
Genetic Contribution of Endometriosis to the Risk of Developing Hormone-Related Cancers

 ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Results
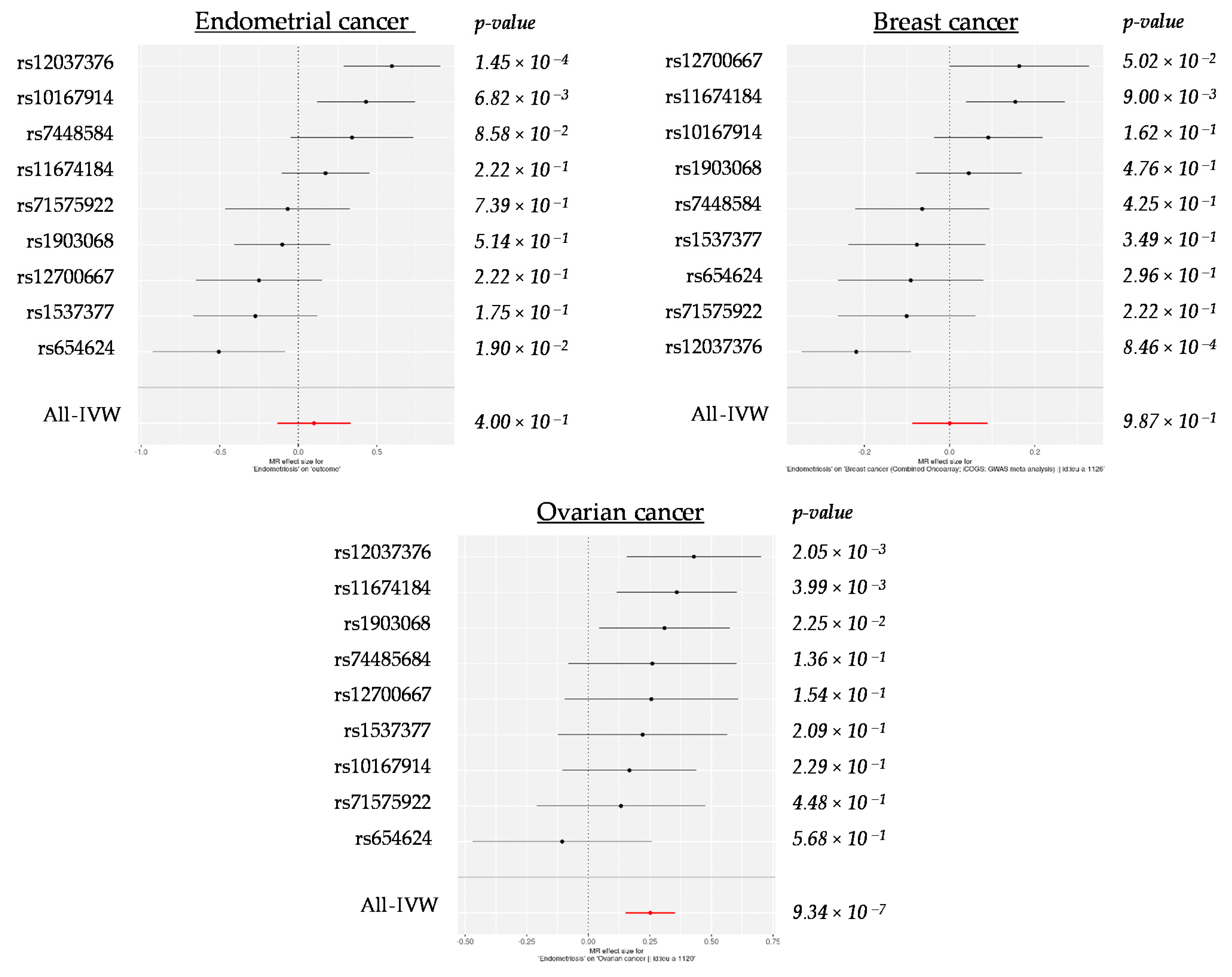
2.1. 2SMR Analyses between Endometriosis and Hormone-Related Cancers Suggest a Potential Causal Relationship between Endometriosis and Ovarian Cancer
2.2. Sensitivity Analyses between Endometriosis and Hormone-Related Cancers Point to Heterogeneity with Breast Cancer and Horizontal Pleiotropy with Endometrial Cancer
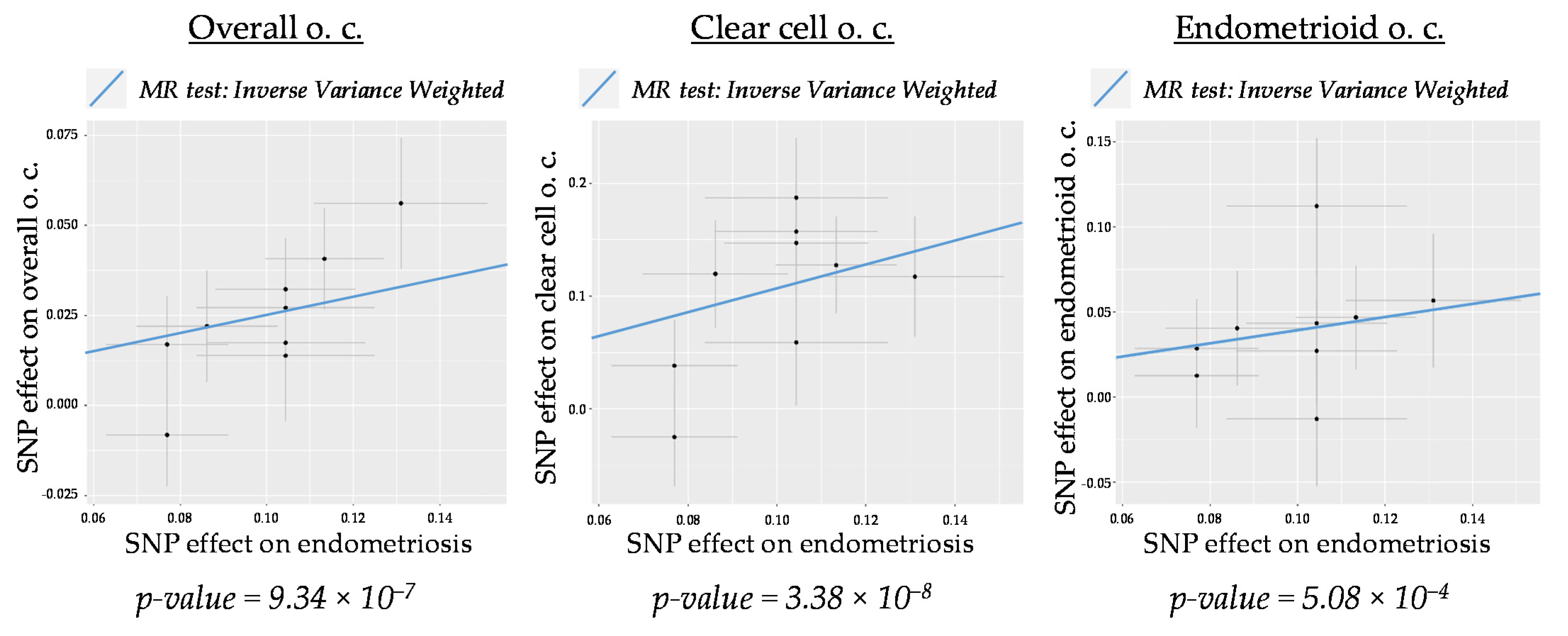
2.3. 2SMR Estimates between Endometriosis and Ovarian Cancer Subtypes Suggest a Stronger Causal Genetic Link between Endometriosis and Clear Cell and Endometrioid Histotypes
3. Discussion
4. Materials and Methods
4.1. GWAS Data Sources
4.2. Two-Sample Mendelian Randomization (2SMR) Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zondervan, K.T.; Becker, C.M.; Missmer, S.A. Endometriosis. N. Engl. J. Med. 2020, 382, 1244–1256. [Google Scholar] [CrossRef]
- Mogensen, J.B.; Kjær, S.K.; Mellemkjær, L.; Jensen, A. Endometriosis and risks for ovarian, endometrial and breast cancers: A nationwide cohort study. Gynecol. Oncol. 2016, 143, 87–92. [Google Scholar] [CrossRef]
- Kvaskoff, M.; Mahamat-Saleh, Y.; Farland, L.V.; Shigesi, N.; Terry, K.L.; Harris, H.R.; Roman, H.; Becker, C.M.; As-Sanie, S.; Zondervan, K.T.; et al. Endometriosis and cancer: A systematic review and meta-analysis. Hum. Reprod. Update 2020, 27, 393–420. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, A.; Sebastian, A.; Thomas, A.; George, R.; Thomas, V.; Peedicayil, A. Endometriosis and malignancy: The intriguing relationship. Int. J. Gynecol. Obstet. 2021, 13585. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, R.; Tang, S.; Feng, F.; Liu, C.; Wang, L.; Zhao, W.; Zhang, T.; Yao, Y.; Wang, X.; et al. Impact of endometriosis on risk of ovarian, endometrial and cervical cancers: A meta-analysis. Arch. Gynecol. Obstet. 2019, 299, 35–46. [Google Scholar] [CrossRef]
- Gandini, S.; Lazzeroni, M.; Peccatori, F.A.; Bendinelli, B.; Saieva, C.; Palli, D.; Masala, G.; Caini, S. The risk of extra-ovarian malignancies among women with endometriosis: A systematic literature review and meta-analysis. Crit. Rev. Oncol. Hematol. 2019, 134, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Johnatty, S.E.; Stewart, C.J.R.; Smith, D.; Nguyen, A.; O’Dwyer, J.; O’Mara, T.A.; Webb, P.M.; Spurdle, A.B. Co-existence of leiomyomas, adenomyosis and endometriosis in women with endometrial cancer. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Yu, H.C.; Lin, C.Y.; Chang, W.C.; Shen, B.J.; Chang, W.P.; Chuang, C.M. Increased association between endometriosis and endometrial cancer: A nationwide population-based retrospective cohort study. Int. J. Gynecol. Cancer 2015, 25, 447–452. [Google Scholar] [CrossRef]
- Pontikaki, A.; Sifakis, S.; Spandidos, D.A. Endometriosis and breast cancer: A survey of the epidemiological studies. Oncol. Lett. 2016, 11, 23–30. [Google Scholar] [CrossRef]
- Munksgaard, P.S.; Blaakaer, J. The association between endometriosis and gynecological cancers and breast cancer: A review of epidemiological data. Gynecol. Oncol. 2011, 123, 157–163. [Google Scholar] [CrossRef]
- Bertelsen, L.; Mellemkjær, L.; Frederiksen, K.; Kjær, S.K.; Brinton, L.A.; Sakoda, L.C.; Van Valkengoed, I.; Olsen, J.H. Risk for breast cancer among women with endometriosis. Int. J. Cancer 2007, 120, 1372–1375. [Google Scholar] [CrossRef] [PubMed]
- Saavalainen, L.; Lassus, H.; But, A.; Tiitinen, A.; Härkki, P.; Gissler, M.; Pukkala, E.; Heikinheimo, O. A cohort study of 49,933 women with surgically verified endometriosis: Increased incidence of breast cancer below the age of 40. Acta Obstet. Gynecol. Scand. 2019, 98, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Matta, J.L.; Flores, I.; Morales, L.M.; Monteiro, J.; Alvarez-Garriga, C.; Bayona, M. Women with endometriosis have a higher DNA repair capacity and diminished breast cancer risk. Mol. Cancer Boil. 2013, 1, 1. [Google Scholar]
- Morales, L.; Alvarez-Garriga, C.; Matta, J.; Ortiz, C.; Vergne, Y.; Vargas, W.; Acosta, H.; Ramírez, J.; Perez-Mayoral, J.; Bayona, M. Factors associated with breast cancer in Puerto Rican women. J. Epidemiol. Glob. Health 2013, 3, 205–215. [Google Scholar] [CrossRef]
- Karnezis, A.N.; Cho, K.R.; Gilks, C.B.; Pearce, C.L.; Huntsman, D.G. The disparate origins of ovarian cancers: Pathogenesis and prevention strategies. Nat. Rev. Cancer 2017, 17, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Brilhante, A.V.M.; Augusto, K.L.; Portela, M.C.; Sucupira, L.C.G.; Oliveira, L.A.F.; Pouchaim, A.J.M.V.; Nóbrega, L.R.M.; De Magalhães, T.F.; Sobreira, L.R.P. Endometriosis and ovarian cancer: An integrative review (endometriosis and ovarian cancer). Asian Pac. J. Cancer Prev. 2017, 18, 11–16. [Google Scholar] [PubMed]
- Wang, C.; Liang, Z.; Liu, X.; Zhang, Q.; Li, S. The association between endometriosis, tubal ligation, hysterectomy and epithelial ovarian cancer: Meta-analyses. Int. J. Environ. Res. Public Health 2016, 13, 1138. [Google Scholar] [CrossRef]
- Murakami, K.; Kotani, Y.; Nakai, H.; Matsumura, N. Endometriosis-associated ovarian cancer: The origin and targeted therapy. Cancers 2020, 12, 1676. [Google Scholar] [CrossRef]
- Pearce, C.L.; Templeman, C.; Rossing, M.A.; Lee, A.; Near, A.M.; Webb, P.M.; Nagle, C.M.; Doherty, J.A.; Cushing-Haugen, K.L.; Wicklund, K.G.; et al. Association between endometriosis and risk of histological subtypes of ovarian cancer: A pooled analysis of case-control studies. Lancet Oncol. 2012, 13, 385–394. [Google Scholar] [CrossRef]
- Wentzensen, N.; Poole, E.M.; Trabert, B.; White, E.; Arslan, A.A.; Patel, A.V.; Setiawan, V.W.; Visvanathan, K.; Weiderpass, E.; Adami, H.O.; et al. Ovarian cancer risk factors by histologic subtype: An analysis from the Ovarian Cancer Cohort Consortium. J. Clin. Oncol. 2016, 34, 2888–2898. [Google Scholar] [CrossRef]
- Anglesio, M.S.; Yong, P.J. Endometriosis-associated ovarian cancers. Clin. Obstet. Gynecol. 2017, 60, 711–727. [Google Scholar] [CrossRef]
- Saavalainen, L.; Lassus, H.; But, A.; Tiitinen, A.; Härkki, P.; Gissler, M.; Pukkala, E.; Heikinheimo, O. Risk of gynecologic cancer according to the type of endometriosis. Obstet. Gynecol. 2018, 131, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Hermens, M.; Van Altena, A.M.; Nieboer, T.E.; Schoot, B.C.; Van Vliet, H.A.A.M.; Siebers, A.G.; Bekkers, R.L.M. Incidence of endometrioid and clear-cell ovarian cancer in histological proven endometriosis: The ENOCA population-based cohort study. Am. J. Obstet. Gynecol. 2020, 223, 107.e1–107.e11. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.B.; Hankinson, S.E. Endogenous estrogens and the risk of breast, endometrial, and ovarian cancers. Steroids 2015, 99, 8–10. [Google Scholar] [CrossRef]
- Leenen, S.; Hermens, M.; De Vos van Steenwijk, P.J.; Bekkers, R.L.M.; Van Esch, E.M.G. Immunologic factors involved in the malignant transformation of endometriosis to endometriosis-associated ovarian carcinoma. Cancer Immunol. Immunother. 2021, 1–9. [Google Scholar]
- Painter, J.N.; O’Mara, T.A.; Morris, A.P.; Cheng, T.H.T.; Gorman, M.; Martin, L.; Hodson, S.; Jones, A.; Martin, N.G.; Gordon, S.; et al. Genetic overlap between endometriosis and endometrial cancer: Evidence from cross-disease genetic correlation and GWAS meta-analyses. Cancer Med. 2018, 7, 1978–1987. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Cuellar-Partida, G.; Painter, J.N.; Nyholt, D.R.; Morris, A.P.; Fasching, P.A.; Hein, A.; Burghaus, S.; Beckmann, M.W.; Lambrechts, D.; et al. Shared genetics underlying epidemiological association between endometriosis and ovarian cancer. Hum. Mol. Genet. 2015, 24, 5955–5964. [Google Scholar] [CrossRef]
- Lee, A.W.; Templeman, C.; Stram, D.A.; Beesley, J.; Tyrer, J.; Berchuck, A.; Pharoah, P.P.; Chenevix-Trench, G.; Pearce, C.L.; Ness, R.B.; et al. Evidence of a genetic link between endometriosis and ovarian cancer. Fertil. Steril. 2016, 105, 35–43.e10. [Google Scholar] [CrossRef]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-base platform supports systematic causal inference across the human phenome. Elife 2018, 7, e34408. [Google Scholar] [CrossRef]
- Cho, Y.; Haycock, P.C.; Sanderson, E.; Gaunt, T.R.; Zheng, J.; Morris, A.P.; Davey Smith, G.; Hemani, G. Exploiting horizontal pleiotropy to search for causal pathways within a Mendelian randomization framework. Nat. Commun. 2020, 11, 1–13. [Google Scholar] [CrossRef]
- Powell, J.E.; Fung, J.N.; Shakhbazov, K.; Sapkota, Y.; Cloonan, N.; Hemani, G.; Hillman, K.M.; Kaufmann, S.; Luong, H.T.; Bowdler, L.; et al. Endometriosis risk alleles at 1p36.12 act through inverse regulation of CDC42 and LINC00339. Hum. Mol. Genet. 2016, 25, 5046–5058. [Google Scholar] [PubMed]
- Fung, J.N.; Mortlock, S.; Girling, J.E.; Holdsworth-Carson, S.J.; Teh, W.T.; Zhu, Z.; Lukowski, S.W.; McKinnon, B.D.; McRae, A.; Yang, J.; et al. Genetic regulation of disease risk and endometrial gene expression highlights potential target genes for endometriosis and polycystic ovarian syndrome. Sci. Rep. 2018, 8, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Sapkota, Y.; Steinthorsdottir, V.; Morris, A.P.; Fassbender, A.; Rahmioglu, N.; De Vivo, I.; Buring, J.E.; Zhang, F.; Edwards, T.L.; Jones, S.; et al. Meta-analysis identifies five novel loci associated with endometriosis highlighting key genes involved in hormone metabolism. Nat. Commun. 2017, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, 1001779. [Google Scholar] [CrossRef] [PubMed]
- O’Mara, T.A.; Glubb, D.M.; Amant, F.; Annibali, D.; Ashton, K.; Attia, J.; Auer, P.L.; Beckmann, M.W.; Black, A.; Bolla, M.K.; et al. Identification of nine new susceptibility loci for endometrial cancer. Nat. Commun. 2018, 9, 1–12. [Google Scholar] [CrossRef]
- Michailidou, K.; Lindström, S.; Dennis, J.; Beesley, J.; Hui, S.; Kar, S.; Lemaçon, A.; Soucy, P.; Glubb, D.; Rostamianfar, A.; et al. Association analysis identifies 65 new breast cancer risk loci. Nature 2017, 551, 92–94. [Google Scholar] [CrossRef]
- Phelan, C.M.; Kuchenbaecker, K.B.; Tyrer, J.P.; Kar, S.P.; Lawrenson, K.; Winham, S.J.; Dennis, J.; Pirie, A.; Riggan, M.J.; Chornokur, G.; et al. Identification of 12 new susceptibility loci for different histotypes of epithelial ovarian cancer. Nat. Genet. 2017, 49, 680–691. [Google Scholar] [CrossRef]
- Prat, J. Ovarian carcinomas: Five distinct diseases with different origins, genetic alterations, and clinicopathological features. Virchows Arch. 2012, 460, 237–249. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Outcome and Method | Beta | SE | p-Value |
|---|---|---|---|
| Endometrial cancer | |||
| IVW | 0.100 | 0.118 | 0.400 |
| WM | 0.028 | 0.093 | 0.767 |
| MRE | 1.786 | 0.420 | 0.004 |
| Breast cancer | |||
| IVW | 0.001 | 0.045 | 0.987 |
| WM | 0.007 | 0.038 | 0.849 |
| MRE | −0.068 | 0.294 | 0.824 |
| Ovarian cancer | |||
| IVW | 0.251 | 0.051 | 9.34 × 10−7 |
| WM | 0.258 | 0.068 | 1.37 × 10−4 |
| MRE | 0.840 | 0.311 | 3.09 × 10−2 |
| Heterogeneity Test | |||
| Outcome and Method | Q | Q_df | p-Value |
| Endometrial cancer | |||
| IVW | 32.67 | 8 | 0.00007 |
| MRE | 9.69 | 7 | 0.20671 |
| Breast cancer | |||
| IVW | 28.34 | 8 | 0.00041 |
| MRE | 28.12 | 7 | 0.00021 |
| Ovarian cancer | |||
| IVW | 7.12 | 8 | 0.52346 |
| MRE | 3.46 | 7 | 0.83951 |
| Horizontal Pleiotropy Test | |||
| Outcome | Egger Intercept | SE | p-Value |
| Endometrial cancer | −0.171 | 0.042 | 0.00472 |
| Breast cancer | 0.007 | 0.029 | 0.81924 |
| Ovarian cancer | −0.059 | 0.031 | 0.09719 |
| Phenotype | Data Source | GWAS ID | Sample Size (Cases/Controls) | Population | 1st Author, Year [Reference] |
|---|---|---|---|---|---|
| Endometriosis | |||||
| Discovery | GWAS catalog | GCST004549 | 208,641 (17,045/191,596) | European and Japanese 1 | Sapkota, 2017 [33] |
| Replication | IEU GWAS db | ukb-b-10903 | 462,933 (3809/459,124) | European (UK) | UKBB cohort [34] |
| Endometrial cancer (e. c.) | GWAS catalog | GCST006464 | 121,885 (12,906/108,979) | O’Mara, 2018 [35] | |
| Breast cancer (b. c.) | IEU GWAS db | ieu-a-1126 | 228,951 (122,977/105,974) | European | Michailidou, 2017 [36] |
| Ovarian cancer (o. c.)2 | Phelan, 2017 [37] | ||||
| Overall o. c. | IEU GWAS db | ieu-a-1120 | 66,450 (25,509/40,941) | European | |
| High grade serous o. c. | IEU GWAS db | ieu-a-1121 | 53,978 (13,037/40,941) | European | |
| Low grade serous o. c. | IEU GWAS db | ieu-a-1122 | 41,953 (1012/40,941) | European | |
| Invasive mucinous o. c. | IEU GWAS db | ieu-a-1223 | 42,358 (1417/40,941) | European | |
| Clear cell o. c. | IEU GWAS db | ieu-a-1124 | 42,307 (1366/40,941) | European | |
| Endometrioid o. c. | IEU GWAS db | ieu-a-1125 | 43,751 (2810/40,941) | European | |
| High grade and low grade serous o. c. | IEU GWAS db | ieu-a-1228 | 54,990 (14,049/40,941) | European | |
| Serous o. c.: low grade and low malignant pot. | IEU GWAS db | ieu-a-1229 | 43,907 (2966/40,941) | European | |
| Serous o. c.: low malignant pot. | IEU GWAS db | ieu-a-1230 | 42,895 (1954/40,941) | European | |
| Mucinous o. c.: invasive and low malignant pot. | IEU GWAS db | ieu-a-1231 | 43,507 (2566/40,941) | European | |
| Low malignant potential mucinous o. c. | IEU GWAS db | ieu-a-1232 | 42,090 (1149/40,941) | European | |
| Low malignant potential o. c. | IEU GWAS db | ieu-a-1233 | 47,147 (3103/40,941) | European |
| SNP | Effect/Other Allele | Chr. | Nearest TSS | EAF 1 | Beta | SE | p-Value |
|---|---|---|---|---|---|---|---|
| Sapkota et al. | |||||||
| rs11674184 | G/T | 2 | GREB1 | 0.39 | −0.113 | 0.014 | 3 × 10−14 |
| rs12037376 | A/G | 1 | WNT4 | 0.17 | 0.131 | 0.020 | 1 × 10−12 |
| rs1903068 | A/G | 4 | KDR | 0.68 | 0.104 | 0.016 | 2 × 10−11 |
| rs12700667 | A/G | 7 | Intergenic | 0.74 | 0.086 | 0.016 | 2 × 10−8 |
| rs1537377 | C/T | 9 | CDKN2B-AS1 | 0.40 | 0.077 | 0.014 | 2 × 10−8 |
| rs71575922 | G/C | 6 | SYNE1 | 0.16 | 0.104 | 0.021 | 2 × 10−8 |
| rs74485684 | T/C | 11 | FSHB | 0.84 | 0.104 | 0.021 | 3 × 10−8 |
| rs10167914 | G/A | 2 | IL1A | 0.30 | 0.104 | 0.018 | 5 × 10−8 |
| rs760794 | T/C | 6 | ID4 | 0.43 | 0.077 | 0.014 | 7 × 10−8 |
| rs6546324 | A/C | 2 | ETAA1 | 0.31 | 0.077 | 0.014 | 3 × 10−7 |
| rs4762326 | T/C | 12 | VEZT | 0.47 | 0.068 | 0.014 | 1 × 10−6 |
| UKBB | |||||||
| rs61768001 | C/T | 1 | WNT4 | 0.16 | 0.002 | 0.0003 | 1 × 10−11 |
| rs9992737 | T/C | 4 | KDR | 0.28 | −0.001 | 0.0002 | 2 × 10−10 |
| rs11031005 | C/T | 11 | FSHB | 0.14 | −0.002 | 0.0003 | 1.5 × 10−9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rueda-Martínez, A.; Garitazelaia, A.; Cilleros-Portet, A.; Marí, S.; Arauzo, R.; de Miguel, J.; González-García, B.P.; Fernandez-Jimenez, N.; Bilbao, J.R.; García-Santisteban, I. Genetic Contribution of Endometriosis to the Risk of Developing Hormone-Related Cancers. Int. J. Mol. Sci. 2021, 22, 6083. https://doi.org/10.3390/ijms22116083
Rueda-Martínez A, Garitazelaia A, Cilleros-Portet A, Marí S, Arauzo R, de Miguel J, González-García BP, Fernandez-Jimenez N, Bilbao JR, García-Santisteban I. Genetic Contribution of Endometriosis to the Risk of Developing Hormone-Related Cancers. International Journal of Molecular Sciences. 2021; 22(11):6083. https://doi.org/10.3390/ijms22116083
Chicago/Turabian StyleRueda-Martínez, Aintzane, Aiara Garitazelaia, Ariadna Cilleros-Portet, Sergi Marí, Rebeca Arauzo, Jokin de Miguel, Bárbara P. González-García, Nora Fernandez-Jimenez, Jose Ramon Bilbao, and Iraia García-Santisteban. 2021. "Genetic Contribution of Endometriosis to the Risk of Developing Hormone-Related Cancers" International Journal of Molecular Sciences 22, no. 11: 6083. https://doi.org/10.3390/ijms22116083
APA StyleRueda-Martínez, A., Garitazelaia, A., Cilleros-Portet, A., Marí, S., Arauzo, R., de Miguel, J., González-García, B. P., Fernandez-Jimenez, N., Bilbao, J. R., & García-Santisteban, I. (2021). Genetic Contribution of Endometriosis to the Risk of Developing Hormone-Related Cancers. International Journal of Molecular Sciences, 22(11), 6083. https://doi.org/10.3390/ijms22116083