
Is Cenobamate the Breakthrough We Have Been Wishing for?


Abstract
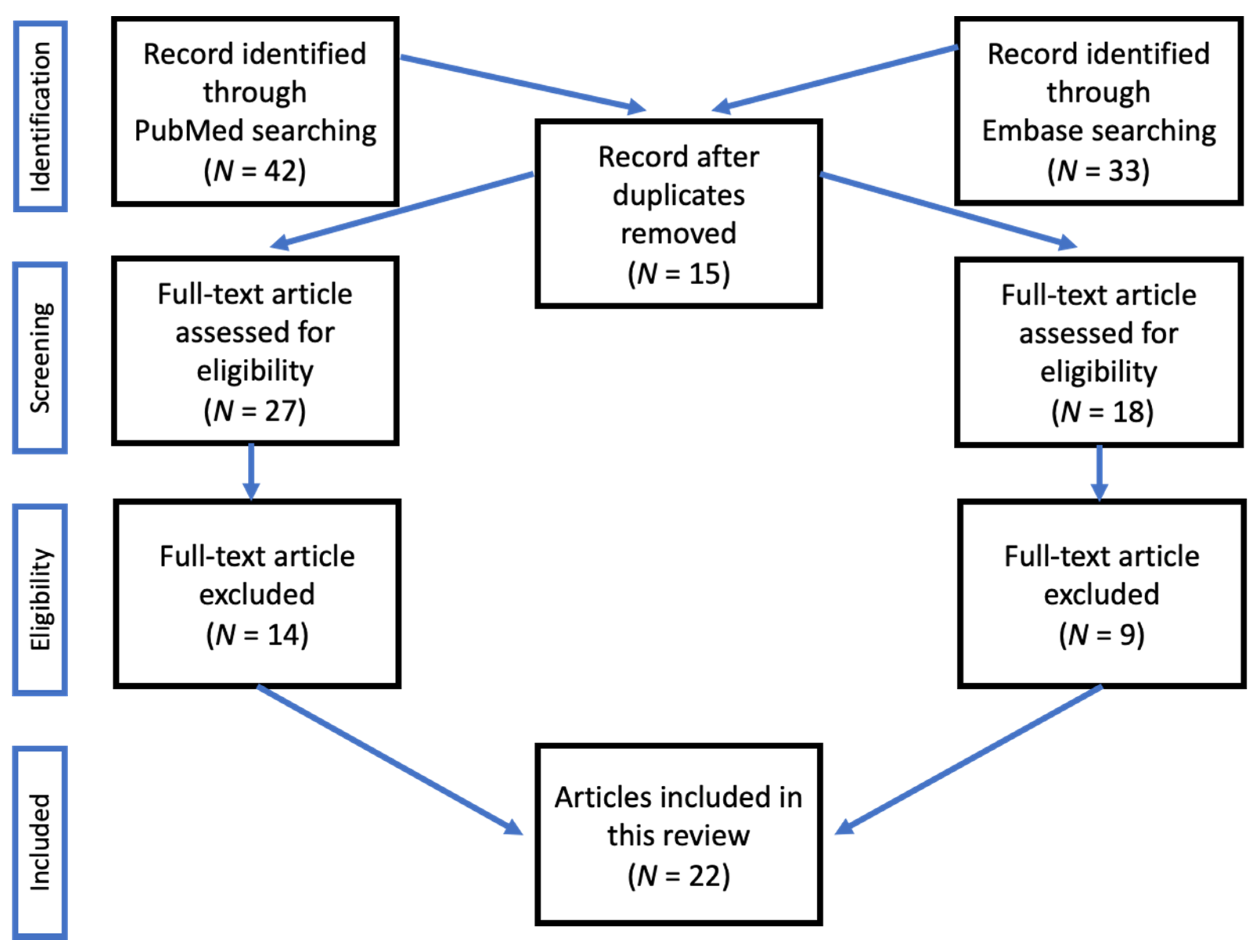
:1. Introduction
2. Mechanism of Action
3. Experimental Models
- Cenobamate prevented:
- -
- In mouse models, seizures induced by maximal electro-shock (MES), with ED50 values of 9.8 mg/kg intraperitoneally;
- -
- In rat models, seizures induced by MES, with ED50 values of 1.9 mg/kg per os [24].
- In mice, cenobamate prevented clonic seizures induced by the subcutaneous administration of pentylenetetrazole (PTZ) and picrotoxin, with ED50 values of 28.5 and 34.5 mg/kg i.p., respectively. In rats, clonic seizures induced by PTZ and status epilepticus induced by lithium/pilocarpine were both abated by cenobamate, with ED50 values of 14 and 7 mg/kg i.p., respectively [24].
- Cenobamate was effective in two models of focal seizures [24]. The ED50 value in the hippocampal kindled rat model was 16.4 mg/kg i.p. In the mouse psychomotor seizure model, the ED50 value at 6 Hz 22 mA was 11 mg/kg i.p. An increase in the current to 32 or 44 mA in this mouse model had little influence on the potency of cenobamate (ED50 values = 18 and 17 mg/kg i.p., respectively).
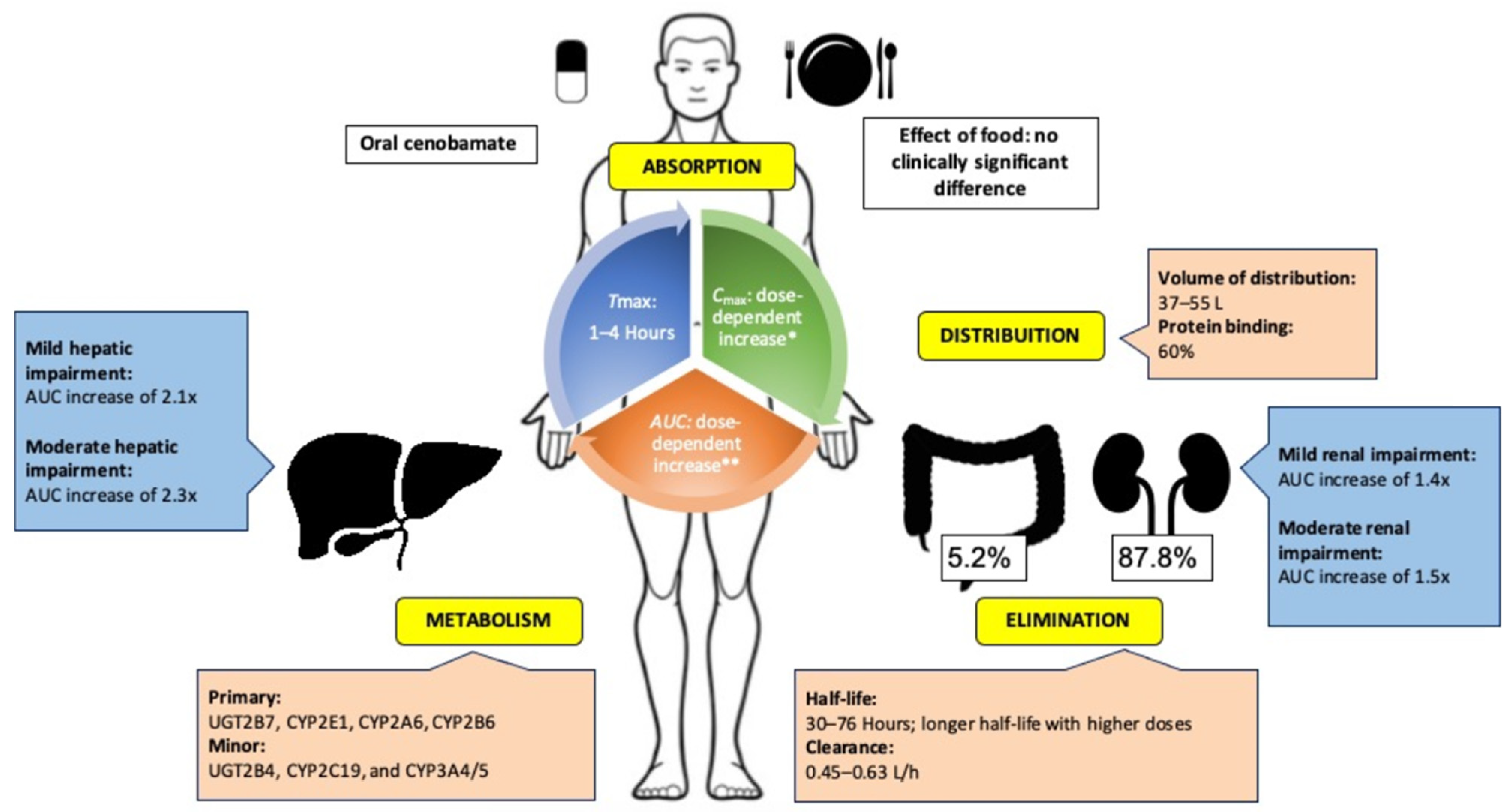
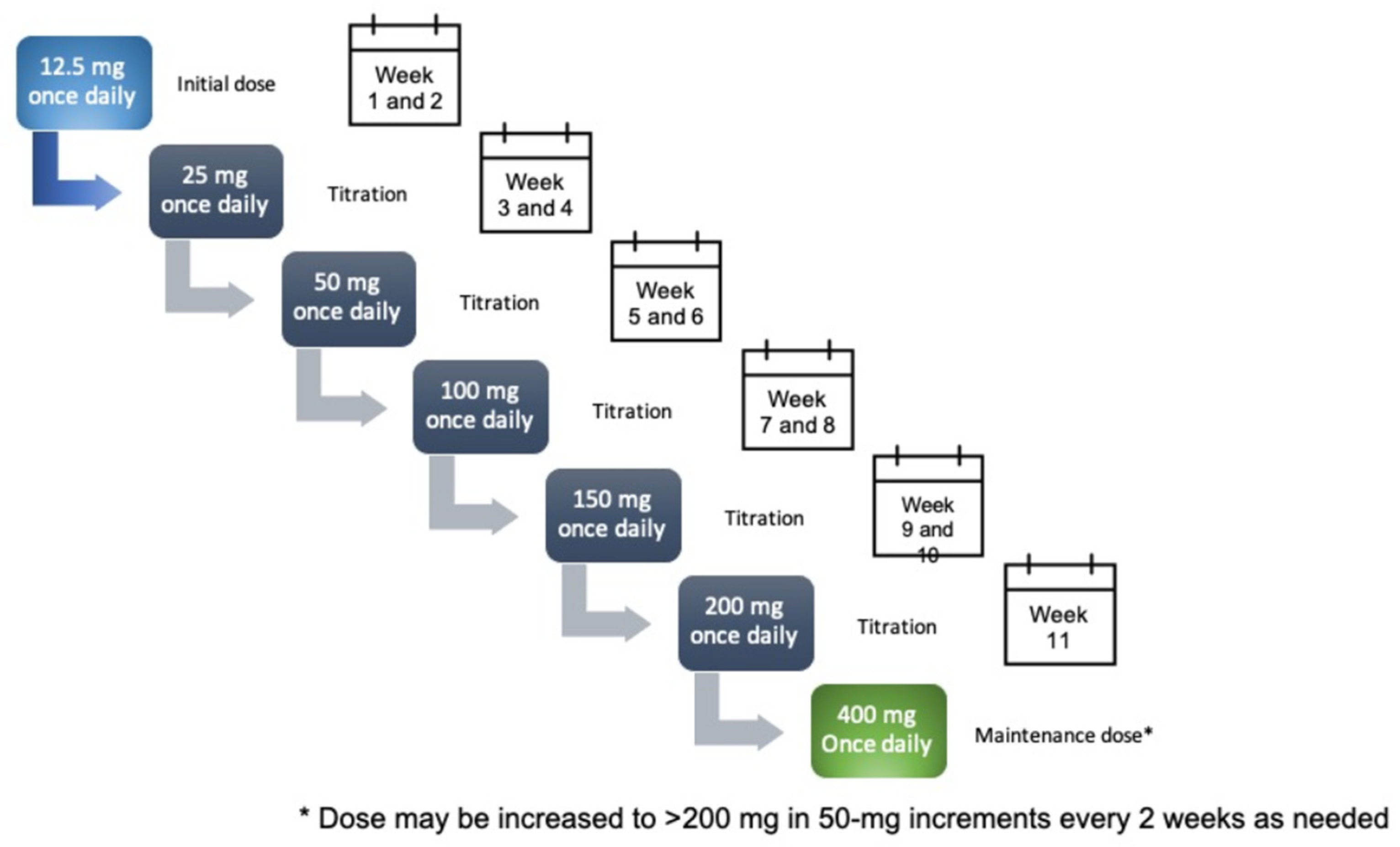
4. Pharmacokinetics
5. Drug Interactions
6. Efficacy Data
6.1. First Clinical Evidence
6.2. Randomised Double-Blind Trials
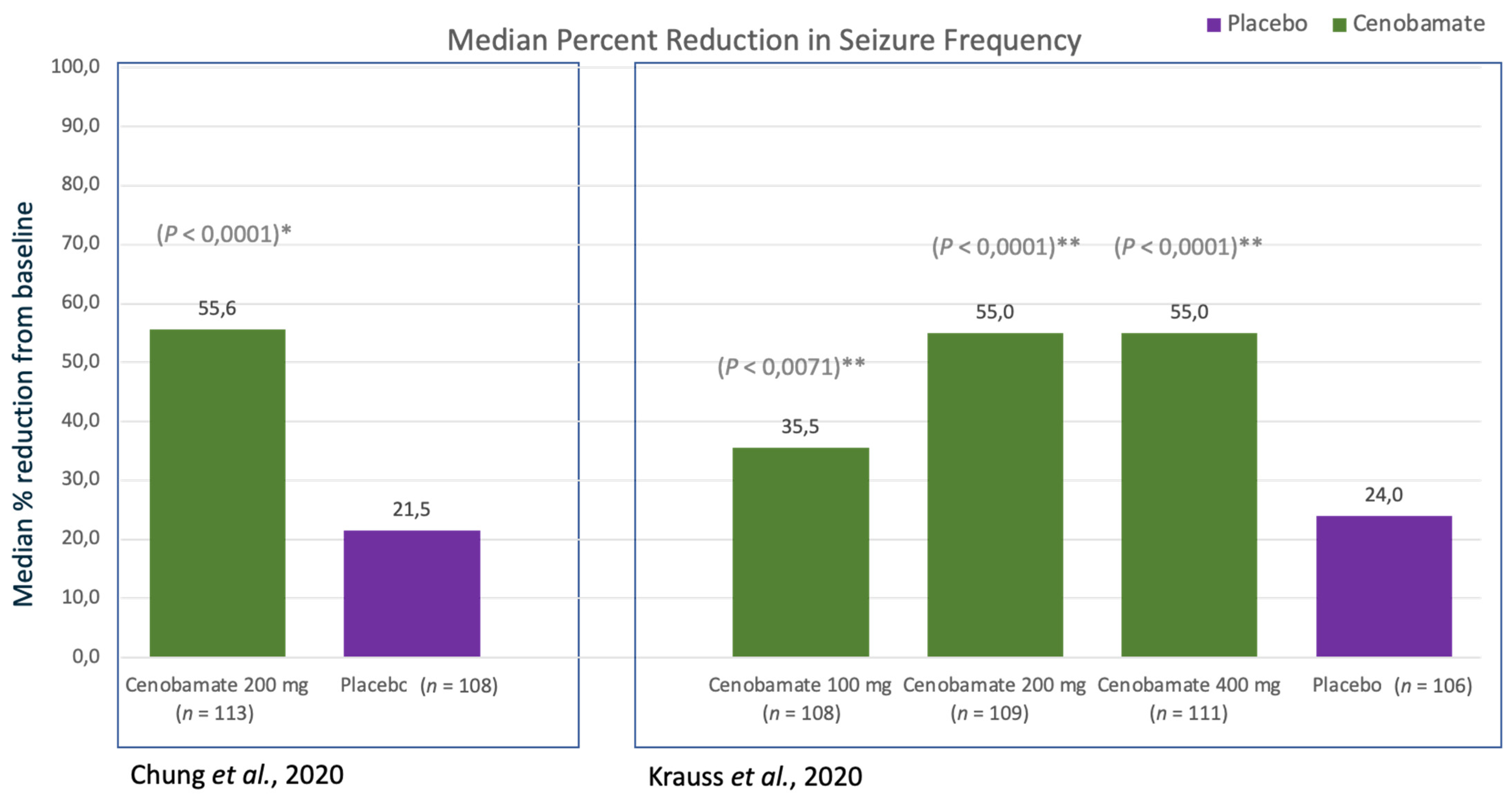
6.2.1. Phase 2 Study by Chung et al.
Relative Change in Seizure Frequency
Responder Rate
6.2.2. Phase 2 Study by Krauss et al.
Relative Change in Seizure Frequency
Responder Rate
6.3. Ongoing Open-Label Efficacy Studies
6.3.1. Extension of First Phase II Study (C013; NCT01397968)
6.3.2. Extension of Second Phase II Study (C017; NCT01866111)
7. Tolerability and Adverse Effect Profile
Ongoing Phase III Open-Label Safety Studies
8. Conclusions and Expert Opinion
9. Future
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perucca, E.; Brodie, M.J.; Kwan, P.; Tomson, T. 30 years of second-generation antiseizure medications: Impact and future perspectives. Lancet Neurol. 2000, 19, 544–556. [Google Scholar] [CrossRef]
- Laxer, K.D.; Trinka, E.; Hirsch, L.J.; Cendes, F.; Langfitt, J.; Delanty, N.; Resnick, T.; Benbadis, S.R. The consequences of refractory epilepsy and its treatment. Epilepsy Behav. 2014, 37, 59–70. [Google Scholar] [CrossRef] [Green Version]
- US Food and Drug Administration (FDA). FDA Approves New Treatment for Adults with Partial-Onset Seizures. 2019. Available online: www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-adults-partial-onset-seizures (accessed on 14 August 2020).
- Krauss, G.L.; Klein, P.; Brandt, C.; Lee, S.K.; Milanov, I.; Milovanovic, M.; Steinhoff, B.J.; Kamin, M. Safety and efficacy of adjunctive cenobamate (YKP3089) in patients with uncontrolled focal seizures: A multicentre, double-blind, randomised, placebo-controlled, dose-response trial. Lancet Neurol. 2020, 19, 38–48. [Google Scholar] [CrossRef]
- Chung, S.S.; French, J.A.; Kowalski, J.; Krauss, G.L.; Lee, S.K.; Maciejowski, M.; Rosenfeld, W.E.; Sperling, M.R.; Mizne, S.; Kamin, M. Randomized phase 2 study of adjunctive cenobamate in patients with uncontrolled focal seizures. Neurology 2020, 94, e2311–e2322. [Google Scholar] [CrossRef]
- Guignet, M.; Campbell, A.; White, H.S. Cenobamate (XCOPRI): Can preclinical and clinical evidence provide insight into its mechanism of action? Epilepsia 2020, 61, 2329–2339. [Google Scholar] [CrossRef] [PubMed]
- Wheless, J.W. Adjunctive cenobamate for the treatment of focal onset seizures in adults with epilepsy: A critical review. Expert Rev. Neurother. 2020, 20, 1085–1098. [Google Scholar] [CrossRef] [PubMed]
- Vernillet, L.; Greene, S.A.; Kim, H.W.; Melnick, S.M.; Glenn, K. Mass Balance, Metabolism, and Excretion of Cenobamate, a New Antiepileptic Drug, After a Single Oral Administration in Healthy Male Subjects. Eur. J. Drug Metab. Pharmacokinet. 2020, 45, 513–522. [Google Scholar] [CrossRef]
- Sperling, M.R.; Klein, P.; Aboumatar, S.; Gelfand, M.; Halford, J.J.; Krauss, G.L.; Rosenfeld, W.E.; Vossler, D.G.; Wechsler, R.; Borchert, L.; et al. Cenobamate (YKP3089) as adjunctive treatment for uncontrolled focal seizures in a large, phase 3, multicenter, open-label safety study. Epilepsia 2020, 61, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Bialer, M.; Johannessen, S.I.; Koepp, M.J.; Levy, R.H.; Perucca, E.; Perucca, P.; Tomson, T.; White, H.S. Progress report on new antiepileptic drugs: A summary of the Fifteenth Eilat Conference on New Antiepileptic Drugs and Devices (EILAT XV). II. Drugs in more advanced clinical development. Epilepsia 2020, 61, 2365–2385. [Google Scholar] [CrossRef]
- Steinhoff, B.J. Cenobamate tablets as a treatment for focal-onset seizures in adults. Expert Rev. Clin. Pharmacol. 2021, 14, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Elizebath, R.; Zhang, E.; Coe, P.; Gutierrez, E.G.; Yang, J.; Krauss, G.L. Cenobamate treatment of focal-onset seizures: Quality of life and outcome during up to eight years of treatment. Epilepsy Behav. 2021, 116, 107796. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M. Cenobamate in focal seizures: A profile of its use. Drugs Ther. Perspect. 2020, 36, 327–334. [Google Scholar] [CrossRef]
- Glenn, K.J.; Greene, S.; Kim, H.W.; Melnick, S.M.; Vernill, L. Absorption, distribution, metabolism, and excretion of the novel antiepileptic drug cenobamate: Mass balance following oral administration in healthy male subjects. Drug Metab. Pharmacokinet. 2020, 35, S69. [Google Scholar] [CrossRef]
- Kasteleijn-Nolst Trenite, D.G.A.; DiVentura, B.D.; Pollard, J.R.; Krauss, G.L.; Mizne, S.; French, J.A. Suppression of the photoparoxysmal response in photosensitive epilepsy with cenobamate (YKP3089). Neurology 2019, 93, e559–e567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernillet, L.; Kamin, M. Drug–drug interactions between cenobamate and other antiepileptic drugs: Results from phase I studies with carbamazepine, phenobarbital, phenytoin, and divalproex sodium. Clin. Pharmacol. Ther. 2018, 103 (Suppl. 1), S91. [Google Scholar]
- Keam, S.J. Cenobamate: First Approval. Drugs 2020, 80, 73–78. [Google Scholar] [CrossRef]
- Nakamura, M.; Cho, J.H.; Shin, H.; Jang, I.S. Effects of cenobamate (YKP3089), a newly developed anti-epileptic drug, on voltage-gated sodium channels in rat hippocampal CA3 neurons. Eur. J. Pharmacol. 2019, 15, 175–182. [Google Scholar] [CrossRef]
- Lattanzi, S.; Trinka, E.; Zaccara, G.; Striano, P.; Del Giovane, C.; Silvestrini, M.; Brigo, F. Adjunctive Cenobamate for Focal-Onset Seizures in Adults: A Systematic Review and Meta-Analysis. CNS Drugs. 2020, 34, 1105–1120. [Google Scholar] [CrossRef]
- Vernillet, L.; Greene, S.A.; Kamin, M. Pharmacokinetics of Cenobamate: Results From Single and Multiple Oral Ascending-Dose Studies in Healthy Subjects. Clin. Pharmacol. Drug Dev. 2020, 9, 428–443. [Google Scholar] [CrossRef]
- Buckley, C.T.; Waters, O.R.; DeMaagd, G. Cenobamate: A New Adjunctive Agent for Drug-Resistant Focal Onset Epilepsy. Ann. Pharmacother 2021, 55, 318–329. [Google Scholar] [CrossRef]
- Strzelczyk, A.; Mann, C.; Willems, L.M.; Rosenow, F.; Bauer, S. Cenobamate for the treatment of focal epilepsies. Expert Opin. Pharmacother. 2020, 21, 2215–2223. [Google Scholar] [CrossRef]
- Sharma, R.; Nakamura, M.; Neupane, C.; Jeon, B.H.; Shin, H.; Melnick, S.M.; Glenn, K.J.; Jang, I.S.; Park, J.B. Positive allosteric modulation of GABAA receptors by a novel antiepileptic drug cenobamate. Eur. J. Pharmacol. 2020, 15, 173117. [Google Scholar] [CrossRef]
- Bialer, M.; Johannessen, S.I.; Levy, R.H.; Perucca, E.; Tomson, T.; White, H.S. Progress report on new antiepileptic drugs: A summary of the Eleventh Eilat Conference (EILAT XI). Epilepsy Res. 2013, 103, 2–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melnick, S.M.; Shin, H.; Roucard, C.; Glenn, K. Cenobamate (YKP3089) Dose-Dependently Reduced Spike-and-Wave Discharges in the Ge-Netic Absence Epilepsy Rats from Strasbourg (GAERS) Animal Model. In Proceedings of the Neuroscience 2019, Chicago, IL, USA, 19–23 October 2019; Available online: https://www.abstractsonline.com/pp8/#!/7883/presentation/69880 (accessed on 11 March 2020).
- SK Life Science, Inc. XCOPRI® (Cenobamate Tablets), for Oral Use, CV [Prescribing Information]. Paramus, NJ, USA: SK Life Science, Inc. August 2020. Available online: https://www.acce.sdata.fda.gov/drug.atfdadocs/label/2019/212839s000lbl.pdf (accessed on 8 April 2021).
- Zhang, N.; Shon, J.; Kim, M.J.; Yu, C.; Zhang, L.; Huang, S.M.; Lee, L.; Tran, D.; Li, L. Role of CYP3A in Oral Contraceptives Clearance. Clin. Transl. Sci. 2018, 11, 251–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Leon, J.; Spina, E.; Diaz, F.J. Clobazam therapeutic drug monitoring: A comprehensive review of the literature with proposals to improve future studies. Ther. Drug Monit. 2013, 35, 30–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, J.A.; Chung, S.S.; Krauss, G.L.; Lee, S.K.; Maciejowski, M.; Rosenfeld, W.E.; Sperling, M.R.; Kamin, M. Long-term safety of adjunctive cenobamate in patients with uncontrolled focal seizures: Open-label extension of a randomized clinical study. Epilepsia. 2021, 1–9. [Google Scholar] [CrossRef]
- Steinhoff, B.J.; Ben-Menachem, E.; Ryvlin, P.; Shorvon, S.; Kramer, L.; Satlin, A.; Squillacote, D.; Yang, H.; Zhu, J.; Laurenza, A. Efficacy and safety of adjunctive perampanel for the treatment of refractory partial seizures: A pooled analysis of three phase III studies. Epilepsia 2013, 54, 1481–1489. [Google Scholar] [CrossRef]
- Ben-Menachem, E.; Mameniškienė, R.; Quarato, P.P.; Klein, P.; Gamage, J.; Schiemann, J.; Johnson, M.E.; Whitesides, J.; McDonough, B.; Eckhardt, K. Efficacy and safety of brivaracetam for partial-onset seizures in 3 pooled clinical studies. Neurology 2016, 19, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Fareleira, F.; Ascenção, R.; Borges, M.; Sampaio, C.; Vaz-Carneiro, A. Clinical comparability of the new antiepileptic drugs in refractory partial epilepsy: A systematic review and meta-analysis. Epilepsia 2011, 52, 1280–1291. [Google Scholar] [CrossRef] [PubMed]
- Randomized, Double-Blind Study to Evaluate Efficacy and Safety of Cenobamate Adjunctive Therapy in PGTC Seizures. ClinicalTrials.gov Identifier: NCT03678753; Updated 19 September 2019. Available online: https://ClinicalTrials.gov/show/NCT03678753 (accessed on 8 April 2021).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug/Substrate | Effect of Cenomabate on Drug/Substrate | Effect of Drug/Substrate on Cenomabate | Expected Effects | Clinical Recommendation |
|---|---|---|---|---|
| Lamotrigine | ↓ plasma concentrations | - | ↓ concentrations by 21–52% | Monitoring and ↑ the dosage of lamotrigine |
| Carbamazepine | ↓ plasma concentrations | - | ↓ AUC of 24% | Monitoring and ↑ the dosage of carbamazepine |
| Phenytoin | ↑ plasma concentrations | ↓ cenobamate concentrations |
| Monitoring and gradually ↓ PHT dosage by up to 50% during titration |
| Phenobarbital | ↑ plasma concentrations | ↓ cenobamate concentrations |
| Monitoring and ↓ dosage of phenobarbital |
| Desmethylclobazam | ↑ plasma concentrations | - | ↑ concentrations of N-CLB | Monitoring and ↓ dosage of clobazam |
| CYP2B6 Substrates | ↓ plasma concentrations | - | ↓ AUC of 39% and Cmax of 23% | ↑ the dosage of CYP2B6 substrates |
| CYP3A Substrates | ↓ plasma concentrations | - | ↓ AUC of 72% and Cmax of 61% | ↑ the dosage of CYP2B6 substrates |
| CYP2C19 substrates | ↑ plasma concentrations | - | ↓ AUC of 107% and Cmax of 83% | ↓ dosage of CYP2C19 substrates |
| Oral Contraceptives | ↓ plasma concentrations | - | ↓ concentrations of oral contraceptives are expected because of CYP3A4 induction | Women should use additional or alternative non-hormonal birth control |
| Drugs That Shorten the QT Interval | Additive effect on QT interval shortening | - | Cenobamate has demonstrated dose-dependent shortening of the QT interval | Caution should be used when administering cenobamate and other drugs that shorten the QT interval |
| CNS Depressants | Additive effect of CNS depressants | - | Cenobamate has demonstrated dose-dependent adverse effects that primarily affect the CNS | CNS depressants should be used cautiously when used in combination with cenobamate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Specchio, N.; Pietrafusa, N.; Vigevano, F. Is Cenobamate the Breakthrough We Have Been Wishing for? Int. J. Mol. Sci. 2021, 22, 9339. https://doi.org/10.3390/ijms22179339
Specchio N, Pietrafusa N, Vigevano F. Is Cenobamate the Breakthrough We Have Been Wishing for? International Journal of Molecular Sciences. 2021; 22(17):9339. https://doi.org/10.3390/ijms22179339
Chicago/Turabian StyleSpecchio, Nicola, Nicola Pietrafusa, and Federico Vigevano. 2021. "Is Cenobamate the Breakthrough We Have Been Wishing for?" International Journal of Molecular Sciences 22, no. 17: 9339. https://doi.org/10.3390/ijms22179339
APA StyleSpecchio, N., Pietrafusa, N., & Vigevano, F. (2021). Is Cenobamate the Breakthrough We Have Been Wishing for? International Journal of Molecular Sciences, 22(17), 9339. https://doi.org/10.3390/ijms22179339