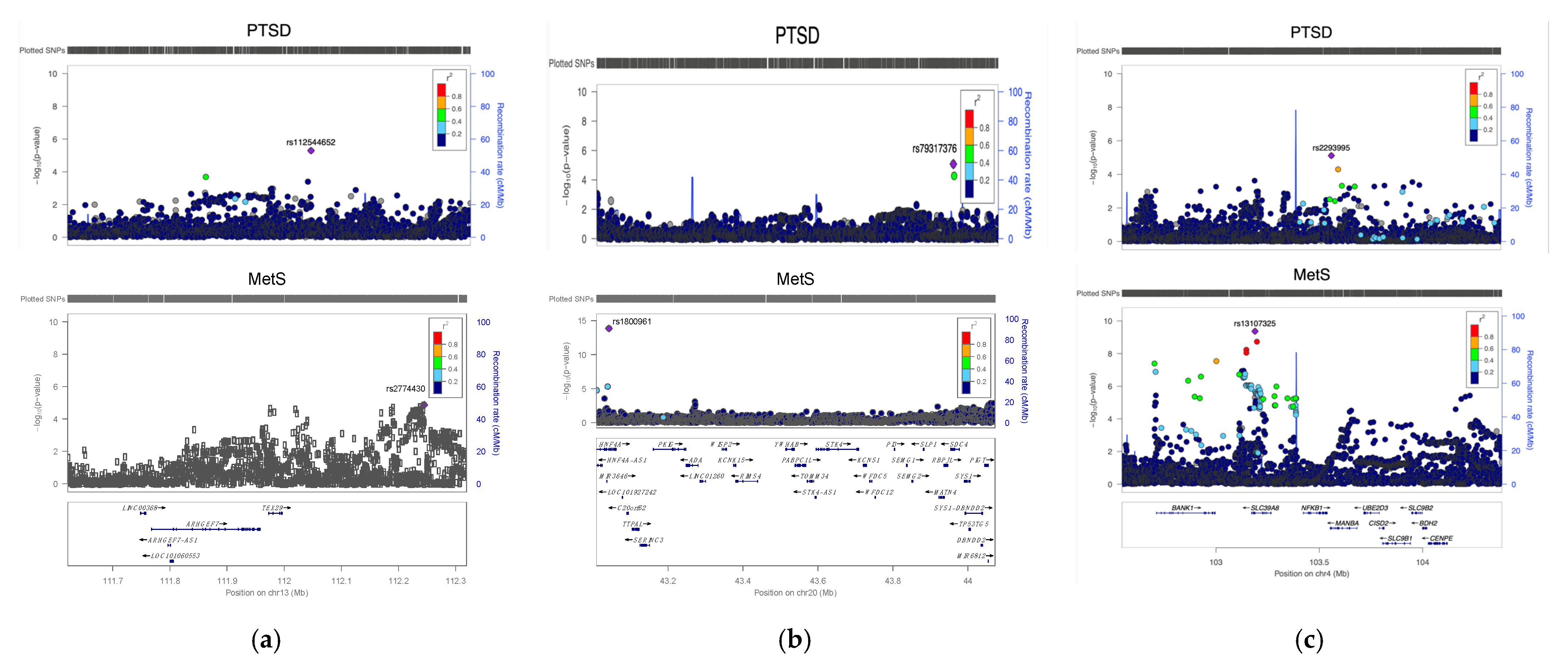
2.3. Genomic Regions with Significant Local Genetic Correlation between PTSD and MetS
2.4. Bidirectional Two-Sample Mendelian Randomization Analysis
3. Discussion
4. Materials and Methods
4.1. Systems Biology Consortuim (SBC) and Fort Campbell Cohort (FCC) Datasets
4.2. GWAS Summary Statistics Data
4.3. Estimating Genome-Wide Genetic Correlations and SNP Heritability
4.4. Estimating Local Genetic Correlations on Independent LD Blocks
4.5. Mendelian Randomization Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Yehuda, R.; Hoge, C.W.; McFarlane, A.C.; Vermetten, E.; Lanius, R.A.; Nievergelt, C.M.; Hobfoll, S.E.; Koenen, K.C.; Neylan, T.C.; Hyman, S.E. Post-traumatic stress disorder. Nat. Rev. Dis. Prim. 2015, 1, 15057. [Google Scholar] [CrossRef] [PubMed]
- Shalev, A.; Liberzon, I.; Marmar, C. Post-traumatic stress disorder. N. Engl. J. Med. 2017, 376, 2459–2469. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Vieweg, W.V.R.; Julius, D.A.; Fernandez, A.; Beatty-Brooks, M.; Hettema, J.M.; Pandurangi, A.K. Posttraumatic stress disorder: Clinical features, pathophysiology, and treatment. Am. J. Med. 2006, 119, 383–390. [Google Scholar] [CrossRef]
- Kulka, R.A.; Schlenger, W.E.; Fairbank, J.A.; Hough, R.L.; Jordan, B.K.; Marmar, C.R.; Weiss, D.S. Trauma and the Vietnam War Generation: Report of Findings from the National Vietnam Veterans Readjustment Study; Brunner/Mazel: New York, NY, USA, 1990. [Google Scholar]
- Ramchand, R.; Karney, B.R.; Osilla, K.C.; Burns, R.M.; Caldarone, L.B. Prevalence of PTSD, depression, and TBI among returning servicemembers. In Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery; Tanielian, T., Jaycox, L.H., Eds.; RAND Corporation: Santa Monica, CA, USA, 2008; pp. 35–86. [Google Scholar]
- Pacella, M.L.; Hruska, B.; Delahanty, D.L. The physical health consequences of PTSD and PTSD symptoms: A meta-analytic review. J. Anxiety Disord. 2013, 27, 33–46. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Stubbs, B.; Ward, P.B.; Steel, Z.; Lederman, O.; Vancampfort, D. The prevalence and risk of metabolic syndrome and its components among people with posttraumatic stress disorder: A systematic review and meta-analysis. Metabolism 2015, 64, 926–933. [Google Scholar] [CrossRef]
- Levesque, J.; Lamarche, B. The metabolic syndrome: Definitions, prevalence and management. J. Nutr. Nutr. 2008, 1, 100–108. [Google Scholar] [CrossRef]
- Mellon, S.H.; Gautam, A.; Hammamieh, R.; Jett, M.; Wolkowitz, O.M. Metabolism, Metabolomics, and Inflammation in Posttraumatic Stress Disorder. Biol. Psychiatry 2018, 83, 866–875. [Google Scholar] [CrossRef]
- Michopoulos, V.; Vester, A.; Neigh, G. Posttraumatic Stress Disorder: A Metabolic Disorder in Disguise? Exp. Neurol. 2016, 284, 220–229. [Google Scholar] [CrossRef]
- Geschwind, D.H.; Flint, J. Genetics and genomics of psychiatric disease. Science 2015, 349, 1489–1494. [Google Scholar] [CrossRef]
- Stander, V.A.; Thomsen, C.J.; Highfill-McRoy, R.M. Etiology of depression comorbidity in combat-related PTSD: A review of the literature. Clin. Psychol. Rev. 2014, 34, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Moradi, Y.; Albatineh, A.N.; Mahmoodi, H.; Gheshlagh, R.G. The relationship between depression and risk of metabolic syndrome: A meta-analysis of observational studies. Clin. Diabetes Endocrinol. 2021, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Gheshlagh, R.G.; Parizad, N.; Sayehmiri, K. The Relationship Between Depression and Metabolic Syndrome: Systematic Review and Meta-Analysis Study. Iran. Red Crescent Med. J. 2016, 18, e26523. [Google Scholar] [CrossRef]
- Zhang, M.; Chen, J.; Yin, Z.; Wang, L.; Peng, L. The association between depression and metabolic syndrome and its components: A bidirectional two-sample Mendelian randomization study. Transl. Psychiatry 2021, 11, 633. [Google Scholar] [CrossRef] [PubMed]
- Nievergelt, C.M.; Maihofer, A.X.; Klengel, T.; Atkinson, E.G.; Chen, C.Y.; Choi, K.W.; Coleman, J.R.I.; Dalvie, S.; Duncan, L.E.; Gelernter, J.; et al. International meta-analysis of PTSD genome-wide association studies identifies sex-and ancestry-specific genetic risk loci. Nat. Commun. 2019, 10, 4558. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Levey, D.F.; Cheng, Z.; Wendt, F.R.; Harrington, K.; Pathak, G.A.; Cho, K.; Quaden, R.; Radhakrishnan, K.; Girgenti, M.J.; et al. Genome-wide association analyses of post-traumatic stress disorder and its symptom subdomains in the Million Veteran Program. Nat. Genet. 2021, 53, 174–184. [Google Scholar] [CrossRef]
- Wray, N.R.; Ripke, S.; Mattheisen, M.; Trzaskowski, M.; Byrne, E.M.; Abdellaoui, A.; Adams, M.J.; Agerbo, E.; Air, T.M.; Andlauer, T.M.F.; et al. Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat. Genet. 2018, 50, 668. [Google Scholar] [CrossRef]
- Lind, L. Genome-Wide Association Study of the Metabolic Syndrome in UK Biobank. Metab. Syndr. Relat. Disord. 2019, 17, 505–511. [Google Scholar] [CrossRef]
- Bartoli, F.; Carrà, G.; Crocamo, C.; Carretta, D.; Clerici, M. Metabolic syndrome in people suffering from posttraumatic stress disorder: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2013, 11, 301–308. [Google Scholar] [CrossRef]
- Kappelmann, N.; Arloth, J.; Georgakis, M.K.; Czamara, D.; Rost, N.; Ligthart, S.; Khandaker, G.M.; Binder, E.B. Dissecting the Association Between Inflammation, Metabolic Dysregulation, and Specific Depressive Symptoms: A Genetic Correlation and 2-Sample Mendelian Randomization Study. JAMA Psychiatry 2021, 78, 161–170. [Google Scholar] [CrossRef]
- Tylee, D.S.; Sun, J.; Hess, J.L.; Tahir, M.A.; Sharma, E.; Malik, R.; Worrall, B.B.; Levine, A.J.; Martinson, J.J.; Nejentsev, S.; et al. Genetic correlations among psychiatric and immune-related phenotypes based on genome-wide association data. Am. J. Med. Genet. Part B Neuropsychiatric Genet. 2018, 177, 641–657. [Google Scholar] [CrossRef]
- Boscarino, J.A. Posttraumatic stress disorder and physical illness: Results from clinical and epidemiologic studies. Ann. N. Y. Acad. Sci. 2004, 1032, 141–153. [Google Scholar] [CrossRef]
- Sodini, S.M.; Kemper, K.E.; Wray, N.R.; Trzaskowski, M. Comparison of Genotypic and Phenotypic Correlations: Cheverud’s Conjecture in Humans. Genetics 2018, 209, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Boscarino, J.A. Posttraumatic stress disorder and mortality among U.S. Army veterans 30 years after military service. Ann. Epidemiol. 2006, 16, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Lambadiari, V.; Dimitriadis, G.; Zampelas, A. Metabolic syndrome and cardiometabolic risk factors. Curr. Vasc. Pharmacol. 2013, 11, 858–879. [Google Scholar] [CrossRef]
- Spinler, S.A. Challenges associated with metabolic syndrome. Pharmacotherapy 2006, 26 Pt 2, 209S–217S. [Google Scholar] [CrossRef]
- Tune, J.D.; Goodwill, A.G.; Sassoon, D.J.; Mather, K.J. Cardiovascular consequences of metabolic syndrome. Transl. Res. J. Lab. Clin. Med. 2017, 183, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Isomaa, B.O.; Almgren, P.; Tuomi, T.; Forsen, B.; Lahti, K.; Nissen, M.; Taskinen, M.R.; Groop, L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef]
- Seligowski, A.V.; Misganaw, B.; Duffy, L.A.; Ressler, K.J.; Guffanti, G. Leveraging Large-Scale Genetics of PTSD and Cardiovascular Disease to Demonstrate Robust Shared Risk and Improve Risk Prediction Accuracy. Am. J. Psychiatry 2022, appiajp21111113. [Google Scholar] [CrossRef]
- Farr, O.M.; Sloan, D.M.; Keane, T.M.; Mantzoros, C.S. Stress- and PTSD-associated obesity and metabolic dysfunction: A growing problem requiring further research and novel treatments. Metabolism 2014, 63, 1463–1468. [Google Scholar] [CrossRef]
- Masodkar, K.; Johnson, J.; Peterson, M.J. A Review of Posttraumatic Stress Disorder and Obesity: Exploring the Link. Prim. Care Companion CNS Disord. 2016, 18, 22710. [Google Scholar] [CrossRef] [PubMed]
- Bharti, V.; Bhardwaj, A.; Elias, D.A.; Metcalfe, A.W.S.; Kim, J.S. A Systematic Review and Meta-Analysis of Lipid Signatures in Post-traumatic Stress Disorder. Front. Psychiatry 2022, 13, 847310. [Google Scholar] [CrossRef] [PubMed]
- Blessing, E.M.; Reus, V.; Mellon, S.H.; Wolkowitz, O.M.; Flory, J.D.; Bierer, L.; Lindqvist, D.; Dhabhar, F.; Li, M.; Qian, M.; et al. Biological predictors of insulin resistance associated with posttraumatic stress disorder in young military veterans. Psychoneuroendocrinology 2017, 82, 91–97. [Google Scholar] [CrossRef]
- Marazziti, D.; Rutigliano, G.; Baroni, S.; Landi, P.; Dell’Osso, L. Metabolic syndrome and major depression. CNS Spectr. 2014, 19, 293–304. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Lange, S.M.M. Metabolic syndrome in psychiatric patients: Overview, mechanisms, and implications. Dialogues Clin. Neurosci. 2018, 20, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Toker, S.; Shirom, A.; Melamed, S. Depression and the metabolic syndrome: Gender-dependent associations. Depress. Anxiety 2008, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Lotta, L.A.; Pietzner, M.; Stewart, I.D.; Wittemans, L.B.; Li, C.; Bonelli, R.; Raffler, J.; Biggs, E.K.; Oliver-Williams, C.; Auyeung, V.P.W.; et al. A cross-platform approach identifies genetic regulators of human metabolism and health. Nat. Genet. 2021, 53, 54–64. [Google Scholar] [CrossRef]
- Shin, S.Y.; Fauman, E.B.; Petersen, A.K.; Krumsiek, J.; Santos, R.; Huang, J.; Arnold, M.; Erte, I.; Forgetta, V.; Yang, T.-P.; et al. An atlas of genetic influences on human blood metabolites. Nat. Genet. 2014, 46, 543–550. [Google Scholar] [CrossRef]
- Mellon, S.H.; Bersani, F.S.; Lindqvist, D.; Hammamieh, R.; Donohue, D.; Dean, K.; Jett, M.; Yehuda, R.; Flory, J.; Reus, V.I.; et al. Metabolomic analysis of male combat veterans with post traumatic stress disorder. PLoS ONE 2019, 14, e0213839. [Google Scholar] [CrossRef]
- Eraly, S.A.; Nievergelt, C.M.; Maihofer, A.X.; Barkauskas, D.A.; Biswas, N.; Agorastos, A.; O’Connor, D.T.; Baker, D.G.; for the Marine Resiliency Study Team. Assessment of plasma C-reactive protein as a biomarker of posttraumatic stress disorder risk. JAMA Psychiatry 2014, 71, 423–431. [Google Scholar] [CrossRef]
- Hagenbeek, F.A.; Pool, R.; van Dongen, J.; Draisma, H.H.; Jan Hottenga, J.; Willemsen, G.; Abdellaoui, A.; Fedko, I.O.; Braber, A.; Visser, P.J.; et al. Heritability estimates for 361 blood metabolites across 40 genome-wide association studies. Nat. Commun. 2020, 11, 39. [Google Scholar] [CrossRef] [PubMed]
- Hübel, C.; Gaspar, H.A.; Coleman, J.R.; Hanscombe, K.B.; Purves, K.; Prokopenko, I.; Graff, M.; Ngwa, J.S.; Workalemahu, T.; ADHD Working Group of the Psychiatric Genomics Consortium; et al. Genetic correlations of psychiatric traits with body composition and glycemic traits are sex- and age-dependent. Nat. Commun. 2019, 10, 5765. [Google Scholar] [CrossRef] [PubMed]
- True, W.R.; Rice, J.; Eisen, S.A.; Heath, A.C.; Goldberg, J.; Lyons, M.J.; Nowak, J. A twin study of genetic and environmental contributions to liability for posttraumatic stress symptoms. Arch. Gen. Psychiatry 1993, 50, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Dean, K.R.; Hammamieh, R.; Mellon, S.H.; Abu-Amara, D.; Flory, J.D.; Guffanti, G.; Wang, K.; Daigle, B.J.; Gautam, A.; Lee, I.; et al. Multi-omic biomarker identification and validation for diagnosing warzone-related post-traumatic stress disorder. Mol. Psychiatry 2020, 25, 3337–3349. [Google Scholar] [CrossRef]
- Misganaw, B.; Guffanti, G.; Lori, A.; Abu-Amara, D.; Flory, J.D.; Mueller, S.; Yehuda, R.; Jett, M.; Marmar, C.R.; Ressler, K.J.; et al. Polygenic risk associated with post-traumatic stress disorder onset and severity. Transl. Psychiatry 2019, 9, 165. [Google Scholar] [CrossRef]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a Clinician-Administered PTSD Scale. J. Trauma. Stress 1995, 8, 75–90. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Schultebraucks, K.; Qian, M.; Abu-Amara, D.; Dean, K.; Laska, E.; Siegel, C.; Gautam, A.; Guffanti, G.; Hammamieh, R.; Misganaw, B.; et al. Pre-deployment risk factors for PTSD in active-duty personnel deployed to Afghanistan: A machine-learning approach for analyzing multivariate predictors. Mol. Psychiatry 2021, 26, 5011–5022. [Google Scholar] [CrossRef]
- Howard, D.M.; Adams, M.J.; Clarke, T.K.; Hafferty, J.D.; Gibson, J.; Shirali, M.; Coleman, J.R.I.; Hagenaars, S.P.; Ward, J.; Wigmore, E.M.; et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat. Neurosci. 2019, 22, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.M.; Adams, M.J.; Shirali, M.; Clarke, T.K.; Marioni, R.E.; Davies, G.; Coleman, J.R.I.; Alloza, C.; Shen, X.; Barbu, M.C.; et al. Genome-wide association study of depression phenotypes in UK Biobank identifies variants in excitatory synaptic pathways. Nat. Commun. 2018, 9, 1470. [Google Scholar] [CrossRef]
- Hoffmann, T.J.; Choquet, H.; Yin, J.; Banda, Y.; Kvale, M.N.; Glymour, M.; Schaefer, C.; Risch, N.; Jorgenson, E. A Large Multiethnic Genome-Wide Association Study of Adult Body Mass Index Identifies Novel Loci. Genetics 2018, 210, 499–515. [Google Scholar] [CrossRef] [PubMed]
- Loh, P.-R.; Kichaev, G.; Gazal, S.; Schoech, A.P.; Price, A.L. Mixed-model association for biobank-scale datasets. Nat. Genet. 2018, 50, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Klimentidis, Y.C.; Arora, A.; Newell, M.; Zhou, J.; Ordovas, J.M.; Renquist, B.J.; Wood, A.C. Phenotypic and Genetic Characterization of Lower LDL Cholesterol and Increased Type 2 Diabetes Risk in the UK Biobank. Diabetes 2020, 69, 2194–2205. [Google Scholar] [CrossRef]
- Richardson, T.G.; Leyden, G.M.; Wang, Q.; Bell, J.A.; Elsworth, B.; Davey Smith, G.; Holmes, M.V. Characterising metabolomic signatures of lipid-modifying therapies through drug target mendelian randomisation. PLoS Biol. 2022, 20, e3001547. [Google Scholar] [CrossRef]
- Chen, J.; Spracklen, C.N.; Marenne, G.; Varshney, A.; Corbin, L.J.; Luan, J.A.; Willems, S.M.; Wu, Y.; Zhang, X.; Horikoshi, M.; et al. The trans-ancestral genomic architecture of glycemic traits. Nat. Genet. 2021, 53, 840–860. [Google Scholar] [CrossRef]
- Bulik-Sullivan, B.K.; Loh, P.R.; Finucane, H.K.; Ripke, S.; Yang, J.; Patterson, N.; Daly, M.J.; Price, A.L.; Neale, B.M. LD Score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat. Genet. 2015, 47, 291–295. [Google Scholar] [CrossRef] [PubMed]
- 1000 Genomes Project Consortium. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Werme, J.; van der Sluis, S.; Posthuma, D.; de Leeuw, C.A. An integrated framework for local genetic correlation analysis. Nat. Genet. 2022, 54, 274–282. [Google Scholar] [CrossRef]
- Pruim, R.J.; Welch, R.P.; Sanna, S.; Teslovich, T.M.; Chines, P.S.; Gliedt, T.P.; Boehnke, M.; Abecasis, G.R.; Willer, C.J. LocusZoom: Regional visualization of genome-wide association scan results. Bioinforma. Oxf. Engl. 2010, 26, 2336–2337. [Google Scholar] [CrossRef] [PubMed]
- Burgess, S.; Butterworth, A.; Thompson, S.G. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet. Epidemiol. 2013, 37, 658–665. [Google Scholar] [CrossRef]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife 2018, 7, e34408. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pearson Correlation | Spearman Rank Correlation | ||||
|---|---|---|---|---|---|
| var1 | var2 | r | p | r | p |
| CAPS | BMI | 0.22 | 3.58E-04 | 0.26 | 1.45E-06 |
| CAPS | LDL-C | 0.14 | 1.82E-02 | 0.14 | 2.08E-02 |
| CAPS | HDL-C | −0.17 | 4.42E-03 | −0.17 | 3.92E-03 |
| CAPS | Triglycerides | 0.12 | 5.30E-02 | 0.14 | 2.10E-02 |
| CAPS | Glucose | 0.25 | 2.15E-05 | 0.37 | 3.34E-10 |
| CAPS | Insulin | 0.29 | 1.10E-06 | 0.35 | 2.63E-09 |
| Phenotype | rg | SE | p |
|---|---|---|---|
| MetS | 0.3305 | 0.0564 | 4.74E-09 |
| BMI | 0.2467 | 0.0456 | 6.42E-08 |
| WHR | 0.1551 | 0.0434 | 3.56E-04 |
| HDL-C | −0.1067 | 0.0582 | 6.66E-02 |
| LDL-C | 0.0583 | 0.0482 | 2.26E-01 |
| Triglycerides | 0.1135 | 0.0667 | 8.90E-02 |
| Insulin | 0.0432 | 0.0676 | 5.23E-01 |
| Glucose | 0.0739 | 0.0581 | 2.04E-01 |
| Negative (n = 164) | Positive (n = 146) | Overall (n = 310) | |
|---|---|---|---|
| CAPS total score | |||
| Mean (SD) | 4.00 (5.14) | 68.1 (18.2) | 34.2 (34.6) |
| Median [Min, Max] | 2.00 [0, 19.0] | 66.0 [24.0, 114] | 15.5 [0, 114] |
| PCL toral score | |||
| Mean (SD) | 25.5 (9.04) | 59.6 (12.9) | 41.9 (20.3) |
| Median [Min, Max] | 23.0 [17.0, 62.0] | 61.0 [25.0, 85.0] | 37.0 [17.0, 85.0] |
| Missing | 24 (14.6%) | 16 (11.0%) | 40 (12.9%) |
| BDI total score | |||
| Mean (SD) | 5.85 (6.46) | 24.3 (11.0) | 14.9 (12.9) |
| Median [Min, Max] | 3.00 [0, 28.0] | 24.0 [0, 56.0] | 13.0 [0, 56.0] |
| Missing | 24 (14.6%) | 11 (7.5%) | 35 (11.3%) |
| Gender | |||
| Female | 29 (17.7%) | 25 (17.1%) | 54 (17.4%) |
| Male | 135 (82.3%) | 121 (82.9%) | 256 (82.6%) |
| Age | |||
| Mean (SD) | 33.1 (7.90) | 33.5 (7.96) | 33.3 (7.91) |
| Median [Min, Max] | 30.0 [20.0, 59.0] | 31.0 [23.0, 59.0] | 31.0 [20.0, 59.0] |
| Missing | 23 (14.0%) | 25 (17.1%) | 48 (15.5%) |
| Ethnicity | |||
| Asian | 12 (7.3%) | 4 (2.7%) | 16 (5.2%) |
| Black | 41 (25.0%) | 49 (33.6%) | 90 (29.0%) |
| White | 76 (46.3%) | 53 (36.3%) | 129 (41.6%) |
| Other | 12 (7.3%) | 15 (10.3%) | 27 (8.7%) |
| Missing | 23 (14.0%) | 25 (17.1%) | 48 (15.5%) |
| BMI | |||
| Mean (SD) | 27.9 (4.51) | 29.5 (5.49) | 28.6 (5.07) |
| Median [Min, Max] | 27.5 [19.5, 45.0] | 28.6 [18.9, 49.9] | 27.9 [18.9, 49.9] |
| Missing | 27 (16.5%) | 15 (10.3%) | 42 (13.5%) |
| HDL-C | |||
| Mean (SD) | 52.0 (13.8) | 48.4 (12.9) | 50.3 (13.5) |
| Median [Min, Max] | 50.0 [25.9, 90.0] | 45.6 [18.8, 94.6] | 48.8 [18.8, 94.6] |
| Missing | 21 (12.8%) | 15 (10.3%) | 36 (11.6%) |
| LDL-C | |||
| Mean (SD) | 99.8 (25.4) | 107 (31.5) | 103 (28.6) |
| Median [Min, Max] | 99.0 [40.6, 164] | 103 [42.0, 237] | 100 [40.6, 237] |
| Missing | 21 (12.8%) | 17 (11.6%) | 38 (12.3%) |
| Triglycerides | |||
| Mean (SD) | 107 (83.3) | 122 (82.6) | 114 (83.2) |
| Median [Min, Max] | 84.0 [26.0, 718] | 101 [38.0, 492] | 92.0 [26.0, 718] |
| Missing | 21 (12.8%) | 14 (9.6%) | 35 (11.3%) |
| Glucose | |||
| Mean (SD) | 80.5 (11.7) | 91.1 (28.4) | 85.6 (22.0) |
| Median [Min, Max] | 80.0 [53.0, 142] | 88.0 [50.0, 309] | 83.0 [50.0, 309] |
| Missing | 21 (12.8%) | 14 (9.6%) | 35 (11.3%) |
| Insulin | |||
| Mean (SD) | 11.6 (8.84) | 18.8 (16.5) | 15.1 (13.6) |
| Median [Min, Max] | 9.75 [2.40, 67.4] | 13.3 [2.20, 108] | 11.1 [2.20, 108] |
| Missing | 22 (13.4%) | 14 (9.6%) | 36 (11.6%) |
| Category | Sum. Data | Phenotype | Sample Size | Source Reference | |
|---|---|---|---|---|---|
| PSY | PTSD (PGC-freeeze-2) | PTSD | 174,659 | 6.50% | [18] |
| Depression (PGC+UKBB) | depression | 500,199 | 6.10% | [52] | |
| MetS | MetS (UKBB) | metabolic syndrome | 291,107 | 9.20% | [21] |
| Anthropometric | BMI | Body mass index | 315,347 | 16.70% | [54] |
| WHR | Waist-to-hip ratio | 502,773 | 13.50% | [55] | |
| Lipids | LDL-C | LDL-C | 431,167 | 18.20% | [56] |
| HDL-C (UKBB) | HDL-C | 115,082 | 16.80% | [57] | |
| Triglycerides | Triglycerides | 115,082 | 19.70% | [57] | |
| Sugar related | Glucose (GIANT) | fasting blood glucose | 200,622 | 8.30% | [58] |
| Insulin (MAGIC) | Fasting insulin | 151,013 | 8.10% | [58] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Misganaw, B.; Yang, R.; Gautam, A.; Muhie, S.; Mellon, S.H.; Wolkowitz, O.M.; Ressler, K.J.; Doyle, F.J., III; Marmar, C.R.; Jett, M.; et al. The Genetic Basis for the Increased Prevalence of Metabolic Syndrome among Post-Traumatic Stress Disorder Patients. Int. J. Mol. Sci. 2022, 23, 12504. https://doi.org/10.3390/ijms232012504
Misganaw B, Yang R, Gautam A, Muhie S, Mellon SH, Wolkowitz OM, Ressler KJ, Doyle FJ III, Marmar CR, Jett M, et al. The Genetic Basis for the Increased Prevalence of Metabolic Syndrome among Post-Traumatic Stress Disorder Patients. International Journal of Molecular Sciences. 2022; 23(20):12504. https://doi.org/10.3390/ijms232012504
Chicago/Turabian StyleMisganaw, Burook, Ruoting Yang, Aarti Gautam, Seid Muhie, Synthia H. Mellon, Owen M. Wolkowitz, Kerry J. Ressler, Francis J. Doyle, III, Charles R. Marmar, Marti Jett, and et al. 2022. "The Genetic Basis for the Increased Prevalence of Metabolic Syndrome among Post-Traumatic Stress Disorder Patients" International Journal of Molecular Sciences 23, no. 20: 12504. https://doi.org/10.3390/ijms232012504
APA StyleMisganaw, B., Yang, R., Gautam, A., Muhie, S., Mellon, S. H., Wolkowitz, O. M., Ressler, K. J., Doyle, F. J., III, Marmar, C. R., Jett, M., & Hammamieh, R. (2022). The Genetic Basis for the Increased Prevalence of Metabolic Syndrome among Post-Traumatic Stress Disorder Patients. International Journal of Molecular Sciences, 23(20), 12504. https://doi.org/10.3390/ijms232012504