
Neurochemical Monitoring of Traumatic Brain Injury by the Combined Analysis of Plasma Beta-Synuclein, NfL, and GFAP in Polytraumatized Patients
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
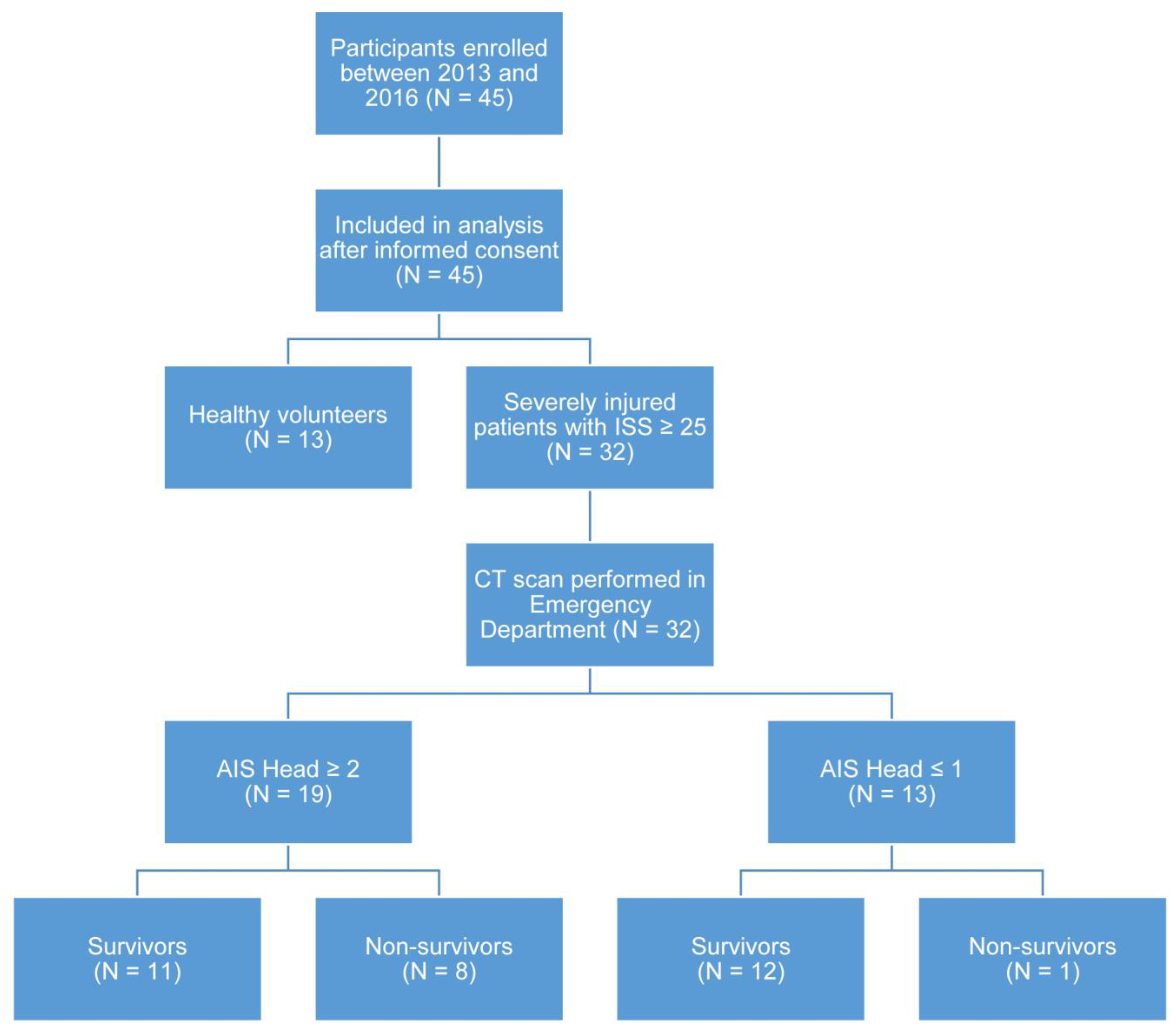
2.1. Clinical and Demographic Features
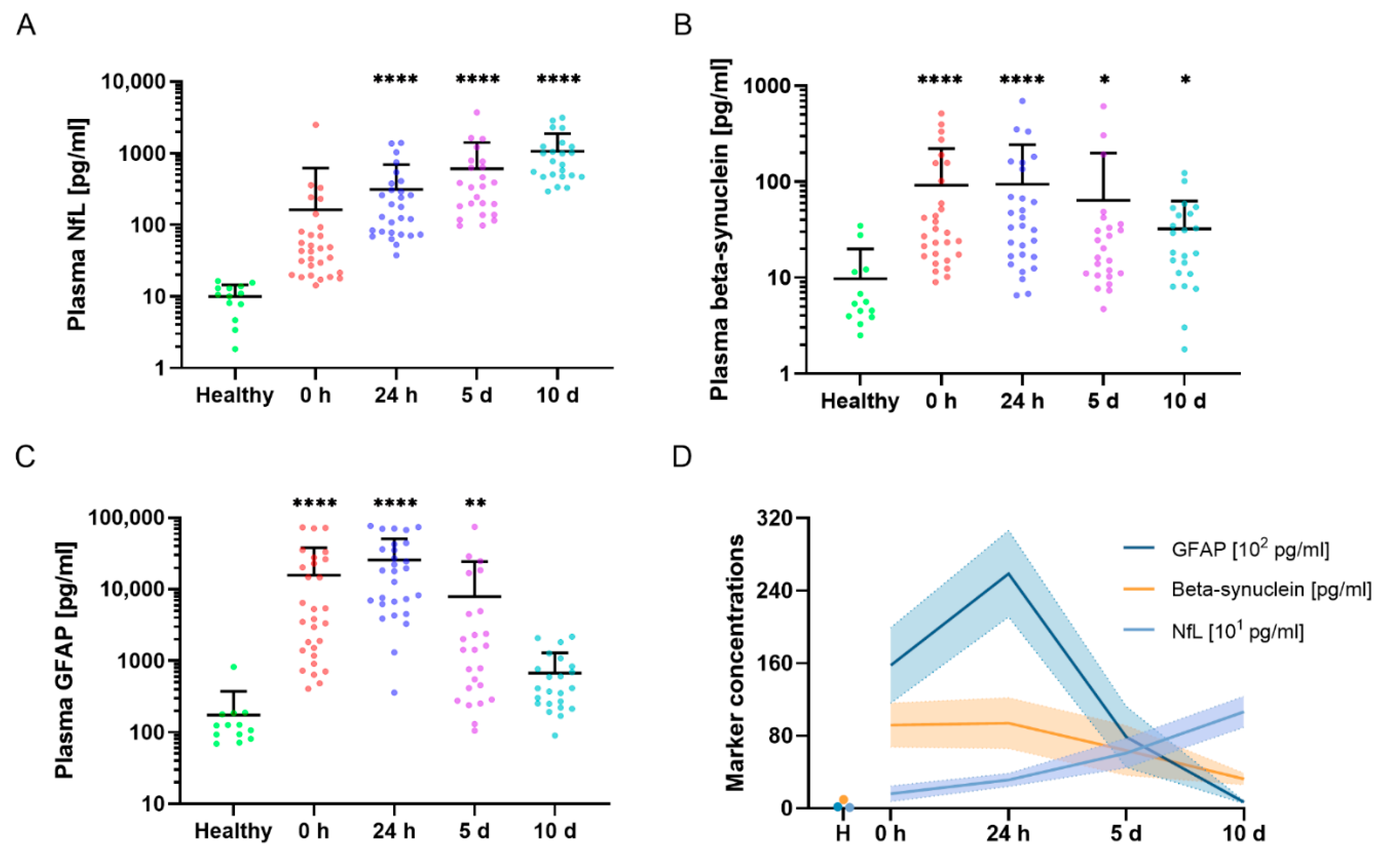
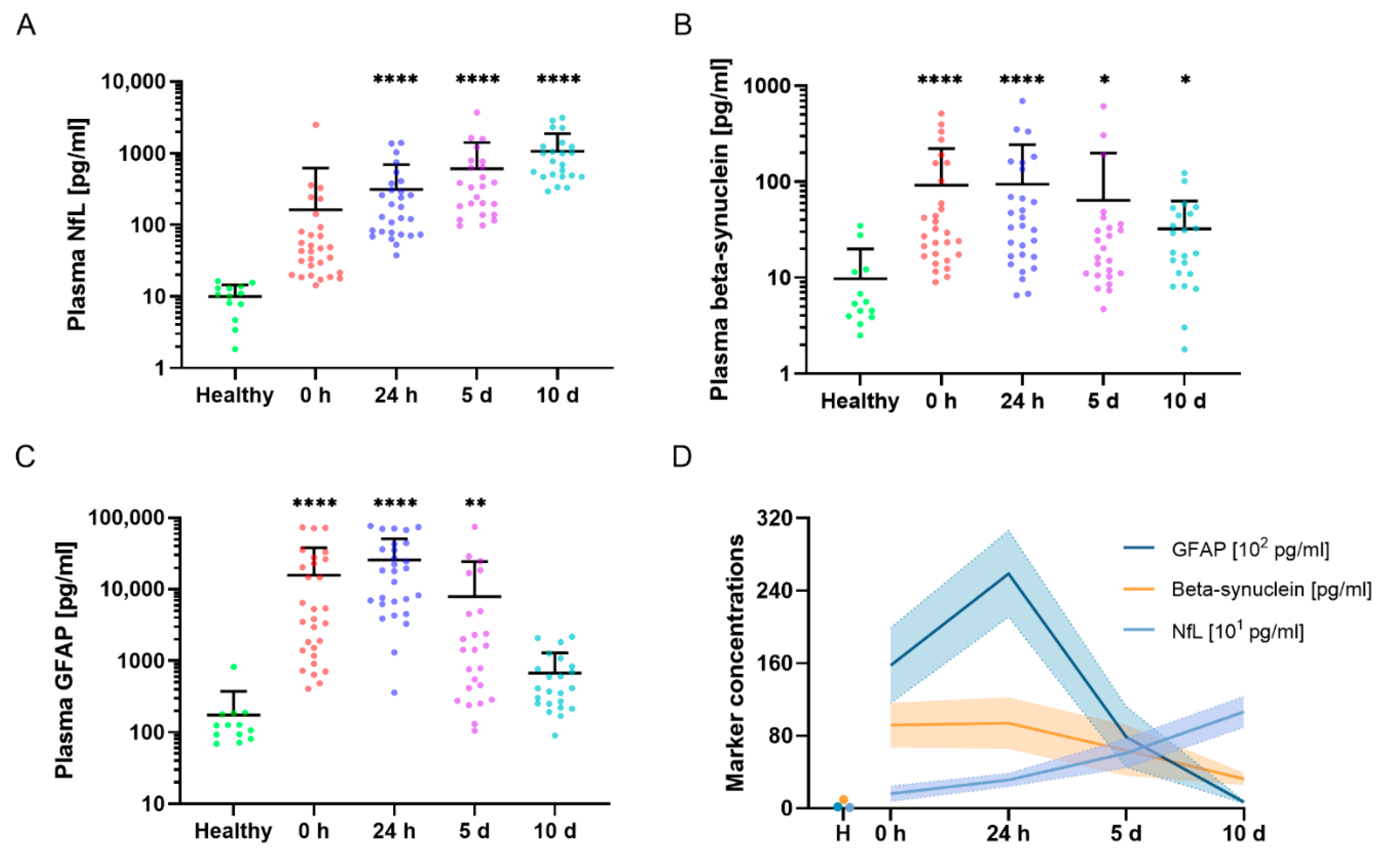
2.2. Blood Neurochemical Marker Levels in the Time Course after Severe Trauma
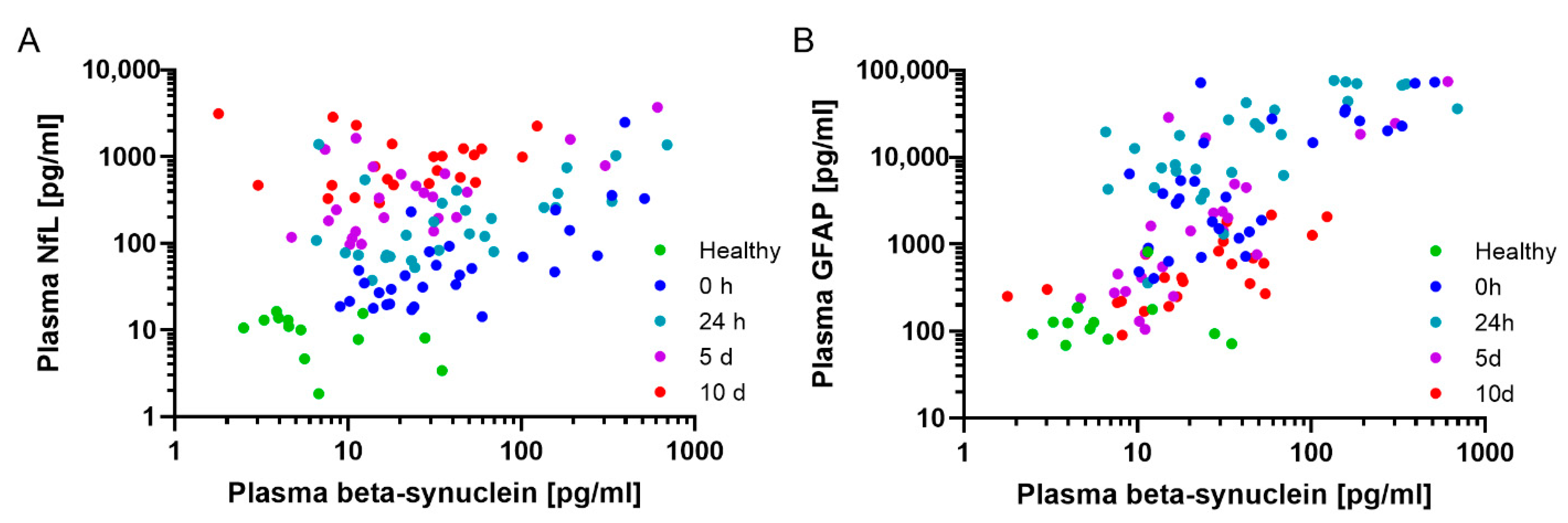
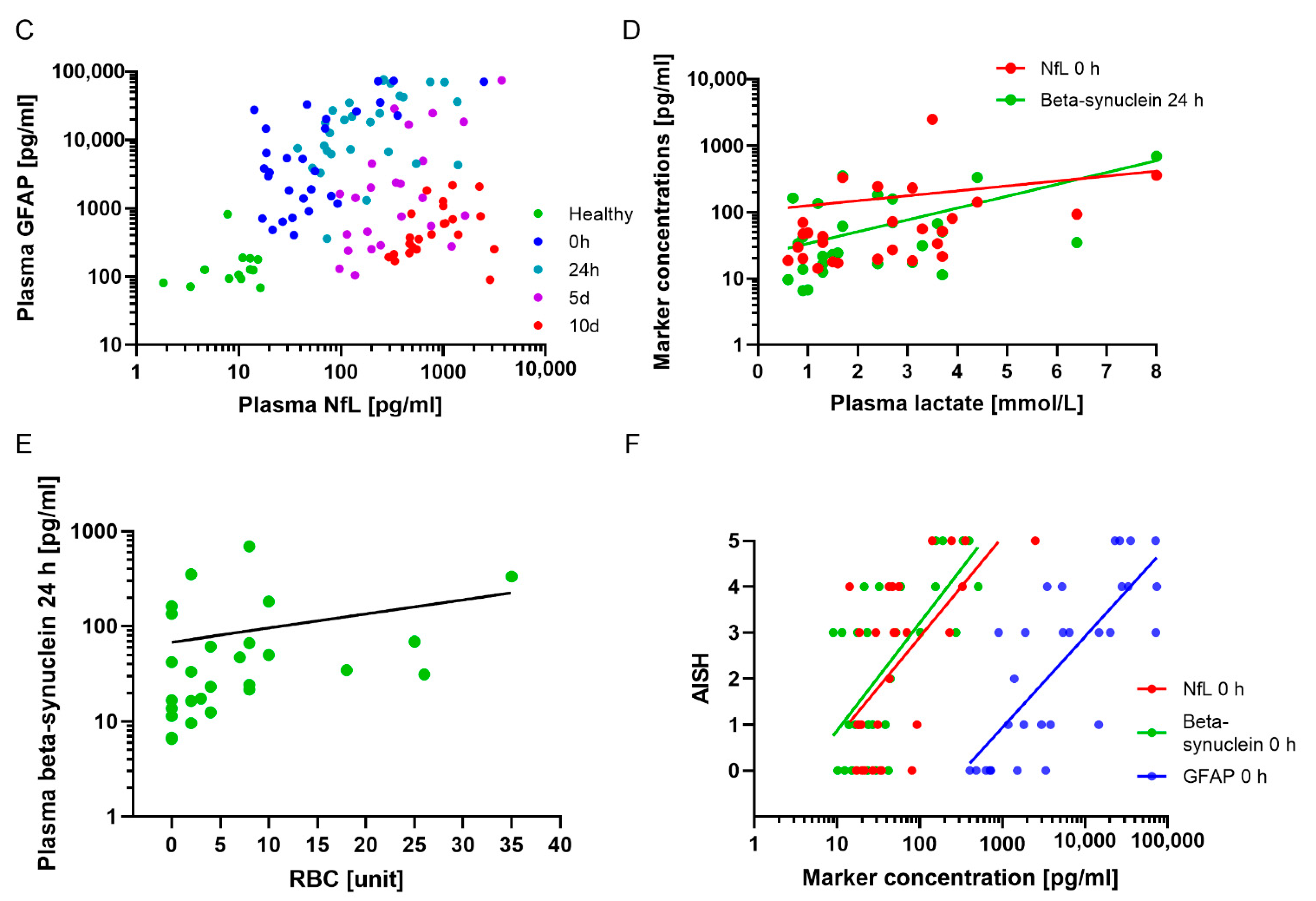
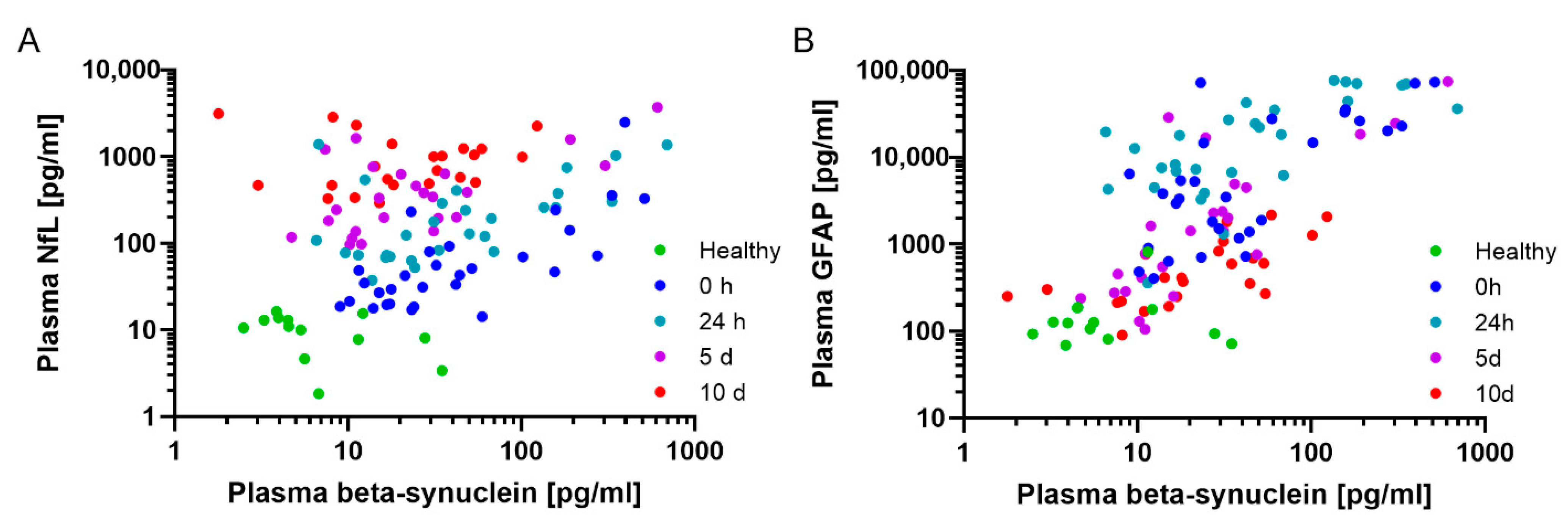
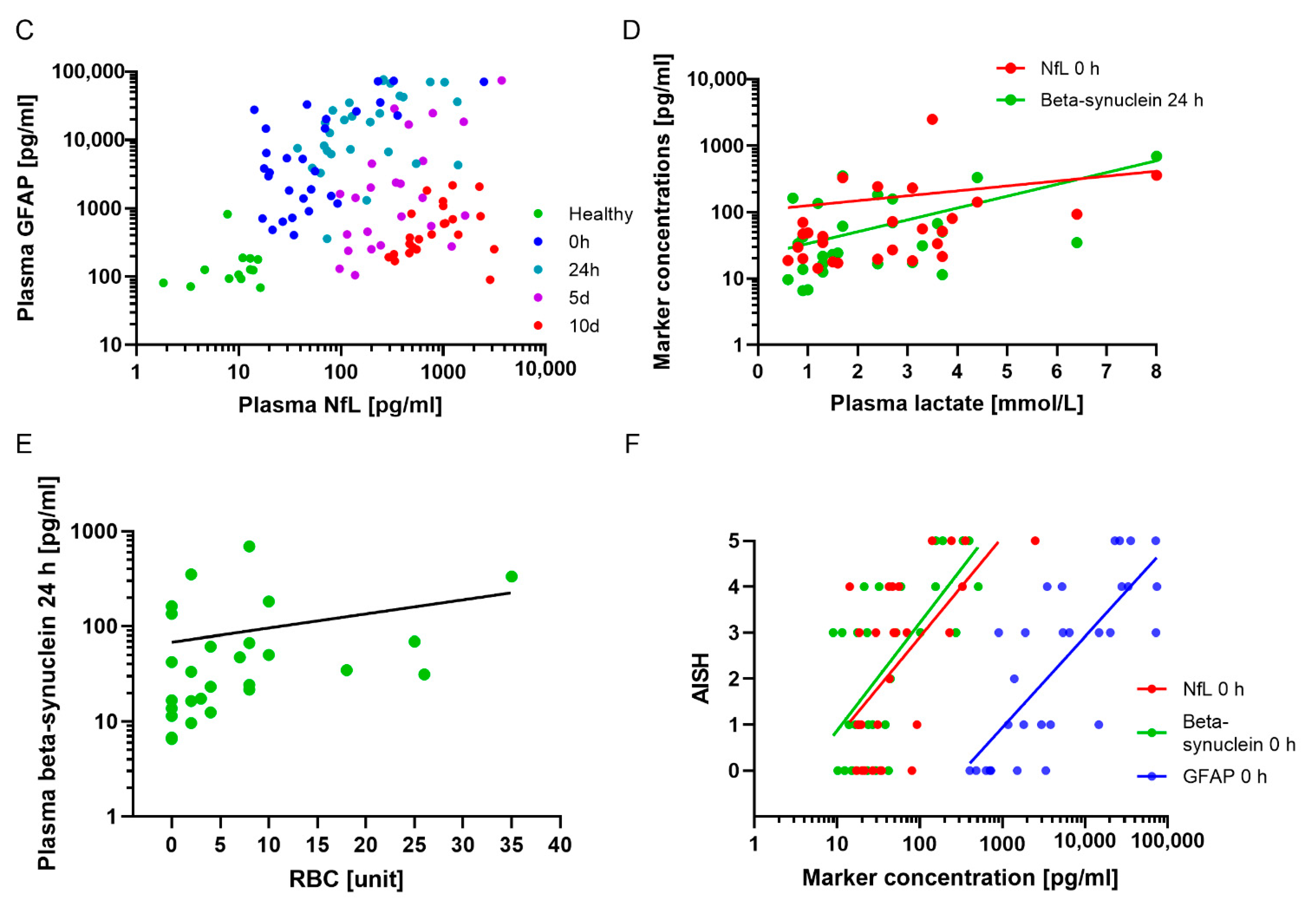
2.3. Correlations of Neurochemical Markers with Clinical Scores and Markers Assessed in the Emergency Room
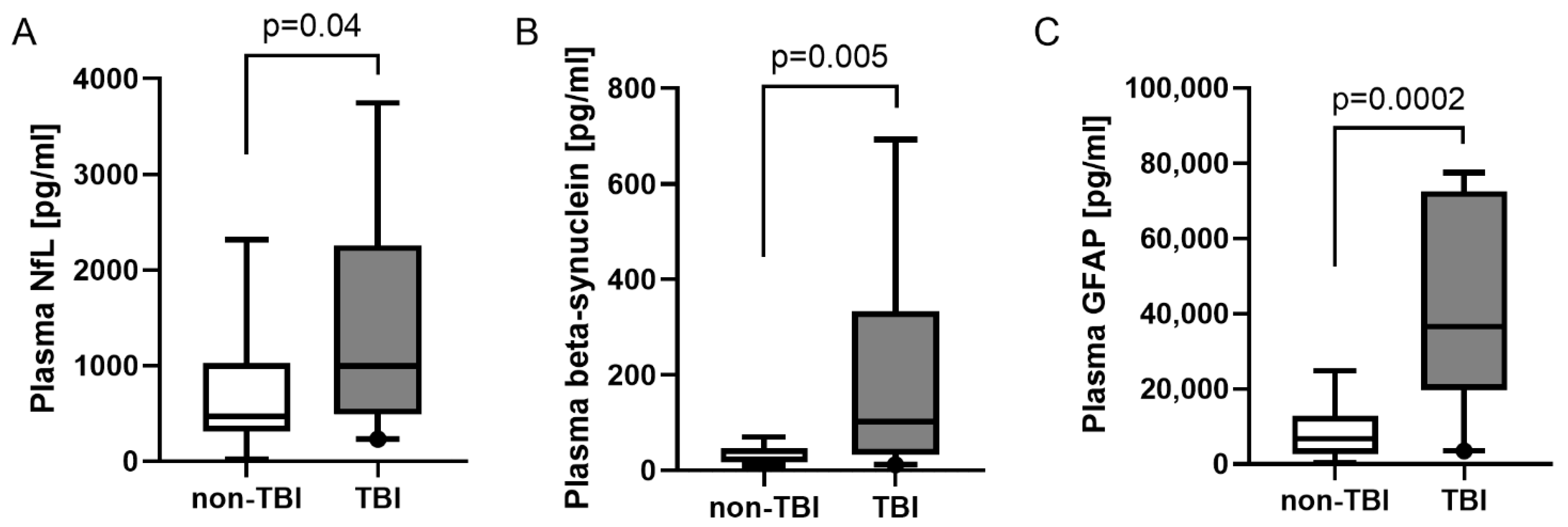
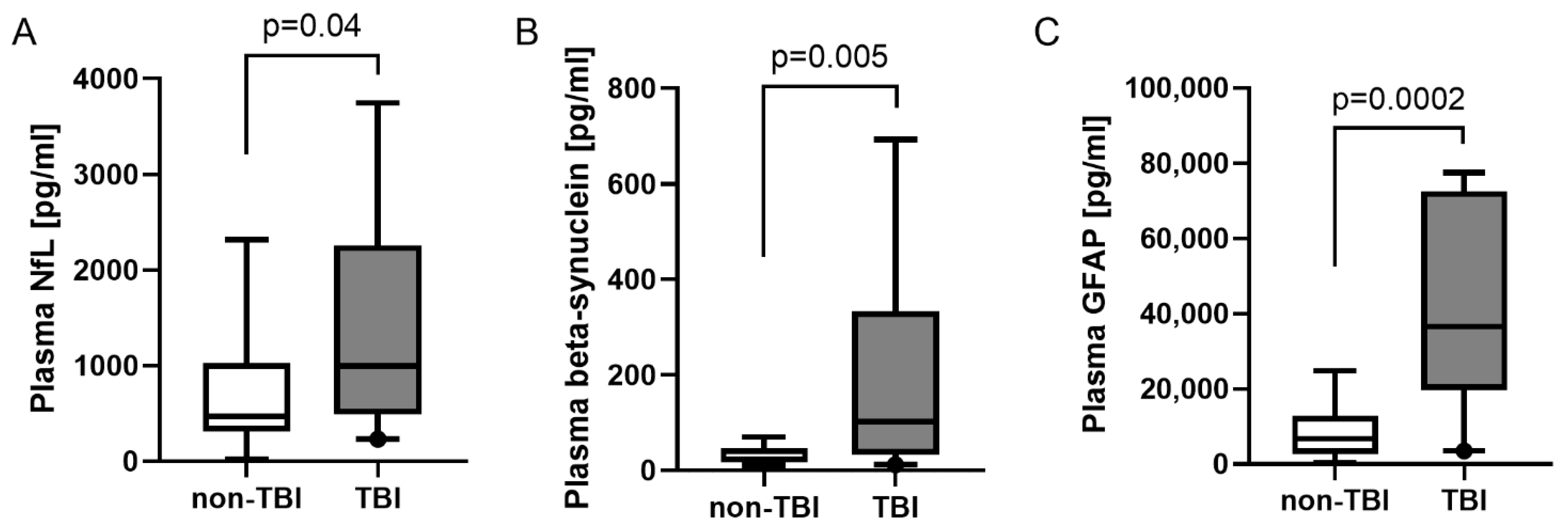
2.4. Discrimination of TBI vs. Non-TBI
2.5. Marker Levels over Time in Severe Trauma Patients with and without TBI
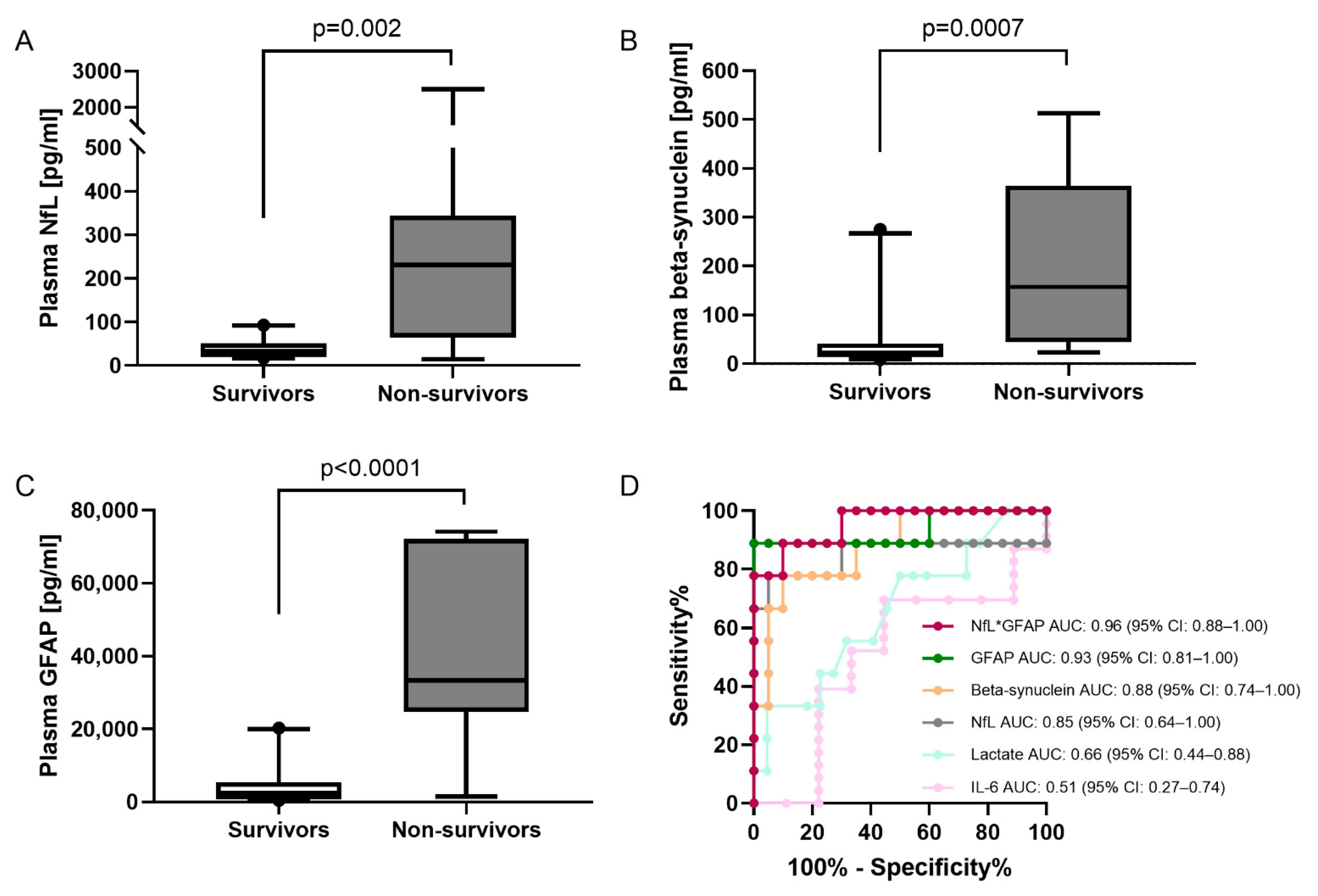
2.6. Marker Concentrations in Survivors and Nonsurvivors
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Plasma Collection and Analysis
4.3. Statistical Analysis
5. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cole, E.; Weaver, A.; Gall, L.; West, A.; Nevin, D.; Tallach, R.; O’Neill, B.; Lahiri, S.; Allard, S.; Tai, N.; et al. A Decade of Damage Control Resuscitation: New Transfusion Practice, New Survivors, New Directions. Ann. Surg. 2021, 273, 1215–1220. [Google Scholar] [CrossRef]
- Pape, H.C.; Lefering, R.; Butcher, N.; Peitzman, A.; Leenen, L.; Marzi, I.; Lichte, P.; Josten, C.; Bouillon, B.; Schmucker, U.; et al. The definition of polytrauma revisited: An international consensus process and proposal of the new ‘Berlin definition’. J. Trauma Acute Care Surg. 2014, 77, 780–786. [Google Scholar] [CrossRef]
- Roozenbeek, B.; Maas, A.I.; Menon, D.K. Changing patterns in the epidemiology of traumatic brain injury. Nat. Rev. Neurol. 2013, 9, 231–236. [Google Scholar] [CrossRef]
- AUC-Academy for Trauma Surgery. Committee on Emergency Medicine, Intensive Care and Trauma Management (Sektion NIS) German Trauma Society (DGU); AUC-Academy for Trauma Surgery TraumaRegister DGU®-Annual Report 2020; AUC-Academy for Trauma Surgery: Berlin, Germany, 2021. [Google Scholar]
- Capizzi, A.; Woo, J.; Verduzco-Gutierrez, M. Traumatic Brain Injury: An Overview of Epidemiology, Pathophysiology, and Medical Management. Med. Clin. N. Am. 2020, 104, 213–238. [Google Scholar] [CrossRef]
- Jamjoom, A.A.B.; Rhodes, J.; Andrews, P.J.D.; Grant, S.G.N. The synapse in traumatic brain injury. Brain A J. Neurol. 2021, 144, 18–31. [Google Scholar] [CrossRef]
- Halbgebauer, S.; Oeckl, P.; Steinacker, P.; Yilmazer-Hanke, D.; Anderl-Straub, S.; von Arnim, C.; Froelich, L.; Gomes, L.A.; Hausner, L.; Huss, A.; et al. Beta-synuclein in cerebrospinal fluid as an early diagnostic marker of Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2020, 92, 349–356. [Google Scholar] [CrossRef]
- Oeckl, P.; Halbgebauer, S.; Anderl-Straub, S.; von Arnim, C.A.F.; Diehl-Schmid, J.; Froelich, L.; Grimmer, T.; Hausner, L.; Denk, J.; Jahn, H.; et al. Targeted Mass Spectrometry Suggests Beta-Synuclein as Synaptic Blood Marker in Alzheimer’s Disease. J. Proteome Res. 2020, 19, 1310–1318. [Google Scholar] [CrossRef]
- Oeckl, P.; Metzger, F.; Nagl, M.; von Arnim, C.A.; Halbgebauer, S.; Steinacker, P.; Ludolph, A.C.; Otto, M. Alpha-, Beta-, and Gamma-synuclein Quantification in Cerebrospinal Fluid by Multiple Reaction Monitoring Reveals Increased Concentrations in Alzheimer’s and Creutzfeldt-Jakob Disease but No Alteration in Synucleinopathies. Mol. Cell. Proteom. 2016, 15, 3126–3138. [Google Scholar] [CrossRef]
- Oeckl, P.; Wagemann, O.; Halbgebauer, S.; Anderl-Straub, S.; Nuebling, G.; Prix, C.; Loosli, S.V.; Wlasich, E.; Danek, A.; Steinacker, P.; et al. Serum Beta-Synuclein Is Higher in Down Syndrome and Precedes Rise of pTau181. Ann. Neurol. 2022, 92, 6–10. [Google Scholar] [CrossRef]
- Halbgebauer, S.; Abu-Rumeileh, S.; Oeckl, P.; Steinacker, P.; Roselli, F.; Wiesner, D.; Mammana, A.; Beekes, M.; Kortazar-Zubizarreta, I.; Perez de Nanclares, G.; et al. Blood beta-Synuclein and Neurofilament Light Chain During the Course of Prion Disease. Neurology 2022, 98, e1434–e1445. [Google Scholar] [CrossRef]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef]
- Shahim, P.; Politis, A.; van der Merwe, A.; Moore, B.; Chou, Y.Y.; Pham, D.L.; Butman, J.A.; Diaz-Arrastia, R.; Gill, J.M.; Brody, D.L.; et al. Neurofilament light as a biomarker in traumatic brain injury. Neurology 2020, 95, e610–e622. [Google Scholar] [CrossRef]
- Shahim, P.; Gren, M.; Liman, V.; Andreasson, U.; Norgren, N.; Tegner, Y.; Mattsson, N.; Andreasen, N.; Ost, M.; Zetterberg, H.; et al. Serum neurofilament light protein predicts clinical outcome in traumatic brain injury. Sci. Rep. 2016, 6, 36791. [Google Scholar] [CrossRef]
- Okonkwo, D.O.; Puffer, R.C.; Puccio, A.M.; Yuh, E.L.; Yue, J.K.; Diaz-Arrastia, R.; Korley, F.K.; Wang, K.K.W.; Sun, X.; Taylor, S.R.; et al. Point-of-Care Platform Blood Biomarker Testing of Glial Fibrillary Acidic Protein versus S100 Calcium-Binding Protein B for Prediction of Traumatic Brain Injuries: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study. J. Neurotrauma 2020, 37, 2460–2467. [Google Scholar] [CrossRef]
- Yue, J.K.; Yuh, E.L.; Korley, F.K.; Winkler, E.A.; Sun, X.; Puffer, R.C.; Deng, H.; Choy, W.; Chandra, A.; Taylor, S.R.; et al. Association between plasma GFAP concentrations and MRI abnormalities in patients with CT-negative traumatic brain injury in the TRACK-TBI cohort: A prospective multicentre study. Lancet Neurol. 2019, 18, 953–961. [Google Scholar] [CrossRef]
- Nylen, K.; Ost, M.; Csajbok, L.Z.; Nilsson, I.; Blennow, K.; Nellgard, B.; Rosengren, L. Increased serum-GFAP in patients with severe traumatic brain injury is related to outcome. J. Neurol. Sci. 2006, 240, 85–91. [Google Scholar] [CrossRef]
- Pelinka, L.E.; Kroepfl, A.; Leixnering, M.; Buchinger, W.; Raabe, A.; Redl, H. GFAP versus S100B in serum after traumatic brain injury: Relationship to brain damage and outcome. J. Neurotrauma 2004, 21, 1553–1561. [Google Scholar] [CrossRef]
- McDonald, S.J.; O’Brien, W.T.; Symons, G.F.; Chen, Z.; Bain, J.; Major, B.P.; Costello, D.; Yamakawa, G.; Sun, M.; Brady, R.D.; et al. Prolonged elevation of serum neurofilament light after concussion in male Australian football players. Biomark. Res. 2021, 9, 4. [Google Scholar] [CrossRef]
- Kobek, M.; Jankowski, Z.; Szala, J.; Gaszczyk-Ozarowski, Z.; Palasz, A.; Skowronek, R. Time-related morphometric studies of neurofilaments in brain contusions. Folia Neuropathol. 2016, 54, 50–58. [Google Scholar] [CrossRef]
- Faden, A.I.; Loane, D.J. Chronic neurodegeneration after traumatic brain injury: Alzheimer disease, chronic traumatic encephalopathy, or persistent neuroinflammation? Neurother. J. Am. Soc. Exp. NeuroTherapeutics 2015, 12, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Garland, P.; Morton, M.; Zolnourian, A.; Durnford, A.; Gaastra, B.; Toombs, J.; Heslegrave, A.J.; More, J.; Zetterberg, H.; Bulters, D.O.; et al. Neurofilament light predicts neurological outcome after subarachnoid haemorrhage. Brain A J. Neurol. 2021, 144, 761–768. [Google Scholar] [CrossRef]
- Huber-Lang, M.; Lambris, J.D.; Ward, P.A. Innate immune responses to trauma. Nat. Immunol. 2018, 19, 327–341. [Google Scholar] [CrossRef]
- Halbgebauer, S.; Ockl, P.; Wirth, K.; Steinacker, P.; Otto, M. Protein biomarkers in Parkinson’s disease: Focus on cerebrospinal fluid markers and synaptic proteins. Mov. Disord. Off. J. Mov. Disord. Soc. 2016, 31, 848–860. [Google Scholar] [CrossRef]
- George, J.M. The synucleins. Genome Biol. 2002, 3, REVIEWS3002. [Google Scholar] [CrossRef]
- Jakes, R.; Spillantini, M.G.; Goedert, M. Identification of two distinct synucleins from human brain. FEBS Lett. 1994, 345, 27–32. [Google Scholar] [CrossRef]
- Huebschmann, N.A.; Luoto, T.M.; Karr, J.E.; Berghem, K.; Blennow, K.; Zetterberg, H.; Ashton, N.J.; Simren, J.; Posti, J.P.; Gill, J.M.; et al. Comparing Glial Fibrillary Acidic Protein (GFAP) in Serum and Plasma Following Mild Traumatic Brain Injury in Older Adults. Front. Neurol. 2020, 11, 1054. [Google Scholar] [CrossRef]
- Okonkwo, D.O.; Yue, J.K.; Puccio, A.M.; Panczykowski, D.M.; Inoue, T.; McMahon, P.J.; Sorani, M.D.; Yuh, E.L.; Lingsma, H.F.; Maas, A.I.; et al. GFAP-BDP as an acute diagnostic marker in traumatic brain injury: Results from the prospective transforming research and clinical knowledge in traumatic brain injury study. J. Neurotrauma 2013, 30, 1490–1497. [Google Scholar] [CrossRef]
- Hausmann, R.; Riess, R.; Fieguth, A.; Betz, P. Immunohistochemical investigations on the course of astroglial GFAP expression following human brain injury. Int. J. Leg. Med. 2000, 113, 70–75. [Google Scholar] [CrossRef]
- Papa, L.; Brophy, G.M.; Welch, R.D.; Lewis, L.M.; Braga, C.F.; Tan, C.N.; Ameli, N.J.; Lopez, M.A.; Haeussler, C.A.; Mendez Giordano, D.I.; et al. Time Course and Diagnostic Accuracy of Glial and Neuronal Blood Biomarkers GFAP and UCH-L1 in a Large Cohort of Trauma Patients With and Without Mild Traumatic Brain Injury. JAMA Neurol. 2016, 73, 551–560. [Google Scholar] [CrossRef]
- Halbgebauer, R.; Braun, C.K.; Denk, S.; Mayer, B.; Cinelli, P.; Radermacher, P.; Wanner, G.A.; Simmen, H.P.; Gebhard, F.; Rittirsch, D.; et al. Hemorrhagic shock drives glycocalyx, barrier and organ dysfunction early after polytrauma. J. Crit. Care 2018, 44, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Kruse, O.; Grunnet, N.; Barfod, C. Blood lactate as a predictor for in-hospital mortality in patients admitted acutely to hospital: A systematic review. Scand. J. Trauma Resusc. Emerg. Med. 2011, 19, 74. [Google Scholar] [CrossRef]
- Badawi, Y.; Ramamoorthy, P.; Shi, H. Hypoxia-inducible factor 1 protects hypoxic astrocytes against glutamate toxicity. ASN Neuro 2012, 4, 231–241. [Google Scholar] [CrossRef]
- Lumpkins, K.M.; Bochicchio, G.V.; Keledjian, K.; Simard, J.M.; McCunn, M.; Scalea, T. Glial fibrillary acidic protein is highly correlated with brain injury. J. Trauma 2008, 65, 778–784. [Google Scholar] [CrossRef]
- Laverse, E.; Guo, T.; Zimmerman, K.; Foiani, M.S.; Velani, B.; Morrow, P.; Adejuwon, A.; Bamford, R.; Underwood, N.; George, J.; et al. Plasma glial fibrillary acidic protein and neurofilament light chain, but not tau, are biomarkers of sports-related mild traumatic brain injury. Brain Commun. 2020, 2, fcaa137. [Google Scholar] [CrossRef]
- Gulbransen, B.D.; Sharkey, K.A. Novel functional roles for enteric glia in the gastrointestinal tract. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 625–632. [Google Scholar] [CrossRef]
- Eng, L.F.; Ghirnikar, R.S.; Lee, Y.L. Glial fibrillary acidic protein: GFAP-thirty-one years (1969–2000). Neurochem. Res. 2000, 25, 1439–1451. [Google Scholar] [CrossRef]
- Trojanowski, J.Q.; Walkenstein, N.; Lee, V.M. Expression of neurofilament subunits in neurons of the central and peripheral nervous system: An immunohistochemical study with monoclonal antibodies. J. Neurosci. Off. J. Soc. Neurosci. 1986, 6, 650–660. [Google Scholar] [CrossRef]
- Barro, C.; Chitnis, T.; Weiner, H.L. Blood neurofilament light: A critical review of its application to neurologic disease. Ann. Clin. Transl. Neurol. 2020, 7, 2508–2523. [Google Scholar] [CrossRef]
- Mariotto, S.; Farinazzo, A.; Magliozzi, R.; Alberti, D.; Monaco, S.; Ferrari, S. Serum and cerebrospinal neurofilament light chain levels in patients with acquired peripheral neuropathies. J. Peripher. Nerv. Syst. 2018, 23, 174–177. [Google Scholar] [CrossRef]
- Sandelius, A.; Zetterberg, H.; Blennow, K.; Adiutori, R.; Malaspina, A.; Laura, M.; Reilly, M.M.; Rossor, A.M. Plasma neurofilament light chain concentration in the inherited peripheral neuropathies. Neurology 2018, 90, e518–e524. [Google Scholar] [CrossRef] [Green Version]
- Association for the Advancement of Automotive Medicine. Abbreviated Injury Scale, 6th ed.; Association for the Advancement of Automotive Medicine: Chicago, IL, USA, 2018. [Google Scholar]
- Paget, L.M.; Boutonnet, M.; Moyer, J.D.; Delhaye, N.; D’Aranda, E.; Beltzer, N.; Hamada, S.R. Trauma centre admissions for traumatic brain injury in France: One-year epidemiological analysis of prospectively collected data. Anaesth. Crit. Care Pain Med. 2021, 40, 100804. [Google Scholar] [CrossRef]
- Camarano, J.G.; Ratliff, H.T.; Korst, G.S.; Hrushka, J.M.; Jupiter, D.C. Predicting in-hospital mortality after traumatic brain injury: External validation of CRASH-basic and IMPACT-core in the national trauma data bank. Injury 2021, 52, 147–153. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | Polytrauma All | TBI | Non-TBI | |||
|---|---|---|---|---|---|---|
| N | 13 | 32 | 19 | 13 | ||
| m/f | 8/5 | 26/6 | p = 0.2 | 17/2 | 9/4 | p = 0.2 |
| Age (y) | 32 (26–49.5) | 47.5 (34.8–58) | p = 0.06 | 46 (37–52) | 53 (30.5–58.5) | p = 0.5 |
| ISS | n/a | 34 (29–41) | 34 (29–43) | 34 (29–39.5) | p = 0.5 | |
| AISH | n/a | 3 (0.3–4) | 4 (3–4) | 0 (0–1) | p < 0.0001 | |
| Initial base excess [mmol/l] | n/a | −2.9 (−5.3–−1.7) | −2.4 (−4.6–−0.9) | −3.1 (−5.4–−2.7) | p = 0.3 | |
| Initial lactate [mmol/l] | n/a | 2.4 (1.2–3.6) | 1.7 (0.9–3.3) | 2.9 (1.5–3.7) | p = 0.1 | |
| RBC in first 24 h [units] | n/a | 3 (0–8) | 2 (0–10) | 4 (0–8) | p = 0.8 | |
| Initial IL-6 [pg/mL] | n/a | 235 (84–827) | 123 (38–478) | 534 (216–969) | p = 0.07 |
| Healthy | 0 h | 24 h | 5 d | 10 d | |
|---|---|---|---|---|---|
| Analyzed samples | n = 13 | n = 29 | n = 28 | n = 24 | n = 23 |
| NfL [pg/mL] (mean (SD); median (IQR)) | 9.9 (4.6); 10.6 (6.2–13.5) | 163 (459); 43.1 (20.8–86.6) | 314 (379); 154 (74.6–360) | 611 (802); 340 (150–734) | 1067 (824); 774 (472–1246) |
| Beta-synuclein [pg/mL] (mean (SD); median (IQR)) | 9.8 (10); 5.3 (3.9–11.8) | 92 (130); 29.4 (17.1–129) | 94 (149); 34.1 (16.6–119) | 64 (135); 18.2 (10.7–35.5) | 32 (31); 18.2 (10.9–46.2) |
| GFAP [pg/mL] (mean (SD); median (IQR)) | 174 (198); 1 25 (87.2–182) | 15,768 (22,438); 3832 (1287–24,745) | 25,887 (25,297); 18,225 (6361–41,277) | 7892 (16,551); 1428 (319–4838) | 672 (617); 412 (251–833) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halbgebauer, R.; Halbgebauer, S.; Oeckl, P.; Steinacker, P.; Weihe, E.; Schafer, M.K.-H.; Roselli, F.; Gebhard, F.; Huber-Lang, M.; Otto, M. Neurochemical Monitoring of Traumatic Brain Injury by the Combined Analysis of Plasma Beta-Synuclein, NfL, and GFAP in Polytraumatized Patients. Int. J. Mol. Sci. 2022, 23, 9639. https://doi.org/10.3390/ijms23179639
Halbgebauer R, Halbgebauer S, Oeckl P, Steinacker P, Weihe E, Schafer MK-H, Roselli F, Gebhard F, Huber-Lang M, Otto M. Neurochemical Monitoring of Traumatic Brain Injury by the Combined Analysis of Plasma Beta-Synuclein, NfL, and GFAP in Polytraumatized Patients. International Journal of Molecular Sciences. 2022; 23(17):9639. https://doi.org/10.3390/ijms23179639
Chicago/Turabian StyleHalbgebauer, Rebecca, Steffen Halbgebauer, Patrick Oeckl, Petra Steinacker, Eberhard Weihe, Martin K.-H. Schafer, Francesco Roselli, Florian Gebhard, Markus Huber-Lang, and Markus Otto. 2022. "Neurochemical Monitoring of Traumatic Brain Injury by the Combined Analysis of Plasma Beta-Synuclein, NfL, and GFAP in Polytraumatized Patients" International Journal of Molecular Sciences 23, no. 17: 9639. https://doi.org/10.3390/ijms23179639
APA StyleHalbgebauer, R., Halbgebauer, S., Oeckl, P., Steinacker, P., Weihe, E., Schafer, M. K.-H., Roselli, F., Gebhard, F., Huber-Lang, M., & Otto, M. (2022). Neurochemical Monitoring of Traumatic Brain Injury by the Combined Analysis of Plasma Beta-Synuclein, NfL, and GFAP in Polytraumatized Patients. International Journal of Molecular Sciences, 23(17), 9639. https://doi.org/10.3390/ijms23179639