
Efficacy and Safety of Ginger on the Side Effects of Chemotherapy in Breast Cancer Patients: Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Results
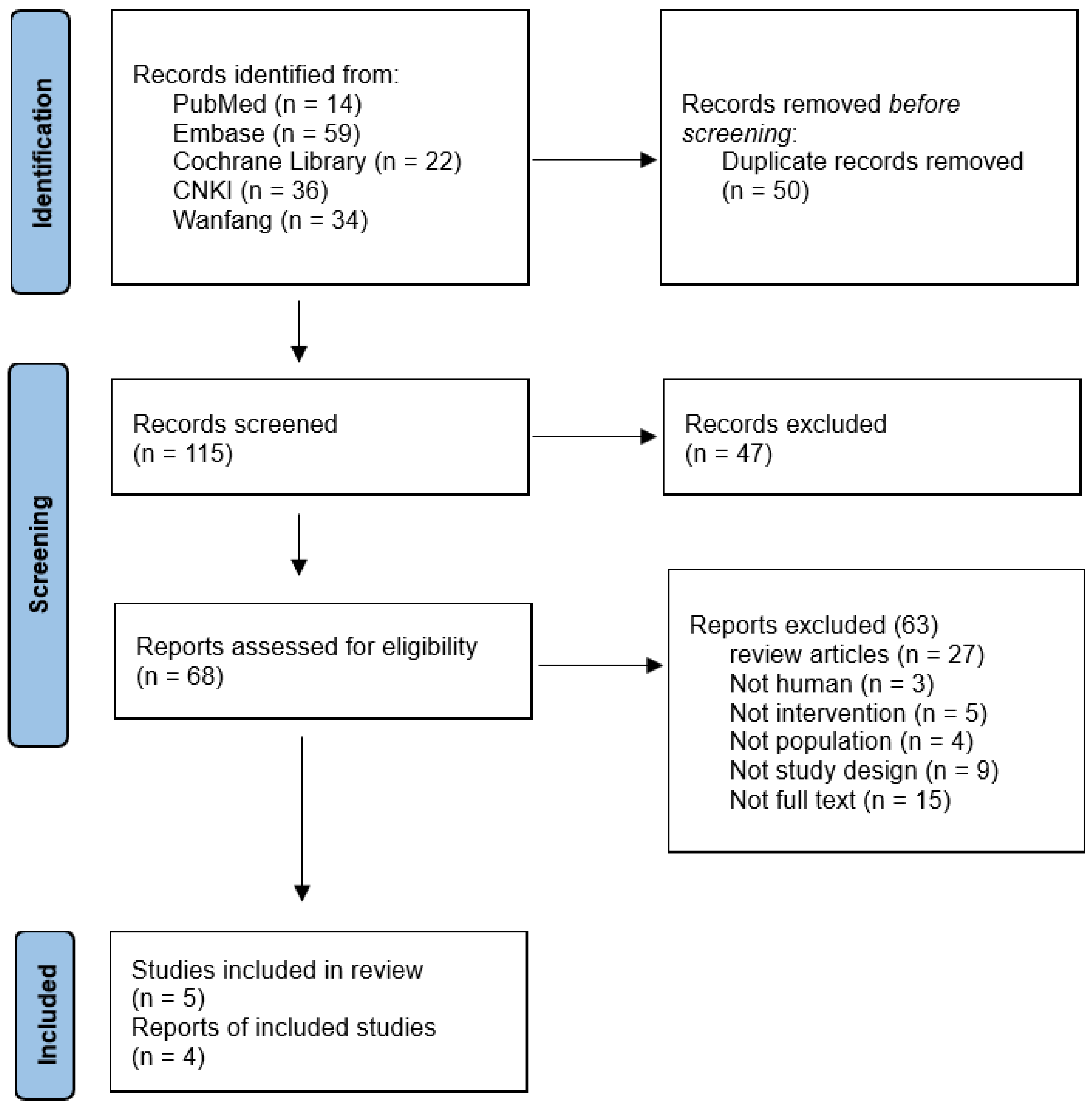
2.1. Literature Search Results
2.2. Characteristics of Included Studies
2.3. Risk of Bias Associated with Included Trials
2.4. Effects of Ginger Intake in Managing CINV on Breast Cancer Patients
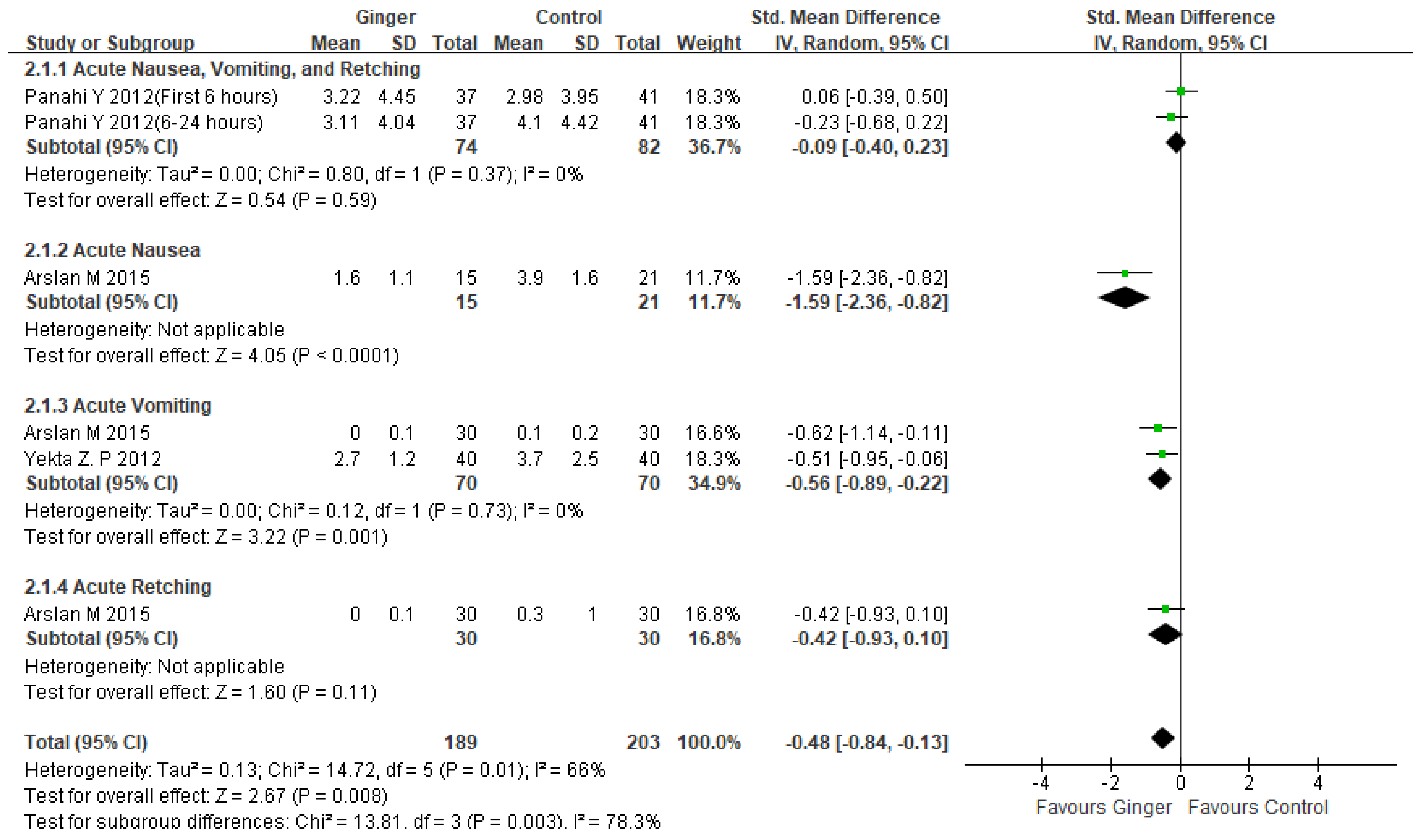
2.4.1. Effects of Ginger Intake in Managing Acute CINV on Breast Cancer Patients
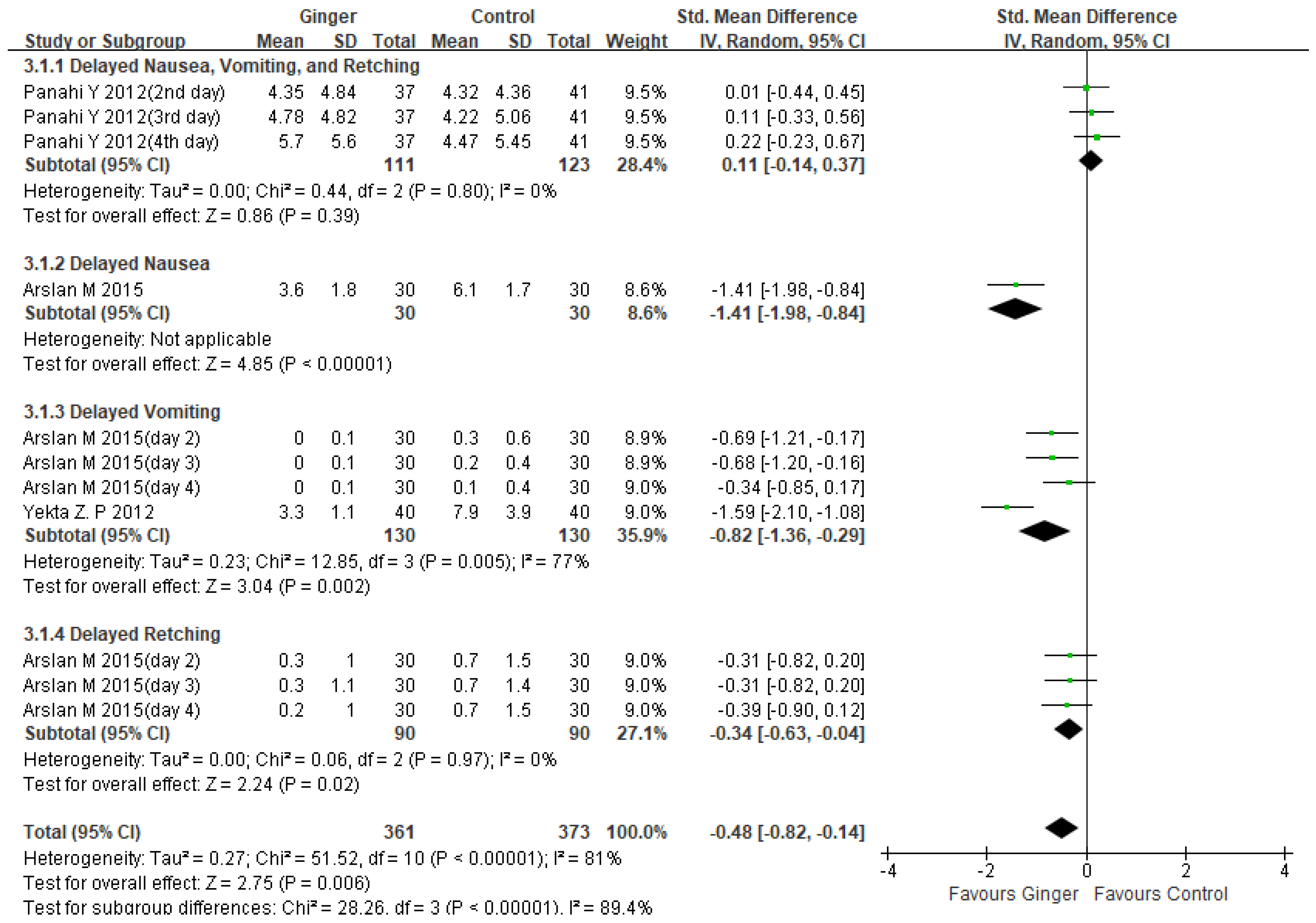
2.4.2. Effects of Ginger Intake in Managing Delayed CINV on Breast Cancer Patients
2.5. Safety
3. Discussion
4. Limitations
5. Methods
5.1. Objective
5.2. Criteria to Select Articles
5.3. Search Strategy, Data Selection, and Data Extraction
5.4. Risk of Bias
5.5. Meta-Analysis
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Adel, N. Overview of chemotherapy-induced nausea and vomiting and evidence-based therapies. Am. J. Manag. Care 2017, 23 (Suppl. 14), S259–S265. [Google Scholar]
- Natale, J.J. Overview of the prevention and management of CINV. Am. J. Manag. Care 2018, 24 (Suppl. 18), S391–S397. [Google Scholar]
- Wood, D.E.; Kazerooni, E.A.; Baum, S.L.; Eapen, G.A.; Ettinger, D.S.; Hou, L.; Jackman, D.M.; Klippenstein, D.; Kumar, R.; Lackner, R.P.; et al. Lung Cancer Screening, Version 3.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 412–441. [Google Scholar] [CrossRef]
- Vardy, J.; Chiew, K.S.; Galica, J.; Pond, G.R.; Tannock, I.F. Side effects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br. J. Cancer 2006, 94, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Razvi, Y.; Chan, S.; McFarlane, T.; McKenzie, E.; Zaki, P.; DeAngelis, C.; Pidduck, W.; Bushehri, A.; Chow, E.; Jerzak, K.J. ASCO, NCCN, MASCC/ESMO: A comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in adult patients. Support. Care Cancer 2019, 27, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Baliga, M.S.; Haniadka, R.; Pereira, M.M.; D’Souza, J.J.; Pallaty, P.L.; Bhat, H.P.; Popuri, S. Update on the chemopreventive effects of ginger and its phytochemicals. Crit. Rev. Food Sci. Nutr. 2011, 51, 499–523. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Ried, K.; McCarthy, A.L.; Vitetta, L.; Sali, A.; McKavanagh, D.; Isenring, L. Ginger-Mechanism of action in chemotherapy-induced nausea and vomiting: A review. Crit. Rev. Food Sci. Nutr. 2017, 57, 141–146. [Google Scholar] [CrossRef]
- Navari, R.M.; Qin, R.; Ruddy, K.J.; Liu, H.; Powell, S.F.; Bajaj, M.; Dietrich, L.; Biggs, D.; Lafky, J.M.; Loprinzi, C.L. Olanzapine for the Prevention of Chemotherapy-Induced Nausea and Vomiting. N. Engl. J. Med. 2016, 375, 134–142. [Google Scholar] [CrossRef]
- Rapoport, B.L. Delayed Chemotherapy-Induced Nausea and Vomiting: Pathogenesis, Incidence, and Current Management. Front. Pharmacol. 2017, 8, 19. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Tejani, M.A.; Kamen, C.; Peoples, A.R.; Mustian, K.M.; Morrow, G.R. Current pharmacotherapy for chemotherapy-induced nausea and vomiting in cancer patients. Expert Opin. Pharmacother. 2013, 14, 757–766. [Google Scholar] [CrossRef]
- Yamahara, J.; Rong, H.Q.; Iwamoto, M.; Kobayashi, G.; Matsuda, H.; Fujimura, H. Active components of ginger exhibiting anti-serotonergic action. Phytother. Res. 1989, 3, 70–71. [Google Scholar] [CrossRef]
- Abdel-Aziz, H.; Windeck, T.; Ploch, M.; Verspohl, E.J. Mode of action of gingerols and shogaols on 5-HT3 receptors: Binding studies, cation uptake by the receptor channel and contraction of isolated guinea-pig ileum. Eur. J. Pharmacol. 2006, 530, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Bossi, P.; Cortinovis, D.; Fatigoni, S.; Cossu Rocca, M.; Fabi, A.; Seminara, P.; Ripamonti, C.; Alfieri, S.; Granata, R.; Bergamini, C.; et al. A randomized, double-blind, placebo-controlled, multicenter study of a ginger extract in the management of chemotherapy-induced nausea and vomiting (CINV) in patients receiving high-dose cisplatin. Ann. Oncol. 2017, 28, 2547–2551. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; McCarthy, A.L.; Ried, K.; McKavanagh, D.; Vitetta, L.; Sali, A.; Lohning, A.; Isenring, E. The Effect of a Standardized Ginger Extract on Chemotherapy-Induced Nausea-Related Quality of Life in Patients Undergoing Moderately or Highly Emetogenic Chemotherapy: A Double Blind, Randomized, Placebo Controlled Trial. Nutrients 2017, 9, 867. [Google Scholar] [CrossRef] [PubMed]
- Pillai, A.K.; Sharma, K.K.; Gupta, Y.K.; Bakhshi, S. Anti-emetic effect of ginger powder versus placebo as an add-on therapy in children and young adults receiving high emetogenic chemotherapy. Pediatr. Blood Cancer 2011, 56, 234–238. [Google Scholar] [CrossRef]
- Martin, A.; Fuzer, A.M.; Becceneri, A.B.; da Silva, J.A.; Tomasin, R.; Denoyer, D.; Kim, S.H.; McIntyre, K.A.; Pearson, H.B.; Yeo, B.; et al. [10]-gingerol induces apoptosis and inhibits metastatic dissemination of triple negative breast cancer In Vivo. Oncotarget 2017, 8, 72260–72271. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, S.; Meng, X.; Gan, R.-Y.; Zhang, J.-J.; Li, H.-B. Dietary Natural Products for Prevention and Treatment of Breast Cancer. Nutrients 2017, 9, 728. [Google Scholar] [CrossRef] [PubMed]
- Elkady, A.I.; Abuzinadah, O.A.; Baeshen, N.A.; Rahmy, T.R. Differential control of growth, apoptotic activity, and gene expression in human breast cancer cells by extracts derived from medicinal herbs Zingiber officinale. J. Biomed. Biotechnol. 2012, 2012, 614356. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.P.; Peng, Y.X. Does the Oral Administration of Ginger Reduce Chemotherapy-Induced Nausea and Vomiting?: A Meta-analysis of 10 Randomized Controlled Trials. Cancer Nurs. 2019, 42, E14–E23. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, Ed000142. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.; Porouhan, P.; Mohammadianpanah, M.; Omidvari, S.; Mosalaei, A.; Ahmadloo, N.; Nasrollahi, H.; Hamedi, S.H. Efficacy of Ginger in Control of Chemotherapy Induced Nausea and Vomiting in Breast Cancer Patients Receiving Doxorubicin-Based Chemotherapy. Asian Pac. J. Cancer Prev. 2016, 17, 3877–3880. [Google Scholar] [PubMed]
- Arslan, M.; Ozdemir, L. Oral intake of ginger for chemotherapy-induced nausea and vomiting among women with breast cancer. Clin. J. Oncol. Nurs. 2015, 19, E92–E97. [Google Scholar] [CrossRef]
- Panahi, Y.; Saadat, A.; Sahebkar, A.; Hashemian, F.; Taghikhani, M.; Abolhasani, E. Effect of ginger on acute and delayed chemotherapy-induced nausea and vomiting: A pilot, randomized, open-label clinical trial. Integr. Cancer Ther. 2012, 11, 204–211. [Google Scholar] [CrossRef]
- Yekta, Z.P.; Ebrahimi, S.M.; Hosseini, M.; Nasrabadi, A.N.; Sedighi, S.; Surmaghi, M.H.; Madani, H. Ginger as a miracle against chemotherapy-induced vomiting. Iran. J. Nurs. Midwifery Res. 2012, 17, 325–329. [Google Scholar] [PubMed]
- Liu, C.; Su, Y.; Zhao, M.; You, H.; Wang, X. Curative effects of ginger combined with tropisetron on chemotherapy-induced nausea and vomiting of breast cancer. Chin. J. Mod. Nurs. 2020, 26, 4657–4660. [Google Scholar] [CrossRef]
- Gupta, K.; Walton, R.; Kataria, S.P. Chemotherapy-Induced Nausea and Vomiting: Pathogenesis, Recommendations, and New Trends. Cancer Treat. Res. Commun. 2021, 26, 100278. [Google Scholar] [CrossRef] [PubMed]
- Navari, R.M.; Aapro, M. Antiemetic Prophylaxis for Chemotherapy-Induced Nausea and Vomiting. N. Engl. J. Med. 2016, 374, 1356–1367. [Google Scholar] [CrossRef]
- Palatty, P.L.; Haniadka, R.; Valder, B.; Arora, R.; Baliga, M.S. Ginger in the prevention of nausea and vomiting: A review. Crit. Rev. Food Sci. Nutr. 2013, 53, 659–669. [Google Scholar] [CrossRef]
- Uthaipaisanwong, A.; Oranratanaphan, S.; Musigavong, N. Effects of ginger adjunct to the standard prophylaxis on reducing carboplatin and paclitaxel-induced nausea vomiting: A randomized controlled study. Support. Care Cancer 2020, 28, 3831–3838. [Google Scholar] [CrossRef]
- Levine, M.E.; Gillis, M.G.; Koch, S.Y.; Voss, A.C.; Stern, R.M.; Koch, K.L. Protein and ginger for the treatment of chemotherapy-induced delayed nausea. J. Altern. Complement. Med. 2008, 14, 545–551. [Google Scholar] [CrossRef]
- Semwal, R.B.; Semwal, D.K.; Combrinck, S.; Viljoen, A.M. Gingerols and shogaols: Important nutraceutical principles from ginger. Phytochemistry 2015, 117, 554–568. [Google Scholar] [CrossRef]
- Al Kury, L.T.; Mahgoub, M.; Howarth, F.C.; Oz, M. Natural Negative Allosteric Modulators of 5-HT3 Receptors. Molecules 2018, 23, 3186. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Qin, Z.; Yao, Q.; Wang, Y.; Liu, Z. Moxibustion for Chemotherapy-Induced Nausea and Vomiting: A Systematic Review and Meta-Analysis. Evid. Based Complement. Alternat. Med. 2017, 2017, 9854893. [Google Scholar] [CrossRef]
- Liu, Y.Q.; Sun, S.; Dong, H.J.; Zhai, D.X.; Zhang, D.Y.; Shen, W.; Bai, L.L.; Yu, J.; Zhou, L.H.; Yu, C.Q. Wrist-ankle acupuncture and ginger moxibustion for preventing gastrointestinal reactions to chemotherapy: A randomized controlled trial. Chin. J. Integr. Med. 2015, 21, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Toniolo, J.; Delaide, V.; Beloni, P. Effectiveness of Inhaled Aromatherapy on Chemotherapy-Induced Nausea and Vomiting: A Systematic Review. J. Altern. Complement. Med. 2021, 27, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.; Grunberg, S. Chemotherapy-induced nausea and vomiting: Challenges and opportunities for improved patient outcomes. Clin. J. Oncol. Nurs. 2009, 13, 54–64. [Google Scholar] [CrossRef]
- Tina Shih, Y.C.; Xu, Y.; Elting, L.S. Costs of uncontrolled chemotherapy-induced nausea and vomiting among working-age cancer patients receiving highly or moderately emetogenic chemotherapy. Cancer 2007, 110, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Ansari, J.A.; Ahmad, M.K.; Khan, A.R.; Fatima, N.; Khan, H.J.; Rastogi, N.; Mishra, D.P.; Mahdi, A.A. Anticancer and Antioxidant activity of Zingiber officinale Roscoe rhizome. Indian J. Exp. Biol. 2016, 54, 767–773. [Google Scholar]
- Joo, J.H.; Hong, S.S.; Cho, Y.R.; Seo, D.W. 10-Gingerol inhibits proliferation and invasion of MDA-MB-231 breast cancer cells through suppression of Akt and p38MAPK activity. Oncol. Rep. 2016, 35, 779–784. [Google Scholar] [CrossRef]
- Lee, H.S.; Seo, E.Y.; Kang, N.E.; Kim, W.K. [6]-Gingerol inhibits metastasis of MDA-MB-231 human breast cancer cells. J. Nutr. Biochem. 2008, 19, 313–319. [Google Scholar] [CrossRef]
- Ling, H.; Yang, H.; Tan, S.H.; Chui, W.K.; Chew, E.H. 6-Shogaol, an active constituent of ginger, inhibits breast cancer cell invasion by reducing matrix metalloproteinase-9 expression via blockade of nuclear factor-κB activation. Br. J. Pharmacol. 2010, 161, 1763–1777. [Google Scholar] [CrossRef]
- Hong, B.H.; Wu, C.H.; Yeh, C.T.; Yen, G.C. Invadopodia-associated proteins blockade as a novel mechanism for 6-shogaol and pterostilbene to reduce breast cancer cell motility and invasion. Mol. Nutr. Food Res. 2013, 57, 886–895. [Google Scholar] [CrossRef]
- Ray, A.; Vasudevan, S.; Sengupta, S. 6-Shogaol Inhibits Breast Cancer Cells and Stem Cell-Like Spheroids by Modulation of Notch Signaling Pathway and Induction of Autophagic Cell Death. PLoS ONE 2015, 10, e0137614. [Google Scholar] [CrossRef]
- Hsu, Y.L.; Chen, C.Y.; Hou, M.F.; Tsai, E.M.; Jong, Y.J.; Hung, C.H.; Kuo, P.L. 6-Dehydrogingerdione, an active constituent of dietary ginger, induces cell cycle arrest and apoptosis through reactive oxygen species/c-Jun N-terminal kinase pathways in human breast cancer cells. Mol. Nutr. Food Res. 2010, 54, 1307–1317. [Google Scholar] [CrossRef]
- Lua, P.L.; Salihah, N.; Mazlan, N. Effects of inhaled ginger aromatherapy on chemotherapy-induced nausea and vomiting and health-related quality of life in women with breast cancer. Complement. Ther. Med. 2015, 23, 396–404. [Google Scholar] [CrossRef]
- Lee, J.; Oh, H. Ginger as an antiemetic modality for chemotherapy-induced nausea and vomiting: A systematic review and meta-analysis. Oncol. Nurs. Forum 2013, 40, 163–170. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Age | Chemotherapy Drugs | Sample Size | Intervention | Control | Duration | Primary Results | Adverse Effects |
|---|---|---|---|---|---|---|---|---|---|
| Panahi 2012 [25] | Open-label RCT | 51.8 | Docetaxel, epirubicin, cyclophosphamide | E:37 C:41 | Powdered ginger root capsule 1.5 g/d in 3 divided doses every 8 h, antiemetic regimen | Antiemetic regimen (granisetron + dexamethason) | 4 days | Ginger was observed no significant advantage on the prevalence or severity of acute or delayed CINV | Heartburn, headache, and vertigo |
| Yekta 2012 [26] | Double-blind placebo RCT | E:41.8 C:45.1 | Not reported | E:40 C:40 | Powdered ginger root capsule 1.0 g/d with 6 h, four times a day, antiemetic regimen | Placebo, antiemetic regimen (granisetron + dexamethason) | 6 days | Ginger group showed significantly lower vomiting cases of anticipatory, acute, and delayed phases | Heartburn; Anticipatory: E:4, C:1; Acute: E:5, C:0; Delayed E:2, C:0 |
| Arslan 2015 [24] | RCT | 48.5 | Anthracycline-Based Chemotherapy | E:30 C:30 | 500 mg powdered ginger, mixed with a yogurt, twice a day, antiemetic | 5-HT3 antagonist, dexamethasone, antihistamine, ranitidine, aprepitant | 3 days | Significantly lower severity of nausea and cases of vomiting in the ginger group than in control group | No adverse effects |
| Ansari 2016 [23] | RCT | 48.6 | Doxorubicin-Based Chemotherapy | E:57 C:62 | 2 Powdered ginger (250 mg per one capsule) capsules every 13 h | Placebo (starch capsule) | 3 days | Ginger group exhibited no significant benefits to the severity of nausea and vomiting | No adverse effects |
| Liu 2020 [27] | RCT | E:51.6 C:52.1 | Anthracycline-Based Chemotherapy, cyclophosphamide | E:40 C:40 | Slices of fresh ginger under the tongue 30 min before chemotherapy, applied to acupoint, antiemetic | 5-HT3 antagonist | 5 days | Ginger group effectively alleviate chemotherapy-induced nausea and vomiting symptoms | Not reported |
| PubMed | (“CINV”[Title/Abstract] OR “chemotherapy induced nausea and vomiting”[Title/Abstract] OR “Vomiting”[MeSH Terms] OR “Nausea”[MeSH Terms] OR “Vomiting”[Title/Abstract] OR “Nausea”[Title/Abstract]) AND (“breast cancer”[Title/Abstract] OR “breast neoplasms”[Title/Abstract] OR “breast neoplasms”[MeSH Terms]) AND (“ginger”[Title/Abstract] OR “ginger”[MeSH Terms] OR “zingiber officinale”[Title/Abstract] OR “ShengJiang”[Title/Abstract] OR “Zingiberis Rhizoma Recens”[Title/Abstract]) |
| Embase | (‘breast neoplasms’/exp OR ‘breast neoplasms’:ti,ab,kw OR ‘breast cancer’:ti,ab,kw) AND (‘cinv’/exp OR ‘cinv’:ti,ab,kw OR ‘chemotherapy induced nausea and vomiting’:ti,ab,kw OR ‘vomiting’/exp OR ‘nausea’/exp OR ‘vomiting’:ti,ab,kw OR ‘nausea’:ti,ab,kw) AND (‘ginger’/exp OR ‘ginger’:ti,ab,kw OR ‘zingiber officinale’:ti,ab,kw OR ‘ShengJiang’:ti,ab,kw OR ‘Zingiberis Rhizoma Recens’:ti,ab,kw) |
| Cochrane Library | ID→Search→Hits #1→(“CINV”):ti,ab,kw OR (chemotherapy induced nausea and vomiting):ti,ab,kw OR (Vomiting):ti,ab,kw OR (Nausea):ti,ab,kw→58,816 #2→MeSH descriptor: [Nausea] explode all trees→5992 #3→MeSH descriptor: [Vomiting] explode all trees→5733 #4→#1 OR #2 OR #3→58,851 #5→(breast cancer):ti,ab,kw OR (breast neoplasms):ti,ab,kw→40,959 #6→MeSH descriptor: [Breast Neoplasms] explode all trees→14,567 #7→#5 OR #6→40,961 #8→(ginger):ti,ab,kw OR (zingiber officinale):ti,ab,kw OR (ShengJiang):ti,ab,kw OR (Zingiberis Rhizoma Recens):ti,ab,kw→1075 #9→MeSH descriptor: [Ginger] explode all trees→159 #10→#8 OR #9→1075 #11→#4 AND #7 Additionally, #10→22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-D.; Kwag, E.-B.; Yang, M.-X.; Yoo, H.-S. Efficacy and Safety of Ginger on the Side Effects of Chemotherapy in Breast Cancer Patients: Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 11267. https://doi.org/10.3390/ijms231911267
Kim S-D, Kwag E-B, Yang M-X, Yoo H-S. Efficacy and Safety of Ginger on the Side Effects of Chemotherapy in Breast Cancer Patients: Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2022; 23(19):11267. https://doi.org/10.3390/ijms231911267
Chicago/Turabian StyleKim, Soo-Dam, Eun-Bin Kwag, Ming-Xiao Yang, and Hwa-Seung Yoo. 2022. "Efficacy and Safety of Ginger on the Side Effects of Chemotherapy in Breast Cancer Patients: Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 23, no. 19: 11267. https://doi.org/10.3390/ijms231911267
APA StyleKim, S.-D., Kwag, E.-B., Yang, M.-X., & Yoo, H.-S. (2022). Efficacy and Safety of Ginger on the Side Effects of Chemotherapy in Breast Cancer Patients: Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 23(19), 11267. https://doi.org/10.3390/ijms231911267