
Chemistry and Toxicology of Major Bioactive Substances in Inocybe Mushrooms

 ,
, 
 and
and 
Abstract
1. Introduction
2. Mycology
3. Inocybe Poisoning
3.1. Animal Poisoning
3.2. Human Poisoning
4. Inocybe Poisonous Substances
4.1. Muscarine
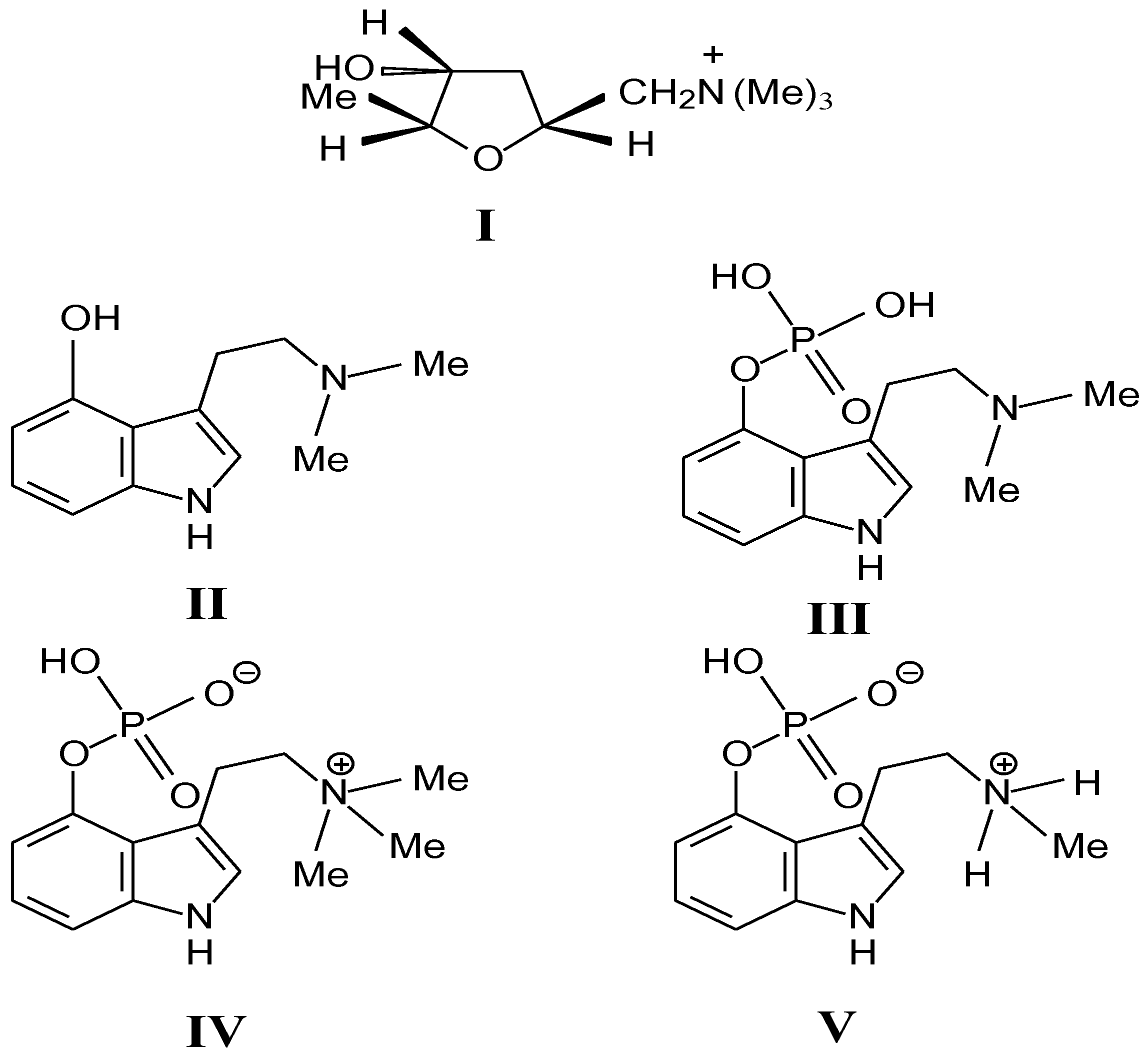
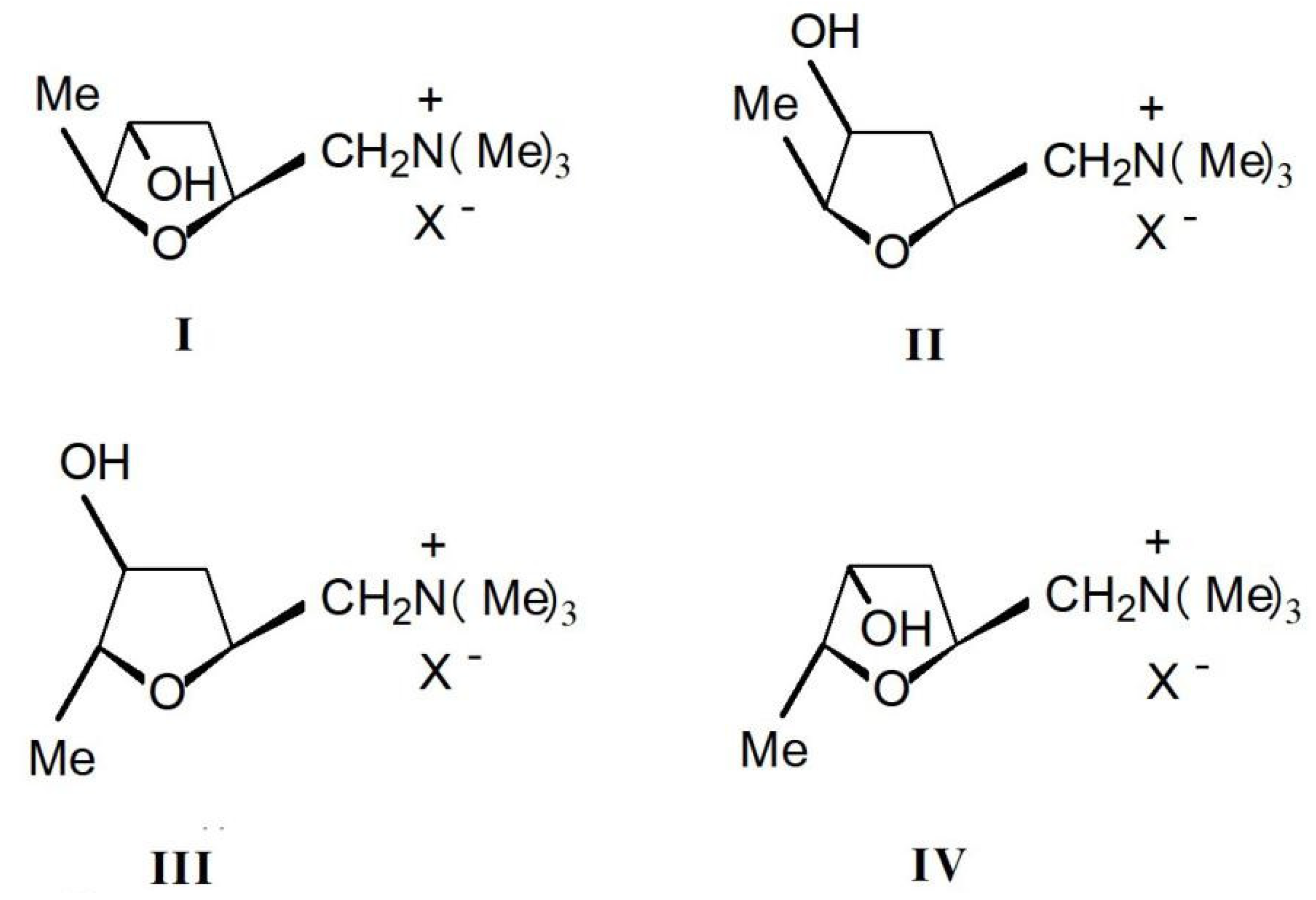
4.1.1. Chemistry and Stereochemistry
4.1.2. Poisonous Mechanism
4.1.3. Clinical Response
4.1.4. Experimental Toxicity
4.1.5. Human Toxicity
4.1.6. Treatment
4.2. Psilocybin and Psilocin
4.2.1. Chemical Structure
4.2.2. Physico-Chemical Characteristics
4.2.3. Poisonous Mechanism
4.2.4. Clinical Response
4.2.5. Treatment
4.2.6. Application
Medical
Physiological Research
4.3. Aeruginascin
4.4. Baeocystin
4.5. Lectins
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lurie, Y.; Wasser, S.P.; Taha, M.; Shehade, H.; Nijim, J.; Hoffmann, Y.; Basis, F.; Vardi, M.; Lavon, O.; Suaed, S.; et al. Mushroom poisoning from species of genus Inocybe (fiber head mushroom): A case series with exact species identification. Clin. Toxicol. 2009, 47, 562–565. [Google Scholar] [CrossRef]
- Hasuo, H.; Akasu, T.; Gallagher, J.P. Muscarine activates a nonselective cation current through a M3 muscarinic receptor subtype in rat dorsolateral septal nucleus neurons. J. Neurophysiol. 1996, 76, 2221–2230. [Google Scholar] [CrossRef] [PubMed]
- Klaassen, C.D.; Casarett, L.J.; Doull, J. Casarett and Doull’s Toxicology: The Basic Science of Poisons, 8th ed.; McGraw-Hill Education: New York, NY, USA, 2013; ISBN 9780071769235. [Google Scholar]
- Kirk, P.M. Species fungorum (version 20 November 2015). In Species 2000 & ITIS Catalogue of Life; The Catalogue of Life Partnership: Leiden, The Netherlands, 2019. [Google Scholar]
- Ryberg, M.; Kristiansson, E.; Sjökvist, E.; Nilsson, R.H. An outlook on the fungal internal transcribed spacer sequences in GenBank and the introduction of a web-based tool for the exploration of fungal diversity. New Phytol. 2009, 181, 471–477. [Google Scholar] [CrossRef]
- Puschner, B.; Wegenast, C. Mushroom poisoning cases in dogs and cats: Diagnosis and treatment of hepatotoxic, neurotoxic, gastroenterotoxic, nephrotoxic, and muscarineic mushrooms. Vet. Clin. N. Am. Small Anim. Pract. 2018, 48, 1053–1067. [Google Scholar] [CrossRef]
- Lin, H.T. Mushroom poisoning (Inocybe asterospora Quel.)—Report of 3 cases. Zhonghua Yu Fang Yi Xue Za Zhi 1984, 18, 231–233. (in Chinese). [Google Scholar]
- Seljetun, K.O.; von Krogh, A. Acute Inocybe mushroom toxicosis in dogs: 5 cases (2010–2014). J. Vet. Emerg. Crit. Care 2017, 27, 212–217. [Google Scholar] [CrossRef]
- Kohn, R.; Mot’ovská, Z. Mushroom poisoning--classification, symptoms and therapy. Vnitr. Lek. 1997, 43, 230–233. (in Slovak). [Google Scholar]
- Wilson, D. Poisoning by Inocybe fastigiata. Br. Med. J. 1947, 2, 297. [Google Scholar] [CrossRef][Green Version]
- Amitai, I.; Peleg, O.; Ariel, I.; Binyamini, N. Severe poisoning in a child by the mushroom Inocybe tristis, Malençon and Bertault. Isr. J. Med. Sci. 1982, 18, 798–801. [Google Scholar] [PubMed]
- Gartz, J.; Drewitz, G. The green discolored mushroom Inocybe aeruginascens--an Inocybe species with hallucinogenic effects. Z Arztl Fortbild 1986, 80, 551–553. (in German). [Google Scholar]
- Pradeep, C.K.; Vrinda, K.B.; Shibu, P.V.; Hailee, B.K.; Brandon Matheny, P. New species of Inocybe (Agaricales) from tropical India. Mycol. Prog. 2016, 15, 2–25. [Google Scholar] [CrossRef]
- Bijeesh, C.; Vrinda, K.B.; Pradeeo, C.K. Inocybe poisoning in Kerala—A case study. J. Mycopathol. Res. 2020, 57, 255–258. [Google Scholar]
- Xu, F.; Zhang, Y.Z.; Zhang, Y.H.; Guan, G.Y.; Zhang, K.P.; Li, H.J.; Wang, J.J. Mushroom poisoning from Inocybe serotina: A case report from Ningxia, northwest China with exact species identification and muscarine detection. Toxicon 2020, 179, 72–75. [Google Scholar] [CrossRef]
- Beuhler, M.C. Overview of mushroom poisoning. In Critical Care Toxicology: Diagnosis and Management of the Critically Poisoned Patient; Brent, J., Burkhart, K., Dargan, P., Hatten, B., Megarbane, B., Palmer, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 2103–2128. [Google Scholar]
- Hossain, M.A.; Park, S.C. A review on mushroom toxins. In Food Toxicology; Chapter 14; Bagchi, D., Swaroop, A., Eds.; CRC Press: Boca Raton, FL, USA, 2016; 584p, ISBN 9781498708753. [Google Scholar]
- Jin, Z. Muscarine, imidazole, oxazole, and thiazole alkaloids. Nat. Prod. Rep. 2003, 20, 584–605. [Google Scholar] [CrossRef]
- Brown, J.K.; Malone, M.H.; Stuntz, D.E.; Tyler, V.E., Jr. Paper chromatographic determination of muscarinee in Inocybe species. J. Pharm. Sci. 1962, 51, 853–856. [Google Scholar] [PubMed]
- Young, A. Muscarinee-Containing mushrooms. In Handbook of Mushroom Poisoning: Diagnosis and Treatment; Spoerke, D.G., Rumack, B.H., Eds.; CRC Press: Boca Raton, FL, USA, 1994; pp. 289–299. [Google Scholar]
- Malone, M.H.; Robichaud, R.; Tyler, V.E., Jr.; Brady, L. Relative muscarineic potency of thirty Inocybe species. Lloydia 1962, 25, 231–237. [Google Scholar]
- Catalfomo, P.; Eugster, C.H. Muscarinee and muscarinee isomers in selected Inocybe species. Helv. Chim. Acta 1970, 53, 848–851. [Google Scholar] [CrossRef]
- Gurevich, L.S.; Nezdoiminogo, E.L. Psilocybin and muscarinee as possible chemotaxonomic markers for the genus Inocybe (Fr) Fr. Mycol. Phytopathol. 1992, 262, 88–97. [Google Scholar]
- Raufman, J.P.; Samimi, R.; Shah, N.; Shah, N.; Khurana, S.; Shant, J.; Drachenberg, C.; Xie, G.; Wess, J.; Cheng, K. Genetic ablation of M3 muscarinic receptors attenuates murine colon epithelial cell proliferation and neoplasia. J. Cancer Res. 2008, 68, 3573–3578. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, B.; Ferenc, T.; Kusowska, J.; Ciećwierz, J.; Kowalczyk, E. Poisoning with selected mushrooms with neurotropic and hallucinogenic effect. Med. Pr. 2010, 61, 583–595. (in Polish). [Google Scholar]
- White, J.; Weinstein, S.; Haro, L.; Bedry, R.; Schaper, A.; Rumack, B.; Zilker, T. Mushroom poisoning: A proposed new clinical classification. Toxicon 2019, 157, 53–65. [Google Scholar] [CrossRef]
- Colloby, S.J.; Nathan, P.J.; McKeith, I.G.; Bakker, G.; O’Brien, J.T.; Taylor, J.P. Cholinergic muscarinic M(1)/M(4) receptor networks in dementia with Lewy bodies. Brain Commun. 2020, 2, fcaa098. [Google Scholar] [CrossRef] [PubMed]
- Matera, M.G.; Rinaldi, B.; Berardo, C.; Rinaldi, M.; Cazzola, M. A review of the pharmacokinetics of M(3) muscarinic receptor antagonists used for the treatment of asthma. Expert. Opin. Drug Metab. Toxicol. 2020, 16, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Fernández de Sevilla, D.; Núñez, A.; Buño, W. Muscarinic receptors, from synaptic plasticity to its role in network activity. Neuroscience 2021, 456, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.M.; Katzung, B.B. Základni a Klinická Farmakologie; Katzung, B.G., Ed.; H&H, Bom: Ružinov, Slovakia, 1992; p. 83. [Google Scholar]
- Kögl, F.; Duisberg, H.; Erxleben, H. Untersuchungen über Pilzgifte. I. Über das muscarine. I. Justus Leibigs Ann. der Chem. 1931, 489, 156–192. [Google Scholar] [CrossRef]
- Bovet, D.; Bovet-Nitti, F. Structure et Activite Pharmacodyanmique des Medicaments du Systeme Nerveux Vegetatif; Karge, S., Ed.; AAAS: New York, NY, USA, 1948; p. 406. [Google Scholar]
- Staib, A.H.; Schröder, M. Participation of the cholinergic system in temperature regulation by the mouse. Arch. Int. Pharmacodyn. Ther. 1971, 192, 88–95. (in German). [Google Scholar]
- Habermehl, G. Chemistry and biochemistry of amphibian poisons. Naturwissenschaften 1969, 56, 615–622. (in German). [Google Scholar] [CrossRef]
- Eltherington, C.D.; Barnes, L.G. Drug Dosages in Laboratory Animals—A Handbook; University California Press: Berkeley, CA, USA, 1973; 348p. [Google Scholar]
- Mosher, H.S.; Fuhrman, F.A.; Buchwald, H.D.; Fischer, H.G. Tarichatoxin—Tetrodotoxin: A potent neurotoxin. Science 1964, 144, 1100–1110. [Google Scholar] [CrossRef] [PubMed]
- Arena, J.M. Poisoning: Toxicology, Symptoms, Treatments, 2nd ed.; C.C. Thomas: Springfield, IL, USA, 1970; Volume 2, p. 73. [Google Scholar]
- Bresinsky, H.; Besl, A. A Colour Atlas of Poisonous Fungi, 1st ed.; Manson Publishing Ltd.: London, UK, 1989; 295p, ISBN-10: 9780723415763, ISBN-13: 978-0723415763. [Google Scholar]
- Jahodár, L. Prírodní Toxiny a Jedy; Houdek, L., Ed.; Galén: Prague, Czech Republic, 2004; p. 109. [Google Scholar]
- Hofman, A.; Heim, R.; Brack, A.; Kobel, H. Psilocybin einpsychotroper Wirkstoff aus dem mexikanischen Rauschpilz Psilocybe mexieana Heim. Experientia 1958, 14, 107. [Google Scholar] [CrossRef]
- Stebelska, K. Fungal hallucinogens psilocin, ibotenic acid, and muscimol: Analytical methods and biologic activities. Ther. Drug Monit. 2013, 35, 420–442. [Google Scholar] [CrossRef]
- Dinis-Oliveira, R.J. Metabolism of psilocybin and psilocin: Clinical and forensic toxicological relevance. Drug Metab. Rev. 2017, 49, 84–91. [Google Scholar] [CrossRef]
- Beug, M.W.; Bigwood, J. Quantitive analysis of psilocybin andpsilocin in Psilocybe baeocystis by HPLC and TLC. J. Chromatogr. 1981, 207, 379–385. [Google Scholar] [CrossRef]
- Lenz, C.; Wick, J.; Braga, D.; García-Altares, M.; Lackner, G.; Hertweck, C.; Gressler, M.; Hoffmeister, D. Injury-triggered blueing reactions of psilocybe “Magic” mushrooms. Angew Chem. Int. Ed. Engl. 2020, 59, 1450–1454. [Google Scholar] [CrossRef] [PubMed]
- Leikin, J.B.; Krantz, A.J.; Zell-Kanter, M.; Barkin, R.L.; Hryhorczuk, D.O. Clinical features andmanagement of intoxication due to hallucingenic drugs. Med. Toxicol. Advers. Drug Exp. 1989, 4, 324–350. [Google Scholar] [CrossRef]
- Vollenweider, F.X.; Geyer, M.A. A systems model of altered con-sciousness: Integrating natural and grug-induced psychoses. BrainResBull 2001, 56, 495–507. [Google Scholar]
- Vollenweider, F.X.; Vontobel, P.; Hell, D.; Leenders, K.L. 5-HT modulationof dopamine release in basal ganglia in psilocybin—Induced psy-chosis in man---aPET study with [11C] raclopride. Neuropsychopharmacology 1999, 20, 424–433. [Google Scholar] [CrossRef]
- Vollenweider, F.X.; Vollenweider-Schhherpenhuyzen, M.F.; Babler, A.; Vogel, H.; Hell, D. Psilocybin induces schizophrenia-like psychosisin humanvia a serotonin-2 agonist action. Neuroreport 1998, 9, 3897–3902. [Google Scholar] [CrossRef]
- Buckholtz, N.S.; Zhou, D.F.; Freedman, D.X.; Potter, W.Z. LSD administration selectively down regulates serotonin2 receptors in rat brain. Neuropsychopharmacology 1990, 3, 137–148. [Google Scholar] [PubMed]
- Rambousek, L.; Páleníček, T.; Valeš, K.; Stuchlík, A. The effect of psilocin on memory acquisition, retrieval, and consolidation in the rat. Front. Behav. Neurosci. 2014, 8, 180. [Google Scholar] [CrossRef]
- López-Giménez, J.; González-Maeso, J. Hallucinogens and serotonin 5-HT(2A) receptor-mediated signaling pathways. Curr. Top. Behav. Neurosci. 2018, 36, 45–73. [Google Scholar]
- Passie, T.; Seifert, J.; Schneider, U.; Emrich, H.M. The pharmacology of psilocybin. Addict. Biol. 2002, 7, 357–364. [Google Scholar] [CrossRef]
- Bosin, T.R.; Campaigne, E.; Dinner, A.; Rogers, R.B.; Maickel, R.P. Comparative toxicological studies of indole, benzo[b] thiophene, and 1-methylindole derivatives. J. Toxicol. Environ. Health 1976, 1, 515–520. [Google Scholar] [CrossRef]
- Usdin, E.; Efron, D.H. Psychotropic Drugs and Related Compounds, 2nd ed.; Pergamon Pr: Washington, DC, USA, 1972; p. 138. [Google Scholar]
- Mills, P.R.; Lesinskas, D.; Watkinson, G. The danger of hallucinogenic mushrooms. Scot. Med. J. 1979, 24, 316–317. [Google Scholar] [CrossRef]
- Griffiths, R.R. Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology 2006, 187, 268–283. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R. Psilocybin occasioned mystical-type experiences: Immediate and persisting dose-related effects. Psychopharmacology 2011, 218, 649–665. [Google Scholar] [CrossRef]
- Hasler, F. Acute psychological and physiological effects of psilocybin in healthy humans: A double-blind, placebo-controlled dose-effect study. Psychopharmacology 2004, 172, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Smolinske, S.C. Psilocybin-Containing mushrooms. In Handbook of Mushroom Poisoning Diagnosis and Treatment; Spoerke, D.G., Rumack, B.H., Eds.; CRC Press: Boca Raton, FL, USA, 1994; pp. 309–324. [Google Scholar]
- Allen, J.W.; Merlin, M.D.; Jansen, K. An ethnomycological review of psychoactive agarics in Australia and New Iealand. Psychoact. Drugs 1991, 23, 39. [Google Scholar] [CrossRef] [PubMed]
- Lampe, K.F. Toxic fungi. Rev. Pharmacol. Toxicol. 1979, 19, 85. [Google Scholar] [CrossRef]
- Shulgin, A.T. Profiles of psychedelic drugs: 8 psilocybin. Psychedelic Drugs 1980, 12, 79. [Google Scholar] [CrossRef]
- Young, R.E.; Hutchison, S.; Milroy, R. The rising price of mushrooms. Lancet 1982, 1, 213. [Google Scholar] [CrossRef]
- Benjamin, D.R. Mushrooms: Poisons and panaceas:a handbook fornaturalists, mycologosts, and physicans. Nature 1996, 379, 503–504. [Google Scholar]
- Shirota, O.; Hakamata, W.; Goda, Y. Concise large-scale synthesis of psilocin and psilocybin, principal hallucinogenic constituents of “magic mushroom”. J. Nat. Prod. 2003, 66, 885–887. [Google Scholar] [CrossRef] [PubMed]
- Tylš, F.; Páleníček, T.; Horáček, J. Psilocybin–Summary of knowledge and new perspectives. Eur. Neuropsychopharmacol. 2014, 24, 342–356. [Google Scholar] [CrossRef] [PubMed]
- Horgan, J. The electric koolaid clinical trial: LSD and other hallucinogens were once considered promising psychiatric treatments. New Sci. 2005, 185, 36–39. [Google Scholar]
- Grinspoon, L.; Dobin, R. Psychedelics as catalysts of insight-oriented psychotherapy. Soc. Res. 2001, 68, 667–695. [Google Scholar]
- Bressloff, P.C.; Cowan, J.D.; Golubitsky, M.; Thomas, P.J.; Wiener, M.C. What geometric visual hallucinations tell us about the visual cortex. Neural. Comput. 2002, 14, 473–491. [Google Scholar] [CrossRef] [PubMed]
- Carter, O.L.; Burr, D.C.; Pettigrew, J.D.; Wallis, G.M.; Hasler, F.; Vollenweider, F.X. Using psilocybin to investigate the relationship between attention, working memory, and the serotonin 1A and 2A receptors. J. Cogn. Neurosci. 2005, 17, 1497–1508. [Google Scholar] [CrossRef]
- Carter, O.L.; Pettigrew, J.D.; Hasler, F.; Wallis, G.M.; Liu, G.B.; Hell, D.; Vollenweider, F.X. Modulating the rate and rhythmicity of perceptual rivalry alternationswith the mixed 5-HT2A and 5-HTlA agonist psilocybin. Neuropsychopharmacology 2005, 30, 1154–1162. [Google Scholar] [CrossRef]
- Hery, F.; Hamon, M. Neuroleptics and serotonin. L’Encephale 1993, 19, 525–532. [Google Scholar]
- Gartz, J. Analysis of aeruginascin in fruit bodies of the mushroom Inocybe aeruginascens. Int. J. Crude Drug Res. 1989, 27, 141–144. [Google Scholar] [CrossRef]
- Jensen, N.; Gartz, J.; Laatsch, H. Aeruginascin, a trimethylammonium analogue of psilocybin from the hallucinogenic mushroom Inocybe aeruginascens. Planta Med. 2006, 72, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Wieland, H.; Konz, W.; Mittasch, H. Toad poisons. VII. Constitution of bufotenin and bufotenidine. Justus Leibigs Ann. der Chem. 1934, 513, 1–25. [Google Scholar] [CrossRef]
- Leung, A.Y.; Paul, A.G. Baeocystin, a mono-methyl analog of psilocybin from Psilocybe baeocystis saprophytic culture. J. Pharm. Sci. 1967, 56, 146. [Google Scholar] [CrossRef]
- Leung, A.Y.; Paul, A.G. Baeocystin and norbaeocystin: New analogs of psilocybin from Psilocybe baeocystis. J. Pharm. Sci. 1968, 57, 1667–1671. [Google Scholar] [CrossRef]
- Repke, D.B.; Leslie, D.T. Baeocystin in Psilocybe semilanceata. J. Pharm. Sci. 1977, 66, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Repke, D.B.; Leslie, D.T.; Guzman, G. Baeocystin in psilocybe, conocybe and panaeolus. Lloydia 1977, 40, 566–578. [Google Scholar] [PubMed]
- Troxler, F.; Seeman, F.; Hofmann, A. Abwandlungsprodukte von Psilocybin und Psilocin. 2. Mitteilung über synthetische Indolverbindungen. Helvetica Chimica Acta 1959, 42, 2073–2103. (in German). [Google Scholar] [CrossRef]
- Mckenna, D.J.; Repke, D.B.; Lo, L.; Peroutka, S.J. Differential interactions of indolealkylamines with 5-hydroxytryptamine receptor subtypes. Neuropharmacology 1990, 29, 193–198. [Google Scholar] [CrossRef]
- Sarup Singh, R.; Preet Kaur, H.; Rakesh Kanwar, J. Mushroom lectins as promising anticancer substances. Curr. Protein Pept. Sci. 2016, 17, 797–807. [Google Scholar] [CrossRef]
- Zhao, J.K.; Wang, H.X.; Ng, T.B. Purification and characterization of a novel lectin from the toxic wild mushroom Inocybe umbrinella. Toxicon 2009, 53, 360–366. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organism | Test Type | Route | Reported Dose | Literature Source |
|---|---|---|---|---|
| frog | LDLo | parenteral | 0.16 mg/kg | [31] |
| frog | LDLo | unreported | 0.16 mg/kg | [32] |
| mouse | LD50 | intraperitoneal | 5 mg/kg | [33] |
| mouse | LD50 | intravenous | 0.23 mg/kg | Toxnet |
| mouse | LD50 | subcutaneous | 1.1 mg/kg | [34] |
| mouse | LDLo | oral | 750 mg/kg | [35] |
| rabbit | LDLo | oral | 150 mg/kg | Toxnet |
| rabbit | LDLo | subcutaneous | 27 mg/kg | Toxnet |
| cat | LDLo | intravenous | 1.1 mg/kg | [36] |
| cat | LDLo | oral | 7 mg/kg | Toxnet |
| cat | LDLo | subcutaneous | 2 mg/kg | [32] |
| man | LDLo | unreported | 0.735 mg/kg | [37] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patocka, J.; Wu, R.; Nepovimova, E.; Valis, M.; Wu, W.; Kuca, K. Chemistry and Toxicology of Major Bioactive Substances in Inocybe Mushrooms. Int. J. Mol. Sci. 2021, 22, 2218. https://doi.org/10.3390/ijms22042218
Patocka J, Wu R, Nepovimova E, Valis M, Wu W, Kuca K. Chemistry and Toxicology of Major Bioactive Substances in Inocybe Mushrooms. International Journal of Molecular Sciences. 2021; 22(4):2218. https://doi.org/10.3390/ijms22042218
Chicago/Turabian StylePatocka, Jiri, Ran Wu, Eugenie Nepovimova, Martin Valis, Wenda Wu, and Kamil Kuca. 2021. "Chemistry and Toxicology of Major Bioactive Substances in Inocybe Mushrooms" International Journal of Molecular Sciences 22, no. 4: 2218. https://doi.org/10.3390/ijms22042218
APA StylePatocka, J., Wu, R., Nepovimova, E., Valis, M., Wu, W., & Kuca, K. (2021). Chemistry and Toxicology of Major Bioactive Substances in Inocybe Mushrooms. International Journal of Molecular Sciences, 22(4), 2218. https://doi.org/10.3390/ijms22042218