
A Presurgical Study of Curcumin Combined with Anthocyanin Supplements in Patients with Colorectal Adenomatous Polyps


 , ,
, ,
Abstract
:1. Introduction
2. Results
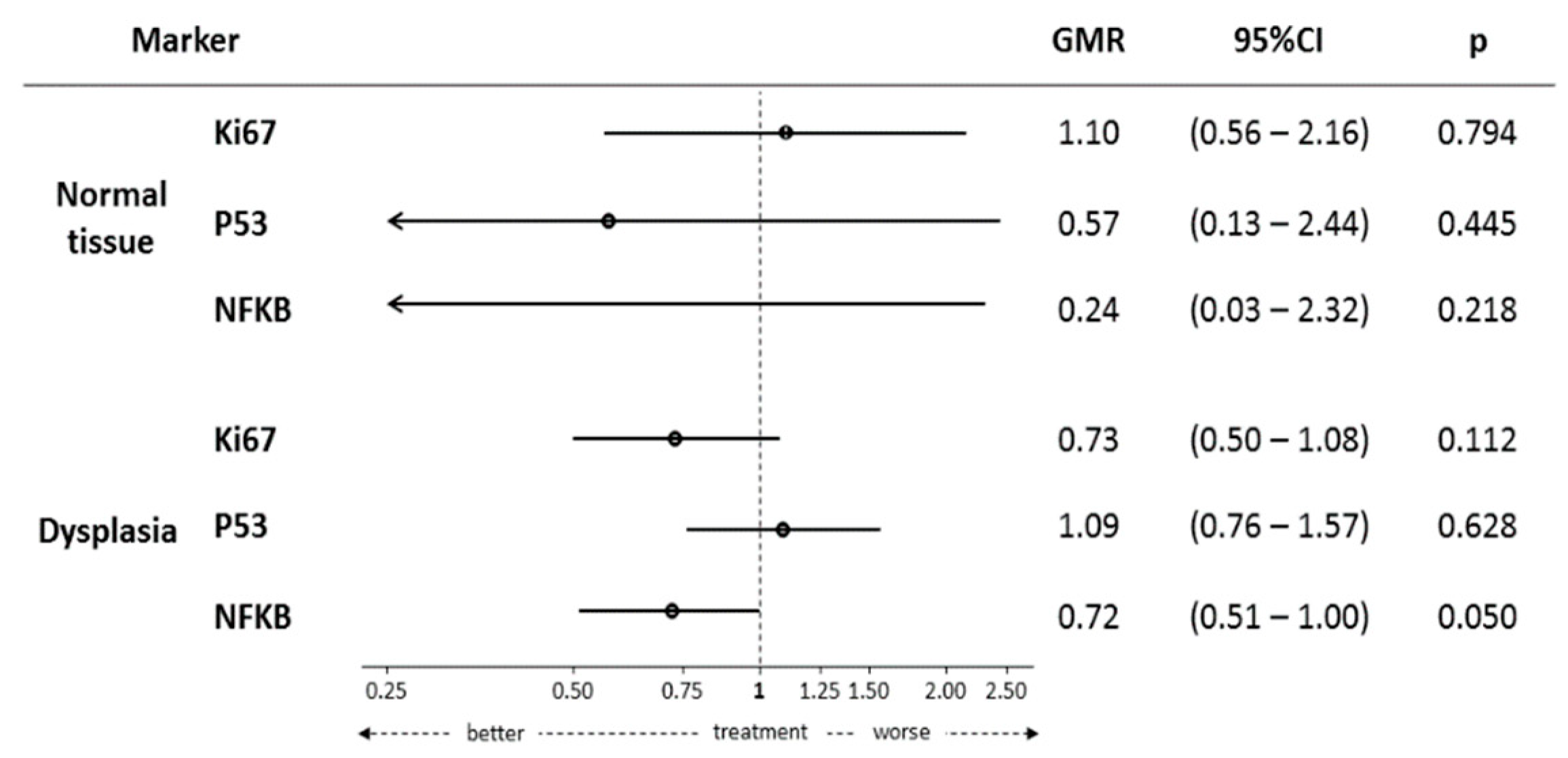
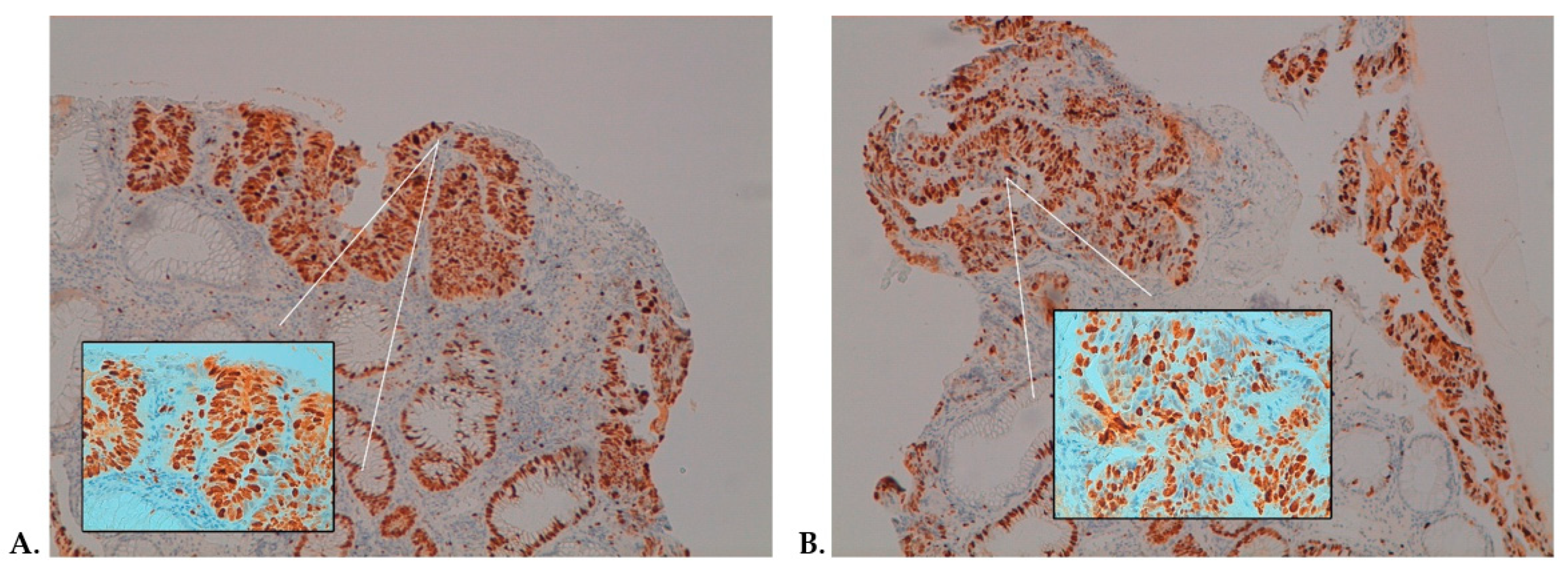
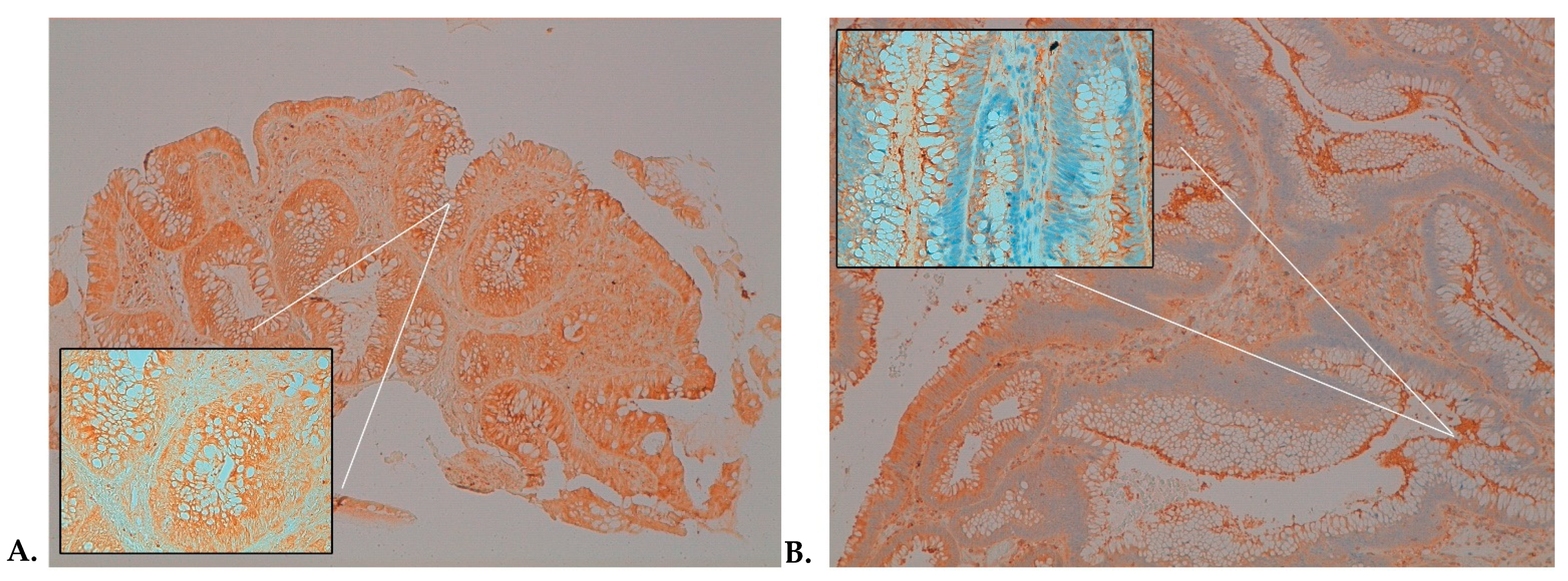
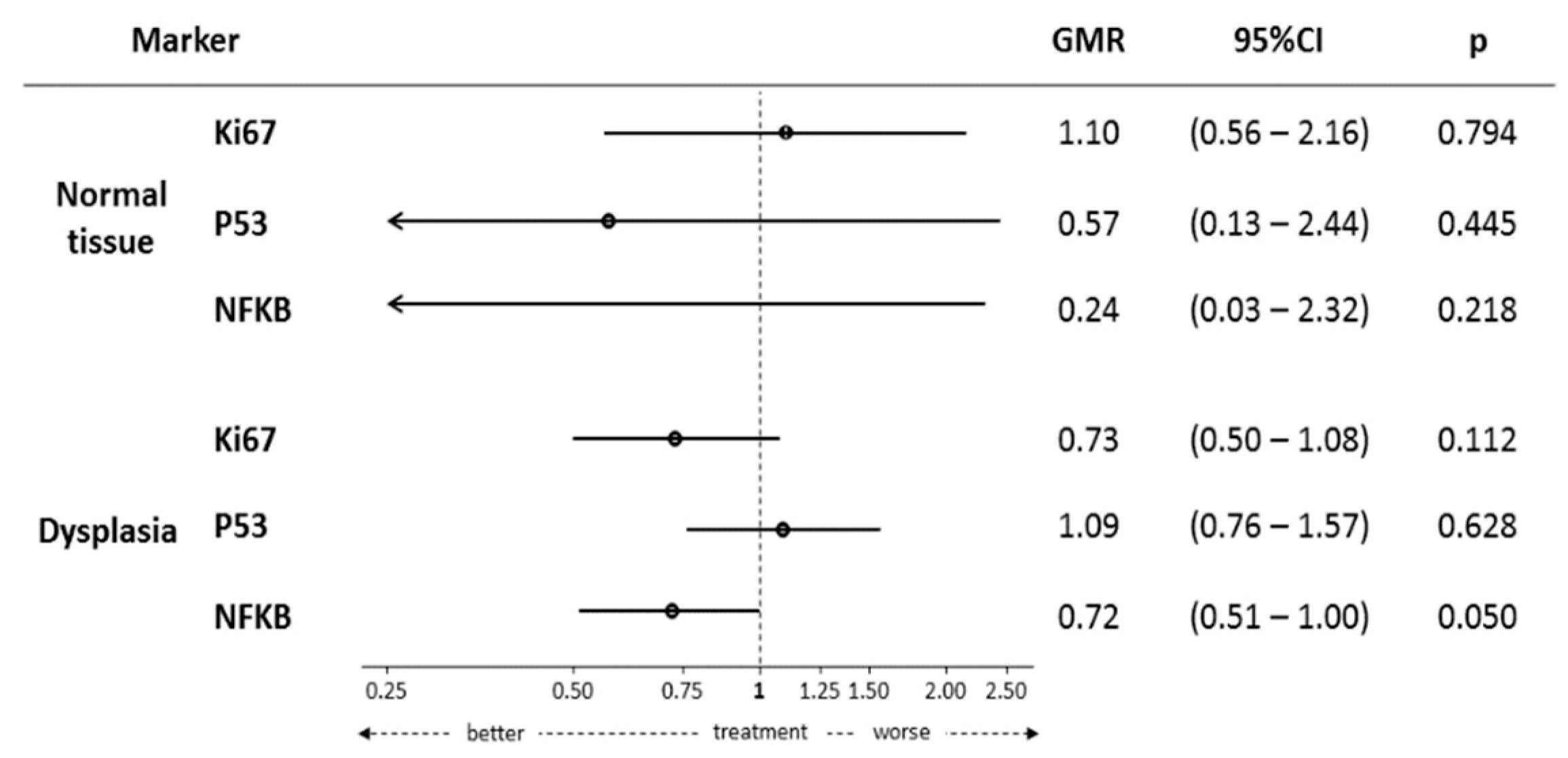
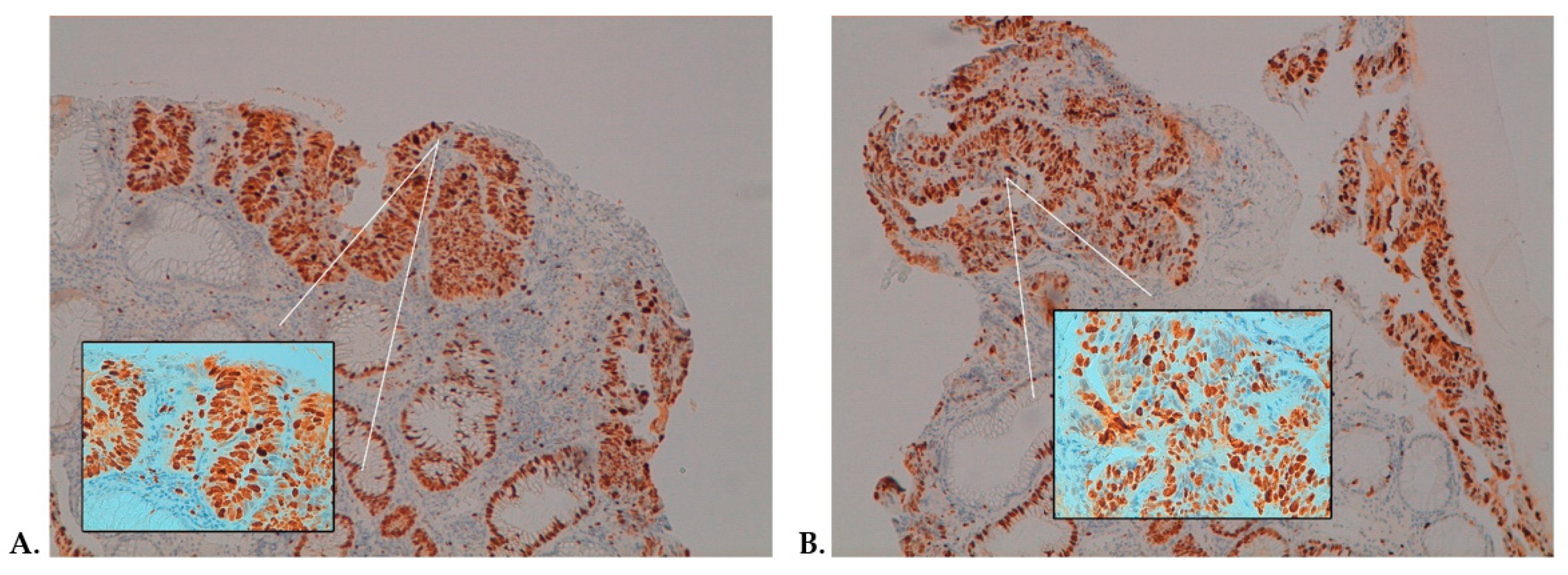
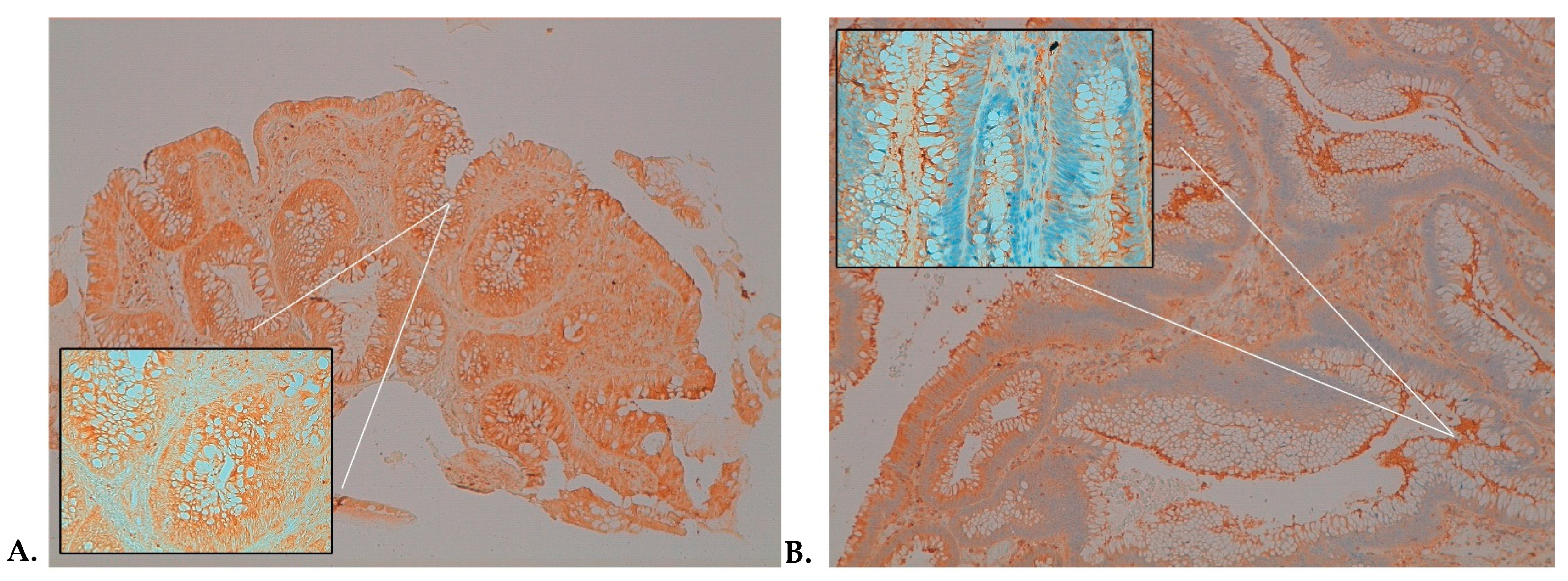
Tissue Biomarker Expression
3. Discussion
4. Materials and Methods
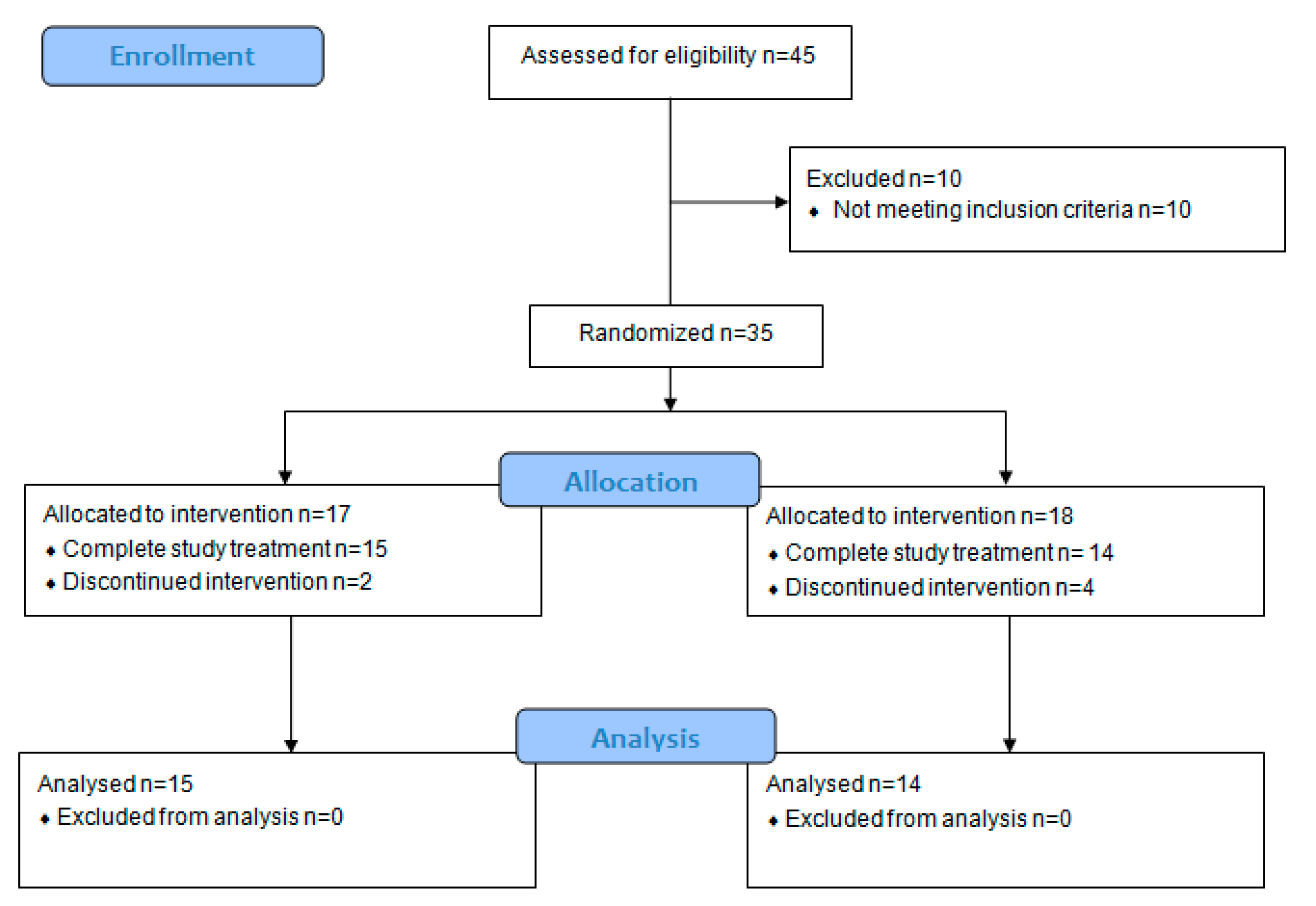
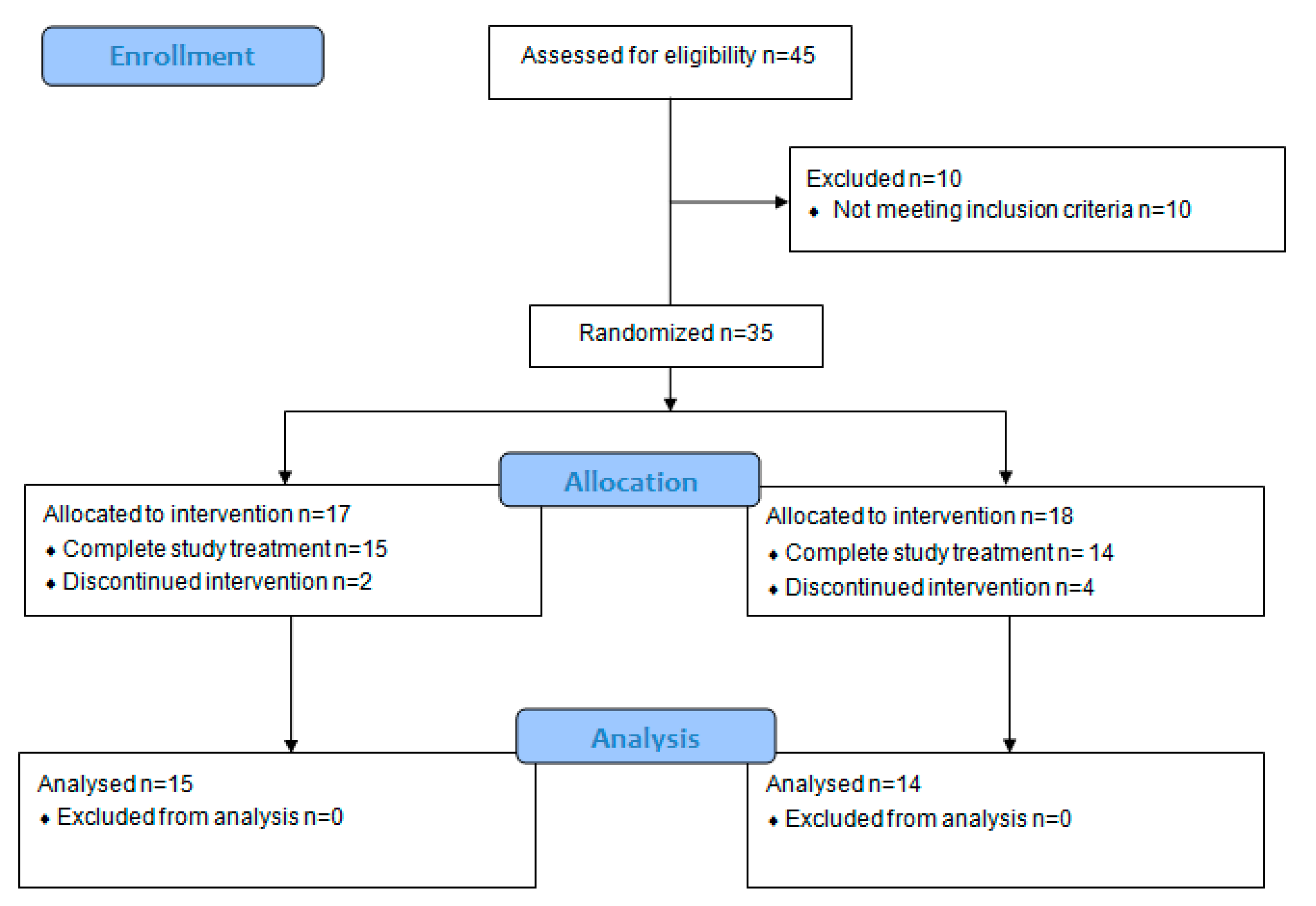
4.1. Study Design and Participants
4.2. Study Procedures
4.3. Dietary Supplements
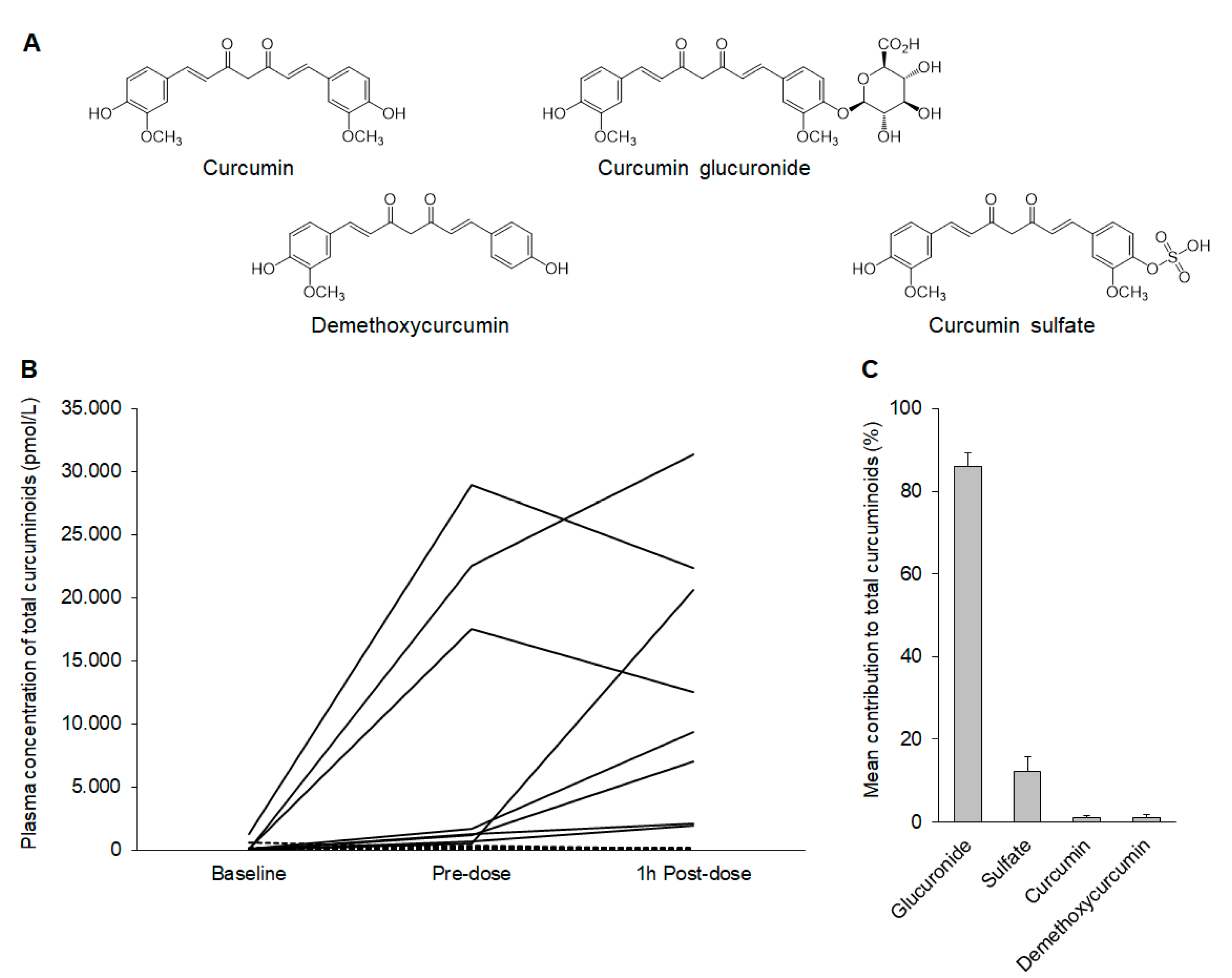
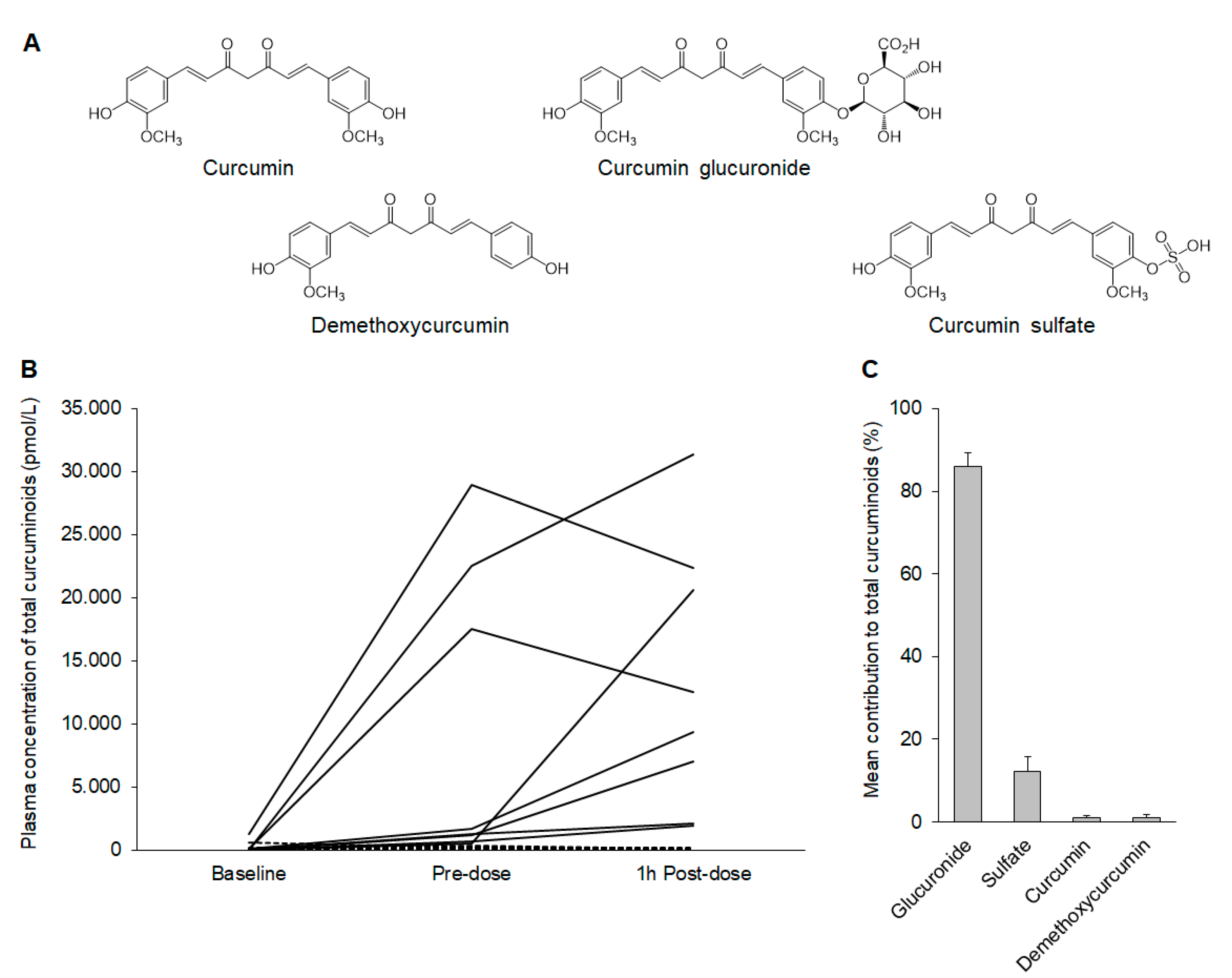
4.4. Liquid Chromatography-Electrospray Ionization (LC-ESI)-MS/MS Analysis and Quantitation of Curcumin and Metabolites
4.5. Tissue Biomarkers Assessment
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of Open Access Journals |
| TLA | three letter acronym |
| LD | linear dichroism |
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef] [PubMed]
- O’Shaughnessy, J.A.; Kelloff, G.J.; Gordon, G.B.; Dannenberg, A.J.; Hong, W.K.; Fabian, C.J.; Sigman, C.C.; Bertagnolli, M.M.; Stratton, S.P.; Lam, S.; et al. Treatment and prevention of intraepithelial neoplasia: An important target for accelerated new agent development. Clin. Cancer Res. 2002, 8, 314–346. [Google Scholar] [PubMed]
- Terzić, J.; Grivennikov, S.; Karin, E.; Karin, M. Inflammation and colon cancer. Gastroenterology 2010, 138, 2101–2114.e5. [Google Scholar] [CrossRef]
- Rothwell, P.M.; Wilson, M.; Elwin, C.E.; Norrving, B.; Algra, A.; Warlow, C.P.; Meade, T.W. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet. 2010, 376, 1741–1750. [Google Scholar] [CrossRef]
- Jakszyn, P.; Cayssials, V.; Buckland, G.; Perez-Cornago, A.; Weiderpass, E.; Boeing, H.; Bergmann, M.M.; Vulcan, A.; Ohlsson, B.; Masala, G.; et al. Inflammatory potential of the diet and risk of colorectal cancer in the European Prospective Investigation into Cancer and Nutrition study. Int. J. Cancer. 2020, 147, 1027–1039. [Google Scholar] [CrossRef]
- Continuous Update Project Report. Food, Nutrition, Physical Activity, and the Prevention of Colorectal Cancer. Available online: http://www.aicr.org/assets/docs/pdf/reports/Second_Expert_Report.pdf (accessed on 8 July 2021).
- Pricci, M.; Girardi, B.; Giorgio, F.; Losurdo, G.; Ierardi, E.; Di Leo, A. Curcumin and Colorectal Cancer: From Basic to Clinical Evidences. Int. J. Mol. Sci. 2020, 21, 2364. [Google Scholar] [CrossRef] [Green Version]
- Howells, L.; Malhotra Mukhtyar, R.; Theofanous, D.; Pepper, C.; Thomas, A.; Brown, K.; Khan, S. A Systematic Review Assessing Clinical Utility of Curcumin with a Focus on Cancer Prevention. Mol. Nutr. Food Res. 2021, 65, e2000977. [Google Scholar] [CrossRef]
- Cuomo, J.; Appendino, G.; Dern, A.S.; Schneider, E.; McKinnon, T.P.; Brown, M.J.; Togni, S.; Dixon, B.M. Comparative absorption of a standardized curcuminoid mixture and its lecithin formulation. J. Nat. Prod. 2011, 74, 664–669. [Google Scholar] [CrossRef]
- Bresciani, L.; Favari, C.; Calani, L.; Francinelli, V.; Riva, A.; Petrangolini, G.; Allegrini, P.; Mena, P.; Del Rio, D. The Effect of Formulation of Curcuminoids on Their Metabolism by Human Colonic Microbiota. Molecules 2020, 25, 940. [Google Scholar] [CrossRef] [Green Version]
- Teng, C.F.; Yu, C.H.; Chang, H.Y.; Hsieh, W.C.; Wu, T.H.; Lin, J.H.; Wu, H.C.; Jeng, L.B.; Su, I.J. Chemopreventive Effect of Phytosomal Curcumin on Hepatitis B Virus-Related Hepatocellular Carcinoma in A Transgenic Mouse Model. Sci. Rep. 2019, 9, 10338. [Google Scholar] [CrossRef] [Green Version]
- Panahi, Y.; Kianpour, P.; Mohtashami, R.; Jafari, R.; Simental-Mendía, L.E.; Sahebkar, A. Efficacy and Safety of Phytosomal Curcumin in Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Drug Res. 2017, 67, 244–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymanski, M.C.; Gillum, T.L.; Gould, L.M.; Morin, D.S.; Kuennen, M.R. Short-term dietary curcumin supplementation reduces gastrointestinal barrier damage and physiological strain responses during exertional heat stress. J. Appl. Physiol. 2018, 124, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Belcaro, G.; Dugall, M.; Peterzan, P.; Hosoi, M.; Ledda, A.; Riva, A.; Giacomelli, L.; Togni, S.; Eggenhoffner, R.; et al. Interaction study between antiplatelet agents, anticoagulants, thyroid replacement therapy and a bioavailable formulation of curcumin (Meriva®). Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5042–5046. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.M.; Almagribi, W.; Al-Rashidi, M.N. Antiradical and reductant activities of anthocyanidins and anthocyanins, structure-activity relationship and synthesis. Food Chem. 2016, 194, 1275–1282. [Google Scholar] [CrossRef]
- Wang, L.S.; Stoner, G.D. Anthocyanins and their role in cancer prevention. Cancer Lett. 2008, 269, 281–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dharmawansa, K.V.S.; Hoskin, D.W.; Rupasinghe, H.P.V. Chemopreventive Effect of Dietary Anthocyanins against Gastrointestinal Cancers: A Review of Recent Advances and Perspectives. Int. J. Mol. Sci. 2020, 21, 6555. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yang, D.Y.; Yang, L.Q.; Zhao, W.Z.; Cai, L.Y.; Shi, H.P. Anthocyanin Consumption and Risk of Colorectal Cancer: A Meta-Analysis of Observational Studies. J. Am. Coll Nutr. 2019, 38, 470–477. [Google Scholar] [CrossRef]
- Riva, A.; Togni, S.; Franceschi, F.; Kawada, S.; Inaba, Y.; Eggenhoffner, R.; Giacomelli, L. The effect of a natural, standardized bilberry extract (Mirtoselect®) in dry eye: A randomized, double blinded, placebo-controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2518–2525. [Google Scholar] [PubMed]
- Hoggard, N.; Cruickshank, M.; Moar, K.M.; Bestwick, C.; Holst, J.J.; Russell, W.; Horgan, G. A single supplement of a standardised bilberry (Vaccinium myrtillus L.) extract (36 % wet weight anthocyanins) modifies glycaemic response in individuals with type 2 diabetes controlled by diet and lifestyle. J. Nutr. Sci. 2013, 2, e22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzolani, F.; Togni, S.; Franceschi, F.; Eggenhoffner, R.; Giacomelli, L. The effect of oral supplementation with standardized bilberry extract (Mirtoselect®) on retino-cortical bioelectrical activity in severe diabetic retinopathy. Minerva Oftalmol. 2017, 59, 38–41. [Google Scholar] [CrossRef]
- Sharma, R.A.; Steward, W.P.; Gescher, A.J. Pharmacokinetics and Pharmacodynamics of Curcumin. In The Molecular Targets and Therapeutic Uses of Curcumin in Health and Disease; Aggarwal, B.B., Surh, Y.J., Shishodia, S., Eds.; Advances in Experimental Medicine and Biology; Springer: Boston, MA, USA, 2007; Volume 595, pp. 453–470. [Google Scholar] [CrossRef] [Green Version]
- Vareed, S.K.; Kakarala, M.; Ruffin, M.T.; Crowell, J.A.; Normolle, D.P.; Djuric, Z.; Brenner, D.E. Pharmacokinetics of curcumin conjugate metabolites in healthy human subjects. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1411–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, F.H.; Li, Y. NF-kappaB: A potential target for cancer chemoprevention and therapy. Front. Biosci. 2008, 13, 2950–2959. [Google Scholar] [CrossRef] [Green Version]
- Rajitha, B.; Belalcazar, A.; Nagaraju, G.P.; Shaib, W.L.; Snyder, J.P.; Shoji, M.; Pattnaik, S.; Alam, A.; El-Rayes, B.F. Inhibition of NF-κB translocation by curcumin analogs induces G0/G1 arrest and downregulates thymidylate synthase in colorectal cancer. Cancer Lett. 2016, 373, 227–233. [Google Scholar] [CrossRef]
- Jobin, C.; Bradham, C.A.; Russo, M.P.; Juma, B.; Narula, A.S.; Brenner, D.A.; Sartor, R.B. Curcumin blocks cytokine-mediated NF-kappa B activation and proinflammatory gene expression by inhibiting inhibitory factor I-kappa B kinase activity. J. Immunol. 1999, 163, 3474–3483. [Google Scholar]
- Thomasset, S.; Berry, D.P.; Cai, H.; West, K.; Marczylo, T.H.; Marsden, D.; Brown, K.; Dennison, A.; Garcea, G.; Miller, A.; et al. Pilot study of oral anthocyanins for colorectal cancer chemoprevention. Cancer Prev. Res. 2009, 2, 625–633. [Google Scholar] [CrossRef] [Green Version]
- Perez-Vizcaino, F.; Duarte, J.; Santos-Buelga, C. The flavonoid paradox: Conjugation and deconjugation as key steps for the biological activity of flavonoids. J. Sci. Food Agric. 2012, 92, 1822–1825. [Google Scholar] [CrossRef]
- Shimoi, K.; Saka, N.; Nozawa, R.; Sato, M.; Amano, I.; Nakayama, T.; Kinae, N. Deglucuronidation of a flavonoid, luteolin monoglucuronide, during inflammation. Drug Metab. Dispos. 2001, 29, 1521–1524. [Google Scholar] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin: Problems and promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef]
- Marczylo, T.H.; Verschoyle, R.D.; Cooke, D.N.; Morazzoni, P.; Steward, W.P.; Gescher, A.J. Comparison of systemic availability of curcumin with that of curcumin formulated with phosphatidylcholine. Cancer Chemother. Pharmacol. 2007, 60, 171–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allegri, P.; Mastromarino, A.; Neri, P. Management of chronic anterior uveitis relapses: Efficacy of oral phospholipidic curcumin treatment. Long-term follow-up. Clin. Ophthalmol. 2010, 4, 1201–1206. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, F.; Feregalli, B.; Togni, S.; Cornelli, U.; Giacomelli, L.; Eggenhoffner, R.; Belcaro, G. A novel phospholipid delivery system of curcumin (Meriva®) preserves muscular mass in healthy aging subjects. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 762–766. [Google Scholar]
- Cai, H.; Thomasset, S.C.; P-Berry, D.; Garcea, G.; Brown, K.; Steward, W.P.; Gescher, A.J. Determination of anthocyanins in the urine of patients with colorectal liver metastases after administration of bilberry extract. Biomed. Chromatogr. 2011, 25, 660–663. [Google Scholar] [CrossRef]
- Carroll, R.E.; Benya, R.V.; Turgeon, D.K.; Vareed, S.; Neuman, M.; Rodriguez, L.; Kakarala, M.; Carpenter, P.M.; McLaren, C.; Meyskens, F.L., Jr.; et al. Phase IIa Clinical Trial of Curcumin for the Prevention of Colorectal Neoplasia. Cancer Prev. Res. 2011, 4, 354–364. [Google Scholar] [CrossRef] [Green Version]
- Mahale, J.; Singh, R.; Howells, L.M.; Britton, R.G.; Khan, S.M.; Brown, K. Detection of Plasma Curcuminoids from Dietary Intake of Turmeric-Containing Food in Human Volunteers. Mol. Nutr. Food Res. 2018, 62, e1800267. [Google Scholar] [CrossRef]
- Irving, G.R.; Howells, L.M.; Sale, S.; Kralj-Hans, I.; Atkin, W.S.; Clark, S.K.; Britton, R.G.; Jones, D.J.; Scott, E.N.; Berry, D.P.; et al. Prolonged biologically active colonic tissue levels of curcumin achieved after oral administration—A clinical pilot study including assessment of patient acceptability. Cancer Prev. Res. 2013, 6, 119–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, A.; Sung, B.; Prasad, B.A.B.; Schuber, P.T., Jr.; Prasad, S.; Aggarwal, B.B.; Bornmann, W.G. Curcumin glucuronides: Assessing the proliferative activity against human cell lines. Bioorg. Med. Chem. 2014, 22, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, S.M.; Raine, L.; Fanger, H. A comparative study of the peroxidase–antiperoxidase method and an avidin–biotin complex method for studying polypeptide hormones with radioimmunoassay antibodies. Am. J. Clin. Pathol. 1981, 75, 734–738. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Treatment | p-Value | ||
|---|---|---|---|---|
| Active | Placebo | |||
| N (%) | 15 (51.7) | 14 (48.3) | ||
| Days of treatment, mean ± SD | 37.7 ± 5.4 | 37.4 ± 4.9 | 0.873 | |
| Gender, n (%) | F | 5 (33.3) | 7 (50.0) | 0.462 |
| M | 10 (66.7) | 7 (50.0) | ||
| Age, mean ± SD | 70.8 ± 9.8 | 67.9 ± 10.8 | 0.454 | |
| Level of education, n (%) | Primary–middle | 5 (33.3) | 6 (42.9) | 0.710 |
| High university | 10 (66.7) | 8 (57.1) | ||
| Smoker, n (%) | No | 4 (26.7) | 5 (35.7) | 1.000 |
| Former | 8 (53.3) | 7 (50.0) | ||
| Yes | 3 (20.0) | 2 (14.3) | ||
| Alcohol habits, n (%) | No | 5 (33.3) | 7 (50.0) | 0.462 |
| Current/former | 10 (66.7) | 7 (50.0) | ||
| Baseline BMI, n (%) | <25 | 7 (46.7) | 9 (64.3) | 0.462 |
| ≥25 | 8 (53.3) | 5 (35.7) | ||
| Family history of CRC, n (%) | No | 10 (66.7) | 7 (50.0) | 0.462 |
| Yes | 5 (33.3) | 7 (50.0) | ||
| Foods rich in anthocyanins, (servings per day) | <2 | 7 (46.7) | 7 (50.0) | 1.000 |
| ≥2 | 7 (53.3) | 7 (50.0) | ||
| Histological type, n (%) | Tubular | 10 (66.7) | 10 (71.4) | 1.000 |
| Villous | 5 (33.3) | 4 (28.6) | ||
| Dysplasia grade, n (%) | Low-grade | 12 (80.0) | 9 (64.3) | 0.427 |
| High-grade | 3 (20.0) | 5 (35.7) | ||
| # of comorbidity | median (IQR) | 1 (0–3) | 2 (1–3) | 0.295 |
| # of concomitant medications | median (IQR) | 2 (0–4) | 4 (2–5) | 0.086 |
| Treatment | p-Value | |||
|---|---|---|---|---|
| Active | Placebo | |||
| N (% of Positive Cells) | 15 (51.7) | 14 (48.3) | ||
| Normal Tissue | ||||
| Ki-67% | Pre | 19.4 ± 13.1 14.6 (0.7) | 21.2 ± 11.4 18.6 (0.5) | 0.565 |
| Post | 16.1 ± 11.8 11.1 (0.7) | 15.9 ± 10.5 11.1 (0.7) | 0.896 | |
| P53% | Pre | 8.7 ± 11.4 4.9 (1.3) | 3.5 ± 4.8 1.9 (1.4) | 0.580 |
| Post | 3.9 ± 4.4 2.3 (1.1) | 5.4 ± 7.3 3.2 (1.3) | 0.886 | |
| NF-κB% | Pre | 36.7 ± 21.3 29.6 (0.6) | 52.7 ± 20.9 49.3 (0.4) | 0.080 |
| Post | 42.3 ± 31.7 37.6 (0.7) | 50.7 ± 26.7 43.5 (0.5) | 0.445 | |
| β-catenin% | Pre | 100.0 ± 0.0 100.0 (0.0) | 100.0 ± 0.0 100.0 (0.0) | 1.000 |
| Post | 100.0 ± 0.0 100.0 (0.0) | 100.0 ± 0.0 100.0 (0.0) | 1.000 | |
| Dysplastic Tissue | ||||
| Ki-67% | Pre | 44.9 ± 26.4 37.6 (0.6) | 42.9 ± 19.5 39.1 (0.5) | 0.913 |
| Post | 58.0 ± 26.0 50.1 (0.4) | 58.2 ± 23.6 53.1 (0.4) | 0.931 | |
| P53% | Pre | 50.0 ± 24.2 44.8 (0.5) | 37.5 ± 20.5 32.4 (0.5) | 0.419 |
| Post | 60.3 ± 27.8 52.4 (0.5) | 51.8 ± 24.1 46.2 (0.5) | 0.413 | |
| NF-κB% | Pre | 69.7 ± 17.2 67.1 (0.2) | 74.3 ± 15.0 72.6 (0.2) | 0.445 |
| Post | 74.3 ± 21.5 67.8 (0.3) | 81.4 ± 13.5 80.3 (0.2) | 0.383 | |
| β-catenin% | Pre | 100.0 ± 0.0 100.0 (0.0) | 98.6 ± 5.3 98.4 (0.1) | 0.743 |
| Post | 100.0 ± 0.0 100.0 (0.0) | 100.0 ± 0.0 100.0 (0.0) | 1.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briata, I.M.; Paleari, L.; Rutigliani, M.; Petrera, M.; Caviglia, S.; Romagnoli, P.; Libera, M.D.; Oppezzi, M.; Puntoni, M.; Siri, G.; et al. A Presurgical Study of Curcumin Combined with Anthocyanin Supplements in Patients with Colorectal Adenomatous Polyps. Int. J. Mol. Sci. 2021, 22, 11024. https://doi.org/10.3390/ijms222011024
Briata IM, Paleari L, Rutigliani M, Petrera M, Caviglia S, Romagnoli P, Libera MD, Oppezzi M, Puntoni M, Siri G, et al. A Presurgical Study of Curcumin Combined with Anthocyanin Supplements in Patients with Colorectal Adenomatous Polyps. International Journal of Molecular Sciences. 2021; 22(20):11024. https://doi.org/10.3390/ijms222011024
Chicago/Turabian StyleBriata, Irene Maria, Laura Paleari, Mariangela Rutigliani, Marilena Petrera, Silvia Caviglia, Paola Romagnoli, Mauro Dalla Libera, Massimo Oppezzi, Matteo Puntoni, Giacomo Siri, and et al. 2021. "A Presurgical Study of Curcumin Combined with Anthocyanin Supplements in Patients with Colorectal Adenomatous Polyps" International Journal of Molecular Sciences 22, no. 20: 11024. https://doi.org/10.3390/ijms222011024
APA StyleBriata, I. M., Paleari, L., Rutigliani, M., Petrera, M., Caviglia, S., Romagnoli, P., Libera, M. D., Oppezzi, M., Puntoni, M., Siri, G., Lazzeroni, M., Howells, L., Singh, R., Brown, K., & DeCensi, A. (2021). A Presurgical Study of Curcumin Combined with Anthocyanin Supplements in Patients with Colorectal Adenomatous Polyps. International Journal of Molecular Sciences, 22(20), 11024. https://doi.org/10.3390/ijms222011024