
Monitoring Circulating Tumor DNA in Untreated Non-Small-Cell Lung Cancer Patients

 , and
, and
Abstract
1. Introduction
2. Results
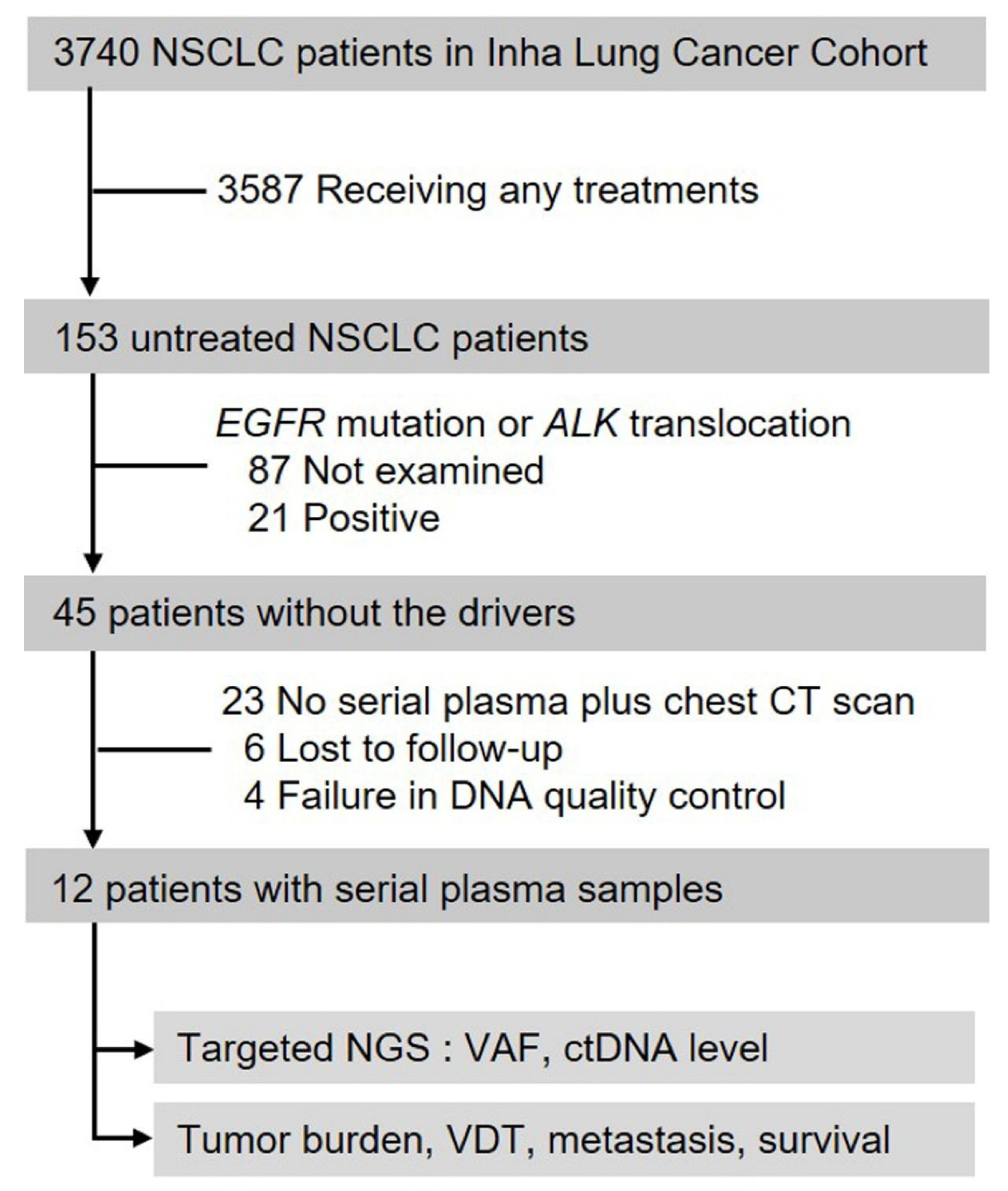
2.1. Patient Characteristics and ctDNA Detection
2.2. Change in ctDNA Levels and Tumor Burden
2.3. Volume Doubling Time, Development of Metastasis and Overall Survival Regarding ctDNA Detection at Diagnosis
3. Discussion
4. Materials and Methods
4.1. Patients and Radiological Evaluation
4.2. Plasma Samples and DNA Extraction
4.3. The Custom Lung Cancer Panel for Korean Population
4.4. Targeted Sequencing
4.5. Preprocessing and Variant Analysis
4.6. Digital Droplet PCR
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aggarwal, C.; Thompson, J.C.; Black, T.A.; Katz, S.I.; Fan, R.; Yee, S.S.; Chien, A.L.; Evans, T.L.; Bauml, J.M.; Alley, E.W.; et al. Clinical Implications of Plasma-Based Genotyping with the Delivery of Personalized Therapy in Metastatic Non-Small Cell Lung Cancer. JAMA Oncol. 2019, 5, 173–180. [Google Scholar] [CrossRef]
- de Bruin, E.C.; McGranahan, N.; Mitter, R.; Salm, M.; Wedge, D.C.; Yates, L.; Jamal-Hanjani, M.; Shafi, S.; Murugaesu, N.; Rowan, A.J.; et al. Spatial and temporal diversity in genomic instability processes defines lung cancer evolution. Science 2014, 346, 251–256. [Google Scholar] [CrossRef]
- Diaz, L.A., Jr.; Bardelli, A. Liquid biopsies: Genotyping circulating tumor DNA. J. Clin. Oncol. 2014, 32, 579–586. [Google Scholar] [CrossRef]
- David, E.A.; Daly, M.E.; Li, C.S.; Chiu, C.L.; Cooke, D.T.; Brown, L.M.; Melnikow, J.; Kelly, K.; Canter, R.J. Increasing Rates of No Treatment in Advanced-Stage Non-Small Cell Lung Cancer Patients: A Propensity-Matched Analysis. J. Thorac. Oncol. 2017, 12, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Detterbeck, F.C.; Gibson, C.J. Turning gray: The natural history of lung cancer over time. J. Thorac. Oncol. 2008, 3, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.D.; Alexandrov, A.; Kim, J.; Wala, J.; Berger, A.H.; Pedamallu, C.S.; Shukla, S.A.; Guo, G.; Brooks, A.N.; Murray, B.A. Distinct patterns of somatic genome alterations in lung adenocarcinomas and squamous cell carcinomas. Nat. Genet. 2016, 48, 607. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.A.; Chabon, J.J.; Lovejoy, A.F.; Newman, A.M.; Stehr, H.; Azad, T.D.; Khodadoust, M.S.; Esfahani, M.S.; Liu, C.L.; Zhou, L.; et al. Early Detection of Molecular Residual Disease in Localized Lung Cancer by Circulating Tumor DNA Profiling. Cancer Discov. 2017, 7, 1394–1403. [Google Scholar] [CrossRef]
- Cabel, L.; Riva, F.; Servois, V.; Livartowski, A.; Daniel, C.; Rampanou, A.; Lantz, O.; Romano, E.; Milder, M.; Buecher, B. Circulating tumor DNA changes for early monitoring of anti-PD1 immunotherapy: A proof-of-concept study. Ann. Oncol. 2017, 28, 1996–2001. [Google Scholar] [CrossRef]
- Horn, L.; Whisenant, J.G.; Wakelee, H.; Reckamp, K.L.; Qiao, H.; Leal, T.A.; Du, L.; Hernandez, J.; Huang, V.; Blumenschein, G.R. Monitoring therapeutic response and resistance: Analysis of circulating tumor DNA in patients with ALK+ lung cancer. J. Thorac. Oncol. 2019, 14, 1901–1911. [Google Scholar] [CrossRef]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra224. [Google Scholar] [CrossRef]
- De Vlaminck, I.; Martin, L.; Kertesz, M.; Patel, K.; Kowarsky, M.; Strehl, C.; Cohen, G.; Luikart, H.; Neff, N.F.; Okamoto, J. Noninvasive monitoring of infection and rejection after lung transplantation. Proc. Natl. Acad. Sci. USA 2015, 112, 13336–13341. [Google Scholar] [CrossRef] [PubMed]
- Riva, F.; Bidard, F.-C.; Houy, A.; Saliou, A.; Madic, J.; Rampanou, A.; Hego, C.; Milder, M.; Cottu, P.; Sablin, M.-P. Patient-specific circulating tumor DNA detection during neoadjuvant chemotherapy in triple-negative breast cancer. Clin. Chem. 2017, 63, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Mehlen, P.; Puisieux, A. Metastasis: A question of life or death. Nat. Rev. Cancer 2006, 6, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Hammerman, P.S.; Kim, J.; Yoon, J.-A.; Lee, Y.; Sun, J.-M.; Wilkerson, M.D.; Pedamallu, C.S.; Cibulskis, K.; Yoo, Y.K. Integrative and comparative genomic analysis of lung squamous cell carcinomas in East Asian patients. J. Clin. Oncol. 2014, 32, 121. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Yang, H.; Teo, A.S.M.; Amer, L.B.; Sherbaf, F.G.; Tan, C.Q.; Alvarez, J.J.S.; Lu, B.; Lim, J.Q.; Takano, A. Genomic landscape of lung adenocarcinoma in East Asians. Nat. Genet. 2020, 52, 177–186. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Choi, S.; Kim, H.R.; Sung, C.O.; Kim, J.; Kim, S.; Ahn, S.-M.; Choi, C.-M.; Chun, S.-M.; Choi, E.K.; Kim, S.-W. Genomic alterations in the RB pathway indicate prognostic outcomes of early-stage lung adenocarcinoma. Clin. Cancer Res. 2015, 21, 2613–2623. [Google Scholar] [CrossRef][Green Version]
- Seo, J.-S.; Ju, Y.S.; Lee, W.-C.; Shin, J.-Y.; Lee, J.K.; Bleazard, T.; Lee, J.; Jung, Y.J.; Kim, J.-O.; Shin, J.-Y. The transcriptional landscape and mutational profile of lung adenocarcinoma. Genome Res. 2012, 22, 2109–2119. [Google Scholar] [CrossRef]
- Li, H.; Durbin, R. Fast and accurate long-read alignment with Burrows–Wheeler transform. Bioinformatics 2010, 26, 589–595. [Google Scholar] [CrossRef]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M. The Genome Analysis Toolkit: A MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Wilm, A.; Aw, P.P.K.; Bertrand, D.; Yeo, G.H.T.; Ong, S.H.; Wong, C.H.; Khor, C.C.; Petric, R.; Hibberd, M.L.; Nagarajan, N. LoFreq: A sequence-quality aware, ultra-sensitive variant caller for uncovering cell-population heterogeneity from high-throughput sequencing datasets. Nucleic Acids Res. 2012, 40, 11189–11201. [Google Scholar] [CrossRef]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.T.; Thorvaldsdóttir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative genomics viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Scherer, F.; Kurtz, D.M.; Newman, A.M.; Stehr, H.; Craig, A.F.; Esfahani, M.S.; Lovejoy, A.F.; Chabon, J.J.; Klass, D.M.; Liu, C.L. Distinct biological subtypes and patterns of genome evolution in lymphoma revealed by circulating tumor DNA. Sci. Transl. Med. 2016, 8, ra155–ra364. [Google Scholar] [CrossRef]
- Schwartz, M. A biomathematical approach to clinical tumor growth. Cancer 1961, 14, 1272–1294. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Time a | ctDNA Detection | VDT (Months) | Site of Metastasis | Pneumonia | Tumor Necrosis |
|---|---|---|---|---|---|---|
| P1 | T1 | Yes | 4.3 | Br | ||
| T2 | Br, Lu, Pl | |||||
| T3 | Br, Lu, Pl, Bo, Al | |||||
| T4 | Br, Lu, Pl, Bo, Al | |||||
| P2 | T1 | No | 7.2 | None | ||
| T2 | None | |||||
| T3 | None | |||||
| P3 | T1 | Yes | 2.4 | Bo, Pl | Yes | |
| T2 | Bo, Pl, Cw | Yes | ||||
| P4 | T1 | No | 2.0 | Pl | ||
| T2 | Pl | |||||
| P5 | T1 | No | 5.9 | Bo, Br, Lu, Pl | ||
| T2 | Bo, Br, Lu, Pl | |||||
| T3 | Bo, Br, Lu, Pl | |||||
| P6 | T1 | Yes | 1.6 | Li, Bo | ||
| T2 | Li, Bo, Pl | |||||
| T3 | Li, Bo, Pl, Pc, Al | |||||
| P7 | T1 | No | 7.0 | None | ||
| T2 | None | |||||
| T3 | None | |||||
| P8 | T1 | No | 4.9 | Pl | Yes | Yes |
| T2 | Pl | Yes | ||||
| T3 | Pl | Yes | Yes | |||
| P9 | T1 | Yes | 4.3 | None | ||
| T2 | Li | |||||
| T3 | Li, Kd, Pt | |||||
| P10 | T1 | Yes | 1.7 | None | ||
| T2 | Pl | |||||
| P11 | T1 | Yes | 1.4 | Br, Lu | ||
| T2 | Br, Lu, Ad, Sp, Li, Pt, Aw | |||||
| P12 | T1 | Yes | 4.7 | Bo | Yes | |
| T2 | Bo, Lu | |||||
| T3 | Bo, Lu, Li | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, W.K.; Oh, S.; Lim, J.H.; Lee, S.J.; Shin, H.-T.; Ryu, J.-S. Monitoring Circulating Tumor DNA in Untreated Non-Small-Cell Lung Cancer Patients. Int. J. Mol. Sci. 2022, 23, 9527. https://doi.org/10.3390/ijms23179527
Ryu WK, Oh S, Lim JH, Lee SJ, Shin H-T, Ryu J-S. Monitoring Circulating Tumor DNA in Untreated Non-Small-Cell Lung Cancer Patients. International Journal of Molecular Sciences. 2022; 23(17):9527. https://doi.org/10.3390/ijms23179527
Chicago/Turabian StyleRyu, Woo Kyung, Sekyung Oh, Jun Hyeok Lim, Seung Jae Lee, Hyun-Tae Shin, and Jeong-Seon Ryu. 2022. "Monitoring Circulating Tumor DNA in Untreated Non-Small-Cell Lung Cancer Patients" International Journal of Molecular Sciences 23, no. 17: 9527. https://doi.org/10.3390/ijms23179527
APA StyleRyu, W. K., Oh, S., Lim, J. H., Lee, S. J., Shin, H.-T., & Ryu, J.-S. (2022). Monitoring Circulating Tumor DNA in Untreated Non-Small-Cell Lung Cancer Patients. International Journal of Molecular Sciences, 23(17), 9527. https://doi.org/10.3390/ijms23179527