
Improving the Management of Endometrial Cancer Patients through the Use of Liquid Biopsy Analyses: A Case Report

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
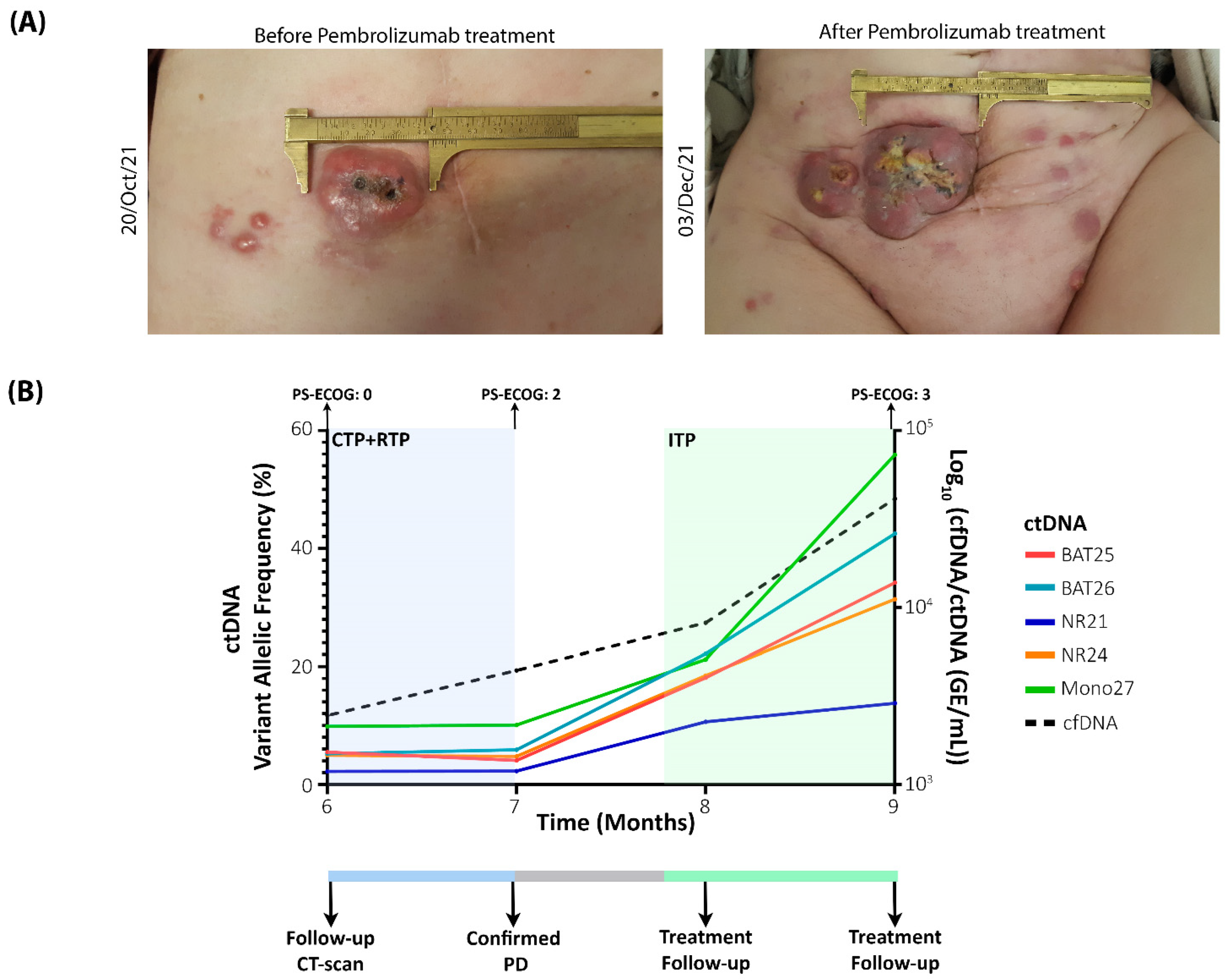
2.1. Clinical Course
2.2. Liquid Biopsy Analysis as a Powerful Monitoring Tool to Identify Recurrences and Monitor Treatment Efficiency
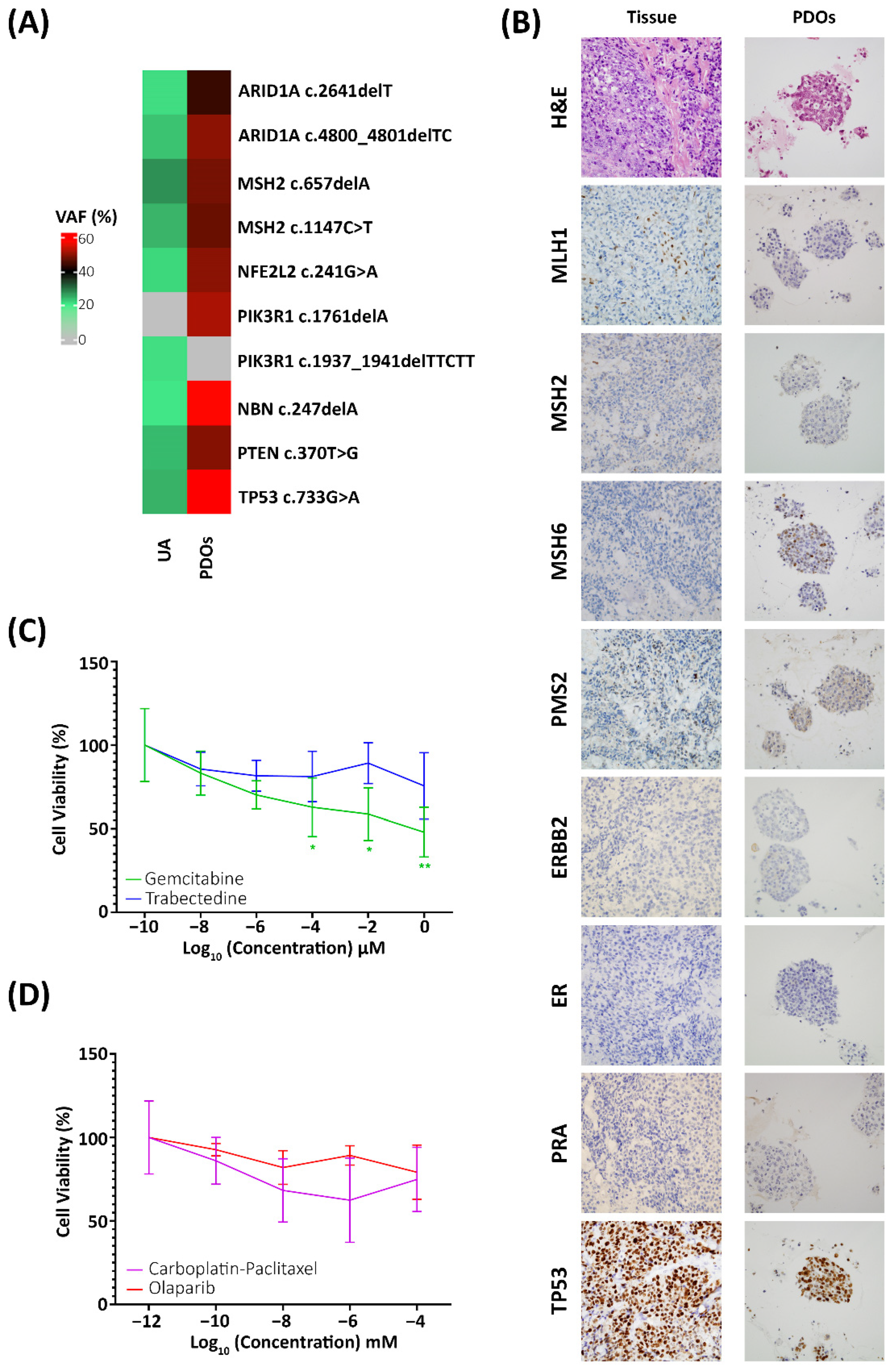
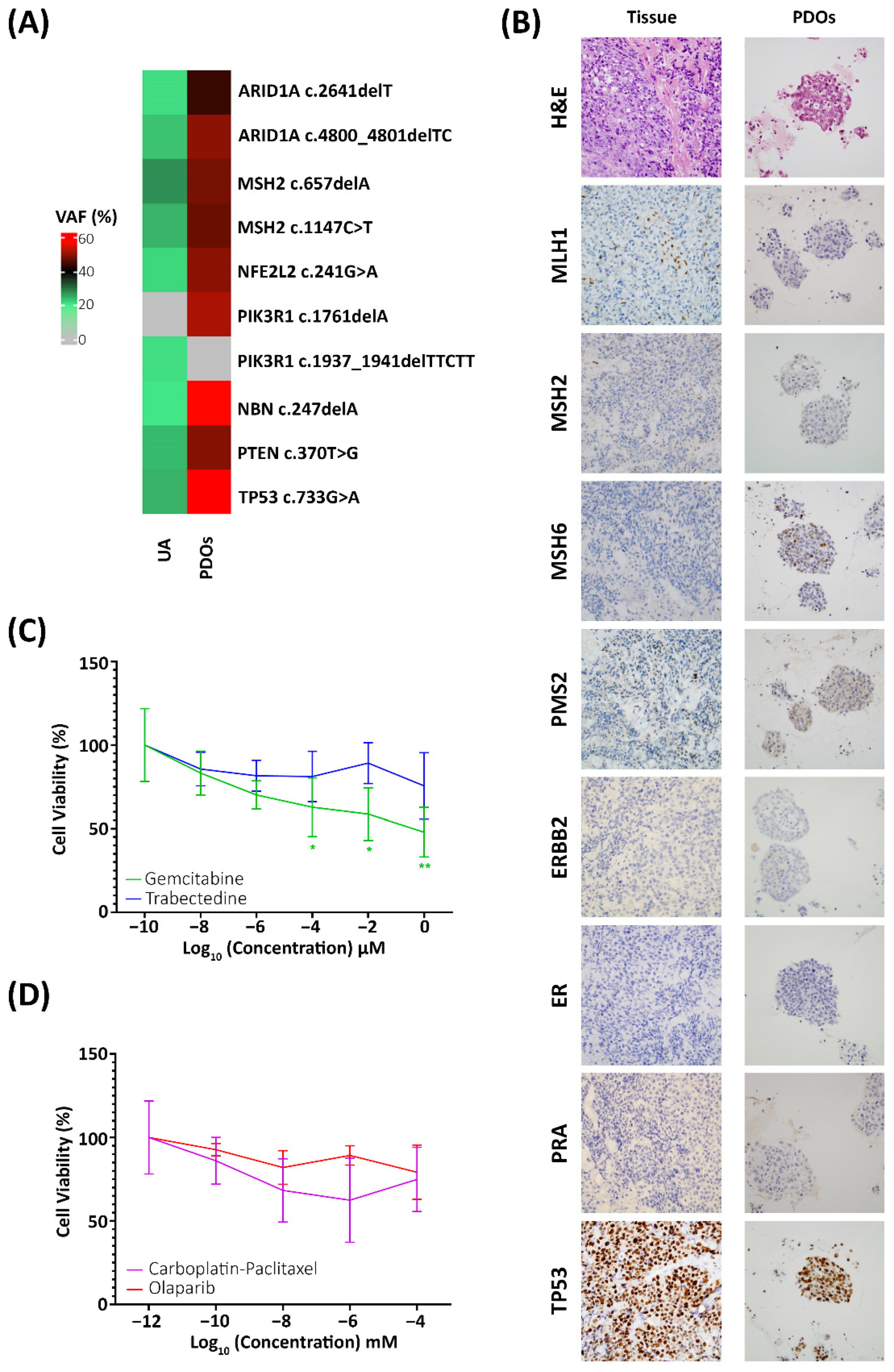
2.3. Preclinical Models for the Identification of Efficient Therapies
3. Discussion
4. Materials and Methods
4.1. Patient Inclusion
4.2. Sample Collection and Processing
4.3. Preclinical Model Generation
4.4. Drug Screening
4.5. Immunohistochemistry Characterisation
4.6. Sequencing Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EC | Endometrial cancer |
| PDOs | Patient-derived organoids |
| cfDNA | circulating free DNA |
| ctDNA | circulating tumour DNA |
| MSI | Microsatellite instability |
| AJCC | American Joint Committee on Cancer |
| TNM | Tumour, nodes, metastases |
| ITP | Immunotherapy |
| IHC | Immunohistochemistry |
| CTP | Chemotherapy |
| RTP | Radiotherapy |
| AB | alamarBlueTM |
| VAF | Variant allelic frequency |
| PS-ECOG | ECOG Scale of Performance Status |
| MMR | Mismatch repair |
| GE | Genomic equivalents |
| BME | Basement membrane extract |
| cEVs | Circulating extracellular vesicles |
References
- Costas, L.; Frias-Gomez, J.; Guardiola, M.; Benavente, Y.; Pineda, M.; Pavón, M.Á.; Martínez, J.M.; Climent, M.; Barahona, M.; Canet, J.; et al. New Perspectives on Screening and Early Detection of Endometrial Cancer. Int. J. Cancer 2019, 145, 3194–3206. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA. Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Llauradó, M.; Ruiz, A.; Majem, B.; Ertekin, T.; Colás, E.; Pedrola, N.; Devis, L.; Rigau, M.; Sequeiros, T.; Montes, M.; et al. Molecular Bases of Endometrial Cancer: New Roles for New Actors in the Diagnosis and the Therapy of the Disease. Mol. Cell. Endocrinol. 2012, 358, 244–255. [Google Scholar] [CrossRef]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef]
- Bolivar, A.M.; Luthra, R.; Mehrotra, M.; Chen, W.; Barkoh, B.A.; Hu, P.; Zhang, W.; Broaddus, R.R. Targeted Next-Generation Sequencing of Endometrial Cancer and Matched Circulating Tumor DNA: Identification of Plasma-Based, Tumor-Associated Mutations in Early Stage Patients. Mod. Pathol. 2019, 32, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Casas-Arozamena, C.; Díaz, E.; Moiola, C.P.; Alonso-Alconada, L.; Ferreiros, A.; Abalo, A.; López Gil, C.; Oltra, S.S.; de Santiago, J.; Cabrera, S.; et al. Genomic Profiling of Uterine Aspirates and CfDNA as an Integrative Liquid Biopsy Strategy in Endometrial Cancer. J. Clin. Med. 2020, 9, 585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Zhang, Z.H.; Wang, S.; Lang, J.H. Circulating Cell-Free DNA or Circulating Tumor Dna in the Management of Ovarian and Endometrial Cancer. Onco. Targets. Ther. 2019, 12, 11517–11530. [Google Scholar] [CrossRef] [Green Version]
- Cicchillitti, L.; Corrado, G.; de Angeli, M.; Mancini, E.; Baiocco, E.; Patrizi, L.; Zampa, A.; Merola, R.; Martayan, A.; Conti, L.; et al. Circulating Cell-Free DNA Content as Blood Based Biomarker in Endometrial Cancer. Oncotarget 2017, 8, 115230–115243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrzycka, B.; Terlikowski, S.J.; Mazurek, A.; Kowalczuk, O.; Niklinska, W.; Chyczewski, L.; Kulikowski, M. Circulating Free DNA, P53 Antibody and Mutations of KRAS Gene in Endometrial Cancer. Int. J. Cancer 2010, 127, 612–621. [Google Scholar] [CrossRef]
- Piñeiro-Pérez, R.; Abal, M.; Muinelo-romay, L. Liquid Biopsy for Monitoring EC Patients: Towards Personalized Treatment. Cancers 2022, 14, 1405. [Google Scholar] [CrossRef]
- Tanaka, H.; Tsuda, H.; Nishimura, S.; Nomura, H.; Kataoka, F.; Chiyoda, T.; Tanaka, K.; Iguchi, Y.; Susumu, N.; Aoki, D. Role of Circulating Free Alu DNA in Endometrial Cancer. Int. J. Gynecol. Cancer 2012, 22, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Jia, N.; Jiao, H.; Chen, J.; Chen, Y.; Zhang, Y.; Zhu, M.; Zhu, C.; Shen, L.; Long, W. Circulating Tumor DNA as a Prognostic Marker in High-Risk Endometrial Cancer. J. Transl. Med. 2021, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pereira, E.; Camacho-Vanegas, O.; Anand, S.; Sebra, R.; Camacho, S.C.; Garnar-Wortzel, L.; Nair, N.; Moshier, E.; Wooten, M.; Uzilov, A.; et al. Personalized Circulating Tumor DNA Biomarkers Dynamically Predict Treatment Response and Survival in Gynecologic Cancers. PLoS ONE 2015, 10, e0145754. [Google Scholar] [CrossRef] [PubMed]
- Mota, A.; Colás, E.; García-Sanz, P.; Campoy, I.; Rojo-Sebastián, A.; Gatius, S.; García, Á.; Chiva, L.; Alonso, S.; Gil-Moreno, A.; et al. Genetic Analysis of Uterine Aspirates Improves the Diagnostic Value and Captures the Intra-Tumor Heterogeneity of Endometrial Cancers. Mod. Pathol. 2017, 30, 134–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofer, M.; Lutolf, M.P. Engineering Organoids. Nat. Rev. Mater. 2021, 6, 402–420. [Google Scholar] [CrossRef] [PubMed]
- LeSavage, B.L.; Suhar, R.A.; Broguiere, N.; Lutolf, M.P.; Heilshorn, S.C. Next-Generation Cancer Organoids. Nat. Mater. 2022, 21, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Gibson, W.J.; Hoivik, E.A.; Halle, M.K.; Taylor-Weiner, A.; Cherniack, A.D.; Berg, A.; Holst, F.; Zack, T.I.; Werner, H.M.J.; Staby, K.M.; et al. The Genomic Landscape and Evolution of Endometrial Carcinoma Progression and Abdominopelvic Metastasis. Physiol. Behav. 2017, 176, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Boretto, M.; Maenhoudt, N.; Luo, X.; Hennes, A.; Boeckx, B.; Bui, B.; Heremans, R.; Perneel, L.; Kobayashi, H.; Van Zundert, I.; et al. Patient-Derived Organoids from Endometrial Disease Capture Clinical Heterogeneity and Are Amenable to Drug Screening. Nat. Cell Biol. 2019, 21, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- Lõhmussaar, K.; Oka, R.; Espejo Valle-Inclan, J.; Smits, M.H.H.; Wardak, H.; Korving, J.; Begthel, H.; Proost, N.; van de Ven, M.; Kranenburg, O.W.; et al. Patient-Derived Organoids Model Cervical Tissue Dynamics and Viral Oncogenesis in Cervical Cancer. Cell Stem Cell 2021, 28, 1380–1396.e6. [Google Scholar] [CrossRef]
- Lõhmussaar, K.; Boretto, M.; Clevers, H. Human-Derived Model Systems in Gynecological Cancer Research. Trends Cancer 2020, 6, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Maru, Y.; Tanaka, N.; Itami, M.; Hippo, Y. Efficient Use of Patient-Derived Organoids as a Preclinical Model for Gynecologic Tumors. Gynecol. Oncol. 2019, 154, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Turco, M.Y.; Gardner, L.; Hughes, J.; Cindrova-Davies, T.; Gomez, M.J.; Farrell, L.; Hollinshead, M.; Marsh, S.G.E.; Brosens, J.J.; Critchley, H.O.; et al. Long-Term, Hormone-Responsive Organoid Cultures of Human Endometrium in a Chemically Defined Medium. Nat. Cell Biol. 2017, 19, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Peng, H.; Qi, X.; Wu, M.; Zhao, X. Targeted Therapies in Gynecological Cancers: A Comprehensive Review of Clinical Evidence. Signal Transduct. Target. Ther. 2020, 5, 137. [Google Scholar] [CrossRef] [PubMed]
- Getz, G.; Gabriel, S.B.; Cibulskis, K.; Lander, E.; Sivachenko, A.; Sougnez, C.; Lawrence, M.; Kandoth, C.; Dooling, D.; Fulton, R.; et al. Integrated Genomic Characterization of Endometrial Carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Wokołorczyk, D.; Kluźniak, W.; Huzarski, T.; Gronwald, J.; Szymiczek, A.; Rusak, B.; Stempa, K.; Gliniewicz, K.; Kashyap, A.; Morawska, S.; et al. Mutations in ATM, NBN and BRCA2 Predispose to Aggressive Prostate Cancer in Poland. Int. J. Cancer 2020, 147, 2793–2800. [Google Scholar] [CrossRef]
- Wu, Z.; Li, S.; Tang, X.; Wang, Y.; Guo, W.; Cao, G.; Chen, K.; Zhang, M.; Guan, M.; Yang, D. Copy Number Amplification of DNA Damage Repair Pathways Potentiates Therapeutic Resistance in Cancer. Theranostics 2020, 10, 3939–3951. [Google Scholar] [CrossRef]
- Santoro, A.; Angelico, G.; Travaglino, A.; Inzani, F.; Arciuolo, D.; Valente, M.; D’Alessandris, N.; Scaglione, G.; Fiorentino, V.; Raffone, A.; et al. New Pathological and Clinical Insights in Endometrial Cancer in View of the Updated ESGO/ESTRO/ESP Guidelines. Cancers 2021, 13, 2623. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Banno, K.; Okawa, R.; Yanokura, M.; Iijima, M.; Iriekunitomi, H.; Nakamura, K.; Iida, M.; Adachi, M.; Umene, K.; et al. ARID1A Gene Mutation in Ovarian and Endometrial Cancers (Review). Oncol. Rep. 2016, 35, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Kurnit, K.C.; Kim, G.N.; Fellman, B.M.; Urbauer, D.L.; Mills, G.B.; Zhang, W.; Broaddus, R.R. CTNNB1 (Beta-Catenin) Mutation Identifies Low Grade, Early Stage Endometrial Cancer Patients at Increased Risk of Recurrence. Mod. Pathol. 2017, 30, 1032–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating Liquid Biopsies into the Management of Cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Herrero, C.; Abal, M.; Muinelo-Romay, L. Circulating Extracellular Vesicles in Gynecological Tumors: Realities and Challenges. Front. Oncol. 2020, 10, 565666. [Google Scholar] [CrossRef] [PubMed]
- Herrero, C.; de la Fuente, A.; Casas-Arozamena, C.; Sebastian, V.; Prieto, M.; Arruebo, M.; Abalo, A.; Colás, E.; Moreno-Bueno, G.; Gil-Moreno, A.; et al. Extracellular Vesicles-Based Biomarkers Represent a Promising Liquid Biopsy in Endometrial Cancer. Cancers 2019, 11, 2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffone, A.; Troisi, J.; Boccia, D.; Travaglino, A.; Capuano, G.; Insabato, L.; Mollo, A.; Guida, M.; Zullo, F. Metabolomics in Endometrial Cancer Diagnosis: A Systematic Review. Acta Obstet. Gynecol. Scand. 2020, 99, 1135–1146. [Google Scholar] [CrossRef] [PubMed]
- Silveira, A.B.; Bidard, F.C.; Kasperek, A.; Melaabi, S.; Tanguy, M.L.; Rodrigues, M.; Bataillon, G.; Cabel, L.; Buecher, B.; Pierga, J.Y.; et al. High-Accuracy Determination of Microsatellite Instability Compatible with Liquid Biopsies. Clin. Chem. 2020, 66, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Wörsdörfer, P.; Rockel, A.; Alt, Y.; Kern, A.; Ergün, S. Generation of Vascularized Neural Organoids by Co-Culturing with Mesodermal Progenitor Cells. STAR Protoc. 2020, 1, 100041. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Product | Concentration | Supplier | Catalog Number |
|---|---|---|---|
| DMEM/F12 | - | Lonza | 12-719F |
| h-R-spondin1 (hRSPO1) | 7.50 nM | Peprotech | 120-38 |
| h-noggin (hNOG) | 2.17 nM | Peprotech | 120-10C |
| B27 supplement | 2% | ThermoFisher | 17504044 |
| N2 supplement | 1% | ThermoFisher | 17502048 |
| Insulin-transferrin-selenium (ITS) | 1% | ThermoFisher | 41400045 |
| GlutaMAXTM supplement | 1% | ThermoFisher | 35050061 |
| Antibiotic-antimycotic | 1% | ThermoFisher | 15240062 |
| Nicotinamide (NICO) | 2 mM | Sigma-Aldrich | N0636 |
| A83-01 | 0.6 µM | Sigma-Aldrich | SML0788 |
| N-acetyl L-cysteine (NAC) | 1.25 mM | Sigma-Aldrich | A7250 |
| EGF | 8 nM | Peprotech | AF-100-15 |
| b-FGF | 0.1 nM | Peprotech | 100-18B |
| SB202190 (p38i) | 10 µM | Sigma-Aldrich | S7067 |
| 17-β estradiol | 1 nM | Sigma-Aldrich | E8875 |
| Y-27632 * | 10 µM | Selleckchem | S1049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casas-Arozamena, C.; Cortegoso, A.; Piñeiro-Perez, R.; Abalo, A.; Arias, E.; Sampayo, V.; Vilar, A.; Bouso, M.; Diaz, E.; Moreno-Bueno, G.; et al. Improving the Management of Endometrial Cancer Patients through the Use of Liquid Biopsy Analyses: A Case Report. Int. J. Mol. Sci. 2022, 23, 8539. https://doi.org/10.3390/ijms23158539
Casas-Arozamena C, Cortegoso A, Piñeiro-Perez R, Abalo A, Arias E, Sampayo V, Vilar A, Bouso M, Diaz E, Moreno-Bueno G, et al. Improving the Management of Endometrial Cancer Patients through the Use of Liquid Biopsy Analyses: A Case Report. International Journal of Molecular Sciences. 2022; 23(15):8539. https://doi.org/10.3390/ijms23158539
Chicago/Turabian StyleCasas-Arozamena, Carlos, Alexandra Cortegoso, Raquel Piñeiro-Perez, Alicia Abalo, Efigenia Arias, Victoria Sampayo, Ana Vilar, Marta Bouso, Eva Diaz, Gema Moreno-Bueno, and et al. 2022. "Improving the Management of Endometrial Cancer Patients through the Use of Liquid Biopsy Analyses: A Case Report" International Journal of Molecular Sciences 23, no. 15: 8539. https://doi.org/10.3390/ijms23158539
APA StyleCasas-Arozamena, C., Cortegoso, A., Piñeiro-Perez, R., Abalo, A., Arias, E., Sampayo, V., Vilar, A., Bouso, M., Diaz, E., Moreno-Bueno, G., López-López, R., Muinelo-Romay, L., Abal, M., & Cueva, J. (2022). Improving the Management of Endometrial Cancer Patients through the Use of Liquid Biopsy Analyses: A Case Report. International Journal of Molecular Sciences, 23(15), 8539. https://doi.org/10.3390/ijms23158539