
Nanomaterials for Antiangiogenic Therapies for Cancer: A Promising Tool for Personalized Medicine

 ,
,  , , and
, , and
Abstract

1. Introduction
2. Angiogenesis Pathways and Biomarkers
2.1. Angiogenesis Pathways in Cancer
2.2. Antiangiogenic Biomarkers
2.2.1. Integrins
2.2.2. VEGF
2.3. Importance of Angiogenesis Biomarker Imaging
3. Clinical Trials in Antiangiogenic Therapeutics
3.1. Selected Examples of FDA Approved Antiangiogenic Agents
3.1.1. Bevacizumab (Avastin®)
3.1.2. Sunitinib (Sutent®)
3.1.3. Everolimus (Afinitor®)
3.2. Angiogenesis Inhibitor Challenges
4. Utilizing Nanomedicine for Antiangiogenic Medication
4.1. Nano-Antiangiogenic-Based Cancer Monotherapy
4.2. Synergistic Antiangiogenetic Activity with Chemotherapy
4.3. Synergistic Antiangiogenic Activity with Gene Therapy
4.4. Synergistic Antiangiogenetic Activity with Immunotherapy
4.5. Synergistic Antitumor Microenvironment Agents/Photodynamic Therapy
5. Significance of Antiangiogenics-Based Theranostic Agents and Possible Mechanisms
6. Imaging Modalities Utilized for the Theranostic Purpose of Better Nanomaterials
7. Conclusions and Future Prospects
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Goding Sauer, A.; Ortiz, A.P.; Fedewa, S.A.; Pinheiro, P.S.; Tortolero-Luna, G.; Martinez-Tyson, D.; Jemal, A.; Siegel, R.L. Cancer statistics for hispanics/latinos, 2018. CA Cancer J. Clin. 2018, 68, 425–445. [Google Scholar] [CrossRef] [PubMed]
- Bergers, G.; Hanahan, D. Modes of resistance to anti-angiogenic therapy. Nat. Rev. Cancer 2008, 8, 592–603. [Google Scholar] [CrossRef]
- De Bock, K.; Mazzone, M.; Carmeliet, P. Antiangiogenic therapy, hypoxia, and metastasis: Risky liaisons, or not? Nat. Rev. Clin. Oncol. 2011, 8, 393. [Google Scholar] [CrossRef]
- Hollebecque, A.; Massard, C.; Soria, J.-C. Vascular disrupting agents: A delicate balance between efficacy and side effects. Curr. Opin. Oncol. 2012, 24, 305–315. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Z.; Zhang, Y.; Cao, F.; Dong, K.; Ren, J.; Qu, X. Erythrocyte membrane cloaked metal–organic framework nanoparticle as biomimetic nanoreactor for starvation-activated colon cancer therapy. ACS Nano 2018, 12, 10201–10211. [Google Scholar] [CrossRef] [PubMed]
- Bussolati, B.; Grange, C.; Camussi, G. Tumor exploits alternative strategies to achieve vascularization. FASEB J. 2011, 25, 2874–2882. [Google Scholar] [CrossRef]
- de Oliveira, R.L.; Hamm, A.; Mazzone, M. Growing tumor vessels: More than one way to skin a cat–implications for angiogenesis targeted cancer therapies. Mol. Asp. Med. 2011, 32, 71–87. [Google Scholar] [CrossRef]
- Crawford, Y.; Ferrara, N. Tumor and stromal pathways mediating refractoriness/resistance to anti-angiogenic therapies. Trends Pharmacol. Sci. 2009, 30, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Potente, M.; Gerhardt, H.; Carmeliet, P. Basic and therapeutic aspects of angiogenesis. Cell 2011, 146, 873–887. [Google Scholar] [CrossRef] [PubMed]
- Carmeliet, P.; Jain, R.K. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011, 473, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Eavarone, D.; Capila, I.; Zhao, G.; Watson, N.; Kiziltepe, T.; Sasisekharan, R. Temporal targeting of tumour cells and neovasculature with a nanoscale delivery system. Nature 2005, 436, 568–572. [Google Scholar] [CrossRef]
- Li, S.; Jiang, Q.; Liu, S.; Zhang, Y.; Tian, Y.; Song, C.; Wang, J.; Zou, Y.; Anderson, G.J.; Han, J.-Y. A DNA nanorobot functions as a cancer therapeutic in response to a molecular trigger in vivo. Nat. Biotechnol. 2018, 36, 258. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Tang, Z.; Hu, C.; Zhang, D.; Shen, N.; Yu, H.; Chen, X. Selectively Potentiating Hypoxia Levels by Combretastatin A4 Nanomedicine: Toward Highly Enhanced Hypoxia-Activated Prodrug Tirapazamine Therapy for Metastatic Tumors. Adv. Mater. 2019, 31, 1805955. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, D.; Song, W.; Tang, Z.; Zhu, J.; Ma, Z.; Wang, X.; Chen, X.; Tong, T. A poly (L-glutamic acid)-combretastatin A4 conjugate for solid tumor therapy: Markedly improved therapeutic efficiency through its low tissue penetration in solid tumor. Acta Biomater. 2017, 53, 179–189. [Google Scholar] [CrossRef]
- Zhang, E.; Xing, R.; Liu, S.; Li, K.; Qin, Y.; Yu, H.; Li, P. Vascular targeted chitosan-derived nanoparticles as docetaxel carriers for gastric cancer therapy. Int. J. Biol. Macromol. 2019, 126, 662–672. [Google Scholar] [CrossRef]
- Zhang, R.; Feng, L.; Dong, Z.; Wang, L.; Liang, C.; Chen, J.; Ma, Q.; Chen, Q.; Wang, Y.; Liu, Z. Glucose & oxygen exhausting liposomes for combined cancer starvation and hypoxia-activated therapy. Biomaterials 2018, 162, 123–131. [Google Scholar]
- Chen, Y.; Huang, X.; Zhang, S.; Li, S.; Cao, S.; Pei, X.; Zhou, J.; Feng, X.; Wang, B. Shaping of metal–organic frameworks: From fluid to shaped bodies and robust foams. J. Am. Chem. Soc. 2016, 138, 10810–10813. [Google Scholar] [CrossRef]
- Chung, B.L.; Toth, M.J.; Kamaly, N.; Sei, Y.J.; Becraft, J.; Mulder, W.J.; Fayad, Z.A.; Farokhzad, O.C.; Kim, Y.; Langer, R. Nanomedicines for endothelial disorders. Nano Today 2015, 10, 759–776. [Google Scholar] [CrossRef]
- Guarnieri, D.; Malvindi, M.A.; Belli, V.; Pompa, P.P.; Netti, P. Effect of silica nanoparticles with variable size and surface functionalization on human endothelial cell viability and angiogenic activity. J. Nanopart. Res. 2014, 16, 1–14. [Google Scholar] [CrossRef]
- Veeranarayanan, S.; Poulose, A.C.; Mohamed, M.S.; Nagaoka, Y.; Kashiwada, S.; Maekawa, T.; Kumar, D.S. FITC/suramin harboring silica nanoformulations for cellular and embryonic imaging/anti-angiogenic theranostics. J. Mater. Chem. B 2015, 3, 8079–8087. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, A.; Melillo, G. Role of the VEGF/VEGFR axis in cancer biology and therapy. In Advances in Cancer Research; Elsevier: Amsterdam, The Netherlands, 2012; Volume 114, pp. 237–267. [Google Scholar]
- Clarke, J.M.; Hurwitz, H.I. Targeted inhibition of VEGF receptor 2: An update on ramucirumab. Expert Opin. Biol. Ther. 2013, 13, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.M.; Hurwitz, H.I. Understanding and targeting resistance to anti-angiogenic therapies. J. Gastrointest. Oncol. 2013, 4, 253. [Google Scholar]
- Hatch, A.J.; Clarke, J.M.; Nixon, A.B.; Hurwitz, H.I. Identifying blood-based protein biomarkers for antiangiogenic agents in the clinic: A decade of progress. Cancer J. 2015, 21, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Secord, A.A.; Nixon, A.B.; Hurwitz, H.I. The search for biomarkers to direct antiangiogenic treatment in epithelial ovarian cancer. Gynecol. Oncol. 2014, 135, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Teleanu, R.I.; Chircov, C.; Grumezescu, A.M.; Teleanu, D.M. Tumor angiogenesis and anti-angiogenic strategies for cancer treatment. J. Clin. Med. 2020, 9, 84. [Google Scholar] [CrossRef]
- Crich, S.G.; Terreno, E.; Aime, S. Nano-sized and other improved reporters for magnetic resonance imaging of angiogenesis. Adv. Drug Deliv. Rev. 2017, 119, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhang, K.; Tao, H.; Du, W.; Wang, D.; Huang, Z.; Zhou, M.; Xu, Y.; Wang, Y.; Liu, N. Molecular imaging of tumor angiogenesis and therapeutic effects with dual bioluminescence. Curr. Pharm. Biotechnol. 2017, 18, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Alday-Parejo, B.; Stupp, R.; Rüegg, C. Are integrins still practicable targets for anti-cancer therapy? Cancers 2019, 11, 978. [Google Scholar] [CrossRef]
- Avraamides, C.J.; Garmy-Susini, B.; Varner, J.A. Integrins in angiogenesis and lymphangiogenesis. Nat. Rev. Cancer 2008, 8, 604–617. [Google Scholar] [CrossRef]
- Beer, A.J.; Schwaiger, M. Imaging of integrin αvβ3 expression. Cancer Metastasis Rev. 2008, 27, 631–644. [Google Scholar] [CrossRef]
- Koch, S.; Tugues, S.; Li, X.; Gualandi, L.; Claesson-Welsh, L. Signal transduction by vascular endothelial growth factor receptors. Biochem. J. 2011, 437, 169–183. [Google Scholar] [CrossRef]
- Tugues, S.; Koch, S.; Gualandi, L.; Li, X.; Claesson-Welsh, L. Vascular endothelial growth factors and receptors: Anti-angiogenic therapy in the treatment of cancer. Mol. Asp. Med. 2011, 32, 88–111. [Google Scholar] [CrossRef]
- Ribatti, D. Novel angiogenesis inhibitors: Addressing the issue of redundancy in the angiogenic signaling pathway. Cancer Treat. Rev. 2011, 37, 344–352. [Google Scholar] [CrossRef]
- Sharma, P.S.; Sharma, R.; Tyagi, T. VEGF/VEGFR pathway inhibitors as anti-angiogenic agents: Present and future. Curr. Cancer Drug Targets 2011, 11, 624–653. [Google Scholar] [CrossRef]
- Schliemann, C.; Neri, D. Antibody-based vascular tumor targeting. In Angiogenesis Inhibition; Springer: Berlin, Germany, 2010; pp. 201–216. [Google Scholar]
- Carmeliet, P.; Jain, R.K. Principles and mechanisms of vessel normalization for cancer and other angiogenic diseases. Nat. Rev. Drug Discov. 2011, 10, 417–427. [Google Scholar] [CrossRef]
- Abdalla, A.M.; Xiao, L.; Ullah, M.W.; Yu, M.; Ouyang, C.; Yang, G. Current challenges of cancer anti-angiogenic therapy and the promise of nanotherapeutics. Theranostics 2018, 8, 533. [Google Scholar] [CrossRef] [PubMed]
- Fallah, A.; Sadeghinia, A.; Kahroba, H.; Samadi, A.; Heidari, H.R.; Bradaran, B.; Zeinali, S.; Molavi, O. Therapeutic targeting of angiogenesis molecular pathways in angiogenesis-dependent diseases. Biomed. Pharm. 2019, 110, 775–785. [Google Scholar] [CrossRef] [PubMed]
- Alfaleh, M.A.; Alsaab, H.O.; Mahmoud, A.B.; Alkayyal, A.A.; Jones, M.L.; Mahler, S.M.; Hashem, A.M. Phage display derived monoclonal antibodies: From bench to bedside. Front. Immunol. 2020, 11, 1986. [Google Scholar] [CrossRef]
- Darweesh, R.S.; Ayoub, N.M.; Nazzal, S. Gold nanoparticles and angiogenesis: Molecular mechanisms and biomedical applications. Int. J. Nanomed. 2019, 14, 7643. [Google Scholar] [CrossRef]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 2020, 86, 102017. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef]
- Sandler, A.; Gray, R.; Perry, M.C.; Brahmer, J.; Schiller, J.H.; Dowlati, A.; Lilenbaum, R.; Johnson, D.H. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N. Engl. J. Med. 2006, 355, 2542–2550. [Google Scholar] [CrossRef]
- Maj, E.; Papiernik, D.; Wietrzyk, J. Antiangiogenic cancer treatment: The great discovery and greater complexity (Review). Int. J. Oncol. 2016, 49, 1773–1784. [Google Scholar] [CrossRef] [PubMed]
- Grignol, V.P.; Olencki, T.; Relekar, K.; Taylor, C.; Kibler, A.; Kefauver, C.; Wei, L.; Walker, M.J.; Chen, H.X.; Kendra, K.; et al. A phase 2 trial of bevacizumab and high-dose interferon alpha 2B in metastatic melanoma. J. Immunother. 2011, 34, 509–515. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Approves Bevacizumab in Combination with Chemotherapy for Ovarian Cancer. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-bevacizumab-combination-chemotherapy-ovarian-cancer (accessed on 15 April 2020).
- FDA. FDA Approves Atezolizumab Plus Bevacizumab for Unresectable Hepatocellular Carcinoma. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-atezolizumab-plus-bevacizumab-unresectable-hepatocellular-carcinoma (accessed on 15 April 2020).
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Hao, Z.; Sadek, I. Sunitinib: The antiangiogenic effects and beyond. Onco Targets Ther. 2016, 9, 5495–5505. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.-A.; Han, Z.; Popel, A.S.; Pandey, N.B. Antiangiogenic cancer drug sunitinib exhibits unexpected proangiogenic effects on endothelial cells. Onco Targets Ther. 2014, 7, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Moehler, M.; Gepfner-Tuma, I.; Maderer, A.; Thuss-Patience, P.C.; Ruessel, J.; Hegewisch-Becker, S.; Wilke, H.; Al-Batran, S.E.; Rafiyan, M.R.; Weißinger, F.; et al. Sunitinib added to FOLFIRI versus FOLFIRI in patients with chemorefractory advanced adenocarcinoma of the stomach or lower esophagus: A randomized, placebo-controlled phase II AIO trial with serum biomarker program. BMC Cancer 2016, 16, 699. [Google Scholar] [CrossRef]
- Polena, H.; Creuzet, J.; Dufies, M.; Sidibé, A.; Khalil-Mgharbel, A.; Salomon, A.; Deroux, A.; Quesada, J.-L.; Roelants, C.; Filhol, O.; et al. The tyrosine-kinase inhibitor sunitinib targets vascular endothelial (VE)-cadherin: A marker of response to antitumoural treatment in metastatic renal cell carcinoma. Br. J. Cancer 2018, 118, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.-L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Honer, M.; Ebenhan, T.; Allegrini, P.R.; Ametamey, S.M.; Becquet, M.; Cannet, C.; Lane, H.A.; O’Reilly, T.M.; Schubiger, P.A.; Sticker-Jantscheff, M.; et al. Anti-Angiogenic/Vascular Effects of the mTOR Inhibitor Everolimus Are Not Detectable by FDG/FLT-PET. Transl. Oncol. 2010, 3, 264–275, IN6–IN7. [Google Scholar] [CrossRef][Green Version]
- Buti, S.; Leonetti, A.; Dallatomasina, A.; Bersanelli, M. Everolimus in the management of metastatic renal cell carcinoma: An evidence-based review of its place in therapy. Core Evid. 2016, 11, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; Oudard, S.; Hutson, T.E.; Porta, C.; Bracarda, S.; Grünwald, V.; Thompson, J.A.; Figlin, R.A.; Hollaender, N.; et al. Efficacy of everolimus in advanced renal cell carcinoma: A double-blind, randomised, placebo-controlled phase III trial. Lancet 2008, 372, 449–456. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; De Vries, E.G. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef]
- Baselga, J.; Campone, M.; Piccart, M.; Burris, H.A., 3rd; Rugo, H.S.; Sahmoud, T.; Noguchi, S.; Gnant, M.; Pritchard, K.I.; Lebrun, F.; et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 2012, 366, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Lupo, G.; Caporarello, N.; Olivieri, M.; Cristaldi, M.; Motta, C.; Bramanti, V.; Avola, R.; Salmeri, M.; Nicoletti, F.; Anfuso, C.D. Anti-angiogenic Therapy in Cancer: Downsides and New Pivots for Precision Medicine. Front. Pharm. 2017, 7, 519. [Google Scholar] [CrossRef]
- Haibe, Y.; Kreidieh, M.; El Hajj, H.; Khalifeh, I.; Mukherji, D.; Temraz, S.; Shamseddine, A. Resistance Mechanisms to Anti-angiogenic Therapies in Cancer. Front. Oncol. 2020, 10, 221. [Google Scholar] [CrossRef] [PubMed]
- Zarrin, B.; Zarifi, F.; Vaseghi, G.; Javanmard, S.H. Acquired tumor resistance to antiangiogenic therapy: Mechanisms at a glance. J. Res. Med. Sci. 2017, 22, 117. [Google Scholar] [CrossRef]
- Ribatti, D.; Annese, T.; Ruggieri, S.; Tamma, R.; Crivellato, E. Limitations of Anti-Angiogenic Treatment of Tumors. Transl. Oncol. 2019, 12, 981–986. [Google Scholar] [CrossRef]
- Loges, S.; Schmidt, T.; Carmeliet, P. Mechanisms of resistance to anti-angiogenic therapy and development of third-generation anti-angiogenic drug candidates. Genes Cancer 2010, 1, 12–25. [Google Scholar] [CrossRef]
- Jain, R.K.; Duda, D.G.; Willett, C.G.; Sahani, D.V.; Zhu, A.X.; Loeffler, J.S.; Batchelor, T.T.; Sorensen, A.G. Biomarkers of response and resistance to antiangiogenic therapy. Nat. Rev. Clin. Oncol. 2009, 6, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Hashemi Goradel, N.; Ghiyami-Hour, F.; Jahangiri, S.; Negahdari, B.; Sahebkar, A.; Masoudifar, A.; Mirzaei, H. Nanoparticles as new tools for inhibition of cancer angiogenesis. J. Cell. Physiol. 2018, 233, 2902–2910. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, B.; Hojjat-Farsangi, M.; Mohammadi, H.; Anvari, E.; Ghalamfarsa, G.; Yousefi, M.; Jadidi-Niaragh, F. Nanoparticles and targeted drug delivery in cancer therapy. Immunol. Lett. 2017, 190, 64–83. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J. The role of VEGF and EGFR inhibition: Implications for combining anti–VEGF and anti–EGFR agents. Mol. Cancer Res. 2007, 5, 203–220. [Google Scholar] [CrossRef] [PubMed]
- Vasudev, N.S.; Reynolds, A.R. Anti-angiogenic therapy for cancer: Current progress, unresolved questions and future directions. Angiogenesis 2014, 17, 471–494. [Google Scholar] [CrossRef] [PubMed]
- Brioschi, A.M.; Calderoni, S.; Pradotto, L.G.; Guido, M.; Strada, A.; Zenga, F.; Benech, C.A.; Benech, F.; Serpe, L.; Zara, G.P. Solid lipid nanoparticles carrying oligonucleotides inhibit vascular endothelial growth factor expression in rat glioma models. J. Nanoneurosci. 2009, 1, 65–74. [Google Scholar] [CrossRef]
- Bhattacharya, R.; Mukherjee, P.; Xiong, Z.; Atala, A.; Soker, S.; Mukhopadhyay, D. Gold nanoparticles inhibit VEGF165-induced proliferation of HUVEC cells. Nano Lett. 2004, 4, 2479–2481. [Google Scholar] [CrossRef]
- Mukherjee, P.; Bhattacharya, R.; Wang, P.; Wang, L.; Basu, S.; Nagy, J.A.; Atala, A.; Mukhopadhyay, D.; Soker, S. Antiangiogenic properties of gold nanoparticles. Clin. Cancer Res. 2005, 11, 3530–3534. [Google Scholar] [CrossRef]
- Gurunathan, S.; Lee, K.-J.; Kalishwaralal, K.; Sheikpranbabu, S.; Vaidyanathan, R.; Eom, S.H. Antiangiogenic properties of silver nanoparticles. Biomaterials 2009, 30, 6341–6350. [Google Scholar] [CrossRef] [PubMed]
- Jo, D.H.; Kim, J.H.; Yu, Y.S.; Lee, T.G.; Kim, J.H. Antiangiogenic effect of silicate nanoparticle on retinal neovascularization induced by vascular endothelial growth factor. Nanomed. Nanotechnol. Biol. Med. 2012, 8, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S. Recent progress toward antiangiogenesis application of nanomedicine in cancer therapy. Future Sci. OA 2018, 4, FSO318. [Google Scholar] [CrossRef]
- Cheriyan, V.T.; Alsaab, H.; Sekhar, S.; Venkatesh, J.; Mondal, A.; Vhora, I.; Sau, S.; Muthu, M.; Polin, L.A.; Levi, E. A CARP-1 functional mimetic compound is synergistic with BRAF-targeting in non-small cell lung cancers. Oncotarget 2018, 9, 29680. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Harfouche, R.; Sengupta, S. Nanotechnology-mediated targeting of tumor angiogenesis. Vasc. Cell 2011, 3, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Alzhrani, R.; Alsaab, H.O.; Petrovici, A.; Bhise, K.; Vanamala, K.; Sau, S.; Krinock, M.J.; Iyer, A.K. Improving the therapeutic efficiency of noncoding RNAs in cancers using targeted drug delivery systems. Drug Discov. Today 2020, 25, 718–730. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Chen, Z.; Zeng, X.; Chen, X.; Gu, Z. Advances in nanomedicine for cancer starvation therapy. Theranostics 2019, 9, 8026. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.G.; Jo, S.D.; Yhee, J.Y.; Lee, B.S.; Lee, S.J.; Park, S.G.; Kang, S.-W.; Kim, S.H.; Jeong, J.H. Synergistic anti-tumor effects of bevacizumab and tumor targeted polymerized VEGF siRNA nanoparticles. Biochem. Biophys. Res. Commun. 2017, 489, 35–41. [Google Scholar] [CrossRef]
- Kim, J.; Mirando, A.C.; Popel, A.S.; Green, J.J. Gene delivery nanoparticles to modulate angiogenesis. Adv. Drug Deliv. Rev. 2017, 119, 20–43. [Google Scholar] [CrossRef]
- Bharali, D.J.; Rajabi, M.; Mousa, S.A. Application of nanotechnology to target tumor angiogenesis in cancer therapeutics. In Anti-Angiogenesis Strategies in Cancer Therapeutics; Elsevier: Amsterdam, The Netherlands, 2017; pp. 165–178. [Google Scholar]
- Liu, T.; Ye, L.; He, Y.; Chen, X.; Peng, J.; Zhang, X.; Yi, H.; Peng, F.; Leng, A. Combination gene therapy using VEGF-shRNA and fusion suicide gene yCDglyTK inhibits gastric carcinoma growth. Exp. Mol. Pathol. 2011, 91, 745–752. [Google Scholar] [CrossRef]
- Shi, Y.; Lammers, T. Combining nanomedicine and immunotherapy. Acc. Chem. Res. 2019, 52, 1543–1554. [Google Scholar] [CrossRef]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. PD-1 and PD-L1 checkpoint signaling inhibition for cancer immunotherapy: Mechanism, combinations, and clinical outcome. Front. Pharm. 2017, 8, 561. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.A.; Kerbel, R.S. Improving immunotherapy outcomes with anti-angiogenic treatments and vice versa. Nat. Rev. Clin. Oncol. 2018, 15, 310. [Google Scholar] [CrossRef]
- Brown, S.B.; Brown, E.A.; Walker, I. The present and future role of photodynamic therapy in cancer treatment. Lancet Oncol. 2004, 5, 497–508. [Google Scholar] [CrossRef]
- Kobayashi, H.; Watanabe, R.; Choyke, P.L. Improving conventional enhanced permeability and retention (EPR) effects; what is the appropriate target? Theranostics 2014, 4, 81. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Yang, Q.; Shi, K.; Xiao, Y.; Wei, X.; Qian, Z. Intratumoral fate of functional nanoparticles in response to microenvironment factor: Implications on cancer diagnosis and therapy. Adv. Drug Deliv. Rev. 2019, 143, 37–67. [Google Scholar] [CrossRef]
- Gong, H.; Chao, Y.; Xiang, J.; Han, X.; Song, G.; Feng, L.; Liu, J.; Yang, G.; Chen, Q.; Liu, Z. Hyaluronidase to enhance nanoparticle-based photodynamic tumor therapy. Nano Lett. 2016, 16, 2512–2521. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-N.; Bu, W.; Shi, J. Chemical design and synthesis of functionalized probes for imaging and treating tumor hypoxia. Chem. Rev. 2017, 117, 6160–6224. [Google Scholar] [CrossRef] [PubMed]
- Alsaab, H.O.; Alghamdi, M.S.; Alotaibi, A.S.; Alzhrani, R.; Alwuthaynani, F.; Althobaiti, Y.S.; Almalki, A.H.; Sau, S.; Iyer, A.K. Progress in Clinical Trials of Photodynamic Therapy for Solid Tumors and the Role of Nanomedicine. Cancers 2020, 12, 2793. [Google Scholar] [CrossRef]
- Lambert, E.; Gorantla, V.S.; Janjic, J.M. Pharmaceutical design and development of perfluorocarbon nanocolloids for oxygen delivery in regenerative medicine. Nanomedicine 2019, 14, 2697–2712. [Google Scholar] [CrossRef]
- Riess, J.G. Oxygen carriers (“blood substitutes”) raison d’être, chemistry, and some physiology blut ist ein ganz besondrer saft. Chem. Rev. 2001, 101, 2797–2920. [Google Scholar] [CrossRef]
- Cheng, Y.; Cheng, H.; Jiang, C.; Qiu, X.; Wang, K.; Huan, W.; Yuan, A.; Wu, J.; Hu, Y. Perfluorocarbon nanoparticles enhance reactive oxygen levels and tumour growth inhibition in photodynamic therapy. Nat. Commun. 2015, 6, 1–8. [Google Scholar] [CrossRef]
- Backer, M.V.; Backer, J.M. Imaging key biomarkers of tumor angiogenesis. Theranostics 2012, 2, 502. [Google Scholar] [CrossRef]
- O’Connor, J.P.; Aboagye, E.O.; Adams, J.E.; Aerts, H.J.; Barrington, S.F.; Beer, A.J.; Boellaard, R.; Bohndiek, S.E.; Brady, M.; Brown, G. Imaging biomarker roadmap for cancer studies. Nat. Rev. Clin. Oncol. 2017, 14, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Provenzale, J.M. Imaging of angiogenesis: Clinical techniques and novel imaging methods. Am. J. Roentgenol. 2007, 188, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.; Mills, S.; Coope, D.; O’connor, J.; Jackson, A. Imaging biomarkers of angiogenesis and the microvascular environment in cerebral tumours. Br. J. Radiol. 2011, 84, S127–S144. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Niu, G.; Wu, H.; Chen, X. Clinical application of radiolabeled RGD peptides for PET imaging of integrin αvβ3. Theranostics 2016, 6, 78. [Google Scholar] [CrossRef]
- Feng, G.-K.; Ye, J.-C.; Zhang, W.-G.; Mei, Y.; Zhou, C.; Xiao, Y.-T.; Li, X.-L.; Fan, W.; Wang, F.; Zeng, M.-S. Integrin α6 targeted positron emission tomography imaging of hepatocellular carcinoma in mouse models. J. Control. Release 2019, 310, 11–21. [Google Scholar] [CrossRef]
- Huang, C.-W.; Hsieh, W.-C.; Hsu, S.-T.; Lin, Y.-W.; Chung, Y.-H.; Chang, W.-C.; Chiu, H.; Lin, Y.H.; Wu, C.-P.; Yen, T.-C. The use of PET imaging for prognostic integrin α2β1 phenotyping to detect non-small cell lung cancer and monitor drug resistance responses. Theranostics 2017, 7, 4013. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Liang, N.; Wang, M.; Meng, Y.; Jia, B.; Shi, X.; Li, S.; Luo, J.; Luo, Y.; Cui, Q. Integrin Imaging with 99mTc-3PRGD2 SPECT/CT Shows High Specificity in the Diagnosis of Lymph Node Metastasis from Non–Small Cell Lung Cancer. Radiology 2016, 281, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Yan, C.; Zhu, R.; Wang, J.; Wang, Y.; Wang, Y.; Wang, R.; Feng, F.; Ma, W. Imaging biomarkers guided anti-angiogenic therapy for malignant gliomas. Neuroimage Clin. 2018, 20, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Alzhrani, R.M.; Alhadidi, Q.; Bachu, R.D.; Shah, Z.; Dey, S.; Boddu, S.H. Tanshinone IIA inhibits VEGF secretion and HIF-1α expression in cultured human retinal pigment epithelial cells under hypoxia. Curr. Eye Res. 2017, 42, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N. VEGF as a therapeutic target in cancer. Oncology 2005, 69, 11–16. [Google Scholar] [CrossRef]
- Ferrario, A.; von Tiehl, K.F.; Rucker, N.; Schwarz, M.A.; Gill, P.S.; Gomer, C.J. Antiangiogenic treatment enhances photodynamic therapy responsiveness in a mouse mammary carcinoma. Cancer Res. 2000, 60, 4066–4069. [Google Scholar] [PubMed]
- Min, H.; Wang, J.; Qi, Y.; Zhang, Y.; Han, X.; Xu, Y.; Xu, J.; Li, Y.; Chen, L.; Cheng, K. Biomimetic metal–organic framework nanoparticles for cooperative combination of antiangiogenesis and photodynamic therapy for enhanced efficacy. Adv. Mater. 2019, 31, 1808200. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.-L.; Lin, H.-C.; Chiang, W.-L.; Shih, Y.-H.; Chiang, P.-F.; Luo, T.-Y.; Cheng, C.-C.; Shieh, M.-J. Anti-angiogenic treatment (Bevacizumab) improves the responsiveness of photodynamic therapy in colorectal cancer. Photodiagn. Photodyn. Ther. 2018, 23, 111–118. [Google Scholar] [CrossRef]
- Quesada, A.R.; Muñoz-Chápuli, R.; Medina, M.A. Anti-angiogenic drugs: From bench to clinical trials. Med. Res. Rev. 2006, 26, 483–530. [Google Scholar] [CrossRef]
- Lee, W.S.; Yang, H.; Chon, H.J.; Kim, C. Combination of anti-angiogenic therapy and immune checkpoint blockade normalizes vascular-immune crosstalk to potentiate cancer immunity. Exp. Mol. Med. 2020, 52, 1475–1485. [Google Scholar] [CrossRef]
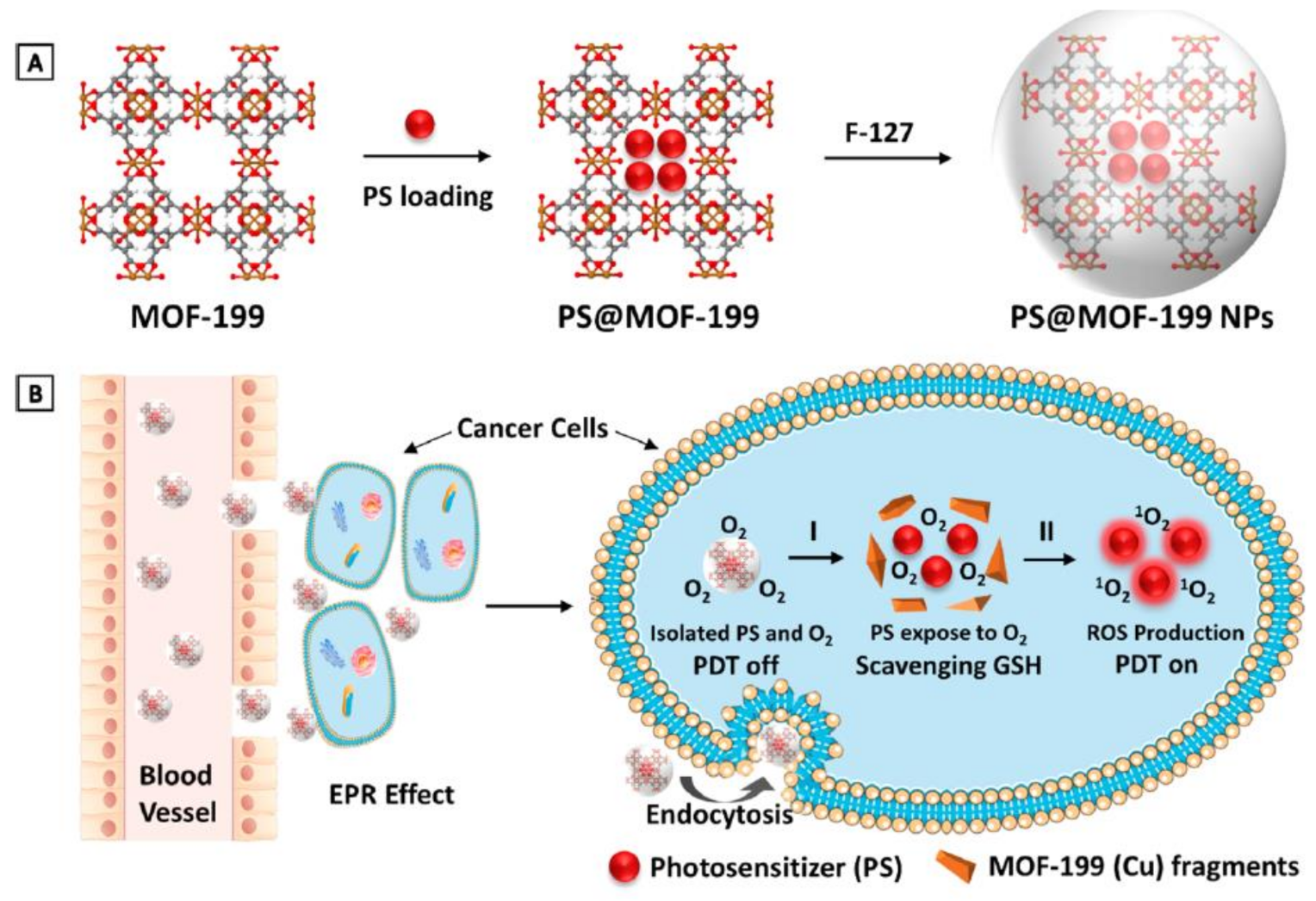
- Wang, Y.; Wu, W.; Liu, J.; Manghnani, P.N.; Hu, F.; Ma, D.; Teh, C.; Wang, B.; Liu, B. Cancer-Cell-Activated Photodynamic Therapy Assisted by Cu (II)-Based Metal–Organic Framework. ACS Nano 2019, 13, 6879–6890. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Liu, L.; Liang, R.; Luo, Z.; He, H.; Wu, Z.; Tian, H.; Zheng, M.; Ma, Y.; Cai, L. Bioinspired hybrid protein oxygen nanocarrier amplified photodynamic therapy for eliciting anti-tumor immunity and abscopal effect. ACS Nano 2018, 12, 8633–8645. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Dominguez, L.; Brandan, M. Quantification of tumor angiogenesis with contrast-enhanced X-ray imaging in preclinical studies: A review. Biomed. Phys. Eng. Express 2018, 4, 062001. [Google Scholar] [CrossRef]
- Mukherjee, S.; Patra, C.R. Therapeutic application of anti-angiogenic nanomaterials in cancers. Nanoscale 2016, 8, 12444–12470. [Google Scholar] [CrossRef]
- Alsaab, H.O.; Alzhrani, R.; Almalki, A.H.; Althobaiti, Y.S.; Sau, S.; Iyer, A.K. Imaging tools to enhance animal tumor models for cancer research and drug discovery. In Animal Models in Cancer Drug Discovery; Elsevier: Amsterdam, The Netherlands, 2019; pp. 75–106. [Google Scholar]
- Andreou, C.; Pal, S.; Rotter, L.; Yang, J.; Kircher, M.F. Molecular imaging in nanotechnology and theranostics. Mol. Imaging Biol. 2017, 19, 363–372. [Google Scholar] [CrossRef]
- Zhou, Z.; Lu, Z.-R. Molecular imaging of the tumor microenvironment. Adv. Drug Deliv. Rev. 2017, 113, 24–48. [Google Scholar] [CrossRef]
- Lin, G.; Lai, C.-H.; Yen, T.-C. Emerging molecular imaging techniques in gynecologic oncology. Pet Clin. 2018, 13, 289–299. [Google Scholar] [CrossRef]
- Cheheltani, R.; Ezzibdeh, R.M.; Chhour, P.; Pulaparthi, K.; Kim, J.; Jurcova, M.; Hsu, J.C.; Blundell, C.; Litt, H.I.; Ferrari, V.A. Tunable, biodegradable gold nanoparticles as contrast agents for computed tomography and photoacoustic imaging. Biomaterials 2016, 102, 87–97. [Google Scholar] [CrossRef]
- Agemy, L.; Friedmann-Morvinski, D.; Kotamraju, V.R.; Roth, L.; Sugahara, K.N.; Girard, O.M.; Mattrey, R.F.; Verma, I.M.; Ruoslahti, E. Targeted nanoparticle enhanced proapoptotic peptide as potential therapy for glioblastoma. Proc. Natl. Acad. Sci. USA 2011, 108, 17450–17455. [Google Scholar] [CrossRef]
- Pan, F.; Yang, W.; Li, W.; Yang, X.-Y.; Liu, S.; Li, X.; Zhao, X.; Ding, H.; Qin, L.; Pan, Y. Conjugation of gold nanoparticles and recombinant human endostatin modulates vascular normalization via interruption of anterior gradient 2–mediated angiogenesis. Tumor Biol. 2017, 39, 1010428317708547. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, R.; Goel, S.; Hong, H.; Chen, F.; Valdovinos, H.F.; Hernandez, R.; Barnhart, T.E.; Cai, W. Hollow mesoporous silica nanoparticles for tumor vasculature targeting and PET image-guided drug delivery. Nanomedicine 2015, 10, 1233–1246. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Yang, J.; Di Jia, M.A.M.; Auguste, D.T. ICAM-1-targeted, Lcn2 siRNA-encapsulating liposomes are potent anti-angiogenic agents for triple negative breast cancer. Theranostics 2016, 6, 1. [Google Scholar] [CrossRef]
- Das, S.; Roy, A.; Barui, A.K.; Alabbasi, M.M.A.; Kuncha, M.; Sistla, R.; Sreedhar, B.; Patra, C.R. Anti-angiogenic vanadium pentoxide nanoparticles for the treatment of melanoma and their in vivo toxicity study. Nanoscale 2020, 12, 7604–7621. [Google Scholar] [CrossRef] [PubMed]
- Gu, G.; Hu, Q.; Feng, X.; Gao, X.; Menglin, J.; Kang, T.; Jiang, D.; Song, Q.; Chen, H.; Chen, J. PEG-PLA nanoparticles modified with APTEDB peptide for enhanced anti-angiogenic and anti-glioma therapy. Biomaterials 2014, 35, 8215–8226. [Google Scholar] [CrossRef]
- Song, H.; Wang, W.; Zhao, P.; Qi, Z.; Zhao, S. Cuprous oxide nanoparticles inhibit angiogenesis via down regulation of VEGFR2 expression. Nanoscale 2014, 6, 3206–3216. [Google Scholar] [CrossRef] [PubMed]
- Giri, S.; Karakoti, A.; Graham, R.P.; Maguire, J.L.; Reilly, C.M.; Seal, S.; Rattan, R.; Shridhar, V. Nanoceria: A rare-earth nanoparticle as a novel anti-angiogenic therapeutic agent in ovarian cancer. PLoS ONE 2013, 8, e54578. [Google Scholar] [CrossRef]
- Cheriyan, V.T.; Alsaab, H.O.; Sekhar, S.; Stieber, C.; Kesharwani, P.; Sau, S.; Muthu, M.; Polin, L.A.; Levi, E.; Iyer, A.K. A CARP-1 functional mimetic loaded vitamin E-TPGS micellar nano-formulation for inhibition of renal cell carcinoma. Oncotarget 2017, 8, 104928. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Yao, Q.; Cao, F.; Liu, Q.; Liu, B.; Wang, X.-H. Silver nanoparticles inhibit the function of hypoxia-inducible factor-1 and target genes: Insight into the cytotoxicity and antiangiogenesis. Int. J. Nanomed. 2016, 11, 6679. [Google Scholar] [CrossRef] [PubMed]
- Divya, M.; Vaseeharan, B.; Abinaya, M.; Vijayakumar, S.; Govindarajan, M.; Alharbi, N.S.; Kadaikunnan, S.; Khaled, J.M.; Benelli, G. Biopolymer gelatin-coated zinc oxide nanoparticles showed high antibacterial, antibiofilm and anti-angiogenic activity. J. Photochem. Photobiol. B Biol. 2018, 178, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Huo, D.; He, J.; Li, H.; Huang, A.J.; Zhao, H.Y.; Ding, Y.; Zhou, Z.Y.; Hu, Y. X-ray CT guided fault-free photothermal ablation of metastatic lymph nodes with ultrafine HER-2 targeting W18O49 nanoparticles. Biomaterials 2014, 35, 9155–9166. [Google Scholar] [CrossRef]
- Du, F.; Lou, J.; Jiang, R.; Fang, Z.; Zhao, X.; Niu, Y.; Zou, S.; Zhang, M.; Gong, A.; Wu, C. Hyaluronic acid-functionalized bismuth oxide nanoparticles for computed tomography imaging-guided radiotherapy of tumor. Int. J. Nanomed. 2017, 12, 5973. [Google Scholar] [CrossRef] [PubMed]
- Krug, P.; Mielczarek, L.; Wiktorska, K.; Kaczyńska, K.; Wojciechowski, P.; Andrzejewski, K.; Ofiara, K.; Szterk, A.; Mazur, M. Sulforaphane-conjugated selenium nanoparticles: Towards a synergistic anticancer effect. Nanotechnology 2018, 30, 065101. [Google Scholar] [CrossRef]
- Grodzik, M.; Sawosz, E.; Wierzbicki, M.; Orlowski, P.; Hotowy, A.; Niemiec, T.; Szmidt, M.; Mitura, K.; Chwalibog, A. Nanoparticles of carbon allotropes inhibit glioblastoma multiforme angiogenesis in ovo. Int. J. Nanomed. 2011, 6, 3041. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trials Number | Intervention (Drug) | Cancer Type | Title of Study |
|---|---|---|---|
| NCT01525550 | Sunitinib | Well-differentiated Pancreatic Neuroendocrine Tumor | A Study of The Efficacy and Safety of Sunitinib In Patients with Advanced Well-Differentiated Pancreatic Neuroendocrine Tumors |
| NCT02582970 | 5-Fluorouracil Bevacizumab Irinotecan Oxaliplatin | Colorectal Cancer | A Study of Bevacizumab (Avastin) in Combination with Chemotherapy in Participants with Metastatic Cancer of the Colon or Rectum |
| NCT00121836 | Capecitabine Bevacizumab | Breast Cancer | A Study of Xeloda (Capecitabine) in Women with HER2-Negative Metastatic Breast Cancer |
| NCT02248571 | Bevacizumab Capecitabine Everolimus Exemestane Other: Patient questionnaires | Breast Cancer Recurrent | Patient Preference for Everolimus in Combination with Exemestane or Capecitabine in Combination with Bevacizumab (IMPROVE) |
| NCT01094184 | Bevacizumab Paclitaxel Docetaxel | Breast Cancer | A Study of Bevacizumab with Taxane Therapy in Participants with Triple-Negative Breast Cancer |
| NCT01695772 | 5-FU based doublet chemotherapy Bevacizumab | Colorectal Cancer | A Study of Bevacizumab Plus 5-Flurouracil (5-FU) Based Doublet Chemotherapy as Neoadjuvant Therapy for Participants with Previously Untreated Unresectable Liver-Only Metastases from Colorectal Cancer |
| NCT00577031 | Bevacizumab (Avastin) Oxaliplatin Xeloda | Colorectal Cancer | OBELIX Study: A Study of Avastin (Bevacizumab) in Combination With XELOX in Patients With Metastatic Cancer of the Colon or Rectum. |
| NCT00451906 | Platinum-based chemotherapy Bevacizumab (Avastin) | Non-Squamous Non-Small Cell Lung Cancer | A Study of Avastin (Bevacizumab) in Combination with Platinum-Containing Chemotherapy in Patients with Advanced or Recurrent Non-Squamous Cell Lung Cancer |
| NCT01588990 | Oxaliplatin Capecitabine Bevacizumab Leucovorin 5-Fluouracil Drug: Irinotecan | Colorectal Neoplasms | A Translational Study of Bevacizumab in Participants with Metastatic Colorectal Cancer |
| NCT00793871 | Sunitinib Malate (SU011248) | Gastrointestinal Neoplasms, Gastrointestinal Stromal Tumors | Safety and Efficacy Study of Sunitinib Malate In Chinese Patients With Imatinib-Resistant Or -Intolerant Malignant Gastrointestinal Stromal Tumor |
| NCT02460380 | Vitamin D3 Other: Placebo | Polycystic Ovary Syndrome Vitamin D Deficiency | The Effects of Vitamin D on Angiogenic Factors in Women with Polycystic Ovary Syndrome |
| NCT01206764 | Everolimus | Renal Cell Carcinoma | A Trial of Everolimus in Patients with Advanced Renal Cell Carcinoma. |
| NCT01731886 | Procedure: autologous peripheral blood stem cell transplant Lenalidomide Dexamethasone Procedure: stem cell collection Melphalan G-CSF Cyclophosphamide Mesna | Multiple Myeloma | Lenalidomide and Dexamethasone With/Without Stem Cell Transplant in Patients with Multiple Myeloma |
| NCT02953938 | Biological: Ranibizumab Radiation: grid and direct short pulse laser photocoagulation | Macular Edema Secondary to Branch Retinal Vein Occlusion (BRVO) | Study to Show a Superior Benefit in Terms of Reduction of Ranibizumab Injections in Patients Receiving Ranibizumab Plus Laser Photocoagulation Combination Therapy Without Loss of Efficacy and Safety |
| NCT00706706 | Sunitinib Malate (SU011248) | Carcinoma, Renal Cell | Safety and Efficacy Study of Sunitinib Malate as First-Line Systemic Therapy In Chinese Patients With Metastatic Renal Cell Carcinoma |
| NCT00022516 | Cyclophosphamide Methotrexate | Breast Cancer | Low-dose Oral Cyclophosphamide and Methotrexate Maintenance for Hormone Receptor-Negative Early Breast Cancer |
| NCT00094055 | AG013736 | Thyroid Neoplasms | Study of the Antiangiogenesis Agent AG-013736 in Patients with Metastatic Thyroid Cancer |
| NCT01105533 | PF-00337210 | Neoplasm | A Dose-Finding Study of a New Medication, PF-00337210, That Will Possibly Decrease Blood Supply to Tumors |
| NCT00140556 | Radiation: Chemoradiotherapy Cisplatin Bevacizumab Erlotinib | Head and Neck Cancer Pharynx Cancer | Angiogenic and EGFR Blockade with Curative Chemoradiation for Advanced Head and Neck Cancer |
| Nanoparticle Types | Targeting Ligand | Targeted Tumor | Therapeutic/Diagnostic or Both | Imaging Technique Used | Results | References |
|---|---|---|---|---|---|---|
| Iron oxide nanoparticles | A tumor-penetrating peptide, iRGD | Glioblastoma (GBM) | Both | MRI | 1- The iron oxide component of the nanoparticles enabled imaging of GBM tumors in mice. 2- Systemic treatment of nanoparticular-bearing GBM mice eradicated most tumors in a GBM animal model and slightly slowed the growth of tumors in another model. 3- The combination of nanoparticles with a tumor-penetrating peptide increased therapeutic efficacy further. | [122] |
| Gold nanoparticles (AuNPs) | Recombinant human endostatin (rhES) | Metastatic colorectal cancer (mCRC) | Therapeutic | ____ | 1- AuNPs normalized vasculature by promoting vessel stability, indicated by increasing pericyte expression and reducing VEGFR2 in mCRC xenografts. 2- rhES-AuNPs interrupted AGR2-induced vascular formation in HUVECs. These findings suggest that rhES-AuNPs might normalize vessels by interfering with AGR2-mediated angiogenesis in mCRC. | [123] |
| Hollow mesoporous silica nanoparticles (HMSN NPs) | Macrocyclic chelator, NOTA, PEGylated, and nanoconjugate were attached with (cRGDyK) and radiolabeled with 64Cu for PET imaging. | Glioblastoma | Both | positron emission tomography “PET” | 1- Progressing synthesized HMSN-based nanoconjugates that can be used not only to image PET integrin αvβ3 but also for the supply of chemical-therapeutic drugs to carcinogenic lesions for tumor vasculature. 2- Tumor-targeting ability of cRGDyK-conjugated nanoconstructs was significantly enhanced in integrin αvβ3-overexpressing U87MG tumor models by integrin αvβ3-mediated active targeting as well as the EPR effect. 3- In U87MG tumor-bearing mice, a model hydrophobilic anti-carcinogenic (SUN) drug was loaded on high-capability (>400 mg/g) HMSNs, which improved in vivo delivery. | [124] |
| Liposomal nanoparticles (ICAM-Lcn2-LPs NPs) | Intercellular adhesion molecule-1 (ICAM-1) antibodies, Lcn2 siRNA- encapsulating liposome (ICAM-Lcn2-LP) | Triple-negative breast cancer (TNBC) | Both | ____ | 1- Synthesized ICAM-1-targeted Lcn2 siRNA-encapsulating liposomes significantly suppress in vitro and in vivo angiogenic activities of TNBC cells. 2- Liposomal nanocarriers have both imaging tools and medicinal molecules on a scalable basis. 3- Two kinds of human endothelial cells were used to observe the antiangiogenic properties of ICAM-Lcn2-LP, as seen in reductions in the development and migration of TNBC-mediated endothelial cells (HMVECs and HUVECs). | [125] |
| Vanadium pentoxide nanoparticles (V2O5 NPs) | Ethylene glycol | Melanoma | Therapeutic | ____ | 1- The use of V2O5 NPs with C57BL6/J mice dramatically improved their survival relative to untreated mouse controls, demonstrating the therapeutic ability of nanoparticles against melanoma. 2- V2O5 NPs impaired and inhibited blood vasculature differentiation and movement of endothelial cells (HUVECs and EA.hy926) in chick embryos, demonstrating antiangiogenic properties. 3- There was no toxic activity in mice at subchronic exposure to V2O5 NPs with in-vivo toxicity analysis. | [126] |
| PEG-PLA nanoparticles NPs | APTEDB | Glioma | Therapeutic | ____ | 1- PTX-loaded APT-NPs indicated satisfactory encapsulated efficiency, loading capacity, and size distribution. 2- In both subcutaneous and intracranial xenograft models, APT-NP-PTX demonstrated increased antiglioma potency over unmodified nanoparticles and Taxol®. 3- APT-NPs achieved much higher and precise aggregation within glioma after IV administration, as both in-vivo animal imaging and tissue dissemination analyses have shown. | [127] |
| Cuprous oxide nanoparticles (CO-NPs) | Nontargeted ligand | ____ | Therapeutic | ____ | 1- CO-NPs are able to cause improvements in cell morphology and in vitro or in vivo doses to prevent cell proliferation, migration, and tube forming. 2- CO-NPs have been shown to inhibit dosage and time of expression based on protein and mRNA levels, but they have little impact on the expression of VEGF or VEGFR1. | [128] |
| Cerium oxide “Nanoceria” nanoparticles (NCe NPs) | Nontargeted ligand | Ovarian cancer | Therapeutic | ____ | 1- Nanocerides (NCes) were crafted from cerium oxide NPs with antioxidant properties for use as a therapeutic agent in ovarian cancer. 2- NCes blocked mediated VEGF165 in human endothelial umbilical vascular cells, capillary tube development, activation of VEGFR2, and MMP 2 (HUVEC). 3- Reduction in tumor mass, as noted by a decreased CD31 stain and specific apoptosis of vascular endothelial cells, followed by a mitigation of angiogenesis. | [129] |
| Vitamin E “TPGS” micellar nanoparticles | Styrene-maleic acid (SMA) | Renal cell carcinoma | Therapeutic | ____ | 1- CFM-4.1 encapsulated in TPGS-based vitamin E nanomicelles, leading to a higher loading CFM-4.16 and water-soluble formulation (30% w/w). 2- The formula of CFM-4.16 prevented the in-vitro and suppressed development of parental A498 RCC cell xenografts by inducing apoptosis of parent RCC cells in vitro and everolimus-resistant cells. | [130] |
| Silver nanoparticles (Ag NPs) | Nontargeted ligand | Breast cancer cell line MCF7 | Therapeutic | ____ | 1- Ag NPs are inhibited by HIF-1α and its aggregation of proteins and downstream target expression in MCF7 cell development. 2- Ag NPs work to suppress the action of HIF-1α in cells under hypoxic conditions, leading to VEGF-A and GLUT1 downregulation and inhibition of angiogenesis. | [131] |
| Zinc oxide nanoparticles (ZnO NPs) | Gelatin biopolymers | Liver cancer cell line (HePG2) | Therapeutic | ____ | 1- Ge-ZnO NPs inhibited the viability of HepG2 cell lines; in addition, Ge-ZnO NPs and zinc acetate showed antiangiogenesis activity in chick embryos. 2- The findings for the CAM test showed that in chick embryos, antiangiogenesis was higher than in biopolymer gelatine for Ge ZnO NPs and zinc acetate. 3- HepG2 cells treated with 100 µg/mL Ge-ZnO NPs showed ruptures and a consequent loss of membrane integrity. | [132] |
| W18O49 nanoparticles | anti-HER-2 monoclonal antibody | Breast cancer | Both | CT | 1- In vivo research verified that WOHA NPs could precisely mark metastatic HER-2 lymph nodes and exclude laser irradiation from cancer cells. 2- WOHA NP-made PTT could prolong the survival rate of breast-bearing mice by inhibition of cancer cell metastases in animals 3- In mice with HER-2 positive metastases, a simple distinction can be made between lymph nodes under CT guidance; laser ablation can selectively remove them. | [133] |
| Bismuth-based nanoparticles (Bi2S3 NPs) | Hyaluronic acid (HA) | Solid tumors | Both | CT | 1- Not only was the intrinsic radioactivity in cancer cells enhanced in HA-Bi2O3 NPs encapsulated with Bi atoms through absorption of high-energy photons and the emission of secondary electrons and Auger electrons, but it also had high ray attenuation coefficients in favor of CT-imaging-guided radiotherapy, which had a substantial increase in radioactivity. 2- HA-Bi2O3 NPs were especially suited to the overexpression of CD44 receptors, possessing favorable water solubility and excellent biocompatibility. | [134] |
| Selenium nanoparticles (Se NPs) | Sulforaphane | Breast, colon, prostate cancers | Therapeutic | ____ | 1- The cell growth inhibitory effect between SFN and SeNPs was highly synergistic in all cancer cell lines. 2- Important high selectivity has been observed between cancer and normal cells. Cytotoxicity is several times smaller in human cells than in cancers. | [135] |
| Carbon allotrope nanoparticles: Ultra-dispersed detonation diamond (UDD) and microwave-radiofrequency (MW-RF) carbon allotrope | Nontargeted ligand | Glioblastoma | Therapeutic | ____ | 1- Nanoparticles of UDD and MW-RF decrease tumor mass and volume and block the production of new blood vessels in in-vivo GBM tumors. 2- UDD NP was found to decrease the expression of FGF-2 and VEGF substantially, while MW-RF NP decreased the expression of VEGF only. | [136] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsaab, H.O.; Al-Hibs, A.S.; Alzhrani, R.; Alrabighi, K.K.; Alqathama, A.; Alwithenani, A.; Almalki, A.H.; Althobaiti, Y.S. Nanomaterials for Antiangiogenic Therapies for Cancer: A Promising Tool for Personalized Medicine. Int. J. Mol. Sci. 2021, 22, 1631. https://doi.org/10.3390/ijms22041631
Alsaab HO, Al-Hibs AS, Alzhrani R, Alrabighi KK, Alqathama A, Alwithenani A, Almalki AH, Althobaiti YS. Nanomaterials for Antiangiogenic Therapies for Cancer: A Promising Tool for Personalized Medicine. International Journal of Molecular Sciences. 2021; 22(4):1631. https://doi.org/10.3390/ijms22041631
Chicago/Turabian StyleAlsaab, Hashem O., Alanoud S. Al-Hibs, Rami Alzhrani, Khawlah K. Alrabighi, Aljawharah Alqathama, Akram Alwithenani, Atiah H. Almalki, and Yusuf S. Althobaiti. 2021. "Nanomaterials for Antiangiogenic Therapies for Cancer: A Promising Tool for Personalized Medicine" International Journal of Molecular Sciences 22, no. 4: 1631. https://doi.org/10.3390/ijms22041631
APA StyleAlsaab, H. O., Al-Hibs, A. S., Alzhrani, R., Alrabighi, K. K., Alqathama, A., Alwithenani, A., Almalki, A. H., & Althobaiti, Y. S. (2021). Nanomaterials for Antiangiogenic Therapies for Cancer: A Promising Tool for Personalized Medicine. International Journal of Molecular Sciences, 22(4), 1631. https://doi.org/10.3390/ijms22041631