
A Cell-Based Systematic Review on the Role of Annexin A1 in Triple-Negative Breast Cancers

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Search for Relevant Studies
2.2. Selection of Articles
3. Results and Discussion
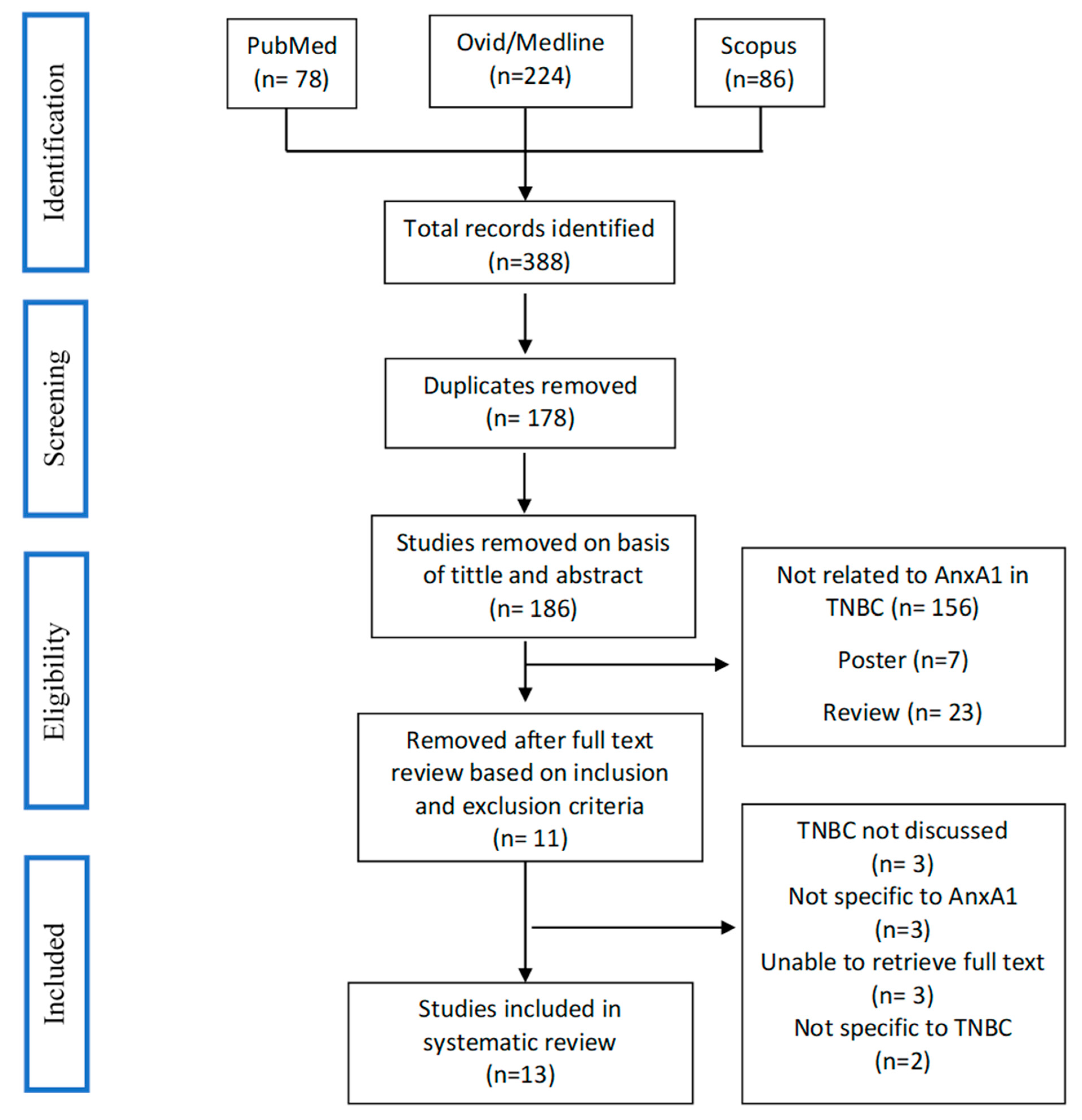
3.1. Study Selection
3.2. Data Extraction and Synthesis
3.3. Quality Assessment
3.4. AnxA1 Is a Subtype-Specific Markers in TNBC
3.5. AnxA1 Induces Epithelial-Mesenchymal Transition in TNBC
3.6. AnxA1 Diminishes Sensitivity of TNBC Cells to Apoptotic Signals
3.7. AnxA1 and Multidrug Resistance (MRD)
3.8. Immunomodulatory Role of AnxA1 in TNBC
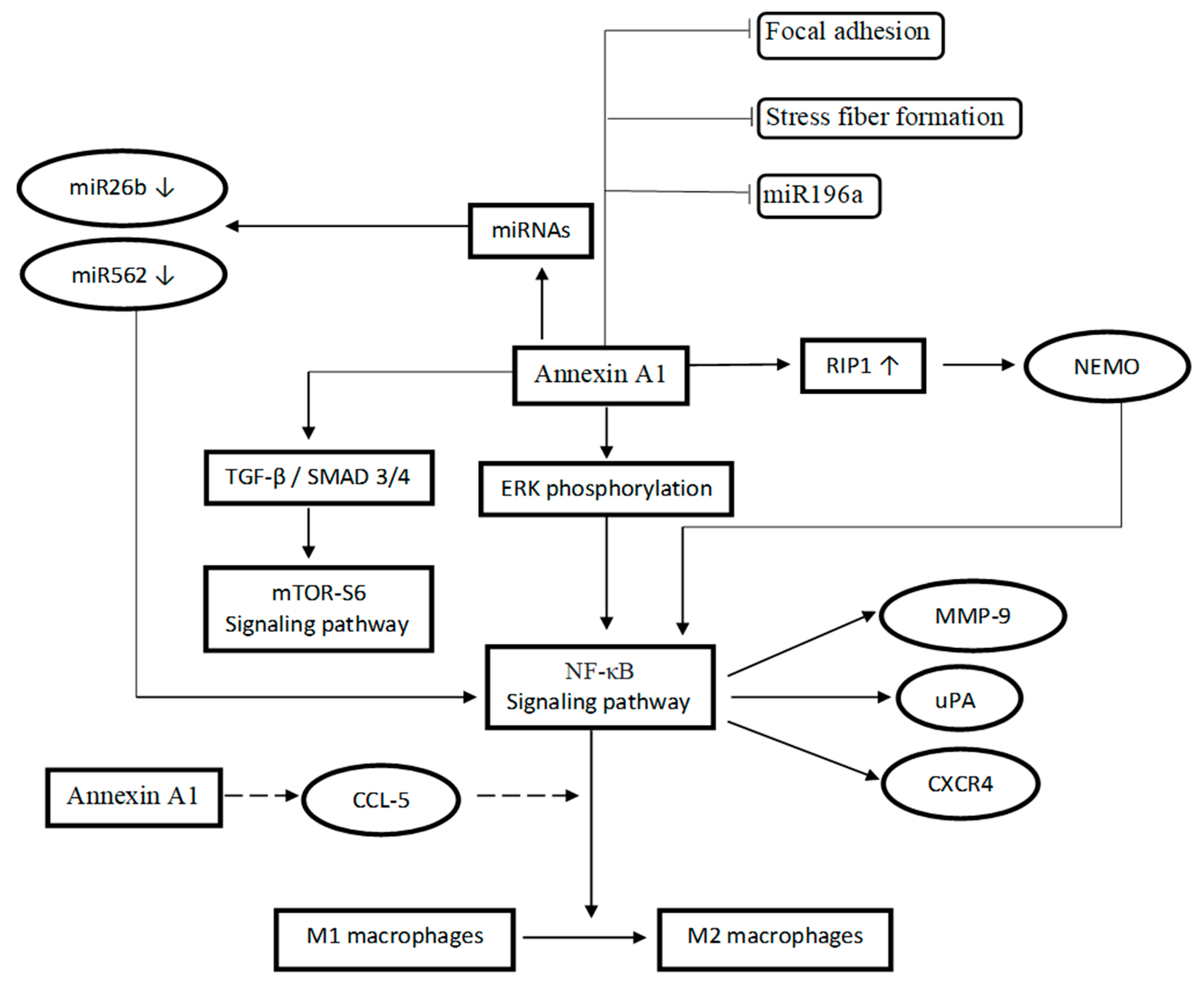
3.9. Mechanism of Action Related to AnxA1
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Competing interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Diana, A.; Franzese, E.; Centonze, S.; Carlino, F.; Della Corte, C.M.; Ventriglia, J.; Petrillo, A.; De Vita, F.; Alfano, R.; Ciardiello, F.; et al. Triple-Negative Breast Cancers: Systematic Review of the Literature on Molecular and Clinical Features with a Focus on Treatment with Innovative Drugs. Curr. Oncol. Rep. 2018, 20, 76. [Google Scholar] [CrossRef]
- Li, L.; Huang, H.; Zhu, M.; Wu, J. Identification of Hub Genes and Pathways of Triple Negative Breast Cancer by Expression Profiles Analysis. Cancer Manag. Res. 2021, 13, 2095–2104. [Google Scholar] [CrossRef]
- Stagg, J.; Allard, B. Immunotherapeutic Approaches in Triple- Negative Breast Cancer: Latest Research and Clinical Prospects. Ther. Adv. Med. Oncol. 2013, 5, 169–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Teijido, P.; Cabal, M.L.; Fernández, I.P.; Pérez, Y.F. Tumor-Infiltrating Lymphocytes in Triple Negative Breast Cancer: The Future of Immune Targeting. Clin. Med. Insights Oncol. 2016, 10, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, K.S.; Yi, Y.W.; Cho, J.; Park, J.S.; Seong, Y.S. Potentiating Therapeutic Effects of Epidermal Growth Factor Receptor Inhibition in Triple-Negative Breast Cancer. Pharmaceuticals 2021, 14, 589. [Google Scholar] [CrossRef]
- Varghese, E.; Samuel, S.M.; Abotaleb, M.; Cheema, S.; Mamtani, R.; Büsselberg, D. The “Yin and Yang” of Natural Compounds in Anticancer Therapy of Triple-Negative Breast Cancers. Cancers 2018, 10, 346. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Ahn, J.; Kim, S. How Shall We Treat Early Triple-Negative Breast Cancer (TNBC): From the Current Standard to Upcoming Immuno- Molecular Strategies. ESMO Open 2018, 3, e000357. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhan, Z.; Yin, X.; Fu, S.; Deng, X. Targeted Therapeutic Strategies for Triple-Negative Breast Cancer. Front. Oncol. 2021, 11, 4517. [Google Scholar] [CrossRef]
- Jhan, J.R.; Andrechek, E.R. Triple-Negative Breast Cancer and the Potential for Targeted Therapy. Pharmacogenomics 2017, 18, 1595–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugimoto, M.A.; Vago, J.P.; Teixeira, M.M.; Sousa, L.P. Annexin A1 and the Resolution of Inflammation: Modulation of Neutrophil Recruitment, Apoptosis, and Clearance. J. Immunol. Res. 2016, 2016, 8239258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, H.; Ko, J.; Jang, S.W. The Role of Annexin A1 in Expression of Matrix Metalloproteinase-9 and Invasion of Breast Cancer Cells. Biochem. Biophys. Res. Commun. 2012, 423, 188–194. [Google Scholar] [CrossRef]
- Yom, C.K.; Han, W.; Kim, S.W.; Kim, H.S.; Shin, H.C.; Chang, J.N.; Koo, M.; Noh, D.Y.; Moon, B.I. Clinical Significance of Annexin A1 Expression in Breast Cancer. J. Breast Cancer 2011, 14, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Okano, M.; Kumamoto, K.; Saito, M.; Onozawa, H.; Saito, K.; Abe, N.; Ohtake, T.; Takenoshita, S. Upregulated Annexin A1 Promotes Cellular Invasion in Triple-Negative Breast Cancer. Oncol. Rep. 2015, 33, 1064–1070. [Google Scholar] [CrossRef] [Green Version]
- Moraes, L.A.; Ampomah, P.B.; Lim, L.H.K.; Moraes, L.A.; Ampomah, P.B.; Annexin, L.H.K.L. Annexin A1 in Inflammation and Breast Cancer: A New Axis in the Tumor Microenvironment. Cell Adh. Migr. 2018, 12, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Boudhraa, Z.; Bouchon, B.; Viallard, C.; D’Incan, M.; Degoul, F. Annexin A1 Localization and Its Relevance to Cancer. Clin. Sci. 2016, 130, 205–220. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Johnstone, C.N.; Stewart, A.G. Annexin A1 Influences in Breast Cancer: Controversies on Contributions to Tumour, Host and Immunoediting Processes. Pharmacol. Res. 2017, 119, 278–288. [Google Scholar] [CrossRef]
- Ganesan, T.; Sinniah, A.; Ibrahim, Z.A.; Chik, Z.; Alshawsh, M.A. Annexin A1: A Bane or a Boon in Cancer? A Systematic Review. Molecules 2020, 25, 3700. [Google Scholar] [CrossRef]
- Bhardwaj, A.; Ganesan, N.; Tachibana, K.; Rajapakshe, K.; Albarracin, C.T.; Gunaratne, P.H.; Coarfa, C.; Bedrosian, I. Annexin A1 Preferentially Predicts Poor Prognosis of Basal-like Breast Cancer Patients by Activating MTOR-S6 Signaling. PLoS ONE 2015, 10, e0127678. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.; Group, P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.J.; Gardner, M.; Higgins, J.; Holly, J.M.P.; Gaunt, T.R.; Claire, M. Developing the WCRF International/University of Bristol Methodology for Identifying and Carrying out Systematic Reviews of Mechanisms of Exposure-Cancer Associations. Cancer Epidemiol. Biomark. Prev. 2018, 26, 1667–1675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Applegate, C.C.; Rowles, J.L.; Erdman, J.W. Can Lycopene Impact the Androgen Axis in Prostate Cancer?: A Systematic Review of Cell Culture and Animal Studies. Nutrients 2019, 11, 633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anbalagan, D.; Yap, G.; Yuan, Y.; Pandey, V.K.; Lau, W.H.; Arora, S.; Bist, P.; Wong, J.S.B.; Sethi, G.; Nissom, P.M.; et al. Annexin-A1 Regulates MicroRNA-26b* and MicroRNA-562 to Directly Target NF-κB and Angiogenesis in Breast Cancer Cells. PLoS ONE 2014, 9, e114507. [Google Scholar] [CrossRef]
- Bist, P.; Leow, S.C.; Phua, Q.H.; Shu, S.; Zhuang, Q.; Loh, W.T.; Nguyen, T.H.; Zhou, J.B.; Hooi, S.C.; Lim, L.H.K. Annexin-1 Interacts with NEMO and RIP1 to Constitutively Activate IKK Complex and NF-B: Implication in Breast Cancer Metastasis. Oncogene 2011, 30, 3174–3185. [Google Scholar] [CrossRef] [Green Version]
- De Graauw, M.; Van Miltenburg, M.H.; Schmidt, M.K.; Pont, C.; Lalai, R.; Kartopawiro, J.; Pardali, E.; Le Dévédec, S.E.; Smit, V.T.; Van Der Wal, A.; et al. Annexin A1 Regulates TGF-β Signaling and Promotes Metastasis Formation of Basal-like Breast Cancer Cells. Proc. Natl. Acad. Sci. USA 2010, 107, 6340–6345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khau, T.; Langenbach, S.Y.; Schuliga, M.; Harris, T.; Johnstone, C.N.; Anderson, R.L.; Stewart, A.G. Annexin-1 Signals Mitogen-Stimulated Breast Tumor Cell Proliferation by Activation of the Formyl Peptide Receptors (FPRs) 1 and 2. FASEB J. 2011, 25, 483–496. [Google Scholar] [CrossRef]
- Moraes, L.A.; Kar, S.; Foo, S.L.; Gu, T.; Toh, Y.Q.; Ampomah, P.B.; Sachaphibulkij, K.; Yap, G.; Zharkova, O.; Lukman, H.M.; et al. Annexin-A1 Enhances Breast Cancer Growth and Migration by Promoting Alternative Macrophage Polarization in the Tumour Microenvironment. Sci. Rep. 2017, 7, 17925. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Serfass, L.; Roy, M.O.; Wong, J.; Bonneau, A.M.; Georges, E. Annexin-I Expression Modulates Drug Resistance in Tumor Cells. Biochem. Biophys. Res. Commun. 2004, 314, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Vecchi, L.; Zóia, M.A.P.; Santos, T.G.; de Oliveira Beserra, A.; Ramos, C.M.C.; Colombo, B.F.M.; Maia, Y.C.P.; de Andrade, V.P.; Mota, S.T.S.; de Araújo, T.G.; et al. Inhibition of the AnxA1/FPR1 Autocrine Axis Reduces MDA-MB-231 Breast Cancer Cell Growth and Aggressiveness in Vitro and in Vivo. Biochim. Biophys. Acta Mol. Cell Res. 2018, 1865, 1368–1382. [Google Scholar] [CrossRef]
- Yuan, Y.; Anbalagan, D.; Lee, L.H.; Samy, R.P.; Shanmugam, K.; Kumar, A.P.; Sethi, G.; Lobie, P.E.; Lim, H.K. ANXA1 Inhibits MiRNA-196a in a Negative Feedback Loop through NF-KB and c-Myc to Reduce Breast Cancer Proliferation. Oncotarget 2016, 7, 27007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zóia, M.A.P.; Azevedo, F.V.P.; Vecchi, L.; Mota, S.T.S.; Rodovalho, V.D.R.; Cordeiro, A.O.; Correia, L.I.V.; Silva, A.C.A.; Ávila, V.D.M.R.; de Araújo, T.G.; et al. Inhibition of Triple-Negative Breast Cancer Cell Aggressiveness by Cathepsin D Blockage: Role of Annexin A1. Int. J. Mol. Sci. 2019, 20, 1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Chen, Y.; Chen, H.; Jiang, P.; Yan, L.; Mo, D.; Tang, X.; Yan, F. DCST1-AS1 Promotes TGF-β-Induced Epithelial–Mesenchymal Transition and Enhances Chemoresistance in Triple-Negative Breast Cancer Cells via ANXA1. Front. Oncol. 2020, 10, 280. [Google Scholar] [CrossRef]
- Sobral-Leite, M.; Wesseling, J.; Smit, V.T.H.B.M.; Nevanlinna, H.; van Miltenburg, M.H.; Sanders, J.; Hofland, I.; Blows, F.M.; Coulson, P.; Patrycja, G.; et al. Annexin A1 Expression in a Pooled Breast Cancer Series: Association with Tumor Subtypes and Prognosis. BMC Med. 2015, 13, 156. [Google Scholar] [CrossRef] [Green Version]
- Foo, S.L.; Yap, G.; Cui, J.; Lim, L.H.K. Annexin-A1—A Blessing or a Curse in Cancer? Trends Mol. Med. 2019, 25, 315–327. [Google Scholar] [CrossRef]
- Okano, M.; Oshi, M.; Butash, A.L.; Katsuta, E.; Tachibana, K.; Saito, K.; Okayama, H.; Peng, X.; Yan, L.; Kono, K.; et al. Triple-Negative Breast Cancer with High Levels of Annexin A1 Expression Is Associated with Mast Cell Infiltration, Inflammation, and Angiogenesis. Int. J. Mol. Sci. 2019, 20, 4197. [Google Scholar] [CrossRef] [Green Version]
- Bai, F.; Zhang, P.; Fu, Y.; Chen, H.; Zhang, M.; Huang, Q.; Li, D.; Li, B.; Wu, K. Targeting ANXA1 Abrogates Treg-Mediated Immune Suppression in Triple-Negative Breast Cancer. J. Immunother. Cancer 2020, 8, e000169. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.D.; Jovanović, B.; Chen, X.; Estrada, M.V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS ONE 2016, 11, e0157368. [Google Scholar] [CrossRef]
- Harano, K.; Wang, Y.; Lim, B.; Seitz, R.S.; Morris, S.W.; Bailey, D.B.; Hout, D.R.; Skelton, R.L.; Ring, B.Z.; Masuda, H.; et al. Rates of Immune Cell Infiltration in Patients with Triple-Negative Breast Cancer by Molecular Subtype. PLoS ONE 2018, 13, e0204513. [Google Scholar] [CrossRef] [Green Version]
- Bist, P.; Hui, Q.; Shu, S.; Yi, Y.; Anbalagan, D.; Hoon, L.; Sethi, G.; Chuan, B.; Lim, L.H.K. Biochemical and Biophysical Research Communications Annexin-A1 Controls an ERK-RhoA e NF k B Activation Loop in Breast Cancer Cells. Biochem. Biophys. Res. Commun. 2015, 461, 47–53. [Google Scholar] [CrossRef]
- Mehner, C.; Hockla, A.; Miller, E.; Ran, S.; Radisky, D.C.; Radisky, E.S. Tumor Cell-Produced Matrix Metalloproteinase 9 (MMP-9) Drives Malignant Progression and Metastasis of Basal-like Triple Negative Breast Cancer. Oncotarget 2014, 5, 2736–2749. [Google Scholar] [CrossRef] [Green Version]
- Zhou, R.; Xu, L.; Ye, M.; Liao, M.; Du, H.; Chen, H.; Surgery, B.; Medicine, C.; Hospital, C.; Hospital, L. Formononetin Inhibits Migration and Invasion of MDA-MB-231 and 4T1 Breast Cancer Cells by Suppressing MMP-2 and MMP-9 Through PI3K/AKT Signaling Pathways. Endocr. Res. 2014, 46, 753–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozumi, A.; Nishimura, Y.; Nishiuma, T.; Kotani, Y.; Yokoyama, M. Induction of MMP-9 in Normal Human Bronchial Epithelial Cells by TNF-α via NF-ΚB-Mediated Pathway. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2001, 281, L1444–L1452. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.W.; You, K.S.; Park, J.S.; Lee, S.G.; Seong, Y.S. Ribosomal Protein S6: A Potential Therapeutic Target against Cancer? Int. J. Mol. Sci. 2022, 23, 48. [Google Scholar] [CrossRef]
- Pópulo, H.; Lopes, J.M.; Soares, P. The MTOR Signalling Pathway in Human Cancer. Int. J. Mol. Sci. 2012, 13, 1886–1918. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Allis, C.D. SWI/SNF Complex in Cancer: ‘Remodeling’ Mechanisms Uncovered. Nat. Genet. 2017, 49, 178–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belvedere, R.; Bizzarro, V.; Forte, G.; Dal Piaz, F.; Parente, L.; Petrella, A. Annexin A1 Contributes to Pancreatic Cancer Cell Phenotype, Behaviour and Metastatic Potential Independently of Formyl Peptide Receptor Pathway. Sci. Rep. 2016, 6, 29660. [Google Scholar] [CrossRef] [Green Version]
- Cheng, T.Y.; Wu, M.S.; Lin, J.T.; Lin, M.T.; Shun, C.T.; Huang, H.Y.; Hua, K.T.; Kuo, M.L. Annexin A1 Is Associated with Gastric Cancer Survival and Promotes Gastric Cancer Cell Invasiveness through the Formyl Peptide Receptor/Extracellular Signal-Regulated Kinase/Integrin Beta-1-Binding Protein 1 Pathway. Cancer 2012, 118, 5757–5767. [Google Scholar] [CrossRef]
- Han, G.; Lu, K.; Xu, W.; Zhang, S. Annexin A1-Mediated Inhibition of Inflammatory Cytokines May Facilitate the Resolution of Inflammation in Acute Radiation-Induced Lung Injury. Oncol. Lett. 2019, 18, 321–329. [Google Scholar] [CrossRef] [Green Version]
- Solinas, G.; Germano, G.; Mantovani, A.; Allavena, P. Tumor-Associated Macrophages (TAM) as Major Players of the Cancer-Related Inflammation. J. Leukoc. Biol. 2009, 86, 1065–1073. [Google Scholar] [CrossRef] [Green Version]
- Siveen, K.S.; Kuttan, G. Role of Macrophages in Tumour Progression. Immunol. Lett. 2009, 123, 97–102. [Google Scholar] [CrossRef]
- Genin, M.; Clement, F.; Fattaccioli, A.; Raes, M.; Michiels, C. M1 and M2 Macrophages Derived from THP-1 Cells Differentially Modulate the Response of Cancer Cells to Etoposide. BMC Cancer 2015, 15, 577. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Di, G. Role of Tumor Microenvironment in Triple-Negative Breast Cancer and Its Prognostic Significance. Chinese J. Cancer Res. 2017, 29, 237–252. [Google Scholar] [CrossRef]
- Teicher, B.A.; Fricker, S.P. CXCL12 (SDF-1)/CXCR4 Pathway in Cancer. Clin. Cancer Res. 2010, 16, 2927–2931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakaria, M.A.; Rajab, N.F.; Chua, E.W.; Selvarajah, G.T.; Masre, S.F. Roles of Rho-Associated Kinase in Lung Cancer (Review). Int. J. Oncol. 2021, 58, 185–198. [Google Scholar] [CrossRef]
- Shaw, R.J. LKB1 and AMP-Activated Protein Kinase Control of MTOR Signalling and Growth. Acta Physiol. 2009, 196, 65–80. [Google Scholar] [CrossRef]
- Zou, Z.; Tao, T.; Li, H.; Zhu, X. MTOR Signaling Pathway and MTOR Inhibitors in Cancer: Progress and Challenges. Cell Biosci. 2020, 10, 31. [Google Scholar] [CrossRef]
- Yang, L.; Pang, Y.; Moses, H.L. TGF-β and Immune Cells: An Important Regulatory Axis in the Tumor Microenvironment and Progression. Trends Immunol. 2010, 31, 220–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abd El-Hafeez, A.A.; Khalifa, H.O.; Mahdy, E.A.M.; Sharma, V.; Hosoi, T.; Ghosh, P.; Ozawa, K.; Montano, M.M.; Fujimura, T.; Ibrahim, A.R.N.; et al. Anticancer Effect of Nor-Wogonin (5, 7, 8-Trihydroxyflavone) on Human Triple-Negative Breast Cancer Cells via Downregulation of TAK1, NF-ΚB, and STAT3. Pharmacol. Rep. 2019, 71, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, M.R.; Baik, J.E.; Lagana, S.M.; Han, R.P.; Raab, W.J.; Sahoo, D.; Dalerba, P.; Wang, T.C.; Han, Y.W. Fusobacterium Nucleatum Promotes Colorectal Cancer by Inducing Wnt/Β-catenin Modulator Annexin A1. EMBO Rep. 2019, 20, e47638. [Google Scholar] [CrossRef]
- Wei, L.; Li, L.; Liu, L.; Yu, R.; Li, X.; Luo, Z. Knockdown of Annexin-A1 Inhibits Growth, Migration and Invasion of Glioma Cells by Suppressing the PI3K/Akt Signaling Pathway. ASN Neuro 2021, 13, 17590914211001218. [Google Scholar] [CrossRef] [PubMed]
- Dey, N.; Young, B.; Abramovitz, M.; Bouzyk, M.; Barwick, B.; De, P.; Leyland-Jones, B. Differential Activation of Wnt-β-Catenin Pathway in Triple Negative Breast Cancer Increases MMP7 in a PTEN Dependent Manner. PLoS ONE 2013, 8, e77425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De, P.; Carlson, J.H.; Jepperson, T.; Willis, S.; Leyland-Jones, B.; Dey, N. RAC1 GTP-Ase Signals Wnt-Beta-Catenin Pathway Mediated Integrin-Directed Metastasis-Associated Tumor Cell Phenotypes in Triple Negative Breast Cancers. Oncotarget 2017, 8, 3072–3103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onozawa, H.; Saito, M.; Saito, K.; Kanke, Y.; Watanabe, Y.; Hayase, S.; Sakamoto, W.; Ishigame, T.; Momma, T.; Ohki, S.; et al. Annexin A1 Is Involved in Resistance to 5-FU in Colon Cancer Cells. Oncol. Rep. 2017, 37, 235–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.H.; Yong, H.M.; Zhuang, Q.X.; Zhang, X.P.; Hou, P.F.; Chen, Y.S.; Zhu, M.H.; Bai, J. Reduced Expression of Annexin A1 Promotes Gemcitabine and 5-Fluorouracil Drug Resistance of Human Pancreatic Cancer. Investig. New Drugs 2020, 38, 350–359. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study | Source a | Experimental Design | Selective Reporting f | Total | |||
|---|---|---|---|---|---|---|---|
| Culture Conditions b | Replicates c | Controls d | Multiple Cell lines e | ||||
| [24] | 1 | 1 | 0 | 1 | 0 | 1 | 4 |
| [20] | 1 | 1 | 1 | 1 | 1 | 0 | 5 |
| [25] | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| [26] | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| [13] | 1 | 1 | 1 | 1 | 1 | 0 | 5 |
| [27] | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| [28] | 1 | 1 | 1 | 1 | 0 | 1 | 5 |
| [15] | 1 | 1 | 0 | 1 | 1 | 1 | 5 |
| [29] | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| [30] | 1 | 1 | 0 | 1 | 1 | 0 | 4 |
| [31] | 1 | 1 | 0 | 1 | 1 | 1 | 5 |
| [32] | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| [33] | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| Cell Line(s) | Origin | Findings | Study |
|---|---|---|---|
| MDA-MB 231 | Human breast cancer |
| [32] |
| MDA-MB 231 | Human breast cancer |
| [30] |
| 4-T1 | Mouse mammary tumor |
| [28] |
| MDA-MB 231 | Human breast cancer |
| [13] |
| MDA-MB 231 | Human breast cancer |
| [15] |
| MDA-MB 468 MDA-MB 436 | Human breast cancer |
| [20] |
| MDA-MB 231 | Human breast cancer |
| [25] |
| MDA-MB 231 | Human breast cancer |
| [27] |
| Cell Line (s) | Origin | Findings | Study |
|---|---|---|---|
| MDA-MB 231 | Human breast cancer |
| [32] |
| MDA-MB 231 | Human breast cancer |
| [30] |
| Cell Line(s) | Origin | Findings | Study |
|---|---|---|---|
| MDA-MB 231 | Human breast cancer |
| [30] |
| 4-T1 | Mouse mammary tumor |
| [28] |
| MDA-MB 231 | Human breast cancer |
| [13] |
| MDA-MB 157, MDA-MB 436, HS578T, MDA-MB 468, BT549 | Human breast cancer |
| [20] |
| MDA-MB 231 | Human breast cancer |
| [27] |
| MDA-MB 231 | Human breast cancer |
| [25] |
| MDA-MB 231 | Human breast cancer |
| [26] |
| BT-549, MDA-MB 231 | Human breast cancer |
| [33] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearanpan, L.; Nordin, F.J.; Siew, E.L.; Kumolosasi, E.; Mohamad Hanif, E.A.; Masre, S.F.; Chua, E.W.; Cheng, H.S.; Rajab, N.F. A Cell-Based Systematic Review on the Role of Annexin A1 in Triple-Negative Breast Cancers. Int. J. Mol. Sci. 2022, 23, 8256. https://doi.org/10.3390/ijms23158256
Pearanpan L, Nordin FJ, Siew EL, Kumolosasi E, Mohamad Hanif EA, Masre SF, Chua EW, Cheng HS, Rajab NF. A Cell-Based Systematic Review on the Role of Annexin A1 in Triple-Negative Breast Cancers. International Journal of Molecular Sciences. 2022; 23(15):8256. https://doi.org/10.3390/ijms23158256
Chicago/Turabian StylePearanpan, Lishantini, Fariza Juliana Nordin, Ee Ling Siew, Endang Kumolosasi, Ezanee Azlina Mohamad Hanif, Siti Fathiah Masre, Eng Wee Chua, Hong Sheng Cheng, and Nor Fadilah Rajab. 2022. "A Cell-Based Systematic Review on the Role of Annexin A1 in Triple-Negative Breast Cancers" International Journal of Molecular Sciences 23, no. 15: 8256. https://doi.org/10.3390/ijms23158256
APA StylePearanpan, L., Nordin, F. J., Siew, E. L., Kumolosasi, E., Mohamad Hanif, E. A., Masre, S. F., Chua, E. W., Cheng, H. S., & Rajab, N. F. (2022). A Cell-Based Systematic Review on the Role of Annexin A1 in Triple-Negative Breast Cancers. International Journal of Molecular Sciences, 23(15), 8256. https://doi.org/10.3390/ijms23158256