
The Gestational Effects of Maternal Bone Marker Molecules on Fetal Growth, Metabolism and Long-Term Metabolic Health: A Systematic Review

 ,
,  and
and 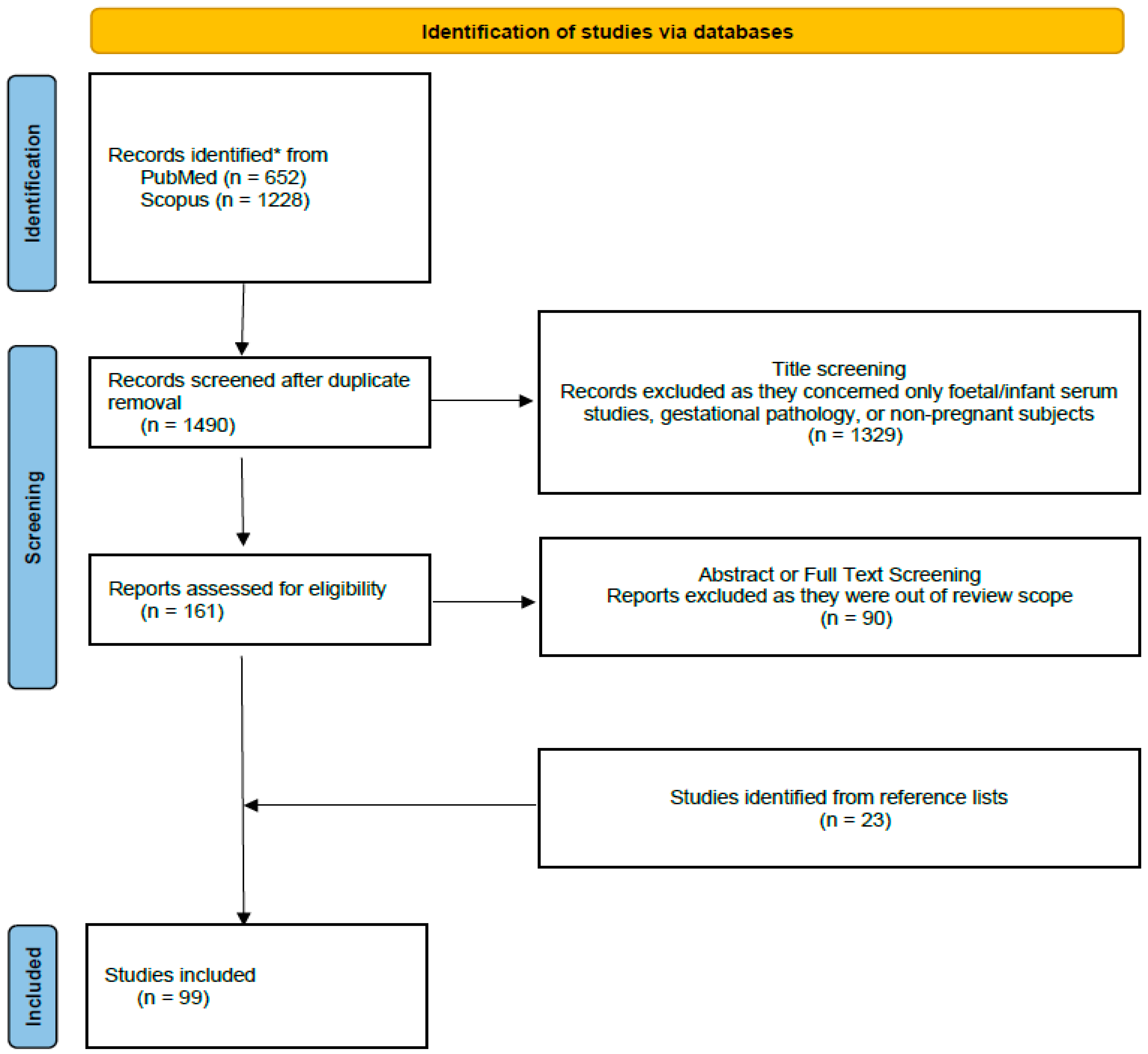{kind=link}
Abstract
1. Introduction
2. Methods
3. Results and Discussion
3.1. Maternal Bone Turnover Molecules during Pregnancy and Intrauterine Fetal Growth
3.1.1. Maternal Vit-D during Early Gestation and Intrauterine Fetal Growth
3.1.2. Maternal Vit-D during Second and Third Trimesters and Intrauterine Fetal Growth
3.1.3. Maternal Sclerostin and sRANKL during Pregnancy and Intrauterine Fetal Growth
3.2. Maternal Bone Turnover Molecules during Pregnancy and Anthropometrics at Birth
3.2.1. Maternal Vit-D during Early Gestation and Anthropometrics at Birth
3.2.2. Maternal Vit-D during Mid—Gestation and Anthropometrics at Birth
3.2.3. Maternal Vit-D during Third Trimester or Peripartum and Anthropometrics at Birth
3.2.4. Maternal Vit-D throughout Gestation and Anthropometrics at Birth
3.2.5. Randomized Control Trials and Systematic Reviews
3.2.6. Maternal Sclerostin Levels during Pregnancy and Anthropometrics at Birth
3.2.7. Maternal Osteocalcin Levels during Pregnancy and Anthropometrics at Birth
3.2.8. Maternal Osteoprotegerin Levels during Pregnancy and Anthropometrics at Birth
3.3. Maternal Bone Turnover Molecules during Pregnancy and Intrauterine Fetal Glucose Metabolism and Insulin Resistance
3.4. Maternal Bone Turnover Molecules during Pregnancy and Possible Metabolic, Endocrine, and Immunological Consequences in Offspring
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fitzgerald, E.; Hor, K.; Drake, A.J. Maternal influences on fetal brain development: The role of nutrition, infection and stress, and the potential for intergenerational consequences. Early Hum. Dev. 2020, 150, 105190. [Google Scholar] [CrossRef]
- Briana, D.D.; Malamitsi-Puchner, A. Perinatal biomarkers implying ‘Developmental Origins of Health and Disease’ consequences in intrauterine growth restriction. Acta Paediatr. 2020, 109, 1317–1322. [Google Scholar] [CrossRef] [PubMed]
- Cowan, C.S.M.; Callaghan, B.L.; Kan, J.M.; Richardson, R. The lasting impact of early-life adversity on individuals and their descendants: Potential mechanisms and hope for intervention. Genes Brain Behav. 2016, 15, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Kitsiou-Tzeli, S.; Tzetis, M. Maternal epigenetics and fetal and neonatal growth. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 24, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Namgung, R.; Tsang, R.C. Bone in the pregnant mother and newborn at birth. Clin. Chim. Acta. Int. J. Clin. Chem. 2003, 333, 1–11. [Google Scholar] [CrossRef]
- Anderson, P.H. Vitamin D Activity and Metabolism in Bone. Curr. Osteoporos Rep. 2017, 15, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Dimova, R.; Tankova, T.; Chakarova, N. Vitamin D in the Spectrum of Prediabetes and Cardiovascular Autonomic Dysfunction. J. Nutr. 2017, 2, jn250209. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.L.; Muyayalo, K.P.; Zhang, Y.H.; Hu, X.H.; Liao, A.H. Immunological function of vitamin D during human pregnancy. Am. J. Reprod. Immunol. 2017, 78, e12716. [Google Scholar] [CrossRef] [PubMed]
- Ciebiera, M.; Wojtyła, C.; Łukaszuk, K.; Zgliczyńska, M.; Zaręba, K.; Rawski, W.; Jakiel, G. The role of vitamin D in perinatology. An up-to-date review. Arch. Med. Sci. 2021, 17, 992–1005. [Google Scholar] [CrossRef]
- Franasiak, J.M.; Lara, E.E.; Pellicer, A. Vitamin D in human reproduction. Curr. Opin. Obstet. Gynecol. 2017, 29, 189–194. [Google Scholar] [CrossRef]
- Kim, R.H.; Ryu, B.J.; Lee, K.M.; Han, J.W.; Lee, S.K. Vitamin D facilitates trophoblast invasion through induction of epithelial-mesenchymal transition. Am. J. Reprod. Immunol. 2018, 79, e12796. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W.; Wagner, C.L. Vitamin D and pregnancy: Skeletal effects, nonskeletal effects, and birth outcomes. Calcif. Tissue Int. 2013, 92, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q. Vitamin D and pregnancy outcomes. Curr. Opin. Obstet. Gynecol. 2014, 26, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Palaniswamy, S.; Williams, D.; Järvelin, M.R.; Sebert, S. Vitamin D and the Promotion of Long-Term Metabolic Health from a Programming Perspective. Nutr. Metab. Insights. 2015, 8 (Suppl. 1), 11–21. [Google Scholar] [CrossRef]
- Chi, M.-Z.; Zhu, L.; Zhang, Z.-L.; Jin, F.-F.; Shao, H.-R.; Zheng, J.-Y.; Wu, C.; Hu, G.-Q. The Relationship between Maternal Serum Vitamin D Levels and Infant Neurodevelopment and Anthropometry: A Prospective Observational Study. J. Nutr. Sci. Vitaminol. 2018, 64, 161–167. [Google Scholar] [CrossRef]
- Hyde, N.K.; Brennan-Olsen, S.L.; Wark, J.D.; Hosking, S.M.; Holloway-Kew, K.L.; Pasco, J.A. Vitamin D during pregnancy and offspring body composition: A prospective cohort study. Pediatr Obes. 2018, 13, 514–521. [Google Scholar] [CrossRef]
- Lee, N.K.; Sowa, H.; Hinoi, E.; Ferron, M.; Ahn, J.D.; Confavreux, C.; Dacquin, R.; Mee, P.J.; McKee, M.D.; Jung, D.Y. Endocrine regulation of energy metabolism by the skeleton. Cell 2007, 130, 456–469. [Google Scholar] [CrossRef]
- Wei, J.; Karsenty, G. An overview of the metabolic functions of osteocalcin. Rev. Endocr. Metab Disord. 2015, 16, 93–98. [Google Scholar] [CrossRef]
- Lacey, D.L.; Timms, E.; Tan, H.L.; Kelley, M.J.; Dunstan, C.R.; Burgess, T.; Elliott, R.; Colombero, A.; Elliott, G.; Scully, S.; et al. Osteoprotegerin ligand is a cytokine that regulates osteoclast differentiation and activation. Cell 1998, 93, 165–176. [Google Scholar] [CrossRef]
- Hsu, H.; Lacey, D.L.; Dunstan, C.R.; Solovyev, I.; Colombero, A.; Timms, E.; Tan, H.-L.; Elliott, G.; Kelley, M.J.; Sarosi, I.; et al. Tumor necrosis factor receptor family member RANK mediates osteoclast differentiation and activation induced by osteoprotegerin ligand. Proc. Natl. Acad. Sci. USA 1999, 96, 3540–3545. [Google Scholar] [CrossRef]
- Briana, D.D.; Boutsikou, M.; Baka, S.; Hassiakos, D.; Gourgiotis, D.; Malamitsi-Puchner, A. Circulating Osteoprotegerin and sRANKL Concentrations in the Perinatal Period at Term. Neonatology 2009, 96, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Essley, B.; McNanley, T.; Cooper, B.; McIntyre, A.; Witter, F.; Harris, Z.; O’Brien, K. Osteoprotegerin in pregnant adolescents differs by race and is related to infant birth weight z -score. J. Dev. Orig Health Dis. 2011, 2, 272–279. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Delgado-Calle, J.; Sato, A.Y.; Bellido, T. Role and mechanism of action of sclerostin in bone. Bone 2017, 96, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Cain, C.J.; Rueda, R.; McLelland, B.; Collette, N.M.; Loots, G.G.; Manilay, J.O. Absence of sclerostin adversely affects B-cell survival. J. Bone Miner Res. Off. J. Am. Soc. Bone Miner. Res. 2012, 27, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Koos, R.; Brandenburg, V.; Mahnken, A.H.; Schneider, R.; Dohmen, G.; Autschbach, R.; Marx, N.; Kramann, R. Sclerostin as a potential novel biomarker for aortic valve calcification: An in-vivo and ex-vivo study. J. Heart Valve Dis. 2013, 22, 317–325. [Google Scholar] [PubMed]
- Amrein, K.; Amrein, S.; Drexler, C.; Dimai, H.P.; Dobnig, H.; Pfeifer, K.; Tomaschitz, A.; Pieber, T.R.; Fahrleitner-Pammer, A. Sclerostin and its association with physical activity, age, gender, body composition, and bone mineral content in healthy adults. J. Clin. Endocrinol. Metab. 2012, 97, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Urano, T.; Shiraki, M.; Ouchi, Y.; Inoue, S. Association of circulating sclerostin levels with fat mass and metabolic disease--related markers in Japanese postmenopausal women. J. Clin. Endocrinol. Metab. 2012, 97, E1473–E1477. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Riddle, R.C.; Clemens, T.L. Bone and the regulation of global energy balance. J. Intern. Med. 2015, 277, 681–689. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Amegah, A.K.; Nsoh, M.; Ashley-Amegah, G.; Anaman-Togbor, J. What factors influences dietary and non-dietary vitamin D intake among pregnant women in an African population? Nutrition 2018, 50, 36–44. [Google Scholar] [CrossRef]
- Richard, A.; Rohrmann, S.; Quack Lötscher, K. Prevalence of Vitamin D Deficiency and Its Associations with Skin Color in Pregnant Women in the First Trimester in a Sample from Switzerland. Nutrients 2017, 9, 260. [Google Scholar] [CrossRef] [PubMed]
- Man, R.; Li, L.J.; Cheng, C.Y.; Wong, T.; Lamoureux, E.; Sabanayagam, C. Prevalence and Determinants of Suboptimal Vitamin D Levels in a Multiethnic Asian Population. Nutrients 2017, 9, 313. [Google Scholar] [CrossRef]
- Lowe, N.M.; Bhojani, I. Special considerations for vitamin D in the south Asian population in the UK. Adv. Musculoskelet Dis. 2017, 9, 137–144. [Google Scholar] [CrossRef]
- Josefson, J.L.; Reisetter, A.; Scholtens, D.M.; Price, H.E.; Metzger, B.E.; Langman, C.B.; HAPO Study Cooperative Research Group. Maternal BMI Associations with Maternal and Cord Blood Vitamin D Levels in a North American Subset of Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study Participants. Nerurkar PV, editor. PLoS ONE 2016, 11, e0150221. [Google Scholar] [CrossRef] [PubMed]
- Gilani, S.; Janssen, P. Maternal Vitamin D Levels During Pregnancy and Their Effects on Maternal—Fetal Outcomes: A Systematic Review. J. Obstet. Gynaecol. Can. 2020, 42, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhang, C.; Wang, Y.; Zhao, J.; Li, H.; Shen, Q.; Wang, X.; Ni, M.; Ouyang, F.; Vinturache, A.; et al. Relationship of maternal obesity and vitamin D concentrations with fetal growth in early pregnancy. Eur. J. Nutr. 2022, 61, 915–924. [Google Scholar] [CrossRef]
- Judistiani, R.T.D.; Madjid, T.H.; Irianti, S.; Natalia, Y.A.; Indrati, A.R.; Ghozali, M.; Sribudiani, Y.; Yuniati, T.; Abdulah, R.; Setiabudiawan, B. Association of first trimester maternal vitamin D, ferritin and hemoglobin level with third trimester fetal biometry: Result from cohort study on vitamin D status and its impact during pregnancy and childhood in Indonesia. BMC Pregnancy Childbirth 2019, 19, 112. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.M.; Kilbane, M.; McGowan, C.A.; McKenna, M.J.; McAuliffe, F.M. Pregnancy in dark winters: Implications for fetal bone growth? Fertil. Steril. 2013, 99, 206–211. [Google Scholar] [CrossRef]
- Lee, D.H.; Ryu, H.M.; Han, Y.J.; Lee, S.W.; Park, S.Y.; Yim, C.H.; Kim, S.H.; Yoon, H.K. Effects of Serum 25-hydroxy-vitamin D and Fetal Bone Growth during Pregnancy. J. Bone Metab. 2015, 22, 127. [Google Scholar] [CrossRef][Green Version]
- Aydeniz, E.G.; Sari, U.; Tekin, I.; Dilek, T.U.K. The Relationship between First Trimester 25-Hydroxyvitamin D3 Levels and Second Trimester Femur Length and Their Effects on Birth Weight and Length at Birth: A Preliminary Study. Obs. Gynecol. Int. 2019, 2019, 1–4. [Google Scholar] [CrossRef]
- Morales, E.; Rodriguez, A.; Valvi, D.; Iñiguez, C.; Esplugues, A.; Vioque, J.; Marina, L.S.; Jiménez, A.; Espada, M.; Dehli, C.R.; et al. Deficit of vitamin D in pregnancy and growth and overweight in the offspring. Int. J. Obes. 2015, 39, 61–68. [Google Scholar] [CrossRef]
- Fernández-Alonso, A.M.; Fiol-Ruiz, G.; Chedraui, P.; Pérez-López, F.R. Lack of correlation between first trimester maternal serum 25-hydroxyvitamin D levels and ultrasound measured crown-rump length and nuchal translucency. Arch. Gynecol. Obstet. 2011, 284, 1585–1588. [Google Scholar] [CrossRef] [PubMed]
- Miliku, K.; Vinkhuyzen, A.; Blanken, L.M.E.; McGrath, J.; Eyles, D.; Burne, T.; Hofman, A.; Tiemeier, H.; Steegers, E.A.; Gaillard, R.; et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am. J. Clin. Nutr. 2016, 103, 1514–1522. [Google Scholar] [CrossRef]
- Sarma, D.; Saikia, U.; Das, D. Fetal skeletal size and growth are relevant biometric markers in Vitamin D deficient mothers: A North East India prospective cohort study. Indian J. Endocrinol. Metab. 2018, 22, 212. [Google Scholar] [CrossRef]
- Mahon, P.; Harvey, N.; Crozier, S.; Inskip, H.; Robinson, S.; Arden, N.; Swaminathan, R.; Cooper, C.; Godfrey, K.; SWS Study Group. Low maternal vitamin D status and fetal bone development: Cohort study. J. Bone Miner Res. 2010, 25, 14–19. [Google Scholar] [CrossRef]
- Ioannou, C.; Javaid, M.K.; Mahon, P.; Yaqub, M.K.; Harvey, N.C.; Godfrey, K.M.; Noble, J.A.; Cooper, C.; Papageorghiou, A.T. The Effect of Maternal Vitamin D Concentration on Fetal Bone. J. Clin. Endocrinol. Metab. 2012, 97, E2070–E2077. [Google Scholar] [CrossRef]
- Marçal, V.M.G.; Sousa, F.L.P.; Daher, S.; Grohmann, R.M.; Peixoto, A.B.; Júnior, E.A.; Nardozza, L.M.M. The Assessment of Vitamin D Levels in Pregnant Women is not Associated to Fetal Growth Restriction: A Cross Sectional Study. Rev. Bras. Ginecol. E Obs. RBGO Gynecol. Obstet. 2021, 43, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Galthen-Sørensen, M.; Andersen, L.B.; Sperling, L.; Christesen, H.T. Maternal 25-hydroxyvitamin D level and fetal bone growth assessed by ultrasound: A systematic review. Ultrasound Obs. Gynecol. 2014, 44, 633–640. [Google Scholar] [CrossRef]
- Mastorakos, G.; Maliopoulos, D.; Kasioni, S.; Bargiota, A.; Barber, T.M.; Skevaki, C.; Papassotiriou, I.; Vrachnis, N.; Farmakides, G.; Vlahos, N.F. Relationship Between Maternal Bone Biomarkers and Fetal Adiposity Through Normal Pregnancy. J. Clin. Endocrinol. Metab. 2021, 106, e2647–e2655. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.P.; Frey, J.L.; Li, Z.; Kushwaha, P.; Zoch, M.L.; Tomlinson, R.E.; Da, H.; Aja, S.; Noh, H.L.; Kim, J.K.; et al. Sclerostin influences body composition by regulating catabolic and anabolic metabolism in adipocytes. Proc. Natl. Acad. Sci. USA 2017, 114, E11238–E11247. [Google Scholar] [CrossRef] [PubMed]
- Fairfield, H.; Falank, C.; Harris, E.; Demambro, V.; McDonald, M.; Pettitt, J.A.; Mohanty, S.T.; Croucher, P.; Kramer, I.; Kneissel, M.; et al. The skeletal cell-derived molecule sclerostin drives bone marrow adipogenesis. J. Cell Physiol. 2018, 233, 1156–1167. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, N.; Bourgoin, L.; Biver, E.; Douni, E.; Ferrari, S. RANKL inhibition improves muscle strength and insulin sensitivity and restores bone mass. J. Clin. Invest. 2019, 129, 3214–3223. [Google Scholar] [CrossRef] [PubMed]
- Kiechl, S.; Wittmann, J.; Giaccari, A.; Knoflach, M.; Willeit, P.; Bozec, A.; Moschen, A.R.; Muscogiuri, G.; Sorice, G.P.; Kireva, T.; et al. Blockade of receptor activator of nuclear factor-κB (RANKL) signaling improves hepatic insulin resistance and prevents development of diabetes mellitus. Nat Med. 2013, 19, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xiao, Y.; Zhang, L.; Gao, Q. Maternal early pregnancy vitamin D status in relation to low birth weight and small-for-gestational-age offspring. J. Steroid. Biochem. Mol. Biol. 2018, 175, 146–150. [Google Scholar] [CrossRef]
- Fernando, M.; Coster, T.G.; Ellery, S.J.; de Guingand, D.; Lim, S.; Harrison, C.L.; Teede, H.J.; Naderpoor, N.; Mousa, A. Relationships between Total, Free and Bioavailable Vitamin D and Vitamin D Binding Protein in Early Pregnancy with Neonatal Outcomes: A Retrospective Cohort Study. Nutrients 2020, 12, 2495. [Google Scholar] [CrossRef]
- Leffelaar, E.R.; Vrijkotte, T.G.M.; van Eijsden, M. Maternal early pregnancy vitamin D status in relation to fetal and neonatal growth: Results of the multi-ethnic Amsterdam Born Children and their Development cohort. Br. J. Nutr. 2010, 104, 108–117. [Google Scholar] [CrossRef]
- Van den Berg, G.; van Eijsden, M.; Vrijkotte, T.G.M.; Gemke, R.J.B.J. Suboptimal maternal vitamin D status and low education level as determinants of small-for-gestational-age birth weight. Eur. J. Nutr. 2013, 52, 273–279. [Google Scholar] [CrossRef]
- Gernand, A.D.; Simhan, H.N.; Klebanoff, M.A.; Bodnar, L.M. Maternal Serum 25-Hydroxyvitamin D and Measures of Newborn and Placental Weight in a U.S. Multicenter Cohort Study. J. Clin. Endocrinol. Metab. 2013, 98, 398–404. [Google Scholar] [CrossRef]
- Rodriguez, A.; García-Esteban, R.; Basterretxea, M.; Lertxundi, A.; Rodríguez-Bernal, C.; Iñiguez, C.; Rodriguez-Dehli, C.; Tardón, A.; Espada, M.; Sunyer, J.; et al. Associations of maternal circulating 25-hydroxyvitamin D3 concentration with pregnancy and birth outcomes. BJOG Int. J. Obs. Gynaecol. 2015, 122, 1695–1704. [Google Scholar] [CrossRef]
- Schneuer, F.J.; Roberts, C.L.; Guilbert, C.; Simpson, J.M.; Algert, C.S.; Khambalia, A.Z.; Tasevski, V.; Ashton, A.W.; Morris, J.M.; Nassar, N. Effects of maternal serum 25-hydroxyvitamin D concentrations in the first trimester on subsequent pregnancy outcomes in an Australian population. Am. J. Clin. Nutr. 2014, 99, 287–295. [Google Scholar] [CrossRef]
- Aji, A.S.; Yusrawati, Y.; GMalik, S.; Lipoeto, N.I. The Association of Maternal Vitamin D Status during Pregnancy and Neonatal Anthropometric Measurements: A Longitudinal Study in Minangkabau Pregnant Women, Indonesia. J. Nutr. Sci. Vitaminol. 2020, 66, S63–S70. [Google Scholar] [CrossRef] [PubMed]
- Yuniati, T.; Judistiani, R.T.D.; Natalia, Y.A.; Irianti, S.; Madjid, T.H.; Ghozali, M.; Sribudiani, Y.; Indrati, A.R.; Abdulah, R.; Setiabudiawan, B. First trimester maternal vitamin D, ferritin, hemoglobin level and their associations with neonatal birthweight: Result from cohort study on vitamin D status and its impact during pregnancy and childhood in Indonesia. J. Neonatal-Perinat Med. 2020, 13, 63–69. [Google Scholar] [CrossRef]
- Park, S.; Yoon, H.K.; Ryu, H.M.; Han, Y.J.; Lee, S.W.; Park, B.K.; Park, S.Y.; Yim, C.H.; Kim, S.H. Maternal Vitamin D Deficiency in Early Pregnancy Is Not Associated with Gestational Diabetes Mellitus Development or Pregnancy Outcomes in Korean Pregnant Women in a Prospective Study. J. Nutr. Sci. Vitaminol. 2014, 60, 269–275. [Google Scholar] [CrossRef]
- Liu, Z.; Meng, T.; Liu, J.; Xu, X.; Luo, S.; Jin, C.; Han, N.; Wang, H.J. The individual and joint effects of maternal 25(OH)D deficiency and gestational diabetes on infant birth size. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 2398–2405. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Pang, T.; Li, P.; Zhou, Z.; Lin, D.; Fan, D.; Guo, X.; Liu, Z. Early pregnancy vitamin D and the risk of adverse maternal and infant outcomes: A retrospective cohort study. BMC Pregnancy Childbirth. 2020, 20, 465. [Google Scholar] [CrossRef] [PubMed]
- Casey, C.; McGinty, A.; Holmes, V.A.; Patterson, C.C.; Young, I.S.; McCance, D.R. Maternal vitamin D and neonatal anthropometrics and markers of neonatal glycaemia: Belfast Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study. Br. J. Nutr. 2018, 120, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Mosavat, M.; Arabiat, D.; Smyth, A.; Newnham, J.; Whitehead, L. Second-trimester maternal serum vitamin D and pregnancy outcome: The Western Australian Raine cohort study. Diabetes Res. Clin. Pract. 2021, 175, 108779. [Google Scholar] [CrossRef]
- Morley, R.; Carlin, J.B.; Pasco, J.A.; Wark, J.D. Maternal 25-Hydroxyvitamin D and Parathyroid Hormone Concentrations and Offspring Birth Size. J. Clin. Endocrinol. Metab. 2006, 91, 906–912. [Google Scholar] [CrossRef]
- Gernand, A.D.; Simhan, H.N.; Caritis, S.; Bodnar, L.M. Maternal Vitamin D Status and Small-for-Gestational-Age Offspring in Women at High Risk for Preeclampsia. Obs. Gynecol. 2014, 123, 40–48. [Google Scholar] [CrossRef]
- Burris, H.H.; Rifas-Shiman, S.L.; Camargo, C.A.; Litonjua, A.A.; Huh, S.Y.; Rich-Edwards, J.W.; Gillman, M.W. Plasma 25-hydroxyvitamin D during pregnancy and small-for-gestational age in black and white infants. Ann Epidemiol. 2012, 22, 581–586. [Google Scholar] [CrossRef][Green Version]
- Eckhardt, C.L.; Gernand, A.D.; Roth, D.E.; Bodnar, L.M. Maternal vitamin D status and infant anthropometry in a US multi-centre cohort study. Ann. Hum. Biol. 2015, 42, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Holzman, C.; Siega-Riz, A.M.; Williams, M.A.; Dole, N.; Enquobahrie, D.A.; Ferre, C.D. Maternal Serum 25-Hydroxyvitamin D Concentrations during Pregnancy and Infant Birthweight for Gestational Age: A Three-Cohort Study: Maternal vitamin D and infant birthweight for gestational age. Paediatr Perinat Epidemiol. 2016, 30, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Eggemoen, Å.R.; Jenum, A.K.; Mdala, I.; Knutsen, K.V.; Lagerløv, P.; Sletner, L. Vitamin D levels during pregnancy and associations with birth weight and body composition of the newborn: A longitudinal multiethnic population-based study. Br. J. Nutr. 2017, 117, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Kang, C.; Wang, J.; Cui, X.; Hong, Q.; Wang, X.; Zhu, L.; Xu, P.; Fu, Z.; You, L. Association of maternal serum 25-hydroxyvitamin D concentrations in second and third trimester with risk of macrosomia. Sci. Rep. 2018, 8, 6169. [Google Scholar] [CrossRef] [PubMed]
- Tint, M.T.; Chong, M.F.; Aris, I.M.; Godfrey, K.M.; Quah, P.L.; Kapur, J.; Saw, S.M.; Gluckman, P.D.; Rajadurai, V.S.; Yap, F.; et al. Association between maternal mid-gestation vitamin D status and neonatal abdominal adiposity. Int. J. Obes. 2018, 42, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Godang, K.; Frøslie, K.F.; Henriksen, T.; Qvigstad, E.; Bollerslev, J. Seasonal variation in maternal and umbilical cord 25(OH) vitamin D and their associations with neonatal adiposity. Eur. J. Endocrinol. 2014, 170, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Catov, J.M.; Zmuda, J.M.; Cooper, M.E.; Parrott, M.S.; Roberts, J.M.; Marazita, M.L.; Simhan, H.N. Maternal Serum 25-Hydroxyvitamin D Concentrations Are Associated with Small-for-Gestational Age Births in White Women. J. Nutr. 2010, 140, 999–1006. [Google Scholar] [CrossRef]
- Yu, L.; Ke, H.J.; Che, D.; Guo, Y.; Wu, J.L. Large retrospective cohort study of the association between maternal 25-hydroxyvitamin D status and birth weight of neonate. J. Matern. Fetal. Neonatal. Med. 2021, 5, 1–7. [Google Scholar] [CrossRef]
- Boyle, V.T.; Thorstensen, E.B.; Mourath, D.; Jones, M.B.; McCowan, L.M.E.; Kenny, L.C.; Barker, P.N. The relationship between 25-hydroxyvitamin D concentration in early pregnancy and pregnancy outcomes in a large, prospective cohort. Br. J. Nutr. 2016, 116, 1409–1415. [Google Scholar] [CrossRef]
- Zhou, J.; Su, L.; Liu, M.; Liu, Y.; Cao, X.; Wang, Z.; Xiao, H. Associations between 25-hydroxyvitamin D levels and pregnancy outcomes: A prospective observational study in southern China. Eur. J. Clin. Nutr. 2014, 68, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Bärebring, L.; Bullarbo, M.; Glantz, A.; Hulthén, L.; Ellis, J.; Jagner, Å.; Schoenmakers, I.; Winkvist, A.; Augustin, H. Trajectory of vitamin D status during pregnancy in relation to neonatal birth size and fetal survival: A prospective cohort study. BMC Pregnancy Childbirth. 2018, 18, 51. [Google Scholar] [CrossRef] [PubMed]
- Shakeri, M.; Jafarirad, S. The relationship between maternal vitamin D status during third trimester of pregnancy and maternal and neonatal outcomes: A longitudinal study. Int. J. Reprod. Biomed. 2019, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Wierzejska, R.; Jarosz, M.; Klemińska-Nowak, M.; Tomaszewska, M.; Sawicki, W.; Bachanek, M.; Siuba-Strzelińska, M. Maternal and Cord Blood Vitamin D Status and Anthropometric Measurements in Term Newborns at Birth. Front. Endocrinol. 2018, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Velkavrh, M.; Paro-Panjan, D.; Benedik, E.; Mis, N.F.; Godnov, U.; Salamon, A.S. The Influence of Maternal Levels of Vitamin D and Adiponectin on Anthropometrical Measures and Bone Health in Offspring. PRILOZI 2019, 40, 91–98. [Google Scholar] [CrossRef][Green Version]
- Wang, Y.; Li, H.; Zheng, M.; Wu, Y.; Zeng, T.; Fu, J.; Zeng, D. Maternal vitamin D deficiency increases the risk of adverse neonatal outcomes in the Chinese population: A prospective cohort study. Rosenfeld CS, editor. PLoS ONE 2018, 13, e0195700. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Goel, P.; Chawla, D.; Huria, A.; Arya, A. Vitamin D Status in Mothers and Their Newborns and Its Association with Pregnancy Outcomes: Experience from a Tertiary Care Center in Northern India. J. Obstet. Gynecol. India. 2018, 68, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, T.N. Relationship of Low Maternal Vitamin D3 Level and Adverse Early Neonatal Outcomes. Indian J. Forensic. Med. Toxicol. 2021, 15, 1197. Available online: http://medicopublication.com/index.php/ijfmt/article/view/13580 (accessed on 20 April 2022).
- Lee, C.L.; Ng, B.K.; Wu, L.L.; Cheah, F.C.; Othman, H.; Ismail, N.A.M. Vitamin D deficiency in pregnancy at term: Risk factors and pregnancy outcomes. Horm. Mol. Biol. Clin. Investig. 2017, 31. [Google Scholar] [CrossRef] [PubMed]
- Laird, E.; Thurston, S.; van Wijngaarden, E.; Shamlaye, C.; Myers, G.; Davidson, P.; Watson, G.; McSorley, E.; Mulhern, M.; Yeates, A.; et al. Maternal Vitamin D Status and the Relationship with Neonatal Anthropometric and Childhood Neurodevelopmental Outcomes: Results from the Seychelles Child Development Nutrition Study. Nutrients 2017, 9, 1235. [Google Scholar] [CrossRef]
- Sandal, G.; Pirgon, O.; Dundar, B.; Cetin, H.; Bayram, H.I. Serum Sclerostin Levels in Newborns Born to Mothers With Vitamin D Deficiency. J. Investig. Med. 2015, 63, 878–881. [Google Scholar] [CrossRef] [PubMed]
- Dullaert, B.; Schroven, S.; Jacquemyn, Y. The effect of maternal vitamin D status on pregnancy outcome and child health in the first year of life. Clin. Exp. Obstet. Gynecol. 2018, 45, 677–681. [Google Scholar] [CrossRef]
- MohammadBeigi, R.; Fathollahpour, A.; Fathollahpour, A.; Kashanian, M.; Sheikhansari, N. A Comparison Between Maternal and Neonatal Serum Level of Vitamin D and Its Relationship with Anthropometric Neonatal Factors. J. Obstet. Gynecol. Cancer Res. 2021, 6, 116–121. [Google Scholar] [CrossRef]
- Francis, E.; Hinkle, S.; Song, Y.; Rawal, S.; Donnelly, S.; Zhu, Y.; Chen, L.; Zhang, C. Longitudinal Maternal Vitamin D Status during Pregnancy Is Associated with Neonatal Anthropometric Measures. Nutrients 2018, 10, 1631. [Google Scholar] [CrossRef] [PubMed]
- Boghossian, N.S.; Koo, W.; Liu, A.; Mumford, S.L.; Tsai, M.Y.; Yeung, E.H. Longitudinal measures of maternal vitamin D and neonatal body composition. Eur. J. Clin. Nutr. 2019, 73, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Benaim, C.; Carrilho, T.R.B.; Farias, D.R.; Kac, G. Vitamin D during pregnancy and its association with birth outcomes: A Brazilian cohort study. Eur. J. Clin. Nutr. 2021, 75, 489–500. [Google Scholar] [CrossRef]
- Chen, Y.H.; Fu, L.; Hao, J.H.; Yu, Z.; Zhu, P.; Wang, H.; Xu, Y.Y.; Zhang, C.; Tao, F.B.; Xu, D.X. Maternal Vitamin D Deficiency During Pregnancy Elevates the Risks of Small for Gestational Age and Low Birth Weight Infants in Chinese Population. J. Clin. Endocrinol. Metab. 2015, 100, 1912–1919. [Google Scholar] [CrossRef]
- Chen, B.; Chen, Y.; Xu, Y. Vitamin D deficiency in pregnant women: Influenced by multiple risk factors and increase the risks of spontaneous abortion and small-for-gestational age. Medicine 2021, 100, e27505. [Google Scholar] [CrossRef]
- Anim-Nyame, N.; Sooranna, S.R.; Jones, J.; Alaghband-Zadeh, J.; Steer, P.J.; Johnson, M.R. Biochemical markers of maternal bone turnover are elevated in pre-eclampsia. BJOG Int. J. Obstet. Gynaecol. 2001, 108, 258–262. [Google Scholar] [CrossRef]
- Shaarawy, M.; Zaki, S.; Ramzi, A.M.; Salem, M.E.; El-Minawi, A.M. Feto-maternal bone remodeling in normal pregnancy and preeclampsia. J. Soc.Gynecol. Investig. 2005, 12, 343–348. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Carvalho, G.Q.; dos Santos, D.B.; Oliveira, A.M. Influence of vitamin D serum concentration, prenatal care and social determinants on birth weight: A northeastern Brazilian cohort study. Br. J. Nutr. 2019, 122, 284–292. [Google Scholar] [CrossRef]
- Fang, K.; He, Y.; Mu, M.; Liu, K. Maternal vitamin D deficiency during pregnancy and low birth weight: A systematic review and meta-analysis. J. Matern. Fetal. Neonatal. Med. 2021, 34, 1167–1173. [Google Scholar] [CrossRef]
- Santamaria, C.; Bi, W.G.; Leduc, L.; Tabatabaei, N.; Jantchou, P.; Luo, Z.C.; Audibert, F.; Nuyt, A.M.; Wei, S.Q. Prenatal vitamin D status and offspring’s growth, adiposity and metabolic health: A systematic review and meta-analysis. Br. J. Nutr. 2018, 119, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Tous, M.; Villalobos, M.; Iglesias, L.; Fernández-Barrés, S.; Arija, V. Vitamin D status during pregnancy and offspring outcomes: A systematic review and meta-analysis of observational studies. Eur. J. Clin. Nutr. 2020, 74, 36–53. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016, 14, CD008873. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ 2013, 346, f1169. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A. Hernandez AV Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288.e4. [Google Scholar] [CrossRef] [PubMed]
- Dimas, A.; Politi, A.; Papaioannou, G.; Barber, T.M.; Weickert, M.O.; Grammatopoulos, D.K.; Kumar, S.; Kalantaridou, S.; Valsamakis, G. The Gestational Effects of Maternal Appetite Axis Molecules on Fetal Growth, Metabolism and Long-Term Metabolic Health: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 695. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, C. Maternal Vitamin D Deficiency and Fetal Growth. Donald Sch. J. Ultrasound Obs. Gynecol. 2015, 9, 223–229. [Google Scholar] [CrossRef]
- McGrath, J.J.; Keeping, D.; Saha, S.; Chant, D.C.; Lieberman, D.E.; O’Callaghan, M.J. Seasonal fluctuations in birth weight and neonatal limb length; does prenatal vitamin D influence neonatal size and shape? Early Hum. Dev. 2005, 81, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef]
- Jimenez-Lara, A.M.; Aranda, A. Interaction of Vitamin D and Retinoid Receptors on Regulation of Gene Expression. Horm. Res. Paediatr. 2000, 54, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.; Fuleihan, G.E.H.; Vieth, R. Vitamin D: A Growing Perspective. Crit. Rev. Clin. Lab. Sci. 2008, 45, 339–414. [Google Scholar] [CrossRef]
- Stevens, D.A.; Williams, G.R. Hormone regulation of chondrocyte differentiation and endochondral bone formation. Mol. Cell Endocrinol. 1999, 151, 195–204. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Maleki, M.; Sathyapalan, T.; Iranpanah, H.; Orafai, H.M.; Jamialahmadi, T.; Sahebkar, A. The molecular mechanisms by which vitamin D improve glucose homeostasis: A mechanistic review. Life Sci. 2020, 244, 117305. [Google Scholar] [CrossRef]
- Chagas, C.E.A.; Borges, M.C.; Martini, L.A.; Rogero, M.M. Focus on Vitamin D, Inflammation and Type 2 Diabetes. Nutrients 2012, 4, 52–67. [Google Scholar] [CrossRef]
- Pilz, S.; Kienreich, K.; Rutters, F.; de Jongh, R.; van Ballegooijen, A.J.; Grübler, M.; Tomaschitz, A.; Dekker, J.M. Role of Vitamin D in the Development of Insulin Resistance and Type 2 Diabetes. Curr. Diab. Rep. 2013, 13, 261–270. [Google Scholar] [CrossRef]
- Qin, L.L.; Lu, F.G.; Yang, S.H.; Xu, H.L.; Luo, B.A. Does Maternal Vitamin D Deficiency Increase the Risk of Preterm Birth: A Meta-Analysis of Observational Studies. Nutrients 2016, 8, 301. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, B.; Wu, X.; Li, S.; Tao, F. Association between maternal vitamin D deficiency and small for gestational age: Evidence from a meta-analysis of prospective cohort studies. BMJ Open 2017, 7, e016404. [Google Scholar] [CrossRef]
- Walker, V.P.; Zhang, X.; Rastegar, I.; Liu, P.T.; Hollis, B.W.; Adams, J.S.; Modlin, R.L. Cord Blood Vitamin D Status Impacts Innate Immune Responses. J. Clin. Endocrinol. Metab. 2011, 96, 1835–1843. [Google Scholar] [CrossRef]
- Bogazzi, F.; Rossi, G.; Lombardi, M.; Tomisti, L.; Sardella, C.; Manetti, L.; Curzio, O.; Marcocci, C.; Grasso, L.; Gasperi, M.; et al. Vitamin D status may contribute to serum insulin-like growth factor I concentrations in healthy subjects. J. Endocrinol. Investig. 2011, 34, e200–e203. [Google Scholar]
- Mitri, J.; Pittas, A.G. Vitamin D and diabetes. Endocrinol. Metab. Clin. N. Am. 2014, 43, 205–232. [Google Scholar] [CrossRef] [PubMed]
- Grundmann, M.; Haidar, M.; Haß, S.; Hubel, C.A.; von Versen-Höynck, F. OS063. Vitamin D promotes endothelial progenitor cell differentiationand upregulates VEGF. Pregnancy Hypertens Int. J. Womens Cardiovasc. Health 2012, 2, 211. [Google Scholar] [CrossRef]
- Cleal, J.K.; Day, P.E.; Simner, C.L.; Barton, S.J.; Mahon, P.A.; Inskip, H.M.; Godfrey, K.M.; Hanson, M.A.; Cooper, C.; Lewis, R.M.; et al. Placental amino acid transport may be regulated by maternal vitamin D and vitamin D-binding protein: Results from the Southampton Women’s Survey. Br. J. Nutr. 2015, 113, 1903–1910. [Google Scholar] [CrossRef] [PubMed]
- Yates, N.; Crew, R.C.; Wyrwoll, C.S. Vitamin D deficiency and impaired placental function: Potential regulation by glucocorticoids? Reproduction 2017, 153, R163–R171. [Google Scholar] [CrossRef]
- Ashley, B.; Simner, C.; Manousopoulou, A.; Jenkinson, C.; Hey, F.; Frost, J.M.; Rezwan, F.I.; White, C.H.; Lofthouse, E.M.; Hyde, E.; et al. Placental uptake and metabolism of 25(OH)vitamin D determine its activity within the fetoplacental unit. eLife 2022, 11, e71094. [Google Scholar] [CrossRef]
- Shin, J.S.; Choi, M.Y.; Longtine, M.S.; Nelson, D.M. Vitamin D effects on pregnancy and the placenta. Placenta 2010, 31, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Briana, D.D.; Boutsikou, M.; Marmarinos, A.; Gourgiotis, D.; Malamitsi-Puchner, A. Perinatal sclerostin concentrations in abnormal fetal growth: The impact of gestational diabetes. J. Matern. Fetal. Neonatal. Med. 2019, 32, 2228–2232. [Google Scholar] [CrossRef]
- Godang, K.; Frøslie, K.F.; Henriksen, T.; Isaksen, G.A.; Voldner, N.; Lekva, T.; Ueland, T.; Bollerslev, J. Umbilical cord levels of sclerostin, placental weight, and birth weight are predictors of total bone mineral content in neonates. Eur. J. Endocrinol. 2013, 168, 371–378. [Google Scholar] [CrossRef]
- Wei, L.; Cao, D.; Zhu, X.; Long, Y.; Liu, C.; Huang, S.; Tian, J.; Hou, Q.; Huang, Y.; Ye, J.; et al. High maternal osteocalcin levels during pregnancy is associated with low birth weight infants: A nested case-control study in China. Bone 2018, 116, 35–41. [Google Scholar] [CrossRef]
- Meng, Y.H.; Zhou, W.J.; Jin, L.P.; Liu, L.B.; Chang, K.K.; Mei, J.; Li, H.; Wang, J.; Li, D.J.; Li, M.Q. RANKL-mediated harmonious dialogue between fetus and mother guarantees smooth gestation by inducing decidual M2 macrophage polarization. Cell Death Dis. 2017, 8, e3105. [Google Scholar] [CrossRef]
- Lindberg, B.; Ivarsson, S.A.; Landin-Olsson, M.; Sundkvist, G.; Svanberg, L.; Lernmark, A. Islet autoantibodies in cord blood from children who developed Type I (insulin-dependent) diabetes mellitus before 15 years of age. Diabetologia 1999, 42, 181–187. [Google Scholar] [CrossRef]
- Kayaniyil, S.; Retnakaran, R.; Harris, S.B.; Vieth, R.; Knight, J.A.; Gerstein, H.C.; Perkins, B.A.; Zinman, B.; Hanley, A.J. Prospective Associations of Vitamin D With β-Cell Function and Glycemia. Diabetes 2011, 60, 2947–2953. [Google Scholar] [CrossRef]
- Oury, F.; Khrimian, L.; Denny, C.A.; Gardin, A.; Chamouni, A.; Goeden, N.; Huang, Y.; Lee, H.; Srinivas, P.; Gao, X.B.; et al. Maternal and Offspring Pools of Osteocalcin Influence Brain Development and Functions. Cell 2013, 155, 228–241. [Google Scholar] [CrossRef]
- Benjamin Neelon, S.E.; White, A.J.; Vidal, A.C.; Schildkraut, J.M.; Murtha, A.P.; Murphy, S.K.; Kullman, S.W.; Hoyo, C. Maternal vitamin D, DNA methylation at imprint regulatory regions and offspring weight at birth, 1 year and 3 years. Int. J. Obes. 2018, 42, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Lu, J.; Zhang, Y.; Teng, H.; Pei, J.; Zhang, C.; Guo, B.; Yin, J. Association between maternal vitamin D status with pregnancy outcomes and offspring growth in a population of Wuxi, China. Asia Pac. J. Clin. Nutr. 2021, 30, 464–476. [Google Scholar] [PubMed]
- Crozier, S.R.; Harvey, N.C.; Inskip, H.M.; Godfrey, K.M.; Cooper, C.; Robinson, S.M.; The SWS Study Group. Maternal vitamin D status in pregnancy is associated with adiposity in the offspring: Findings from the Southampton Women’s Survey. Am. J. Clin Nutr. 2012, 96, 57–63. [Google Scholar] [PubMed]
- Krishnaveni, G.V.; Veena, S.R.; Winder, N.R.; Hill, J.C.; Noonan, K.; Boucher, B.J.; Karat, S.C.; Fall, C.H. Maternal vitamin D status during pregnancy and body composition and cardiovascular risk markers in Indian children: The Mysore Parthenon Study. Am. J. Clin Nutr. 2011, 93, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.; Crozier, S.; Harvey, N.; Gale, C.; Dennison, E.; Boucher, B.; Arden, N.; Godfrey, K.; Cooper, C. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. The Lancet 2006, 367, 36–43. [Google Scholar] [CrossRef]
- Gale, C.R.; Robinson, S.M.; Harvey, N.C.; Javaid, M.K.; Jiang, B.; Martyn, C.N.; Godfrey, K.M.; Cooper, C. Maternal vitamin D status during pregnancy and child outcomes. Eur. J. Clin Nutr. 2008, 62, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Ong, Y.L.; Quah, P.L.; Tint, M.T.; Aris, I.M.; Chen, L.W.; van Dam, R.M.; Heppe, D.; Saw, S.M.; Godfrey, K.M.; Gluckman, P.D.; et al. The association of maternal vitamin D status with infant birth outcomes, postnatal growth and adiposity in the first 2 years of life in a multi-ethnic Asian population: The Growing Up in Singapore Towards healthy Outcomes (GUSTO) cohort study. Br. J. Nutr. 2016, 116, 621–631. [Google Scholar] [CrossRef]
- Rytter, D.; Bech, B.H.; Halldorsson, T.I.; Henriksen, T.B.; Grandström, C.; Cohen, A.; Olsen, S.F. Maternal Vitamin D Status at Week 30 of Gestation and Offspring Cardio-Metabolic Health at 20 Years: A Prospective Cohort Study over Two Decades. Slominski AT, editor. PLoS ONE 2016, 11, e0164758. [Google Scholar] [CrossRef] [PubMed]
- Hornsby, E.; Pfeffer, P.E.; Laranjo, N.; Cruikshank, W.; Tuzova, M.; Litonjua, A.A.; Weiss, S.T.; Carey, V.J.; O’Connor, G.; Hawrylowicz, C. Vitamin D supplementation during pregnancy: Effect on the neonatal immune system in a randomized controlled trial. J. Allergy Clin Immunol. 2018, 141, 269–278.e1. [Google Scholar] [CrossRef] [PubMed]
- Zosky, G.R.; Hart, P.H.; Whitehouse, A.J.O.; Kusel, M.M.; Ang, W.; Foong, R.E.; Chen, L.; Holt, P.G.; Sly, P.D.; Hall, G.L. Vitamin D Deficiency at 16 to 20 Weeks’ Gestation Is Associated with Impaired Lung Function and Asthma at 6 Years of Age. Ann. Am. Thorac. Soc. 2014, 11, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Pike, K.C.; Inskip, H.M.; Robinson, S.; Lucas, J.S.; Cooper, C.; Harvey, N.C.; Godfrey, K.M.; Roberts, G. Maternal late-pregnancy serum 25-hydroxyvitamin D in relation to childhood wheeze and atopic outcomes. Thorax 2012, 67, 950–956. [Google Scholar] [CrossRef]
- Morales, E.; Romieu, I.; Guerra, S.; Ballester, F.; Rebagliato, M.; Vioque, J.; Tardón, A.; Rodriguez Delhi, C.; Arranz, L.; Torrent, M.; et al. Maternal Vitamin D Status in Pregnancy and Risk of Lower Respiratory Tract Infections, Wheezing, and Asthma in Offspring. Epidemiology 2012, 23, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Erkkola, M.; Kaila, M.; Nwaru, B.I.; Kronberg-Kippilä, C.; Ahonen, S.; Nevalainen, J.; Veijola, R.; Pekkanen, J.; Ilonen, J.; Simell, O.; et al. Maternal vitamin D intake during pregnancy is inversely associated with asthma and allergic rhinitis in 5-year-old children. Clin Exp. Allergy. 2009, 39, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, I.M.; Joner, G.; Jenum, P.A.; Eskild, A.; Torjesen, P.A.; Stene, L.C. Maternal Serum Levels of 25-Hydroxy-Vitamin D During Pregnancy and Risk of Type 1 Diabetes in the Offspring. Diabetes 2012, 61, 175–178. [Google Scholar] [CrossRef]
- Stene, L.C.; Ulriksen, J.; Magnus, P.; Joner, G. Use of cod liver oil during pregnancy associated with lower risk of Type I diabetes in the offspring. Diabetologia 2000, 43, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Brekke, H.K.; Ludvigsson, J. Vitamin D supplementation and diabetes-related autoimmunity in the ABIS study. Pediatr Diabetes 2007, 8, 11–14. [Google Scholar] [CrossRef]
- Fronczak, C.M.; Barón, A.E.; Chase, H.P.; Ross, C.; Brady, H.L.; Hoffman, M.; Eisenbarth, G.S.; Rewers, M.; Norris, J.M. In Utero Dietary Exposures and Risk of Islet Autoimmunity in Children. Diabetes Care 2003, 26, 3237–3242. [Google Scholar] [CrossRef]
- Marjamäki, L.; Niinistö, S.; Kenward, M.G.; Uusitalo, L.; Uusitalo, U.; Ovaskainen, M.L.; Kronberg-Kippilä, C.; Simell, O.; Veijola, R.; Ilonen, J.; et al. Maternal intake of vitamin D during pregnancy and risk of advanced beta cell autoimmunity and type 1 diabetes in offspring. Diabetologia 2010, 53, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, M.E.; Reinert, L.; Kinnunen, L.; Harjutsalo, V.; Koskela, P.; Surcel, H.M.; Lamberg-Allardt, C.; Tuomilehto, J. Serum 25-hydroxyvitamin D level during early pregnancy and type 1 diabetes risk in the offspring. Diabetologia 2012, 55, 1291–1294. [Google Scholar] [CrossRef]
- Thomas, N.J.; Jones, S.E.; Weedon, M.N.; Shields, B.M.; Oram, R.A.; Hattersley, A.T. Frequency and phenotype of type 1 diabetes in the first six decades of life: A cross-sectional, genetically stratified survival analysis from UK Biobank. Lancet Diabetes Endocrinol 2018, 6, 122–129. [Google Scholar] [CrossRef]
- Ong, K.K.; Emmett, P.; Northstone, K.; Golding, J.; Rogers, I.; Ness, A.R.; Wells, J.C.; Dunger, D.B. Infancy Weight Gain Predicts Childhood Body Fat and Age at Menarche in Girls. J. Clin. Endocrinol. Metab. 2009, 94, 1527–1532. [Google Scholar] [CrossRef] [PubMed]
- Baird, J.; Fisher, D.; Lucas, P.; Kleijnen, J.; Roberts, H.; Law, C. Being big or growing fast: Systematic review of size and growth in infancy and later obesity. BMJ 2005, 331, 929. [Google Scholar] [CrossRef]
- Eriksson, J.G.; Kajantie, E.; Osmond, C.; Thornburg, K.; Barker, D.J.P. Boys live dangerously in the womb. Am. J. Hum. Biol. 2010, 22, 330–335. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimas, A.; Politi, A.; Bargiota, A.; Panoskaltsis, T.; Vlahos, N.F.; Valsamakis, G. The Gestational Effects of Maternal Bone Marker Molecules on Fetal Growth, Metabolism and Long-Term Metabolic Health: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 8328. https://doi.org/10.3390/ijms23158328
Dimas A, Politi A, Bargiota A, Panoskaltsis T, Vlahos NF, Valsamakis G. The Gestational Effects of Maternal Bone Marker Molecules on Fetal Growth, Metabolism and Long-Term Metabolic Health: A Systematic Review. International Journal of Molecular Sciences. 2022; 23(15):8328. https://doi.org/10.3390/ijms23158328
Chicago/Turabian StyleDimas, Angelos, Anastasia Politi, Alexandra Bargiota, Theodoros Panoskaltsis, Nikolaos F. Vlahos, and Georgios Valsamakis. 2022. "The Gestational Effects of Maternal Bone Marker Molecules on Fetal Growth, Metabolism and Long-Term Metabolic Health: A Systematic Review" International Journal of Molecular Sciences 23, no. 15: 8328. https://doi.org/10.3390/ijms23158328
APA StyleDimas, A., Politi, A., Bargiota, A., Panoskaltsis, T., Vlahos, N. F., & Valsamakis, G. (2022). The Gestational Effects of Maternal Bone Marker Molecules on Fetal Growth, Metabolism and Long-Term Metabolic Health: A Systematic Review. International Journal of Molecular Sciences, 23(15), 8328. https://doi.org/10.3390/ijms23158328