Improved Detection of Antibodies against SARS-CoV-2 by Microsphere-Based Antibody Assay

 ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Results
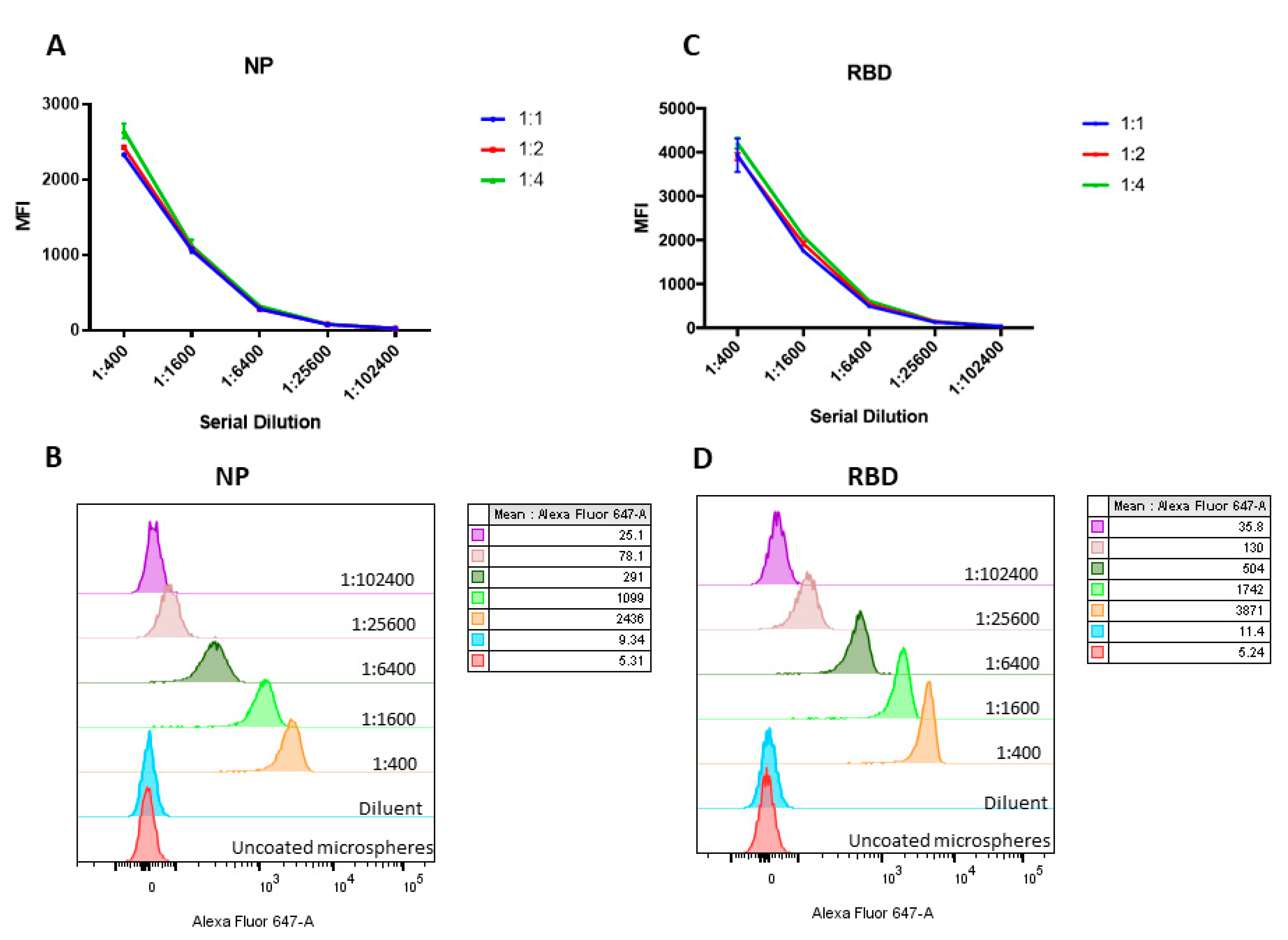
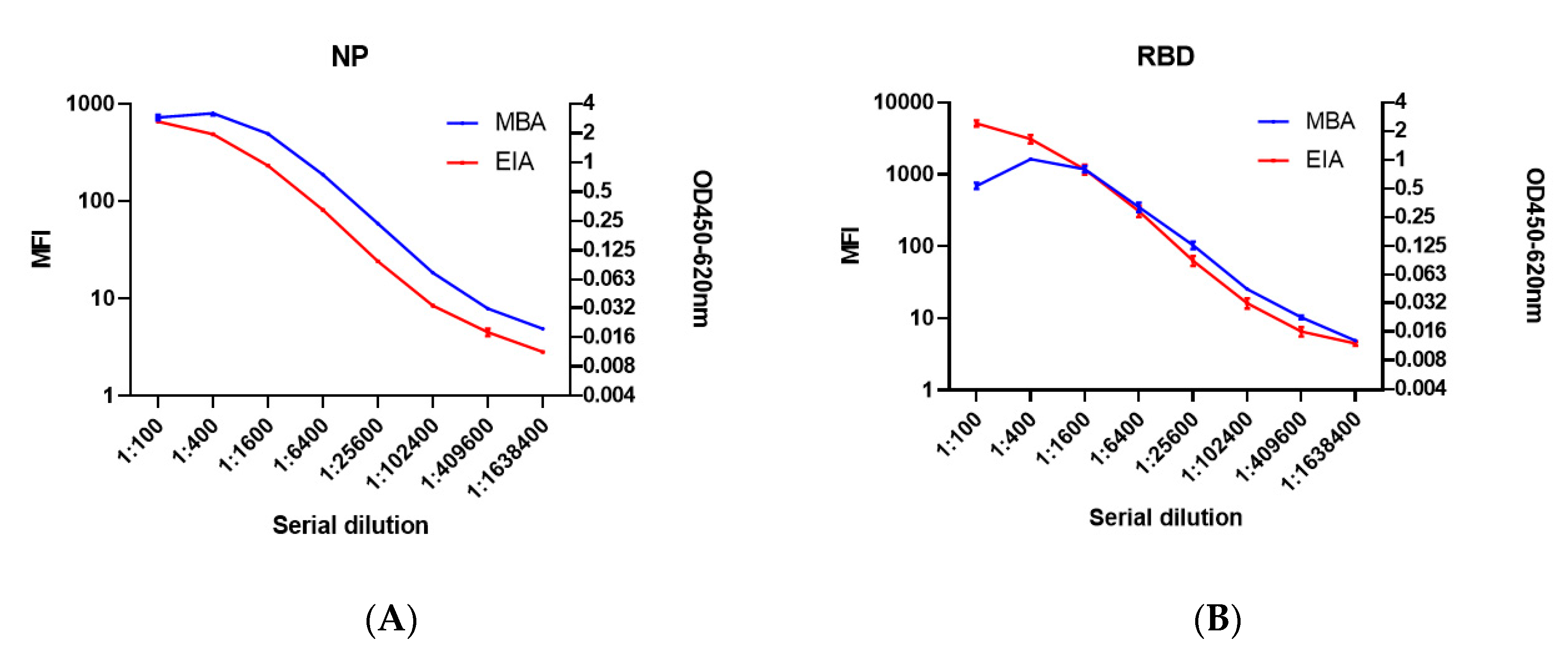
2.1. Establishing the MBA
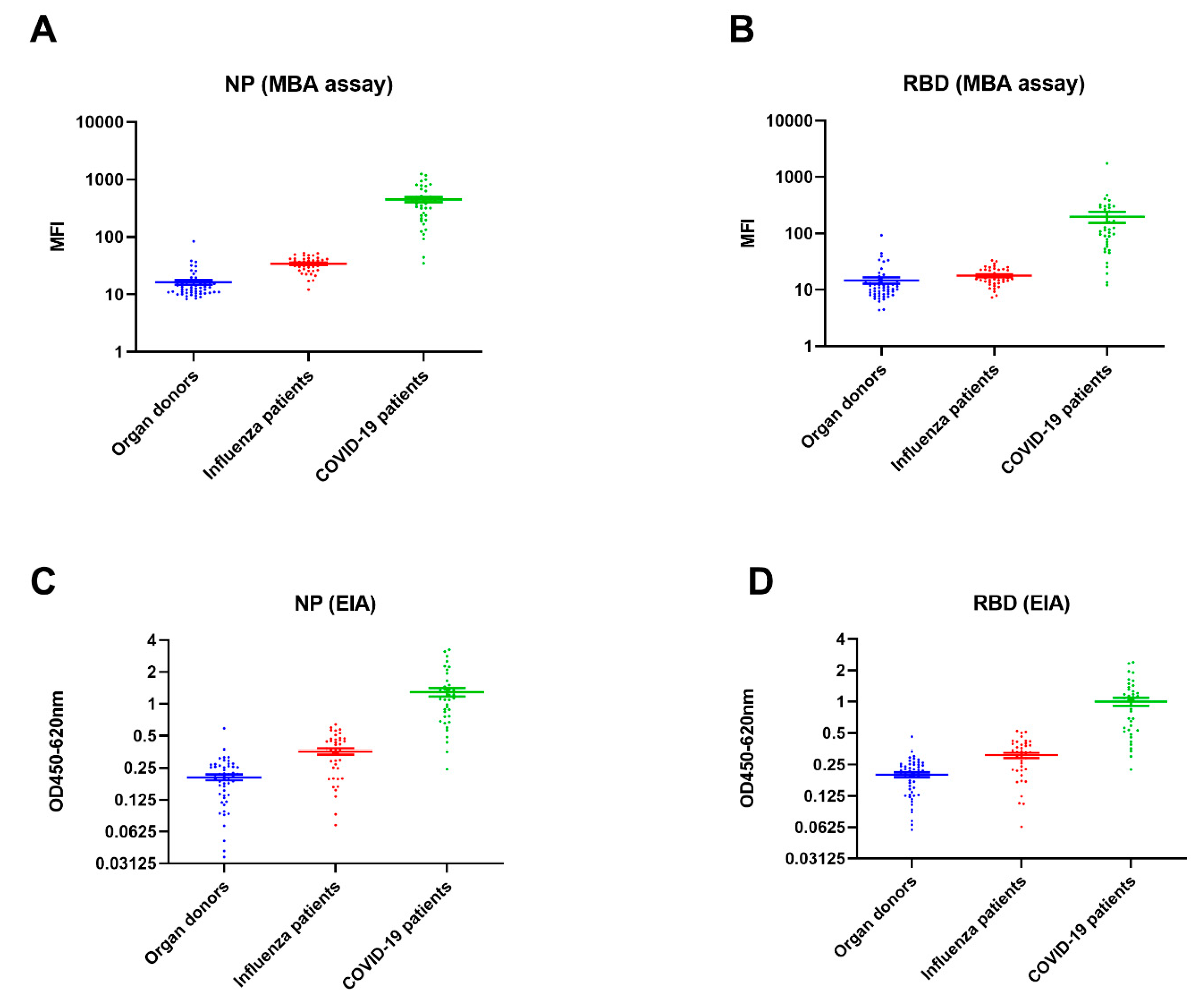
2.2. Seropositive Rate and Time-To-Seropositivity
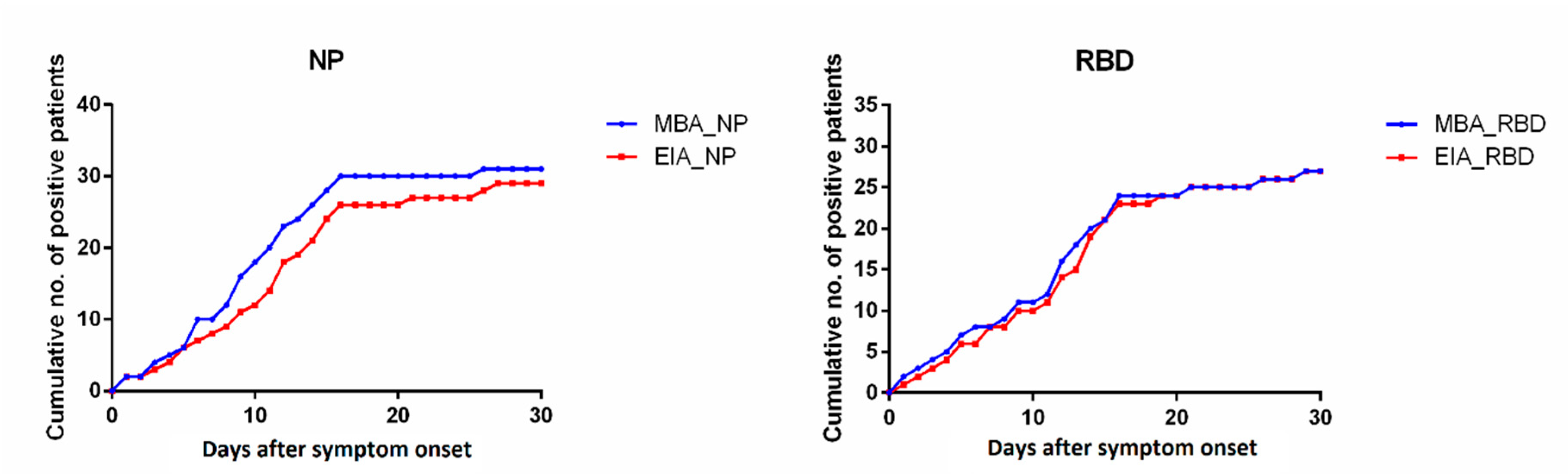
2.3. Time-To-Seropositivity
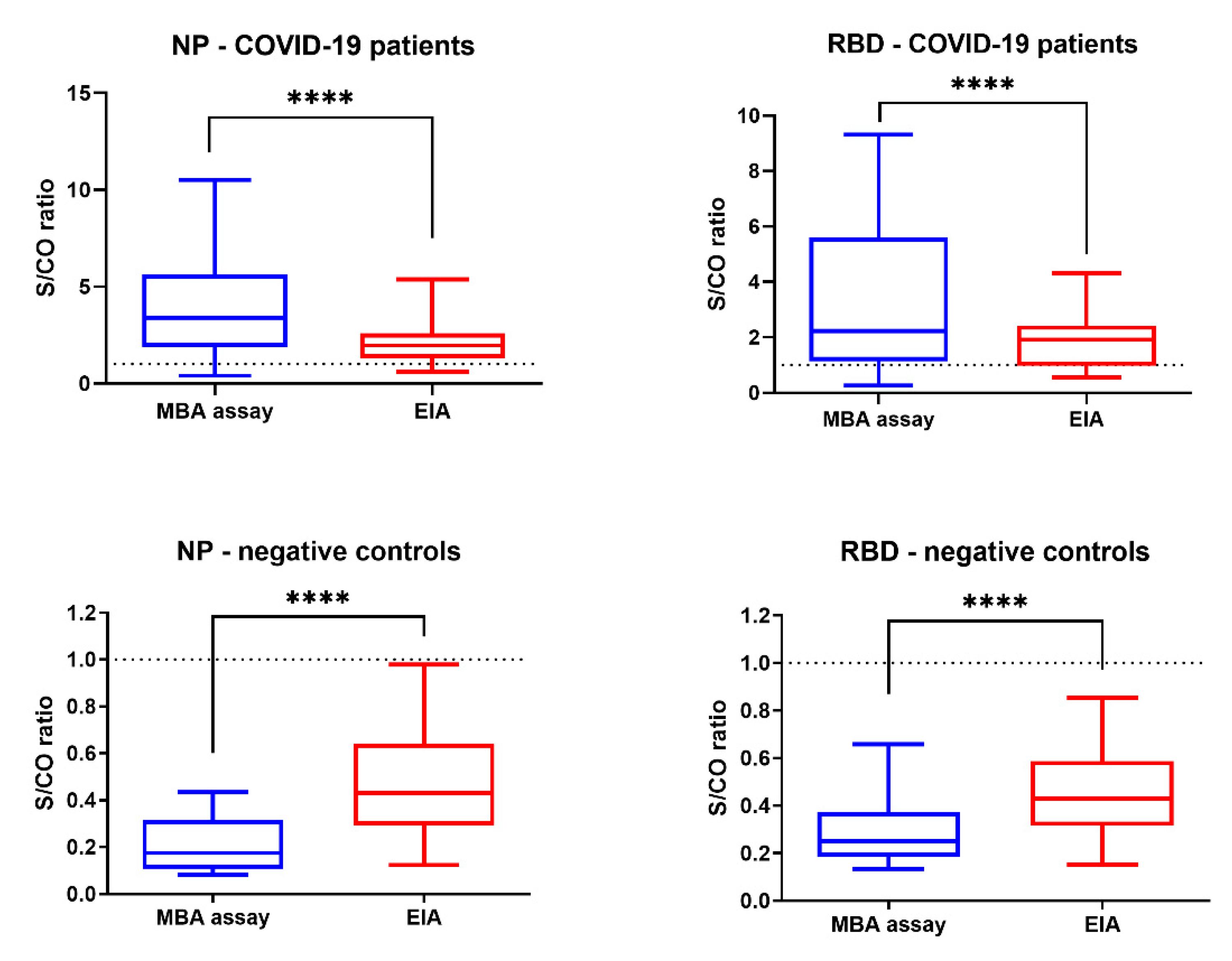
2.4. Comparison of S/CO
3. Discussion
3.1. Principle Outcomes
3.2. Comparison with Other Studies
3.3. Limitations of This Study
3.4. Conclusions and Implications for Clinical Practice and Research Studies
4. Materials and Methods
4.1. Serum Specimens
4.2. Cloning, Purification and Biotinylation of Recombinant NP and Spike Protein RBD of SARS-CoV-2
4.3. Enzyme Immunoassay for NP and Spike RBD
4.4. Microsphere-Based Antibody Assay
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| MBA | Microsphere-based antibody assay |
| EIA | Enzyme immunoassay |
| SARS-CoV | Severe acute respiratory syndrome coronavirus |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| NP | SARS-CoV-2 nucleoprotein |
| RBD | Spike protein receptor binding domain |
| IgG | Immunoglobulin G |
| FBS | Fetal bovine serum |
| PBS | Phosphate-buffered saline |
| S/CO | Signal-to-cutoff |
| CI | Confidence interval |
| MFI | Mean fluorescent intensity |
References
- Peiris, J.S.M.; Lai, S.T.; Poon, L.L.M.; Guan, Y.; Yam, L.Y.C.; Lim, W.; Nicholls, J.; Yee, W.K.S.; Yan, W.W.; Cheung, M.T.; et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet 2003, 361, 1319–1325. [Google Scholar] [CrossRef]
- Cheng, V.C.; Lau, S.K.; Woo, P.C.; Yuen, K.Y. Severe acute respiratory syndrome coronavirus as an agent of emerging and reemerging infection. Clin. Microbiol. Rev. 2007, 20, 660–694. [Google Scholar] [CrossRef]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef]
- To, K.K.; Tsang, O.T.; Chik-Yan Yip, C.; Chan, K.H.; Wu, T.C.; Chan, J.M.C.; Leung, W.S.; Chik, T.S.; Choi, C.Y.; Kandamby, D.H.; et al. Consistent detection of 2019 novel coronavirus in saliva. Clin. Infect. Dis. 2020. [CrossRef]
- To, K.K.-W.; Cheng, V.C.-C.; Cai, J.; Chan, K.; Chen, L.; Wong, L.; Choi, C.Y.; Fong, C.H.; Ng, A.C.; Lu, L.; et al. Seroprevalence of SARS-CoV-2 in Hong Kong Special Administrative Region and our returnees evacuated from Hubei province of China: A multi-cohort study. Lancet Microbe 2020, 1, e111–e118. [Google Scholar] [CrossRef]
- Petherick, A. Developing antibody tests for SARS-CoV-2. Lancet 2020, 395, 1101–1102. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. 2020. [CrossRef]
- Okba, N.M.A.; Muller, M.A.; Li, W.; Wang, C.; GeurtsvanKessel, C.H.; Corman, V.M.; Lamers, M.M.; Sikkema, R.S.; de Bruin, E.; Chandler, F.D.; et al. Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibody Responses in Coronavirus Disease 2019 Patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.; Cai, J.P.; Chan, J.M.; Chik, T.S.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet. Infectious Diseases 2020, 20, 565–574. [Google Scholar] [CrossRef]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef]
- Zhang, Y.; Brooks, W.A.; Goswami, D.; Rahman, M.; Luby, S.P.; Erdman, D.D. A duplex recombinant viral nucleoprotein microbead immunoassay for simultaneous detection of seroresponses to human respiratory syncytial virus and metapneumovirus infections. J. Virol. Methods 2014, 206, 55–62. [Google Scholar] [CrossRef]
- Trivedi, S.U.; Miao, C.; Sanchez, J.E.; Caidi, H.; Tamin, A.; Haynes, L.; Thornburg, N.J. Development and Evaluation of a Multiplexed Immunoassay for Simultaneous Detection of Serum IgG Antibodies to Six Human Coronaviruses. Sci. Rep. 2019, 9, 1390. [Google Scholar] [CrossRef]
- Smits, G.P.; van Gageldonk, P.G.; Schouls, L.M.; van der Klis, F.R.; Berbers, G.A. Development of a bead-based multiplex immunoassay for simultaneous quantitative detection of IgG serum antibodies against measles, mumps, rubella, and varicella-zoster virus. Clin. Vaccine Immunol. 2012, 19, 396–400. [Google Scholar] [CrossRef]
- Basile, A.J.; Horiuchi, K.; Panella, A.J.; Laven, J.; Kosoy, O.; Lanciotti, R.S.; Venkateswaran, N.; Biggerstaff, B.J. Multiplex microsphere immunoassays for the detection of IgM and IgG to arboviral diseases. PLoS ONE 2013, 8, e75670. [Google Scholar] [CrossRef]
- Rogier, E.W.; Moss, D.M.; Mace, K.E.; Chang, M.; Jean, S.E.; Bullard, S.M.; Lammie, P.J.; Lemoine, J.F.; Udhayakumar, V. Use of Bead-Based Serologic Assay to Evaluate Chikungunya Virus Epidemic, Haiti. Emerg. Infect. Dis. 2018, 24, 995–1001. [Google Scholar] [CrossRef]
- Kranz, L.M.; Gartner, B.; Michel, A.; Pawlita, M.; Waterboer, T.; Brenner, N. Development and validation of HIV-1 Multiplex Serology. J. Immunol. Methods 2019, 466, 47–51. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Imai, K.; Takiko, T.; Ikeda, M.; Noguchi, S.; Kitagawa, Y.; Matuoka, M.; Miyoshi, K.; Tarumoto, N.; Sakai, J.; Ito, T.; et al. Clinical evaluation of an immunochromatographic IgM/IgG antibody assay and chest computed tomography for the diagnosis of COVID-19. J. Clin. Virol. 2020, 128, 104393. [Google Scholar] [CrossRef]
- Abbasi, J. The Promise and Peril of Antibody Testing for COVID-19. JAMA 2020, 323, 1881–1883. [Google Scholar] [CrossRef]
- Demey, B.; Daher, N.; François, C.; Lanoix, J.P.; Duverlie, G.; Castelain, S.; Brochot, E. Dynamic profile for the detection of anti-SARS-CoV-2 antibodies using four immunochromatographic assays. J. Infect. 2020, 81, e6–e10. [Google Scholar] [CrossRef]
- Perera, R.A.; Mok, C.K.; Tsang, O.T.; Lv, H.; Ko, R.L.; Wu, N.C.; Yuan, M.; Leung, W.S.; Chan, J.M.; Chik, T.S.; et al. Serological assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), March 2020. Euro Surveill. Bull. Eur. Mal. Trans. Eur. Commun. Dis. Bull. 2020, 25, 2000421. [Google Scholar] [CrossRef]
- Chen, L.L.; Wu, W.L.; Chan, W.M.; Fong, C.H.Y.; Ng, A.C.K.; Ip, J.D.; Lu, L.; Dissanayake, T.K.; Ding, X.; Cai, J.P.; et al. Assessment of population susceptibility to upcoming seasonal influenza epidemic strain using interepidemic emerging influenza virus strains. Epidemiol. Infect. 2019, 147, e279. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specimens Collected at Out-Patient Clinic (n = 39) | Negative Controls (Organ Donors + Influenza Patients) (n-93) | |||
|---|---|---|---|---|
| MBA | NP | RBD | NP | RBD |
| S/CO > 1.1 | 34 (87.2%) | 29 (74.4%) | 0 | 1 (1.1%) |
| S/CO 0-9-1.1 | 2 (5.1%) | 5 (12.8%) | 0 | 1 (1.1%) |
| S/CO < 0.9 | 3 (7.7%) | 5 (12.8%) | 93 (100%) | 91 (97.8%) |
| EIA | NP | RBD | NP | RBD |
| S/CO > 1.1 | 32 (82.1%) | 26 (66.7%) | 0 | 0 |
| S/CO 0-9-1.1 | 3 (7.7%) | 6 (15.4%) | 8 (8.6%) | 5 (12.8%) |
| S/CO < 0.9 | 4 (10.3%) | 7 (18%) | 85 (91.4%) | 88 (94.6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fong, C.H.-Y.; Cai, J.-P.; Dissanayake, T.K.; Chen, L.-L.; Choi, C.Y.-K.; Wong, L.-H.; Ng, A.C.-K.; Pang, P.K.P.; Ho, D.T.-Y.; Poon, R.W.-S.; et al. Improved Detection of Antibodies against SARS-CoV-2 by Microsphere-Based Antibody Assay. Int. J. Mol. Sci. 2020, 21, 6595. https://doi.org/10.3390/ijms21186595
Fong CH-Y, Cai J-P, Dissanayake TK, Chen L-L, Choi CY-K, Wong L-H, Ng AC-K, Pang PKP, Ho DT-Y, Poon RW-S, et al. Improved Detection of Antibodies against SARS-CoV-2 by Microsphere-Based Antibody Assay. International Journal of Molecular Sciences. 2020; 21(18):6595. https://doi.org/10.3390/ijms21186595
Chicago/Turabian StyleFong, Carol Ho-Yan, Jian-Piao Cai, Thrimendra Kaushika Dissanayake, Lin-Lei Chen, Charlotte Yee-Ki Choi, Lok-Hin Wong, Anthony Chin-Ki Ng, Polly K. P. Pang, Deborah Tip-Yin Ho, Rosana Wing-Shan Poon, and et al. 2020. "Improved Detection of Antibodies against SARS-CoV-2 by Microsphere-Based Antibody Assay" International Journal of Molecular Sciences 21, no. 18: 6595. https://doi.org/10.3390/ijms21186595
APA StyleFong, C. H.-Y., Cai, J.-P., Dissanayake, T. K., Chen, L.-L., Choi, C. Y.-K., Wong, L.-H., Ng, A. C.-K., Pang, P. K. P., Ho, D. T.-Y., Poon, R. W.-S., Chung, T. W.-H., Sridhar, S., Chan, K.-H., Chan, J. F.-W., Hung, I. F.-N., Yuen, K.-Y., & To, K. K.-W. (2020). Improved Detection of Antibodies against SARS-CoV-2 by Microsphere-Based Antibody Assay. International Journal of Molecular Sciences, 21(18), 6595. https://doi.org/10.3390/ijms21186595