
Usefulness of Vaccine Adverse Event Reporting System for Machine-Learning Based Vaccine Research: A Case Study for COVID-19 Vaccines


 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Associations of the Most Commonly Reported AEs via ARM and SOM
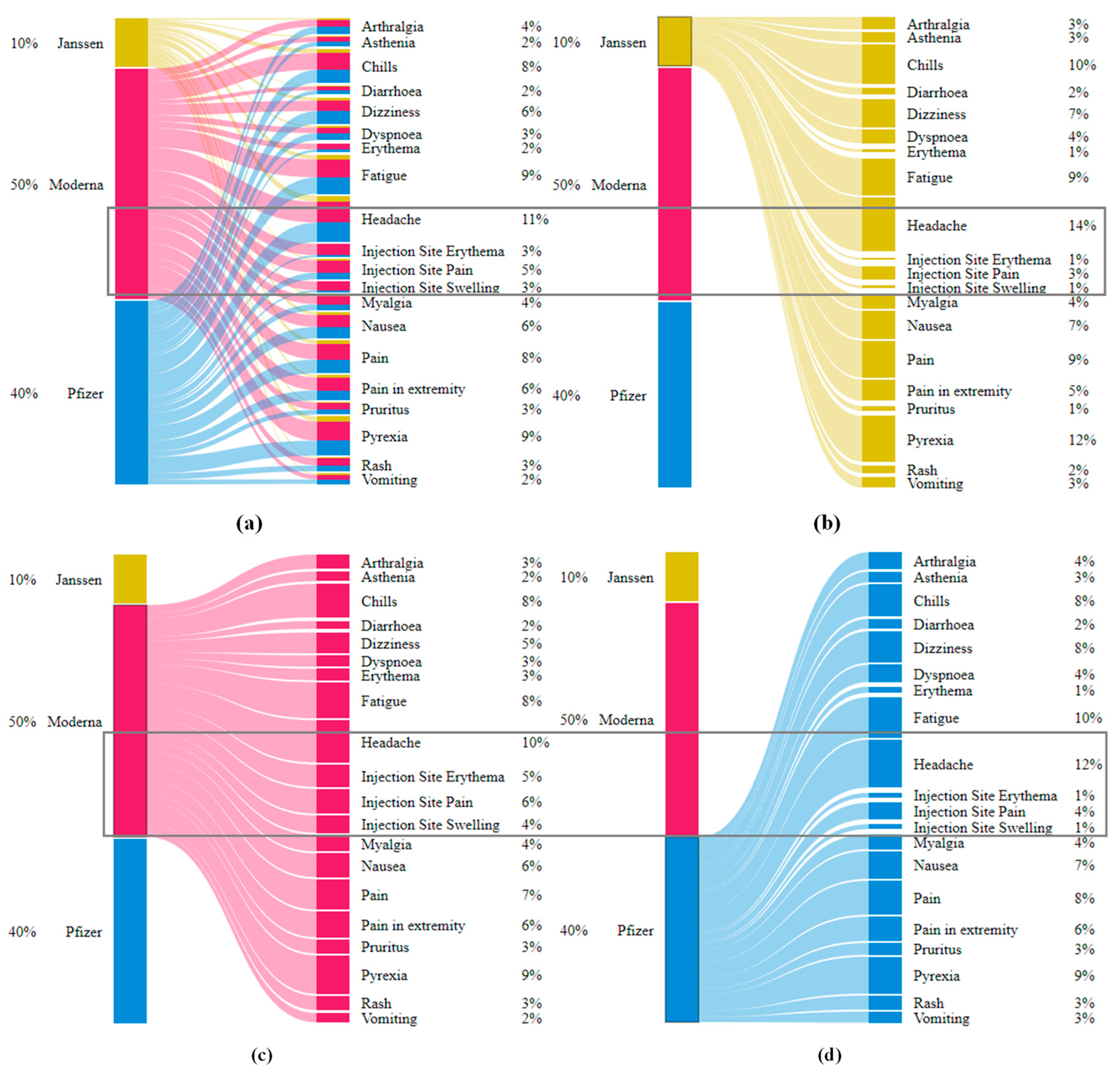
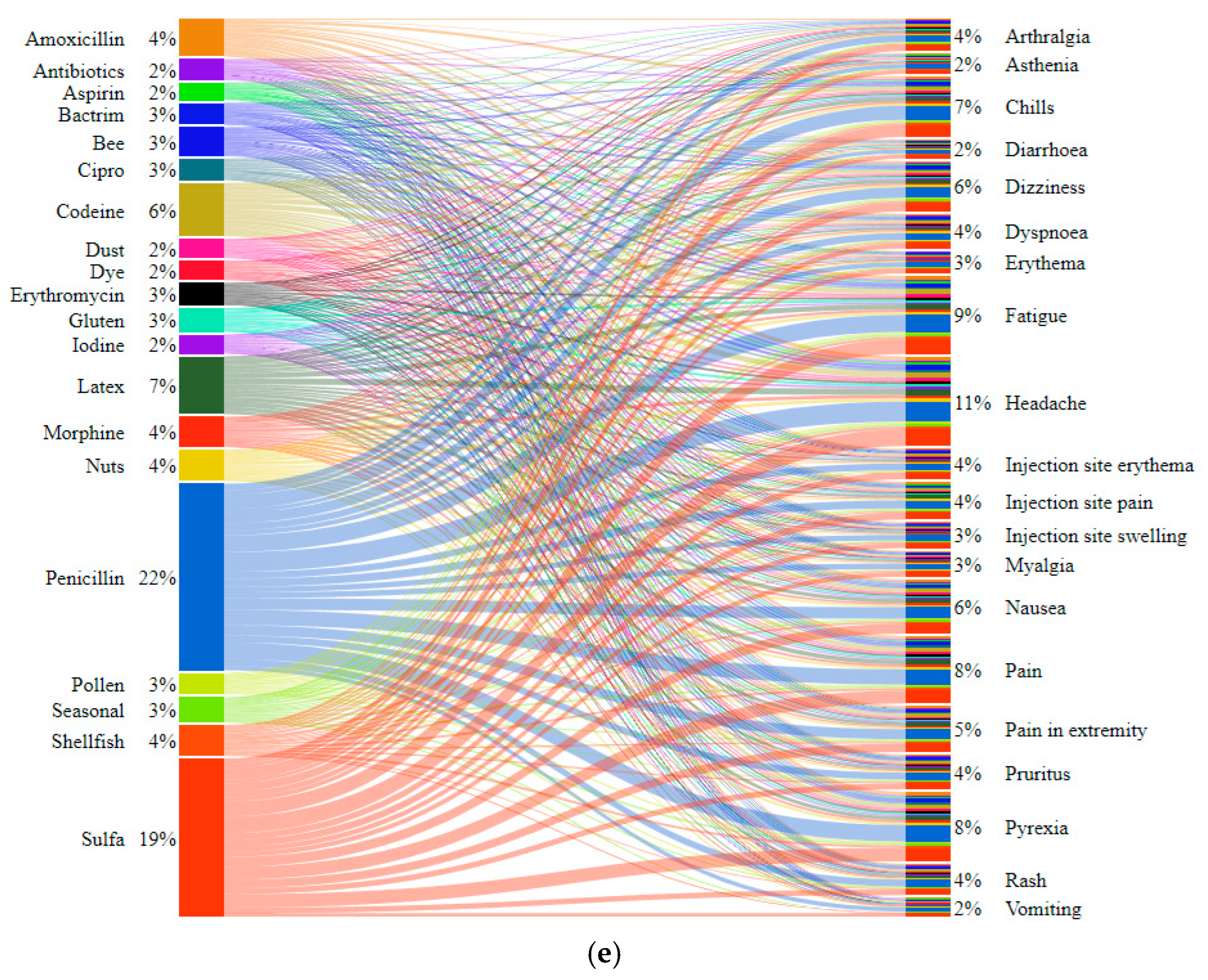
2.2. Interrelations of Vaccine AEs via Bipartite Graphs
3. Discussion
3.1. Flexibility offor Model Features
3.2. Robust Model-Development Pipelines
3.3. ML Model Verification
3.4. Model Stability and Efficiency
4. Materials and Methods
4.1. Compilation, Preprocessing, and Exploration of VAERS Data
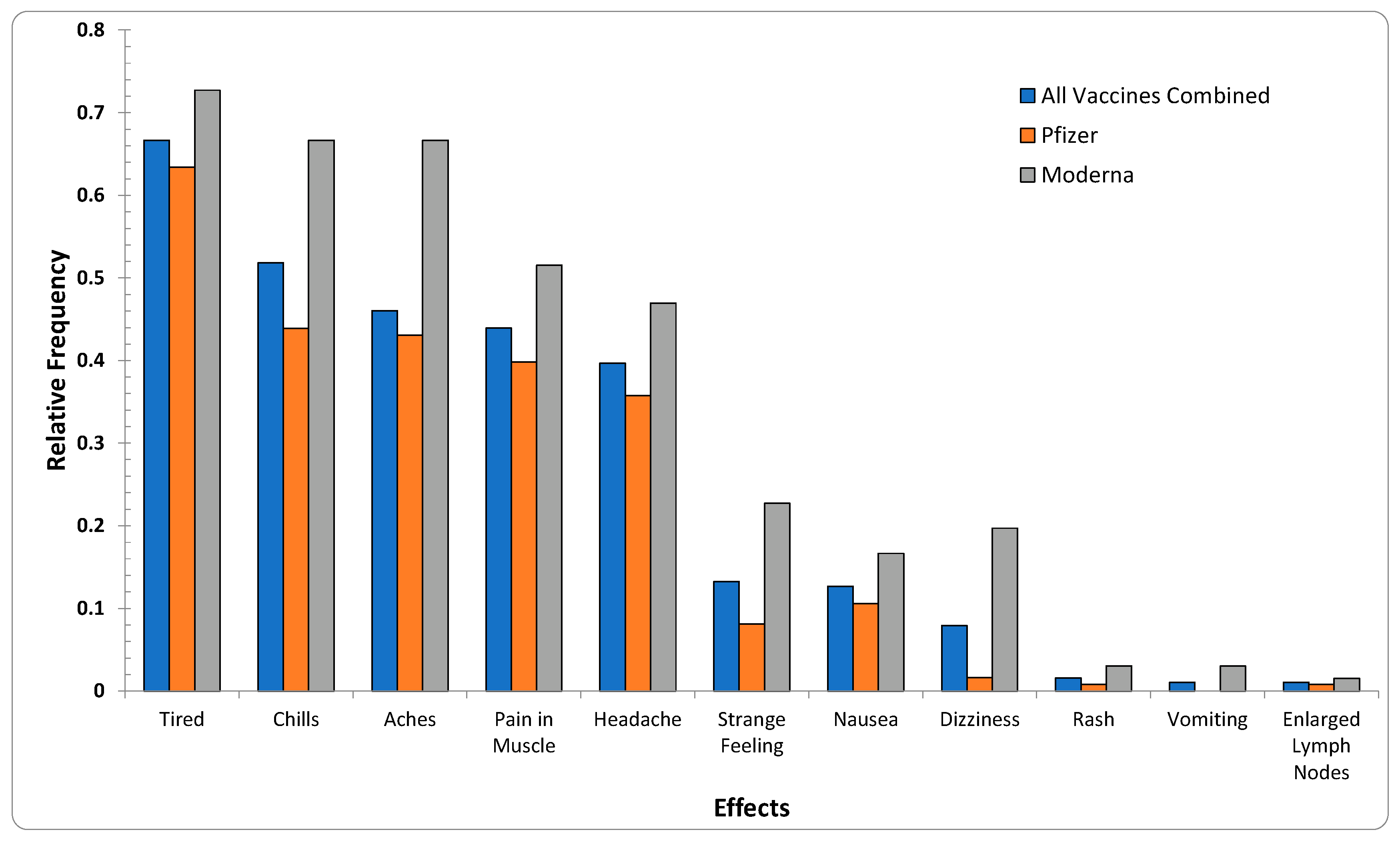
4.2. Exploratory Data Analysis of the COVID-19 Vaccines’ Effects
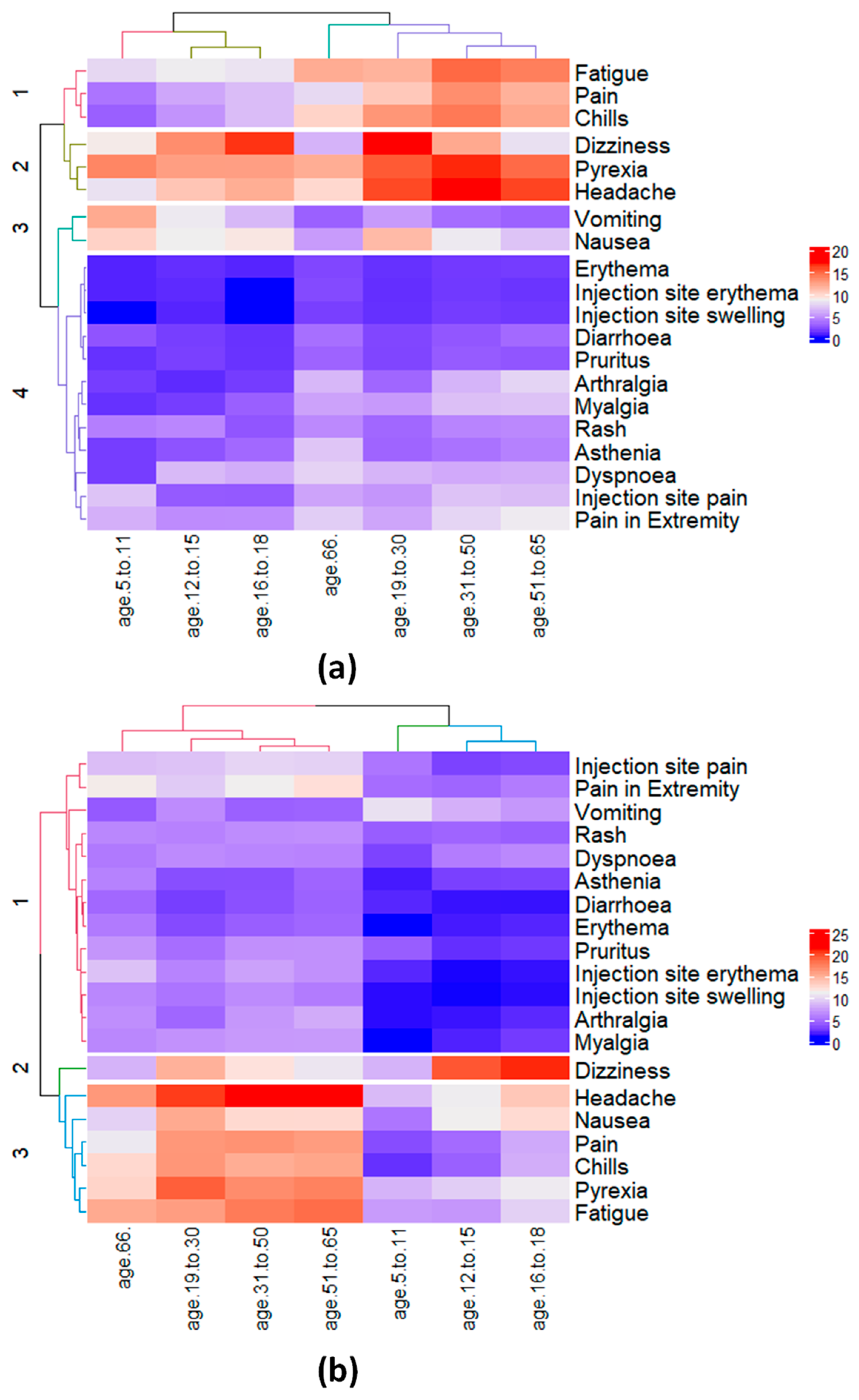
4.3. Correlation Analysis of AEs Based on Age Groups and Allergies
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Health and Human Services (HHS). About VAERS-Background and Public Health Importance 2022. Available online: https://vaers.hhs.gov/about.html (accessed on 23 May 2022).
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, R.; Braun, M.M.; Chen, R.T.; Ellenberg, S.S.; English-Bullard, R.; Haber, P.; Zhou, W. Surveillance for safety after immunization: Vaccine Adverse Event Reporting System (VAERS)—United States, 1991–2001. In MWWR. Surveillance Summaries: Morbidity and Mortality Weekly Report. Surveillance Summaries; CDC: Atlanta, GA, USA, 2003. [Google Scholar]
- Su, J.R. Myopericarditis Following COVID-19 Vaccination: Updates from the Vaccine Adverse Event Reporting System (VAERS) [Internet]. Team. CDCC-19 VTFVS, Editor. Atanta, GA; (ACIP Meeting COVID-19 Vaccines; Volume 202113). Available online: https://stacks.cdc.gov/view/cdc/110920 (accessed on 23 May 2022).
- Myers, T.R.; McNeil, M.M.; Ng, C.S.; Li, R.; Marquez, P.L.; Moro, P.L.; Cano, M.V. Adverse events following quadrivalent meningococcal diphtheria toxoid conjugate vaccine (Menactra®) reported to the Vaccine Adverse Event Reporting System (VAERS), 2005–2016. Vaccine 2020, 38, 6291–6298. [Google Scholar] [CrossRef] [PubMed]
- VAERS. VAERS Data 2021. Available online: https://vaers.hhs.gov/data/datasets.html? (accessed on 23 May 2022).
- Miller, E.R.; McNeil, M.M.; Moro, P.L.; Duffy, J.; Su, J.R. The reporting sensitivity of the Vaccine Adverse Event Reporting System (VAERS) for anaphylaxis and for Guillain-Barré syndrome. Vaccine 2020, 38, 7458–7463. [Google Scholar] [CrossRef] [PubMed]
- Botsis, T.; Nguyen, M.D.; Woo, E.J.; Markatou, M.; Ball, R. Text mining for the Vaccine Adverse Event Reporting System: Medical text classification using informative feature selection. J. Am. Med. Inform. Assoc. 2011, 18, 631–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, J.; Xiang, Y.; Sankaranarayanapillai, M.; Zhang, M.; Wang, J.; Si, Y.; Tao, C. Extracting postmarketing adverse events from safety reports in the vaccine adverse event reporting system (VAERS) using deep learning. J. Am. Med. Inform. Assoc. 2021, 28, 1393–1400. [Google Scholar] [CrossRef]
- Lian, A.T.; Du, J.; Tang, L. Using a Machine Learning Approach to Monitor COVID-19 Vaccine Adverse Events (VAE) from Twitter Data. Vaccines 2022, 10, 103. [Google Scholar] [CrossRef]
- Sujatha, R.; Venkata Siva Krishna, B.; Chatterjee, J.M.; Naidu, P.R.; Jhanjhi, N.Z.; Charita, C.; Baz, M. Prediction of Suitable Candidates for COVID-19 Vaccination. Intell. Autom. Soft Comput. 2022, 32, 525–541. [Google Scholar] [CrossRef]
- Xie, J.; Zhao, L.; Zhou, S.; He, Y. Statistical and Ontological Analysis of Adverse Events Associated with Monovalent and Combination Vaccines against Hepatitis A and B Diseases. Sci. Rep. 2016, 6, 34318. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.R.; Lewis, P.; Shimabukuro, T.T.; Su, J.; Moro, P.; Woo, E.J.; Cano, M. Post-licensure safety surveillance of zoster vaccine live (Zostavax®) in the United States, Vaccine Adverse Event Reporting System (VAERS), 2006–2015. Hum. Vaccin Immunother. 2018, 14, 1963–1969. [Google Scholar] [CrossRef] [Green Version]
- Luo, C.; Jiang, Y.; Du, J.; Tong, J.; Huang, J.; Lo Re, V., III; Chen, Y. Prediction of post-vaccination Guillain-Barré syndrome using data from a passive surveillance system. Pharm. Drug Saf. 2021, 30, 602–609. [Google Scholar] [CrossRef]
- Miller, N.Z. Vaccines and sudden infant death: An analysis of the VAERS database 1990–2019 and review of the medical literature. Toxicol. Rep. 2021, 8, 1324–1335. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.A.; Kaelber, D.C.; Bar-Shain, D.S.; Moro, P.L.; Zambarano, B.; Mazza, M.; Klompas, M. Advanced Clinical Decision Support for Vaccine Adverse Event Detection and Reporting. Clin. Infect. Dis. 2015, 61, 864–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukumaran, L.; McNeil, M.M.; Moro, P.L.; Lewis, P.W.; Winiecki, S.K.; Shimabukuro, T.T. Adverse events following measles, mumps, and rubella vaccine in adults reported to the vaccine adverse event reporting system (VAERS), 2003–2013. Clin. Infect. Dis. 2015, 60, e58–e65. [Google Scholar] [CrossRef] [Green Version]
- Moro, P.L.; Woo, E.J.; Paul, W.; Lewis, P.; Petersen, B.W.; Cano, M. Post-Marketing Surveillance of Human Rabies Diploid Cell Vaccine (Imovax) in the Vaccine Adverse Event Reporting System (VAERS) in the United States, 1990–2015. PLoS Negl. Trop. Dis. 2016, 10, e0004846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loughlin, A.M.; Marchant, C.D.; Adams, W.; Barnett, E.; Baxter, R.; Black, S.; Jakob, K. Causality assessment of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2012, 30, 7253–7259. [Google Scholar] [CrossRef] [PubMed]
- Myers, T.R.; McNeil, M.M.; Ng, C.S.; Li, R.; Lewis, P.W.; Cano, M.V. Adverse events following quadrivalent meningococcal CRM-conjugate vaccine (Menveo®) reported to the Vaccine Adverse Event Reporting system (VAERS), 2010–2015. Vaccine 2017, 35, 1758–1763. [Google Scholar] [CrossRef] [Green Version]
- Gatti, M.; Raschi, E.; Moretti, U.; Ardizzoni, A.; Poluzzi, E.; Diemberger, I. Influenza vaccination and myo-pericarditis in patients receiving immune checkpoint inhibitors: Investigating the likelihood of interaction through the vaccine adverse event reporting system and vigibase. Vaccines 2021, 9, 19. [Google Scholar] [CrossRef]
- Kreimeyer, K.; Menschik, D.; Winiecki, S.; Paul, W.; Barash, F.; Woo, E.J.; Botsis, T. Using Probabilistic Record Linkage of Structured and Unstructured Data to Identify Duplicate Cases in Spontaneous Adverse Event Reporting Systems. Drug Saf. 2017, 40, 571–582. [Google Scholar] [CrossRef]
- Hervé, C.; Laupèze, B.; Del Giudice, G.; Didierlaurent, A.M.; Tavares Da Silva, F. The how’s and what’s of vaccine reactogenicity. npj Vaccines 2019, 4, 39. [Google Scholar] [CrossRef] [Green Version]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone Jr, C.A.; Robinson, L.B.; Long, A.A.; Blumenthal, K.G. mRNA Vaccines to Prevent COVID-19 Disease and Reported Allergic Reactions: Current Evidence and Suggested Approach. J. Allergy Clin. Immunol Pract. 2021, 9, 1423–1437. Available online: https://pubmed.ncbi.nlm.nih.gov/33388478 (accessed on 18 November 2021). [CrossRef]
- Croall, I.D.; Trott, N.; Rej, A.; Aziz, I.; O’Brien, D.J.; George, H.A.; Sanders, D.S. A Population Survey of Dietary Attitudes towards Gluten. Nutrients 2019, 11, 1276. Available online: http://europepmc.org/abstract/MED/31195638 (accessed on 18 November 2021). [CrossRef] [PubMed] [Green Version]
- Jordá, F.C.; Vivancos, J.L. Fatigue as a Determinant of Health in Patients With Celiac Disease. J. Clin. Gastroenterol. 2010, 44, 423–427. Available online: https://journals.lww.com/jcge/Fulltext/2010/07000/Fatigue_as_a_Determinant_of_Health_in_Patients.13.aspx (accessed on 12 April 2022). [CrossRef] [PubMed]
- Freeman, H.J. Iron deficiency anemia in celiac disease. World J. Gastroenterol. 2015, 21, 9233–9238. [Google Scholar] [CrossRef]
- Guzzi, P.H.; Milano, M.; Cannataro, M. Mining Association Rules from Gene Ontology and Protein Networks: Promises and Challenges. Procedia Comput. Sci. 2014, 29, 1970–1980. Available online: http://www.sciencedirect.com/science/article/pii/S1877050914003585 (accessed on 23 May 2022). [CrossRef] [Green Version]
- Schuchat, A.; Anderson, L.J.; Rodewald, L.E.; Cox, N.J.; Hajjeh, R.; Pallansch, M.A.; Wharton, M.; National Center for Immunization and Respiratory Diseases (NCIRD), Division of Viral Diseases. V-Safe After Health Checker. 2022; Volume 24, p. 1178. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/vsafe.html (accessed on 23 May 2022).
- Oellrich, A.; Jacobsen, J.; Papatheodorou, I.; Smedley, D. Using association rule mining to determine promising secondary phenotyping hypotheses. Bioinformatics 2014, 30, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naulaerts, S.; Meysman, P.; Bittremieux, W.; Vu, T.N.; Vanden Berghe, W.; Goethals, B.; Laukens, K. A primer to frequent itemset mining for bioinformatics. Brief. Bioinform. 2015, 16, 216–231. Available online: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4364064/ (accessed on 11 March 2022). [CrossRef] [PubMed] [Green Version]
- Park, S.H.; Reyes, J.A.; Gilbert, D.R.; Kim, J.W.; Kim, S. Prediction of protein-protein interaction types using association rule based classification. BMC Bioinform. 2009, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Nafar, Z.; Golshani, A. Data Mining Methods for Protein-Protein Interactions. In Proceedings of the 2006 Canadian Conference on Electrical and Computer Engineering, Ottawa, ON, Canada, 7–10 May 2006; pp. 991–994. [Google Scholar]
- Liu, R.; France, B.; George, S.; Rallo, R.; Zhang, H.; Xia, T.; Cohen, Y. Association rule mining of cellular responses induced by metal and metal oxide nanoparticles. Analytical 2014, 139, 943–953. [Google Scholar] [CrossRef]
- Mallik, S.; Mukhopadhyay, A.; Maulik, U.; Bandyopadhyay, S. Integrated analysis of gene expression and genome-wide DNA methylation for tumor prediction: An association rule mining-based approach. In Proceedings of the 2013 IEEE Symposium on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), Singapore, 16–19 April 2013; pp. 120–127. [Google Scholar]
- Martinez, R.; Pasquier, N.; Pasquier, C. GenMiner: Mining non-redundant association rules from integrated gene expression data and annotations. Bioinformatics 2008, 24, 2643–2644. [Google Scholar] [CrossRef] [Green Version]
- Alves, R.; Rodriguez-Baena, D.S.; Aguilar-Ruiz, J.S. Gene association analysis: A survey of frequent pattern mining from gene expression data. Brief. Bioinform. 2010, 1, 210–224. [Google Scholar] [CrossRef] [Green Version]
- Chon, T.S. Self-Organizing Maps applied to ecological sciences. Ecol. Inform. 2011, 6, 50–61. [Google Scholar] [CrossRef]
- Tamayo, P.; Slonim, D.; Mesirov, J.; Zhu, Q.; Kitareewan, S.; Dmitrovsky, E.; Golub, T.R. Interpreting patterns of gene expression with self-organizing maps: Methods and application to hematopoietic differentiation. Proc. Natl. Acad Sci. USA. 1999, 96, 2907–2912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Törönen, P.; Kolehmainen, M.; Wong, G.; Castrén, E. Analysis of gene expression data using self-organizing maps. FEBS Lett. 1999, 451, 142–146. Available online: http://www.ncbi.nlm.nih.gov/pubmed/18003033 (accessed on 23 May 2022). [CrossRef]
- Bullinaria, J.A. Self Organizing Maps: Fundamentals 2004. Available online: http://www.cs.bham.ac.uk/~jxb/NN/l16.pdf (accessed on 3 June 2017).
- Dettmer, J.; Benavente, R.; Cummins, P.R.; Sambridge, M. Trans-dimensional finite-fault inversion. Geophys. J. Int. 2014, 199, 735–751. [Google Scholar] [CrossRef] [Green Version]
- Giralt, F.; Espinosa, G.; Arenas, A.; Ferre-Gine, J.; Amat, L.; Girones, X.; Cohen, Y. Estimation of infinite dilution activity coefficients of organic compounds in water with neural classifiers. AIChE J. 2004, 50, 1315–1343. [Google Scholar] [CrossRef]
- Liu, R.; Lin, S.; Rallo, R.; Zhao, Y.; Damoiseaux, R.; Xia, T.; Cohen, Y. Automated Phenotype Recognition for Zebrafish Embryo Based In Vivo High Throughput Toxicity Screening of Engineered Nanomaterials. PLoS ONE 2012, 7, e35014. [Google Scholar] [CrossRef] [Green Version]
- Rallo, R.; France, B.; Liu, R.; Nair, S.; George, S.; Damoiseaux, R.; Cohen, Y. Self-Organizing Map Analysis of Toxicity-Related Cell Signaling Pathways for Metal and Metal Oxide Nanoparticles. Environ. Sci. Technol. 2011, 45, 1695–1702. Available online: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4418424/ (accessed on 23 May 2022). [CrossRef] [Green Version]
- Rhodes, B.C.; Mahaffey, J.A.; Cannady, J.D. Multiple self-organizing maps for intrusion detection. In Proceedings of the 23rd National Information Systems Security Conference, Baltimore, MD, USA, 16–19 October 2000. [Google Scholar]
- Greenacre, M.; Primicerio, R. Multivariate Analysis of Ecological Data; Fundación BBVA: Bilbao, Spain, 2013. [Google Scholar]
- Hahsler, M.; Grün, B.; Hornik, K. Arules—A Computational Environment for Mining Association Rules and Frequent Item Sets. J. Stat. Softw. 2005, 14, 1–25. [Google Scholar] [CrossRef]
- Wehrens, R.; Kruisselbrink, J. Flexible Self-Organizing Maps in kohonen 3.0. J. Stat. Softw. 2018, 87, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Kokoska, S.; Zwillinger, D. CRC Standard Probability and Statistics Tables and Formulae, 1st ed.; CRC Press: Boca Raton, FL, USA, 2000. [Google Scholar]
- Murtagh, F.; Legendre, P. Ward’s Hierarchical Agglomerative Clustering Method: Which Algorithms Implement Ward’s Criterion? J. Classif. 2014, 31, 274–295. [Google Scholar] [CrossRef] [Green Version]
- Pasha. biPartite Graphs—bl.ocks.org. 2022. Available online: http://bl.ocks.org/NPashaP/3ba0031d3d555afca4713e5264455025 (accessed on 23 May 2022).
- Dormann, C.F.; Strauss, R. A method for detecting modules in quantitative bipartite networks. Methods Ecol. Evol. 2014, 5, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Dormann, C.F.; Fründ, J.; Blüthgen, N.; Gruber, B. Indices, Graphs and Null Models: Analyzing Bipartite Ecological Networks. Open Ecol. J. 2009, 2, 7–24. [Google Scholar] [CrossRef]
- Dormann, C.F.; Gruber, B.; Fründ, J. Introducing the bipartite package: Analysing ecological networks. Interaction 2008, 1, 2413793. [Google Scholar]
- Zhang, C.; Zhang, S. Association Rule Mining: Models and Algorithms; Springer: Berlin/Heidelberg, Germany, 2002. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Effects | Vaccine Manufacturer | |||||
|---|---|---|---|---|---|---|
| VAERS | Survey Data | Pfizer-BioNTech | Pfizer-BioNTech Survey Data Points | Moderna | Moderna Survey Data Points | Janssen |
| Headache | Headache | 48,253 (17.05%) | 44 (35.77%) | 51,816 (17.27%) | 31 (46.97%) | 15,234 (25.78%) |
| Pyrexia | Aches | 37,418 (13.22%) | 53 (43.09%) | 47,476 (15,82%) | 44 (66.67%) | 12,811 (21.68%) |
| Fatigue | Tired | 41,022 (14.49%) | 78 (63.41%) | 44,642 (14,88%) | 48 (72.73%) | 10,409 (17.62%) |
| Chills | Chills | 31,965 (11.29%) | 54 (43.90%) | 41,313 (13.77%) | 44 (66.67%) | 11,001 (18.62%) |
| Pain | Pain in muscle | 34,395 (12.15%) | 49 (39.84%) | 37,716 (12.57%) | 34 (51.52%) | 10,424 (17.64%) |
| Dizziness | Dizziness | 32,001 (11.31%) | 2 (1.63%) | 25,924 (8.64%) | 13 (19.70%) | 8075 (13.67%) |
| Nausea | Nausea | 28,179 (9.96%) | 13 (10.57%) | 29,220 (9.74%) | 11 (16.67%) | 7815 (13.23%) |
| Pain in Extremity | NA | 24,708 (8.73%) | NA | 31,813 (10.60%) | NA | 6019 (6.11%) |
| Myalgia | NA | 15,027 (5.31%) | NA | 20,728 (6.91%) | NA | 4059 (6.87%) |
| Arthralgia | NA | 17,469 (6.17%) | NA | 17,713 (5.90%) | NA | 3504 (5.93%) |
| Injection site pain | NA | 16,621 (5.87%) | NA | 30,632 (10.21%) | NA | 3610 (6.11%) |
| Dyspnoea | NA | 17,612 (6.22) | NA | 14,207 (4.74%) | NA | 3895 (6.59%) |
| Rash | Itchy Skin/Rash | 14,178 (5.01%) | 1 (0.81%) | 17,739 (5.91%) | 2 (3.03%) | 2194 (3.71%) |
| Pruritus | NA | 12,013 (4.24%) | NA | 17,697 (5.90%) | NA | 1451 (2.46%) |
| Injection site erythema | NA | 4685 (1.66%) | NA | 27,730 (9.24%) | NA | 600 (1.02%) |
| Asthenia | Strange Feeling | 11,067 (3.91%) | 10 (8.13%) | 12,092 (4.03%) | 15 (22.73%) | 2869 (4.86%) |
| Vomiting | Vomiting | 11,205 (3.96%) | NA | 11,523 (3.84%) | 2 (3.03%) | 3009 (5.09%) |
| Injection-site swelling | Enlarged lymph nodes | 4815 (1.70%) | NA | 21,406 (7.14%) | 1 (1.52%) | 740 (1.25%) |
| Diarrhoea | NA | 9819 (3.47%) | NA | 9682 (3.23%) | NA | 2018 (3.42%) |
| Erythema | NA | 6242 (2.21%) | NA | 14,227 (4.74%) | NA | 838 (1.42%) |
| Age Group (Male Participants) | Age Group (Female Participants) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5–11 | 12–15 | 16–18 | 19–30 | 31–50 | 51–65 | 66+ | 5–11 | 12–15 | 16–18 | 19–30 | 31–50 | 51–65 | 66+ | 25 | |||
| Pyrexia | Vomiting | ||||||||||||||||
| Vomiting | Headache | ||||||||||||||||
| Nausea | Dizziness | ||||||||||||||||
| Dizziness | Pyrexia | ||||||||||||||||
| Headache | Fatigue | ||||||||||||||||
| Fatigue | Injection site pain | ||||||||||||||||
| Injection site pain | Nausea | ||||||||||||||||
| Pain in Extremity | Pain in Extremity | ||||||||||||||||
| Rash | Rash | ||||||||||||||||
| Pain | Pruritus | ||||||||||||||||
| Chills | Pain | ||||||||||||||||
| Diarrhoea | Dyspnoea | ||||||||||||||||
| Arthralgia | Chills | ||||||||||||||||
| Dyspnoea | Injection site erythema | ||||||||||||||||
| Asthenia | Diarrhoea | ||||||||||||||||
| Pruritus | Asthenia | ||||||||||||||||
| Myalgia | Arthralgia | ||||||||||||||||
| Injection site erythema | Injection site swelling | ||||||||||||||||
| Erythema | Myalgia | ||||||||||||||||
| Injection site swelling | Erythema | ||||||||||||||||
| 0 | |||||||||||||||||
| Rule | Antecedent | Consequent | Support | Confidence | Lift | Count |
|---|---|---|---|---|---|---|
| R-1 | Flushing | Hyperhidrosis | 0.016 | 0.80 | 15.18 | 149 |
| R-2 | Flushing | Dizziness | 0.013 | 0.69 | 4.34 | 128 |
| R-3 | Electrocardiogram ST segment elevation | Chest pain | 0.012 | 0.92 | 10.18 | 114 |
| R-4 | Unresponsive to stimuli | Syncope | 0.023 | 0.72 | 6.35 | 223 |
| R-5 | Chest X-ray normal | Chest pain | 0.011 | 0.79 | 8.70 | 103 |
| R-6 | Echocardiogram normal | Troponin increased | 0.011 | 0.55 | 16.59 | 108 |
| R-7 | Echocardiogram normal | Chest pain | 0.018 | 0.87 | 9.62 | 172 |
| R-8 | Myocarditis | Chest pain | 0.021 | 0.74 | 8.22 | 205 |
| R-9 | Electrocardiogram normal | Chest pain | 0.017 | 0.68 | 7.52 | 163 |
| R-10 | Hyperhidrosis | Dizziness | 0.028 | 0.52 | 3.31 | 266 |
| R-11 | C-reactive protein increased | Chest pain | 0.012 | 0.67 | 7.46 | 118 |
| R-12 | Chills | Pyrexia | 0.027 | 0.62 | 5.76 | 263 |
| R-13 | Troponin increased | Chest pain | 0.028 | 0.85 | 9.46 | 270 |
| R-14 | Headache, Pain | Pyrexia | 0.011 | 0.54 | 4.98 | 101 |
| Non-redundant association rules for post-COVID-19 vaccine AEs reported in VAERS reports for Pfizer-BioNTech vaccine. Rules 4–16 were non-redundant many-to-one rules identified for Pfizer-BioNTech. The highlighted regions in gray represent the subset of rules with relatively high counts in the dataset (>6000). The rules below include {pyrexia, fatigue, headache, nausea, vomiting, chills, pain, myalgia}, which were also among the 20 most commonly reported AEs for VAERS reports for Pfizer-BioNTech when explored based on their individual frequencies. | ||||||
| Rule | Antecedent | Consequent | Support | Confidence | Lift | Count |
| R-1 | Body temperature | Pyrexia | 0.016 | 0.86 | 6.53 | 4572 |
| R-2 | Vomiting | Nausea | 0.022 | 0.54 | 5.46 | 6095 |
| R-3 | Chills | Pyrexia | 0.063 | 0.56 | 4.24 | 17,925 |
| R-4 | Chills, Myalgia | Fatigue | 0.011 | 0.53 | 3.65 | 3085 |
| R-5 | Chills, Myalgia | Headache | 0.013 | 0.62 | 3.61 | 3588 |
| R-6 | Myalgia, Pyrexia | Headache | 0.013 | 0.58 | 3.40 | 3589 |
| R-7 | Nausea, Pain | Chills | 0.012 | 0.50 | 4.46 | 3352 |
| R-8 | Chills, Nausea | Headache | 0.018 | 0.60 | 3.52 | 5110 |
| R-9 | Nausea, Pain | Pyrexia | 0.012 | 0.51 | 3.83 | 3371 |
| R-10 | Nausea, Pain | Headache | 0.014 | 0.60 | 3.49 | 3967 |
| R-11 | Nausea, Pyrexia | Headache | 0.017 | 0.59 | 3.45 | 4838 |
| R-12 | Fatigue, Nausea | Headache | 0.019 | 0.57 | 3.36 | 5334 |
| R-13 | Chills, Pain | Headache | 0.024 | 0.54 | 3.17 | 6879 |
| R-14 | Chills, Fatigue | Headache | 0.025 | 0.56 | 3.26 | 7058 |
| R-15 | Fatigue, Pain | Headache | 0.022 | 0.52 | 3.05 | 6130 |
| R-16 | Fatigue, Pyrexia | Headache | 0.025 | 0.52 | 3.05 | 7008 |
| Non-redundant association rules for post-COVID-19 vaccine AEs for Moderna vaccine. Rules 7–25 were many-to-one rules. The highlighted regions represent rules with relatively high count (>10,000). The rules below include {pyrexia, headache, nausea, vomiting, fatigue, chills, pain, injection site pain/swelling/warmth/pruritus/erythema, myalgia}, which were also among the 20 most commonly reported AEs for VAERS reports for Moderna when explored based on their individual frequencies. | ||||||
| R-1 | Injection site induration | Injection site erythema | 0.01 | 0.66 | 7.19 | 3716 |
| R-2 | Injection site warmth | Injection site erythema | 0.03 | 0.70 | 7.55 | 10,203 |
| R-3 | Vomiting | Nausea | 0.02 | 0.56 | 5.72 | 6423 |
| R-4 | Injection site pruritus | Injection site erythema | 0.04 | 0.67 | 7.25 | 13,393 |
| R-5 | Injection site swelling | Injection site erythema | 0.05 | 0.63 | 6.87 | 13,591 |
| R-6 | Chills | Pyrexia | 0.08 | 0.57 | 3.63 | 23,724 |
| R-7 | Injection site pruritus, Injection site warmth | Injection site swelling | 0.01 | 0.51 | 7.09 | 3430 |
| R-8 | Injection site pain, Injection site pruritus | Injection site swelling | 0.01 | 0.52 | 7.24 | 3177 |
| R-9 | Arthralgia, Chills | Headache | 0.01 | 0.60 | 3.45 | 3215 |
| R-10 | Arthralgia, Fatigue | Headache | 0.01 | 0.55 | 3.21 | 3372 |
| R-11 | Arthralgia, Pyrexia | Headache | 0.01 | 0.57 | 3.27 | 3262 |
| R-12 | Chills, Myalgia | Headache | 0.02 | 0.57 | 3.28 | 4685 |
| R-13 | Fatigue, Myalgia | Headache | 0.02 | 0.55 | 3.20 | 4555 |
| R-14 | Myalgia, Pyrexia | Headache | 0.02 | 0.53 | 3.07 | 4696 |
| R-15 | Chills, Injection site pain | Headache | 0.01 | 0.54 | 3.14 | 3263 |
| R-16 | Chills, Pain in extremity | Headache | 0.01 | 0.51 | 2.96 | 3515 |
| R-17 | Nausea, Pain | Chills | 0.01 | 0.55 | 3.99 | 4193 |
| R-18 | Nausea, Pain | Pyrexia | 0.01 | 0.55 | 3.47 | 4187 |
| R-19 | Nausea, Pain | Headache | 0.02 | 0.60 | 3.50 | 4606 |
| R-20 | Chills, Nausea | Headache | 0.02 | 0.60 | 3.48 | 6599 |
| R-21 | Fatigue, Nausea | Headache | 0.02 | 0.58 | 3.38 | 6077 |
| R-22 | Nausea, Pyrexia | Headache | 0.02 | 0.58 | 3.36 | 6198 |
| R-23 | Fatigue, Pain | Headache | 0.02 | 0.52 | 3.04 | 6744 |
| R-24 | Chills, Fatigue | Headache | 0.03 | 0.55 | 3.17 | 8765 |
| R-25 | Fatigue, Pyrexia | Headache | 0.03 | 0.51 | 2.95 | 8442 |
| Non-redundant association rules for post-COVID-19 vaccine AEs for Janssen vaccine. Rules 11–14 were many-to-one rules. The highlighted regions represent rules with relatively high count (>4000). The rules below include {pyrexia, fatigue, headache, pain, nausea, chills, vomiting, myalgia}, which were also among the 20 most commonly reported AEs for VAERS reports for Janssen when explored based on their individual frequencies. | ||||||
| R-1 | Body temperature | Pyrexia | 0.02 | 0.85 | 3.94 | 1223 |
| R-2 | Decreased appetite | Fatigue | 0.01 | 0.53 | 2.99 | 609 |
| R-3 | Vomiting | Nausea | 0.03 | 0.54 | 4.12 | 1638 |
| R-4 | Myalgia | Headache | 0.04 | 0.56 | 2.17 | 2268 |
| R-5 | Nausea | Headache | 0.07 | 0.52 | 2.01 | 4051 |
| R-6 | Pain | Pyrexia | 0.09 | 0.50 | 2.32 | 5237 |
| R-7 | Pain | Headache | 0.09 | 0.50 | 1.96 | 5261 |
| R-8 | Chills | Headache | 0.10 | 0.55 | 2.14 | 6058 |
| R-9 | Fatigue | Headache | 0.09 | 0.51 | 1.97 | 5275 |
| R-10 | Pyrexia | Headache | 0.11 | 0.51 | 1.99 | 6574 |
| R-11 | Myalgia, Nausea | Pyrexia | 0.01 | 0.57 | 2.64 | 614 |
| R-12 | Fatigue, Myalgia | Pyrexia | 0.02 | 0.52 | 2.42 | 942 |
| R-13 | Nausea, Pain | Chills | 0.02 | 0.55 | 2.98 | 1318 |
| R-14 | Fatigue, Pain | Chills | 0.03 | 0.52 | 2.77 | 1869 |
| Vaccine | ||||||
|---|---|---|---|---|---|---|
| Pfizer-BioNTech | Moderna | Janssen | ||||
| Age Group (Years) | Male | Female | Male | Female | Male | Female |
| 5–11 | 233 (0.30%) | 251 (0.14%) | 13 (0.02%) | 13 (0.01%) | 3 (0.02%) | 3 (0.01%) |
| 12–15 | 4133 (5.36%) | 4525 (2.55%) | 96 (0.13%) | 106 (0.05%) | 43 (0.23%) | 38 (0.13%) |
| 16–18 | 3498 (4.54%) | 4396 (2.48%) | 2645 (3.59%) | 3587 (1.83%) | 761 (4.13%) | 753 (2.52%) |
| 19–30 | 10,556 (13.69%) | 24,146 (13.62%) | 8533 (11.58%) | 21,883 (11.19%) | 4054 (22.00%) | 5087 (17.03%) |
| 31–50 | 22,658 (29.39%) | 66,760 (37.65%) | 19,198 (25.06%) | 64,711 (33.08%) | 6561 (35.61%) | 11,901 (39.83%) |
| 51–65 | 18,109 (23.49%) | 45,575 (25.71%) | 18,917 (25.68%) | 52,060 (26.62%) | 4960 (26.92%) | 8754 (29.30%) |
| 66+ | 17,898 (23.22%) | 31,645 (17.85%) | 24,260 (32.93%) | 53,212 (27.21%) | 2045 (11.10%) | 3342 (11.19%) |
| Total | 77,085 | 177,298 | 73,662 | 195,572 | 18,427 | 29,878 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flora, J.; Khan, W.; Jin, J.; Jin, D.; Hussain, A.; Dajani, K.; Khan, B. Usefulness of Vaccine Adverse Event Reporting System for Machine-Learning Based Vaccine Research: A Case Study for COVID-19 Vaccines. Int. J. Mol. Sci. 2022, 23, 8235. https://doi.org/10.3390/ijms23158235
Flora J, Khan W, Jin J, Jin D, Hussain A, Dajani K, Khan B. Usefulness of Vaccine Adverse Event Reporting System for Machine-Learning Based Vaccine Research: A Case Study for COVID-19 Vaccines. International Journal of Molecular Sciences. 2022; 23(15):8235. https://doi.org/10.3390/ijms23158235
Chicago/Turabian StyleFlora, James, Wasiq Khan, Jennifer Jin, Daniel Jin, Abir Hussain, Khalil Dajani, and Bilal Khan. 2022. "Usefulness of Vaccine Adverse Event Reporting System for Machine-Learning Based Vaccine Research: A Case Study for COVID-19 Vaccines" International Journal of Molecular Sciences 23, no. 15: 8235. https://doi.org/10.3390/ijms23158235
APA StyleFlora, J., Khan, W., Jin, J., Jin, D., Hussain, A., Dajani, K., & Khan, B. (2022). Usefulness of Vaccine Adverse Event Reporting System for Machine-Learning Based Vaccine Research: A Case Study for COVID-19 Vaccines. International Journal of Molecular Sciences, 23(15), 8235. https://doi.org/10.3390/ijms23158235