Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events




 ,
, 
Abstract
1. Introduction
2. Results
2.1. Main Plasma Parameters of PAD Patients
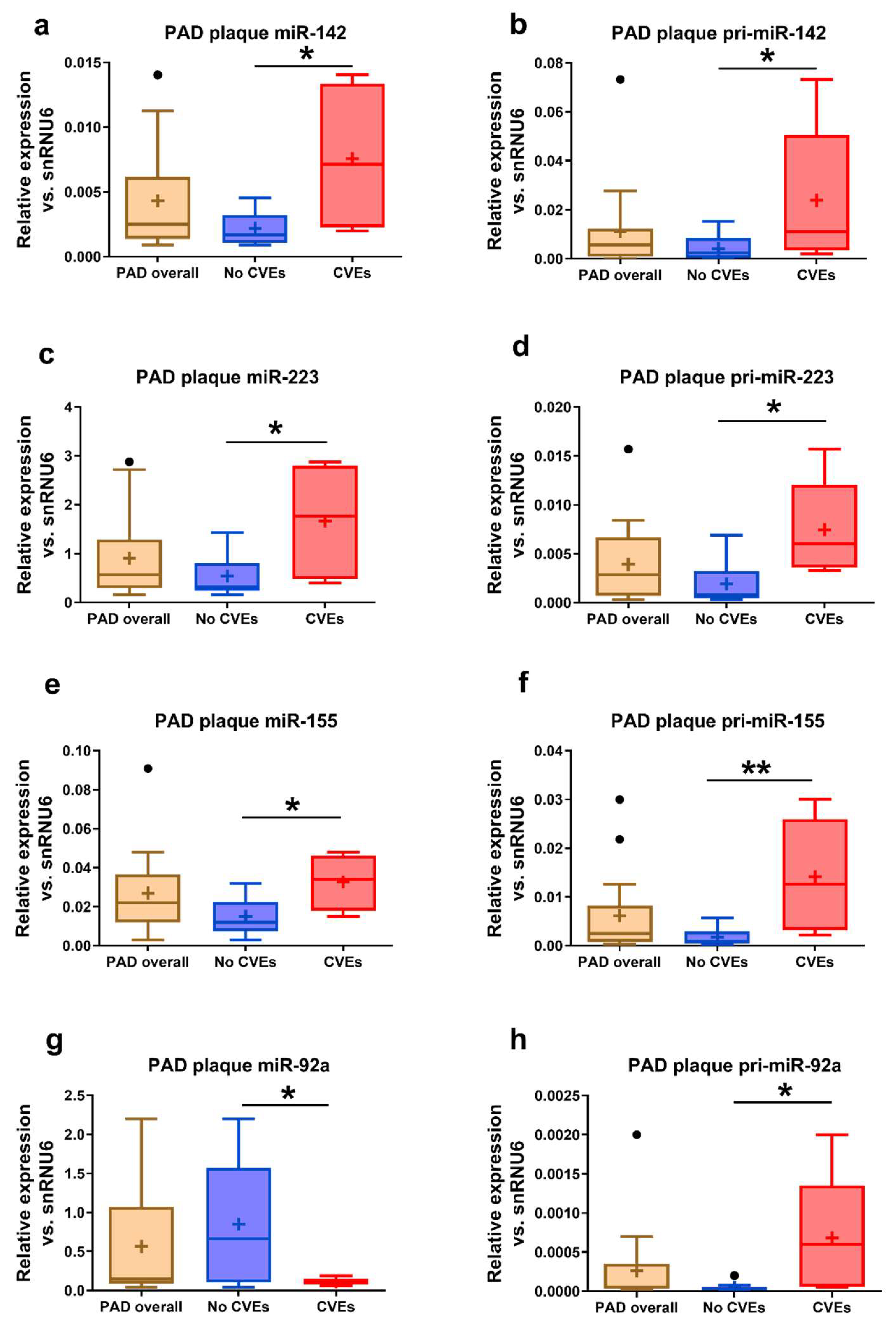
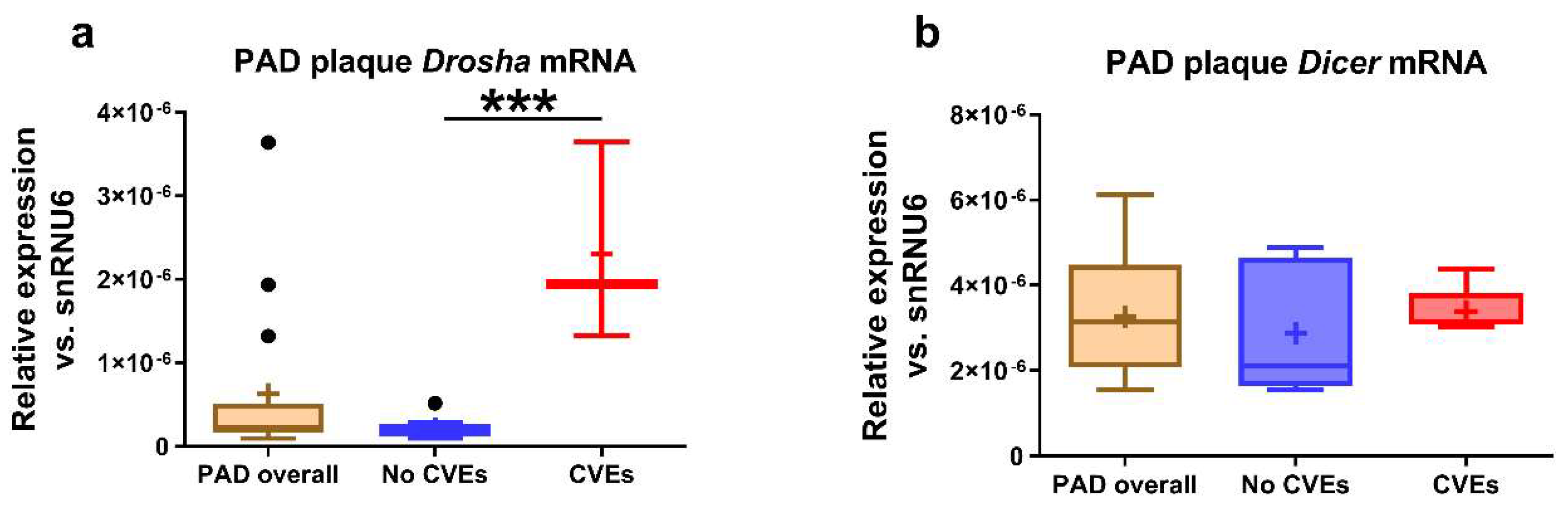
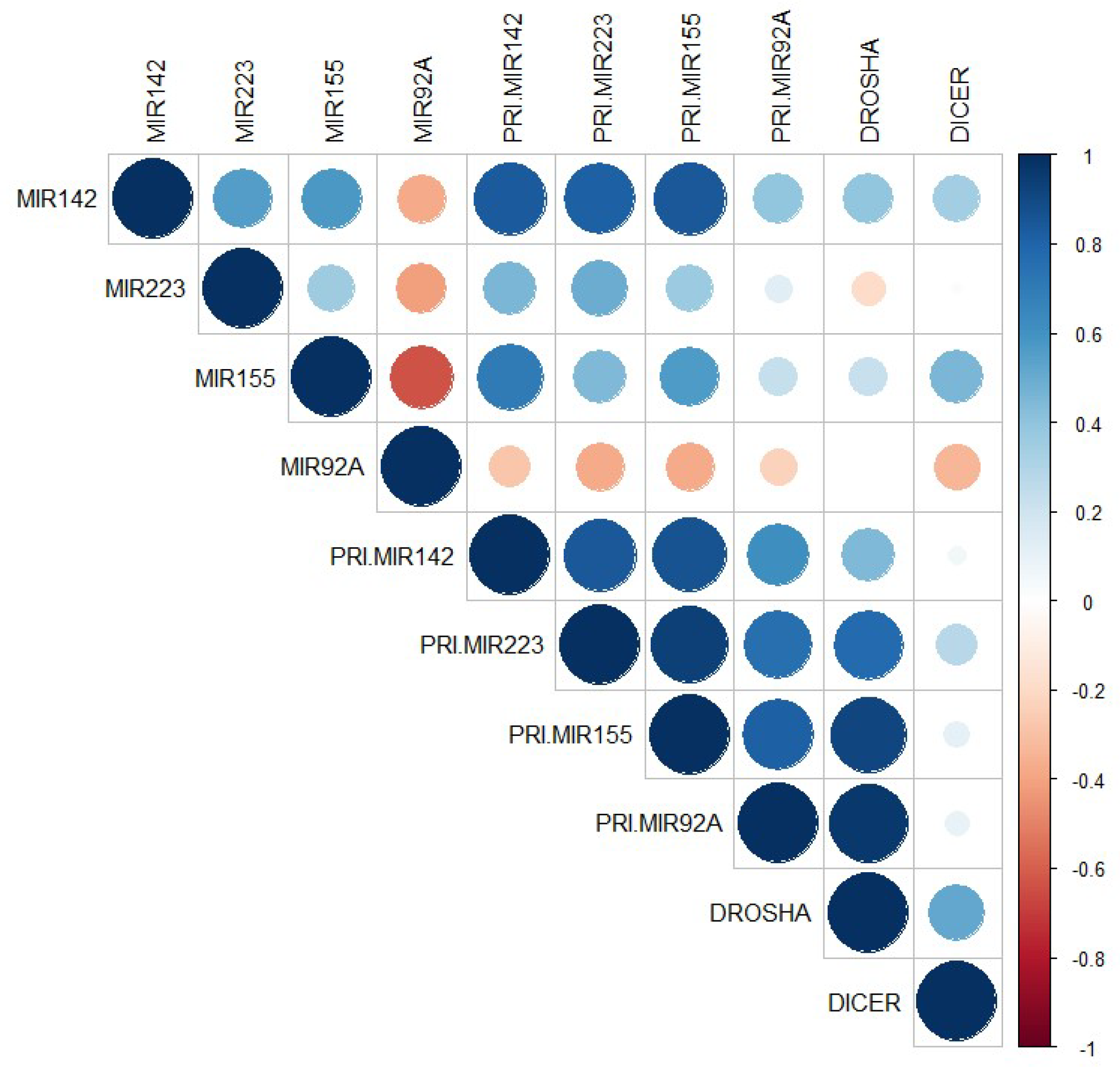
2.2. MiRNA, pri-miRNA, and mRNA Expressions in the Atherosclerotic Plaques Collected from the Femoral Arteries of PAD Patients
2.3. miRNA Levels in the Plasma of PAD Patients
2.4. Associations of Plasma miRNAs Levels with CVEs in Post-Surgery PAD Patients
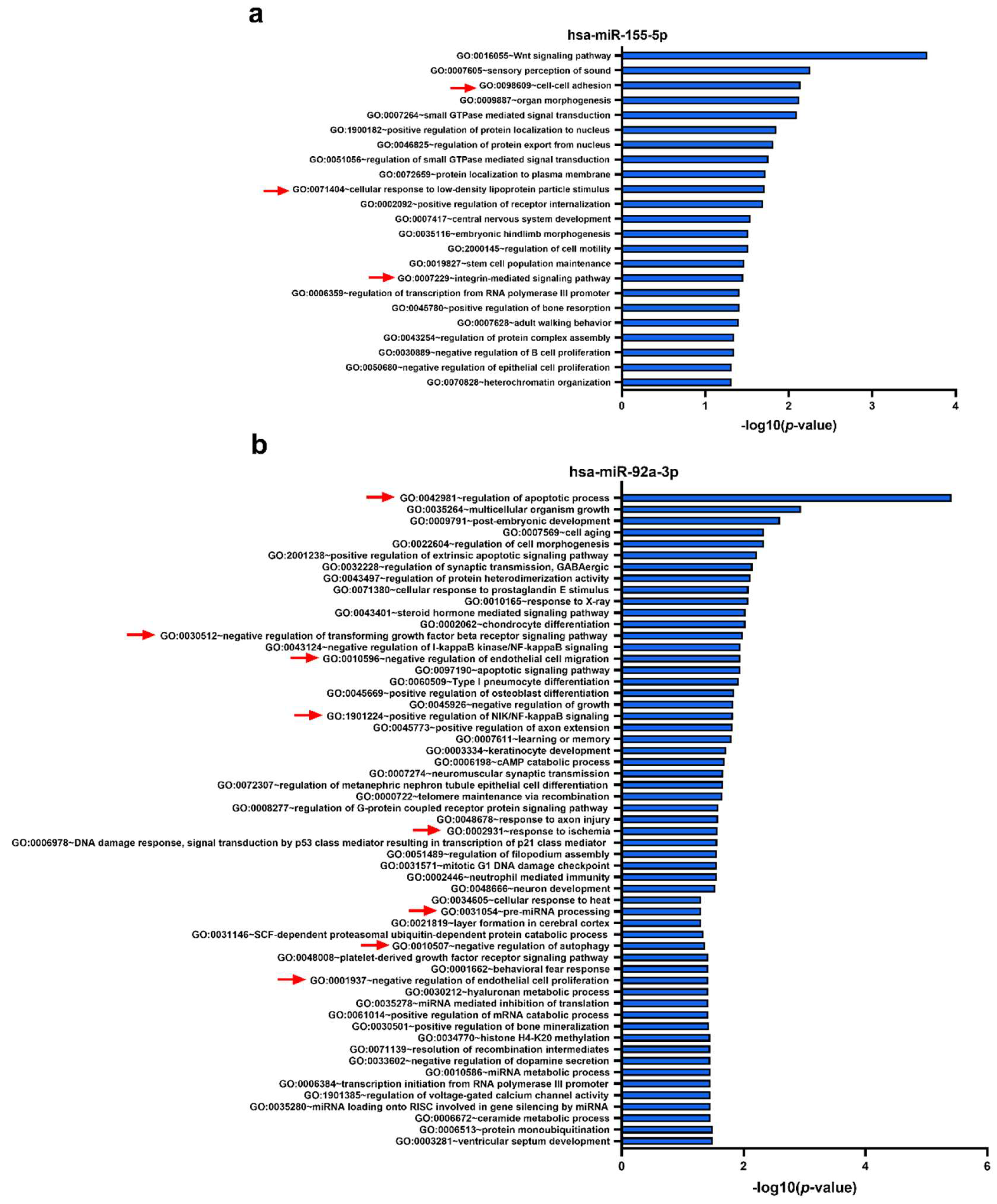
2.5. Functional Analyses—Gene Ontology (GO) Biological Processes Targeted by the Set of Four miRNAs
3. Discussion
4. Materials and Methods
4.1. Study Design and Subjects
4.2. Determination of Plasma Parameters
4.3. Analysis of microRNA in the Plasma and Atherosclerotic Plaques
4.4. Functional Analysis of miRNAs
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | alanine transaminase |
| APOA-I | apolipoprotein A-I |
| APOE | apolipoprotein E |
| AST | aspartate transaminase |
| BLR | binary logistic regression |
| BMI | body mass index |
| CAD | coronary artery disease |
| CP | ceruloplasmin |
| CRP | C-reactive protein |
| CVEs | cardiovascular events |
| DAVID | Database for Annotation, Visualization, and Integrated Discovery |
| EC | endothelial cell |
| GO | Gene Ontology |
| HDL | high-density lipoprotein |
| LDL | low-density lipoprotein |
| LDH | lactate dehydrogenase |
| miRNA | microRNA |
| MLR | multiple linear regression |
| MPO | myeloperoxidase |
| mRNA | messenger RNA |
| PAD | peripheral artery disease |
| PON1 | paraoxonase 1 |
| ROC | receiver operator characteristic |
| SEM | standard error of the mean |
| TC | total cholesterol |
| TG | triglyceride |
References
- Altesha, M.A.; Ni, T.; Khan, A.; Liu, K.; Zheng, X. Circular RNA in cardiovascular disease. J. Cell. Physiol. 2019, 234, 5588–5600. [Google Scholar] [CrossRef]
- Schaftenaar, F.; Frodermann, V.; Kuiper, J.; Lutgens, E. Atherosclerosis: The interplay between lipids and immune cells. Curr. Opin. Lipidol. 2016, 27, 209–215. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Bauersachs, R.; Zeymer, U.; Briere, J.B.; Marre, C.; Bowrin, K.; Huelsebeck, M. Burden of Coronary Artery Disease and Peripheral Artery Disease: A Literature Review. Cardiovasc. Ther. 2019, 2019, 8295054. [Google Scholar] [CrossRef] [PubMed]
- Campia, U.; Gerhard-Herman, M.; Piazza, G.; Goldhaber, S.Z. Peripheral Artery Disease: Past, Present, and Future. Am. J. Med. 2019, 132, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Manfrini, O.; Amaduzzi, P.L.; Cenko, E.; Bugiardini, R. Prognostic implications of peripheral artery disease in coronary artery disease. Curr. Opin. Pharmacol. 2018, 39, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Gregory, R.I. MicroRNA biogenesis pathways in cancer. Nat. Rev. Cancer 2015, 15, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Rupaimoole, R.; Slack, F.J. MicroRNA therapeutics: Towards a new era for the management of cancer and other diseases. Nat. Rev. Drug Discov. 2017, 16, 203–222. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wan, X.; Ruan, Q. The MicroRNA-21 in Autoimmune Diseases. Int. J. Mol. Sci. 2016, 17, 864. [Google Scholar] [CrossRef]
- Yan, L.; Liang, M.; Hou, X.; Zhang, Y.; Zhang, H.; Guo, Z.; Jinyu, J.; Feng, Z.; Mei, Z. The role of microRNA-16 in the pathogenesis of autoimmune diseases: A comprehensive review. Biomed. Pharmacother. 2019, 112, 108583. [Google Scholar] [CrossRef]
- Vogiatzi, G.; Oikonomou, E.; Deftereos, S.; Siasos, G.; Tousoulis, D. Peripheral artery disease: A micro-RNA-related condition? Curr. Opin. Pharmacol. 2018, 39, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Devaux, Y.; Vausort, M.; Goretti, E.; Nazarov, P.V.; Azuaje, F.; Gilson, G.; Corsten, M.F.; Schroen, B.; Lair, M.L.; Heymans, S.; et al. Use of circulating microRNAs to diagnose acute myocardial infarction. Clin. Chem. 2012, 58, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Parahuleva, M.S.; Lipps, C.; Parviz, B.; Holschermann, H.; Schieffer, B.; Schulz, R.; Euler, G. MicroRNA expression profile of human advanced coronary atherosclerotic plaques. Sci. Rep. 2018, 8, 7823. [Google Scholar] [CrossRef] [PubMed]
- Raitoharju, E.; Lyytikainen, L.P.; Levula, M.; Oksala, N.; Mennander, A.; Tarkka, M.; Klopp, N.; Illig, T.; Kahonen, M.; Karhunen, P.J.; et al. miR-21, miR-210, miR-34a, and miR-146a/b are up-regulated in human atherosclerotic plaques in the Tampere Vascular Study. Atherosclerosis 2011, 219, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.J.; Lei, H.P.; Wu, H.; Chen, J.Y.; Deng, C.Y.; Sheng, W.S.; Fu, Y.H.; Li, X.H.; Lin, Y.B.; Han, Y.L.; et al. Plasma miR-142 predicts major adverse cardiovascular events as an intermediate biomarker of dual antiplatelet therapy. Acta Pharmacol. Sin. 2019, 40, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.K.; Ma, J. Alteration in microRNA-155 level correspond to severity of coronary heart disease. Scand. J. Clin. Lab. Investig. 2018, 78, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Bruen, R.; Fitzsimons, S.; Belton, O. miR-155 in the Resolution of Atherosclerosis. Front. Pharmacol. 2019, 10, 463. [Google Scholar] [CrossRef]
- Jeffries, J.; Zhou, W.; Hsu, A.Y.; Deng, Q. miRNA-223 at the crossroads of inflammation and cancer. Cancer Lett. 2019, 451, 136–141. [Google Scholar] [CrossRef]
- Michell, D.L.; Vickers, K.C. Lipoprotein carriers of microRNAs. Biochim. Biophys. Acta 2016, 1861, 2069–2074. [Google Scholar] [CrossRef]
- Singh, S.; de Ronde, M.W.J.; Kok, M.G.M.; Beijk, M.A.; De Winter, R.J.; van der Wal, A.C.; Sondermeijer, B.M.; Meijers, J.C.M.; Creemers, E.E.; Pinto-Sietsma, S.J. MiR-223-3p and miR-122-5p as circulating biomarkers for plaque instability. Open Heart 2020, 7, e001223. [Google Scholar] [CrossRef]
- Chang, Y.J.; Li, Y.S.; Wu, C.C.; Wang, K.C.; Huang, T.C.; Chen, Z.; Chien, S. Extracellular MicroRNA-92a Mediates Endothelial Cell-Macrophage Communication. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 2492–2504. [Google Scholar] [CrossRef] [PubMed]
- Simionescu, N.; Niculescu, L.S.; Carnuta, M.G.; Sanda, G.M.; Stancu, C.S.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; Simionescu, M.; et al. Hyperglycemia Determines Increased Specific MicroRNAs Levels in Sera and HDL of Acute Coronary Syndrome Patients and Stimulates MicroRNAs Production in Human Macrophages. PLoS ONE 2016, 11, e0161201. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Bi, C.; Song, J.; Wang, L.; Ge, C.; Liu, X.; Zhang, M. Upregulation of miR-142-5p in atherosclerotic plaques and regulation of oxidized low-density lipoprotein-induced apoptosis in macrophages. Mol. Med. Rep. 2015, 11, 3229–3234. [Google Scholar] [CrossRef] [PubMed]
- Zhan, L.; Lei, S.; Li, W.; Zhang, Y.; Wang, H.; Shi, Y.; Tian, Y. Suppression of microRNA-142-5p attenuates hypoxia-induced apoptosis through targeting SIRT7. Biomed. Pharmacother. 2017, 94, 394–401. [Google Scholar] [CrossRef]
- Wu, W.; Shang, Y.; Dai, S.; Yu, C.; Wang, J. Downregulation of miR1425p inhibits human aortic smooth muscle cell proliferation and migration by targeting MKL2. Mol. Med. Rep. 2020, 22, 277–285. [Google Scholar] [CrossRef]
- Kee, H.J.; Park, S.; Kwon, J.S.; Choe, N.; Ahn, Y.; Kook, H.; Jeong, M.H. B cell translocation gene, a direct target of miR-142-5p, inhibits vascular smooth muscle cell proliferation by down-regulating cell cycle progression. FEBS Lett. 2013, 587, 2385–2392. [Google Scholar] [CrossRef]
- Qin, B.; Shu, Y.; Long, L.; Li, H.; Men, X.; Feng, L.; Yang, H.; Lu, Z. MicroRNA-142-3p Induces Atherosclerosis-Associated Endothelial Cell Apoptosis by Directly Targeting Rictor. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2018, 47, 1589–1603. [Google Scholar] [CrossRef]
- Tabet, F.; Vickers, K.C.; Cuesta Torres, L.F.; Wiese, C.B.; Shoucri, B.M.; Lambert, G.; Catherinet, C.; Prado-Lourenco, L.; Levin, M.G.; Thacker, S.; et al. HDL-transferred microRNA-223 regulates ICAM-1 expression in endothelial cells. Nat. Commun. 2014, 5, 3292. [Google Scholar] [CrossRef]
- Pan, Y.; Liang, H.; Liu, H.; Li, D.; Chen, X.; Li, L.; Zhang, C.Y.; Zen, K. Platelet-secreted microRNA-223 promotes endothelial cell apoptosis induced by advanced glycation end products via targeting the insulin-like growth factor 1 receptor. J. Immunol. 2014, 192, 437–446. [Google Scholar] [CrossRef]
- Wang, Y.; Ouyang, M.; Wang, Q.; Jian, Z. MicroRNA-142-3p inhibits hypoxia/reoxygenationinduced apoptosis and fibrosis of cardiomyocytes by targeting high mobility group box 1. Int. J. Mol. Med. 2016, 38, 1377–1386. [Google Scholar] [CrossRef]
- Vickers, K.C.; Landstreet, S.R.; Levin, M.G.; Shoucri, B.M.; Toth, C.L.; Taylor, R.C.; Palmisano, B.T.; Tabet, F.; Cui, H.L.; Rye, K.A.; et al. MicroRNA-223 coordinates cholesterol homeostasis. Proc. Natl. Acad. Sci. USA 2014, 111, 14518–14523. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Chen, H.; Ren, J.; Geng, Q.; Song, J.; Lee, C.; Cao, C.; Zhang, J.; Xu, N. MicroRNA-223 inhibits tissue factor expression in vascular endothelial cells. Atherosclerosis 2014, 237, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.; Nair, A.S.; Dhar, P.K. Computational study of ‘HUB’ microRNA in human cardiac diseases. Bioinformation 2017, 13, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kong, D.; Chen, H.; Liu, S.; Hu, H.; Wu, T.; Wang, J.; Chen, W.; Ning, Y.; Li, Y.; et al. miR-155 acts as an anti-inflammatory factor in atherosclerosis-associated foam cell formation by repressing calcium-regulated heat stable protein 1. Sci. Rep. 2016, 6, 21789. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.F.; Yang, L.X.; Guo, R.W.; Liu, H.; Shi, Y.K.; Ye, J.S.; Yang, Z.H. microRNA-155 is inversely associated with severity of coronary stenotic lesions calculated by the Gensini score. Coron. Artery Dis. 2014, 25, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Loyer, X.; Potteaux, S.; Vion, A.C.; Guerin, C.L.; Boulkroun, S.; Rautou, P.E.; Ramkhelawon, B.; Esposito, B.; Dalloz, M.; Paul, J.L.; et al. Inhibition of microRNA-92a prevents endothelial dysfunction and atherosclerosis in mice. Circ. Res. 2014, 114, 434–443. [Google Scholar] [CrossRef]
- Iaconetti, C.; Polimeni, A.; Sorrentino, S.; Sabatino, J.; Pironti, G.; Esposito, G.; Curcio, A.; Indolfi, C. Inhibition of miR-92a increases endothelial proliferation and migration in vitro as well as reduces neointimal proliferation in vivo after vascular injury. Basic Res. Cardiol. 2012, 107, 296. [Google Scholar] [CrossRef]
- Stojkovic, S.; Jurisic, M.; Kopp, C.W.; Koppensteiner, R.; Huber, K.; Wojta, J.; Gremmel, T. Circulating microRNAs identify patients at increased risk of in-stent restenosis after peripheral angioplasty with stent implantation. Atherosclerosis 2018, 269, 197–203. [Google Scholar] [CrossRef]
- Luo, T.; Cui, S.; Bian, C.; Yu, X. Crosstalk between TGF-beta/Smad3 and BMP/BMPR2 signaling pathways via miR-17-92 cluster in carotid artery restenosis. Mol. Cell. Biochem. 2014, 389, 169–176. [Google Scholar] [CrossRef]
- Bonauer, A.; Carmona, G.; Iwasaki, M.; Mione, M.; Koyanagi, M.; Fischer, A.; Burchfield, J.; Fox, H.; Doebele, C.; Ohtani, K.; et al. MicroRNA-92a controls angiogenesis and functional recovery of ischemic tissues in mice. Science 2009, 324, 1710–1713. [Google Scholar] [CrossRef]
- Daniel, J.M.; Penzkofer, D.; Teske, R.; Dutzmann, J.; Koch, A.; Bielenberg, W.; Bonauer, A.; Boon, R.A.; Fischer, A.; Bauersachs, J.; et al. Inhibition of miR-92a improves re-endothelialization and prevents neointima formation following vascular injury. Cardiovasc. Res. 2014, 103, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Sotgia, S.; Porcu, P.; Casu, M.A.; Bivona, G.; Chessa, R.; Deiana, L.; Carru, C. Carotid restenosis is associated with plasma ADMA concentrations in carotid endarterectomy patients. Clin. Chem. Lab. Med. 2011, 49, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, O.; Shih, D.M.; Aviram, M. Paraoxonase 1 (PON1) attenuates macrophage oxidative status: Studies in PON1 transfected cells and in PON1 transgenic mice. Atherosclerosis 2005, 181, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Niculescu, L.S.; Simionescu, N.; Sanda, G.M.; Carnuta, M.G.; Stancu, C.S.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; Simionescu, M.; et al. MiR-486 and miR-92a Identified in Circulating HDL Discriminate between Stable and Vulnerable Coronary Artery Disease Patients. PLoS ONE 2015, 10, e0140958. [Google Scholar] [CrossRef] [PubMed]
- Sticht, C.; De La Torre, C.; Parveen, A.; Gretz, N. miRWalk: An online resource for prediction of microRNA binding sites. PLoS ONE 2018, 13, e0206239. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.W.; Sherman, B.T.; Lempicki, R.A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat. Protoc. 2009, 4, 44–57. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall (n = 47) | No CVEs (n = 35) | CVEs (n = 12) | p-Value |
|---|---|---|---|---|
| Age (years) | 63.5 ± 1.42 | 63.7 ± 1.74 | 62.9 ± 2.42 | 0.797 |
| Gender (men, %) | 43 (91.5) | 31 (88.6) | 12 (100) | 0.221 |
| Hypertension, n (%) | 35 (74.5) | 27 (77.1) | 8 (66.7) | 0.765 |
| Hyperglycemia, n (%) | 17 (36.2) | 11 (31.4) | 6 (50) | 0.187 |
| Dyslipidemia, n (%) | 38 (80.8) | 30 (85.7) | 8 (66.7) | 0.322 |
| Coronary artery disease, n (%) | 22 (46.8) | 17 (48.6) | 5 (41.6) | 0.857 |
| BMI (kg/m2) | 26.1 ± 0.92 | 26.9 ± 1.01 | 22.9 ± 1.38 | 0.052 |
| TC (mg/dL) | 175.7 ± 6.54 | 176.8 ± 7.75 | 172.1 ± 12.45 | 0.756 |
| TG (mg/dL) | 129.7 ± 8.98 | 125.0 ± 9.48 | 149.2 ± 24.53 | 0.420 |
| Glucose (mg/dL) | 116.2 ± 4.56 | 116.0 ± 5.41 | 117.0 ± 8.48 | 0.604 |
| LDL-C (mg/dL) | 106.6 ± 5.63 | 109.9 ± 6.60 | 92.9 ± 8.50 | 0.236 |
| HDL-C (mg/dL) | 42.7 ± 1.54 | 43.6 ± 1.83 | 39.2 ± 2.4 | 0.297 |
| HDL-C/LDL-C ratio | 0.447 ± 0.028 | 0.446 ± 0.032 | 0.453 ± 0.062 | 0.559 |
| APOA-I (mg/dL) | 109.94 ± 9.30 | 117.8 ± 10.38 | 72.7 ± 15.0 | 0.028 * |
| APOE (mg/dL) | 2.02 ± 0.17 | 2.00 ± 0.19 | 2.11 ± 0.46 | 0.836 |
| APOA-I/APOE ratio | 65.2 ± 5.96 | 70.3 ± 6.72 | 42.5 ± 8.81 | 0.025 * |
| PON1 (µg/mL) | 1.68 ± 0.15 | 1.71 ± 0.17 | 1.26 ± 0.34 | 0.433 |
| PON1 activity paraoxon (U/L) | 263.5 ± 38.16 | 315.5 ± 43.46 | 143.2 ± 61.84 | 0.046 * |
| MPO (ng/mL) | 48.14 ± 6.49 | 45.7 ± 7.87 | 57.6 ± 9.69 | 0.645 |
| MPO activity (fmoles/min/mL) | 226.0 ± 38.70 | 226.0 ± 49.10 | 255.0 ± 39.97 | 0.326 |
| CP (µg/mL) | 693.7 ± 43.15 | 626.7 ± 29.95 | 931.8 ± 144.78 | 0.002 * |
| CRP (mg/dL) | 5.86 ± 1.60 | 4.27 ± 1.42 | 10.11 ± 4.28 | 0.022 * |
| LDH (U/L) | 168.1 ± 14.41 | 164.9 ± 13.31 | 179.1 ± 47.37 | 0.539 |
| AST (U/L) | 24.91 ± 1.94 | 24.27 ± 1.24 | 26.67 ± 6.63 | 0.274 |
| ALT (U/L) | 21.24 ± 1.30 | 21.18 ± 1.36 | 22.08 ± 3.24 | 0.990 |
| Age (years) | 63.5 ± 1.42 | 63.7 ± 1.74 | 62.9 ± 2.42 | 0.797 |
| MLR | miR-142-3p | miR-223-3p | miR-155-5p | miR-92a-3p | ||||
|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | |
| Model 1—Clinical data | ||||||||
| Age | −0.054 | 0.891 | −0.921 | 0.325 | 0.203 | 0.700 | 0.135 | 0.846 |
| Gender | 0.323 | 0.117 | 0.429 | 0.375 | 0.132 | 0.629 | 0.370 | 0.306 |
| BMI | 0.908 | 0.025 | 0.423 | 0.651 | 0.393 | 0.456 | 0.760 | 0.277 |
| Obesity | −0.023 | 0.745 | −0.200 | 0.235 | −0.090 | 0.347 | −0.121 | 0.335 |
| Hypertension | 0.092 | 0.484 | 0.365 | 0.244 | −0.023 | 0.895 | 0.366 | 0.119 |
| Dyslipidemia | −0.329 | 0.045 | −0.079 | 0.837 | 0.210 | 0.332 | −0.949 | 0.002 |
| Hyperglycemia | −0.038 | 0.632 | 0.274 | 0.151 | −0.014 | 0.897 | −0.079 | 0.578 |
| R2 (p-value) | 0.845 (1.0 × 10−13) | 0.132 (0.414) | 0.723 (1.9 × 10−11) | 0.517 (5.6 × 10−6) | ||||
| Model 2—Blood lipids | ||||||||
| TC | 0.584 | 0.002 | −0.286 | 0.482 | 0.252 | 0.271 | 0.407 | 0.252 |
| TG | 0.045 | 0.770 | 0.012 | 0.972 | 0.083 | 0.675 | 0.100 | 0.745 |
| HDL-C/LDL-C | 0.376 | 0.012 | 1.007 | 0.004 | 0.588 | 0.003 | 0.278 | 0.343 |
| APOA-I/APOE | −0.057 | 0.679 | −0.476 | 0.135 | −0.030 | 0.866 | −0.147 | 0.594 |
| R2 (p-value) | 0.850 (1.0 × 10−13) | 0.206 (0.018) | 0.751 (1.1 × 10−13) | 0.396 (2.9 × 10−5) | ||||
| Model 3—Oxidative and inflammatory parameters | ||||||||
| PON1 | 0.300 | 0.044 | 0.121 | 0.739 | 0.325 | 0.132 | 0.088 | 0.760 |
| PON1 activity | −0.171 | 0.179 | −0.116 | 0.711 | −0.024 | 0.896 | −0.097 | 0.697 |
| MPO | 0.130 | 0.266 | 0.056 | 0.847 | −0.034 | 0.842 | 0.572 | 0.015 |
| MPO activity | 0.052 | 0.675 | −0.100 | 0.744 | 0.094 | 0.600 | 0.030 | 0.903 |
| CP | 0.645 | 9.4 × 10−6 | 0.123 | 0.706 | 0.340 | 0.081 | 0.166 | 0.523 |
| CRP | 0.095 | 0.349 | 0.182 | 0.470 | 0.276 | 0.066 | 0.017 | 0.933 |
| R2 (p-value) | 0.714 (1.9 × 10−17) | 0.159 (0.764) | 0.671 (1.02 × 10−9) | 0.401 (5.4 × 10−4) | ||||
| Model 4—Other parameters | ||||||||
| LDH | 0.556 | 2.3 × 10−5 | −0.202 | 0.487 | 0.453 | 0.009 | 0.316 | 0.217 |
| AST | 0.077 | 0.568 | −0.286 | 0.378 | 0.100 | 0.595 | −0.132 | 0.641 |
| ALT | 0.324 | 0.018 | 0.766 | 0.020 | 0.323 | 0.088 | 0.412 | 0.148 |
| R2 (p-value) | 0.853 (1.0 × 10−13) | 0.147 (0.039) | 0.712 (1.4 × 10−13) | 0.344 (6.2 × 10−5) | ||||
| Parameter | Wald χ2 Value | p-Value | OR (95% CI) | Model χ2 Value | Model p-Value |
|---|---|---|---|---|---|
| Model 1 | |||||
| Plasma miR-142 | 4.58 | 0.032 | 1.1 × 106 (3.25 − 3.78 × 101) | 24.75 | 5.65 × 10−5 |
| Plasma miR-223 | 1.87 | 0.171 | 3.7 × 10−2 (3.26 × 10−4 − 4.17) | ||
| Plasma miR-155 | 0.86 | 0.354 | 8.2 × 10−2 (4.20 × 10−4 − 16.17) | ||
| Plasma miR-92a | 5.29 | 0.021 | 4.0 × 10−3 (3.70 × 10−5 − 0.44) | ||
| Model 2 | |||||
| Plasma miR-142 | 3.19 | 0.034 | 6.9 × 106 (0.221 − 2.20 × 1014) | 25.47 | 2.80 × 10−4 |
| Plasma miR-223 | 1.57 | 0.210 | 9.7 × 10−3 (6.95 × 10−6 − 13.54) | ||
| Plasma miR-155 | 1.15 | 0.282 | 3.9 × 10−2 (1.05 × 10−4 − 14.47) | ||
| Plasma miR-92a | 3.97 | 0.046 | 2.2 × 10−3 (5.41 × 10−6 − 0.90) | ||
| Age | 0.22 | 0.635 | 1.05 (0.847 − 1.31) | ||
| Gender | 0.15 | 0.699 | 5.34 (1.10 × 10−3 − 2.60 × 104) | ||
| Area Under the Curve | |||||
|---|---|---|---|---|---|
| Test Result Variable(s) * | Area | SE a | Asymptotic Sig. b | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||
| Plasma miR-142 | 0.861 | 0.068 | 0.007 | 0.727 | 0.995 |
| Plasma miR-223 | 0.451 | 0.124 | 0.717 | 0.207 | 0.695 |
| Plasma miR-155 | 0.632 | 0.152 | 0.325 | 0.335 | 0.929 |
| Plasma miR-92a | 0.396 | 0.099 | 0.437 | 0.202 | 0.589 |
| All plasma miRNAs | 0.924 | 0.050 | 0.002 | 0.825 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbalata, T.; Moraru, O.E.; Stancu, C.S.; Devaux, Y.; Simionescu, M.; Sima, A.V.; Niculescu, L.S. Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events. Int. J. Mol. Sci. 2020, 21, 9600. https://doi.org/10.3390/ijms21249600
Barbalata T, Moraru OE, Stancu CS, Devaux Y, Simionescu M, Sima AV, Niculescu LS. Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events. International Journal of Molecular Sciences. 2020; 21(24):9600. https://doi.org/10.3390/ijms21249600
Chicago/Turabian StyleBarbalata, Teodora, Oriana E. Moraru, Camelia S. Stancu, Yvan Devaux, Maya Simionescu, Anca V. Sima, and Loredan S. Niculescu. 2020. "Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events" International Journal of Molecular Sciences 21, no. 24: 9600. https://doi.org/10.3390/ijms21249600
APA StyleBarbalata, T., Moraru, O. E., Stancu, C. S., Devaux, Y., Simionescu, M., Sima, A. V., & Niculescu, L. S. (2020). Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events. International Journal of Molecular Sciences, 21(24), 9600. https://doi.org/10.3390/ijms21249600