Sleep, Autonomic Nervous Function and Atherosclerosis


Abstract
1. Introduction
2. Sleep and Atherosclerosis
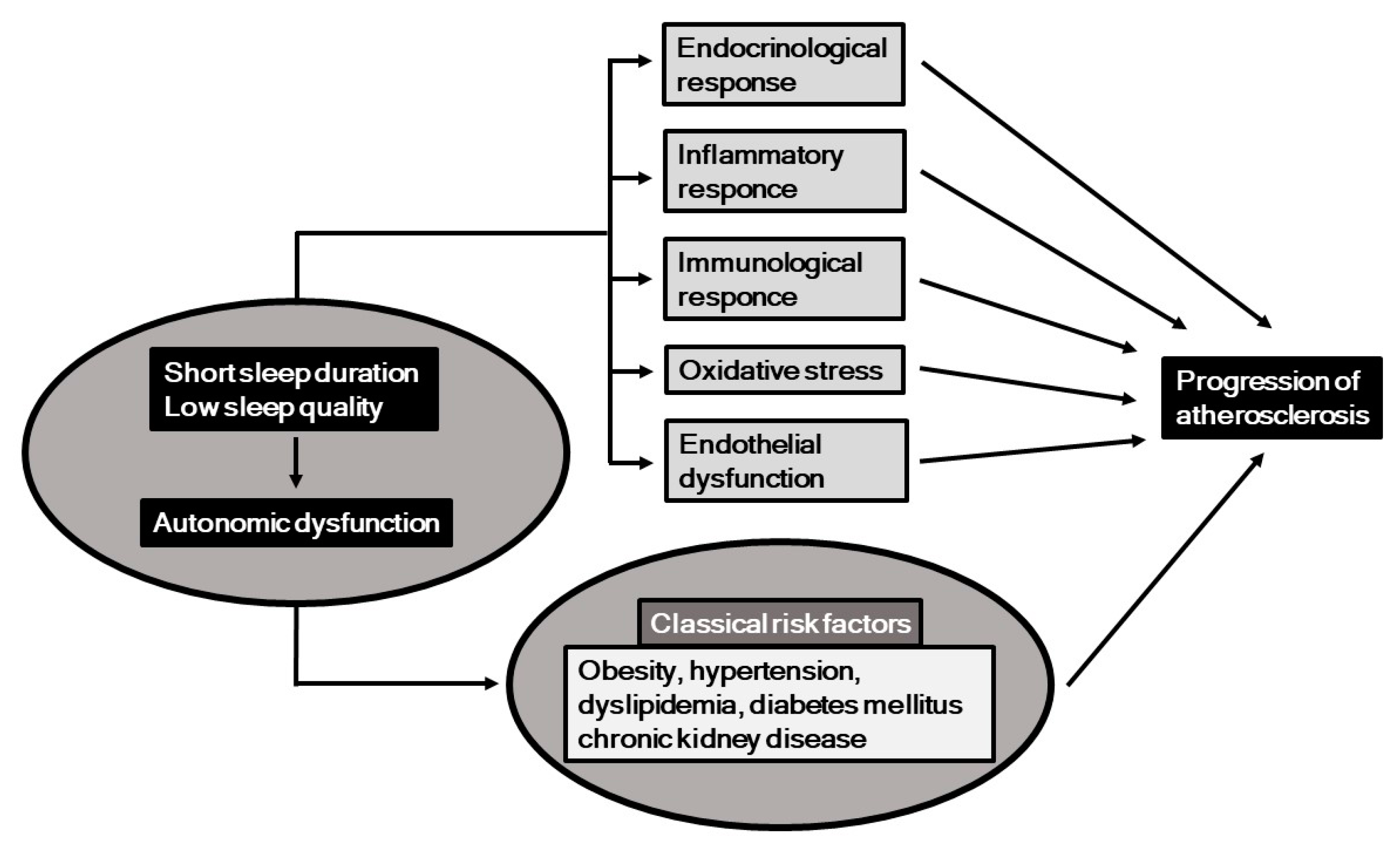
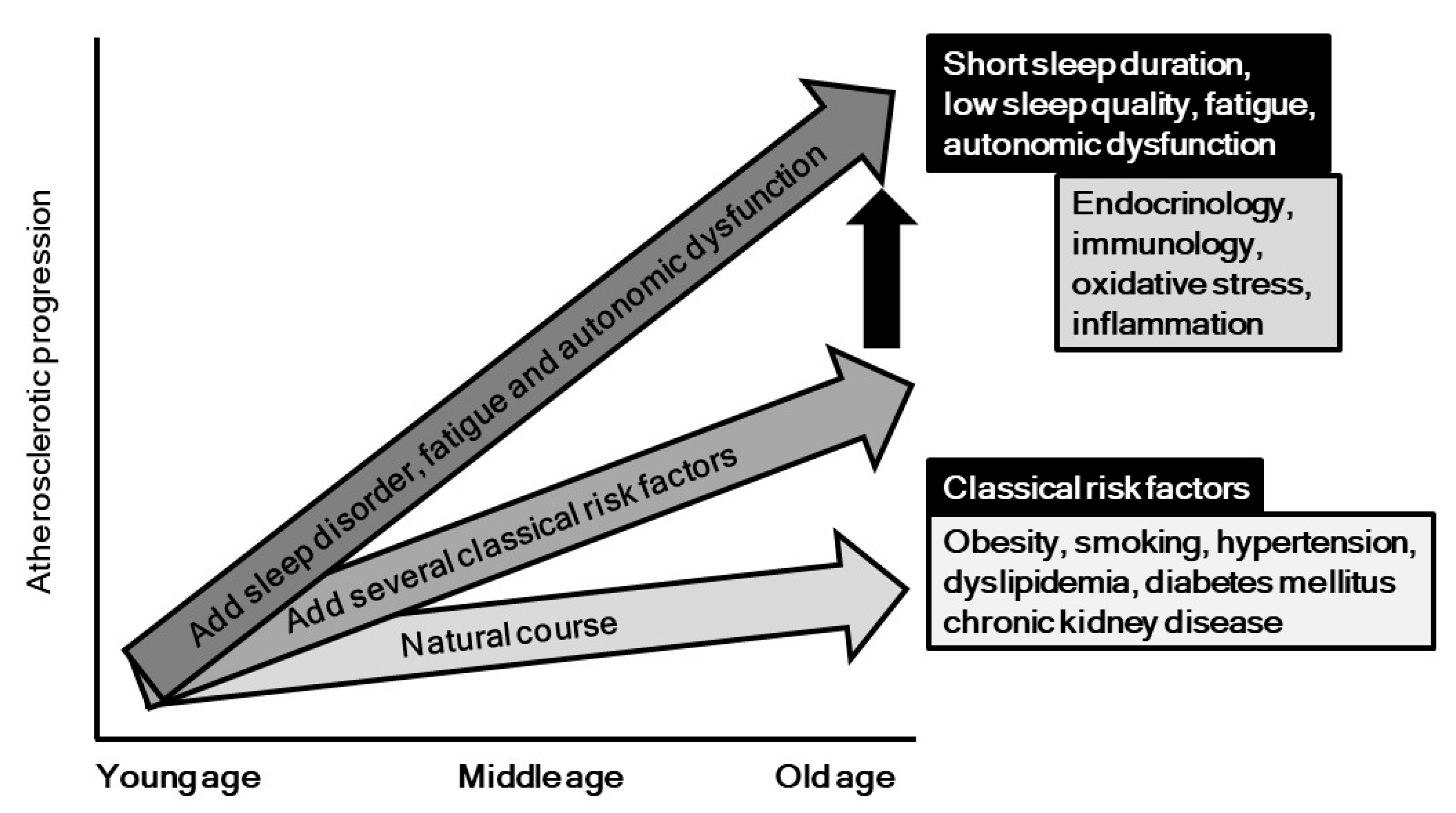
3. Potential Mechanisms underlying Association of Sleep with Atherosclerosis Progression
4. Autonomic Nervous Function and Atherosclerosis
5. Potential Mechanisms underlying Association of Autonomic Nervous Dysfunction and Progression of Atherosclerosis
6. Fatigue, Atherosclerosis and Cardiovascular Diseases
7. Conclusions and Perspectives
Funding
Acknowledgments
Conflicts of Interest
References
- Fujiyoshi, A.; Ohkubo, T.; Miura, K.; Murakami, Y.; Nagasawa, S.Y.; Okamura, T.; Ueshima, H. Observational Cohorts in Japan Research group. Blood pressure categories and long-term risk of cardiovascular disease according to age group in Japanese men and women. Hypertens. Res. 2012, 35, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Doi, Y.; Arima, H.; Yonemoto, K.; Hata, J.; Kubo, M.; Tanizaki, Y.; Ibayashi, S.; Iida, M.; Kiyohara, Y. LDL cholesterol and the development of stroke subtypes and coronary heart disease in a general Japanese population: The Hisayama study. Stroke 2009, 40, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, S.; Okamura, T.; Hozawa, A.; Kadowaki, T.; Kadota, A.; Murakami, Y.; Nakamura, K.; Saitoh, S.; Nakamura, Y.; Hayakawa, T.; et al. Relationship of elevated casual blood glucose level with coronary heart disease, cardiovascular disease and all-cause mortality in a representative sample of the Japanese population. NIPPON DATA80. Diabetologia 2008, 51, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Krantz, D.S.; Sheps, D.S.; Carney, R.M.; Natelson, B.H. Effects of mental stress in patients with coronary artery disease: Evidence and clinical implications. JAMA 2000, 283, 1800–1802. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Castro-Diehl, C.; Diez Roux, A.V.; Redline, S.; Seeman, T.; McKinley, P.; Sloan, R.; Shea, S. Sleep Duration and Quality in Relation to Autonomic Nervous System Measures: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2016, 39, 1927–1940. [Google Scholar] [CrossRef]
- Tsuji, H.; Larson, M.G.; Venditti, F.J., Jr.; Manders, E.S.; Evans, J.C.; Feldman, C.L.; Levy, D. Impact of reduced heart rate variability on risk for cardiac events. The Framingham Heart Study. Circulation 1996, 94, 2850–2855. [Google Scholar] [CrossRef]
- Buysse, D.J.; Hall, M.L.; Strollo, P.J.; Kamarck, T.W.; Owens, J.; Lee, L.; Reis, S.E.; Matthews, K.A. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J. Clin. Sleep Med. 2008, 4, 563–5671. [Google Scholar]
- Practice parameters for the use of actigraphy in the clinical assessment of sleep disorders. American Sleep Disorders Association. Sleep 1995, 18, 285–287. [CrossRef]
- Chen, C.Y.; Chen, C.L.; Yu, C.C. Obstructive sleep apnea is independently associated with arterial stiffness in ischemic stroke patients. J. Neurol. 2015, 262, 1247–1254. [Google Scholar] [CrossRef]
- Kadoya, M.; Koyama, H.; Kurajoh, M.; Kanzaki, A.; Kakutani-Hatayama, M.; Okazaki, H.; Shoji, T.; Moriwaki, Y.; Yamamoto, T.; Emoto, M.; et al. Sleep, cardiac autonomic function, and carotid atherosclerosis in patients with cardiovascular risks: HSCAA study. Atherosclerosis 2015, 238, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Low, P.A. Testing the autonomic nervous system. Semin. Neurol. 2003, 23, 407–421. [Google Scholar] [PubMed]
- Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [CrossRef]
- Polak, J.F.; Pencina, M.J.; Pencina, K.M.; O’Donnell, C.J.; Wolf, P.A.; D’Agostino, R.B., Sr. Carotid-wall intima-media thickness and cardiovascular events. N. Engl. J. Med. 2011, 365, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Kadoya, M.; Koyama, H.; Kanzaki, A.; Kurajoh, M.; Hatayama, M.; Shiraishi, J.; Okazaki, H.; Shoji, T.; Moriwaki, Y.; Yamamoto, T.; et al. Plasma brain-derived neurotrophic factor and reverse dipping pattern of nocturnal blood pressure in patients with cardiovascular risk factors. PLoS ONE 2014, 9, e105977. [Google Scholar] [CrossRef] [PubMed]
- Kadoya, M.; Koyama, H.; Kurajoh, M.; Naka, M.; Miyoshi, A.; Kanzaki, A.; Kakutani, M.; Shoji, T.; Moriwaki, Y.; Yamamoto, T.; et al. Associations of Sleep Quality and Awake Physical Activity with Fluctuations in Nocturnal Blood Pressure in Patients with Cardiovascular Risk Factors. PLoS ONE 2016, 11, e0155116. [Google Scholar] [CrossRef]
- Kadoya, M.; Kurajoh, M.; Kakutani-Hatayama, M.; Morimoto, A.; Miyoshi, A.; Kosaka-Hamamoto, K.; Shoji, T.; Moriwaki, Y.; Inaba, M.; Koyama, H. Low sleep quality is associated with progression of arterial stiffness in patients with cardiovascular risk factors: HSCAA study. Atherosclerosis 2018, 270, 95–101. [Google Scholar] [CrossRef]
- Nakazaki, C.; Noda, A.; Koike, Y.; Yamada, S.; Murohara, T.; Ozaki, N. Association of insomnia and short sleep duration with atherosclerosis risk in the elderly. Am. J. Hypertens. 2012, 25, 1149–1155. [Google Scholar]
- Nagai, M.; Hoshide, S.; Nishikawa, M.; Shimada, K.; Kario, K. Sleep duration and insomnia in the elderly: Associations with blood pressure variability and carotid artery remodeling. Am. J. Hypertens. 2013, 26, 981–989. [Google Scholar]
- Yoda, K.; Inaba, M.; Hamamoto, K.; Yoda, M.; Tsuda, A.; Mori, K.; Imanishi, Y.; Emoto, M.; Yamada, S. Association between poor glycemic control, impaired sleep quality, and increased arterial thickening in type 2 diabetic patients. PLoS ONE 2015, 10, e0122521. [Google Scholar] [CrossRef] [PubMed]
- Osonoi, Y.; Mita, T.; Osonoi, T.; Saito, M.; Tamasawa, A.; Nakayama, S.; Someya, Y.; Ishida, H.; Kanazawa, A.; Gosho, M.; et al. Poor sleep quality is associated with increased arterial stiffness in Japanese patients with type 2 diabetes mellitus. BMC Endocr. Disord. 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Sands, M.R.; Lauderdale, D.S.; Liu, K.; Knutson, K.L.; Matthews, K.A.; Eaton, C.B.; Linkletter, C.D.; Loucks, E.B. Short sleep duration is associated with carotid intima-media thickness among men in the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Stroke 2012, 43, 2858–2864. [Google Scholar] [CrossRef] [PubMed]
- Wolff, B.; Volzke, H.; Schwahn, C.; Robinson, D.; Kessler, C.; John, U. Relation of self-reported sleep duration with carotid intima-media thickness in a general population sample. Atherosclerosis 2008, 196, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Aoki, T.; Yata, S.; Okada, M. Sleep duration is significantly associated with carotid artery atherosclerosis incidence in a Japanese population. Atherosclerosis 2011, 217, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Giles, W.H.; Croft, J.B.; Bliwise, D.L. Habitual sleep patterns and risk for stroke and coronary heart disease: A 10-year follow-up from NHANES I. Neurology 1997, 48, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Burazeri, G.; Gofin, J.; Kark, J.D. Over 8 h of sleep-marker of increased mortality in Mediterranean population: Follow-up population study. Croat. Med. J. 2003, 44, 193–198. [Google Scholar]
- Kim, C.W.; Chang, Y.; Zhao, D.; Cainzos-Achirica, M.; Ryu, S.; Jung, H.S.; Yun, K.E.; Choi, Y.; Ahn, J.; Zhang, Y.; et al. Sleep Duration, Sleep Quality, and Markers of Subclinical Arterial Disease in Healthy Men and Women. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 2238–2245. [Google Scholar] [CrossRef]
- Yoshioka, E.; Saijo, Y.; Kita, T.; Okada, E.; Satoh, H.; Kawaharada, M.; Kishi, R. Relation between self-reported sleep duration and arterial stiffness: A cross-sectional study of middle-aged Japanese civil servants. Sleep 2011, 34, 1681–1686. [Google Scholar] [CrossRef]
- Tsai, T.C.; Wu, J.S.; Yang, Y.C.; Huang, Y.H.; Lu, F.H.; Chang, C.J. Long sleep duration associated with a higher risk of increased arterial stiffness in males. Sleep 2014, 37, 1315–1320. [Google Scholar] [CrossRef]
- Dominguez, F.; Fuster, V.; Fernandez-Alvira, J.M.; Fernandez-Friera, L.; Lopez-Melgar, B.; Blanco-Rojo, R.; Fernandez-Ortiz, A.; Garcia-Pavia, P.; Sanz, J.; Mendiguren, J.M.; et al. Association of Sleep Duration and Quality with Subclinical Atherosclerosis. J. Am. Coll. Cardiol. 2019, 73, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.D.; Ben-Shlomo, Y.; Beswick, A.; Yarnell, J.; Lightman, S.; Elwood, P. Cortisol, testosterone, and coronary heart disease: Prospective evidence from the Caerphilly study. Circulation 2005, 112, 332–340. [Google Scholar] [CrossRef]
- Lee, J.M.; Colangelo, L.A.; Schwartz, J.E.; Yano, Y.; Siscovick, D.S.; Seeman, T.; Schreiner, P.J.; Liu, K.J.; Lloyd-Jones, D.M.; Greenland, P. Associations of cortisol/testosterone and cortisol/sex hormone-binding globulin ratios with atherosclerosis in middle-age women. Atherosclerosis 2016, 248, 203–209. [Google Scholar] [CrossRef]
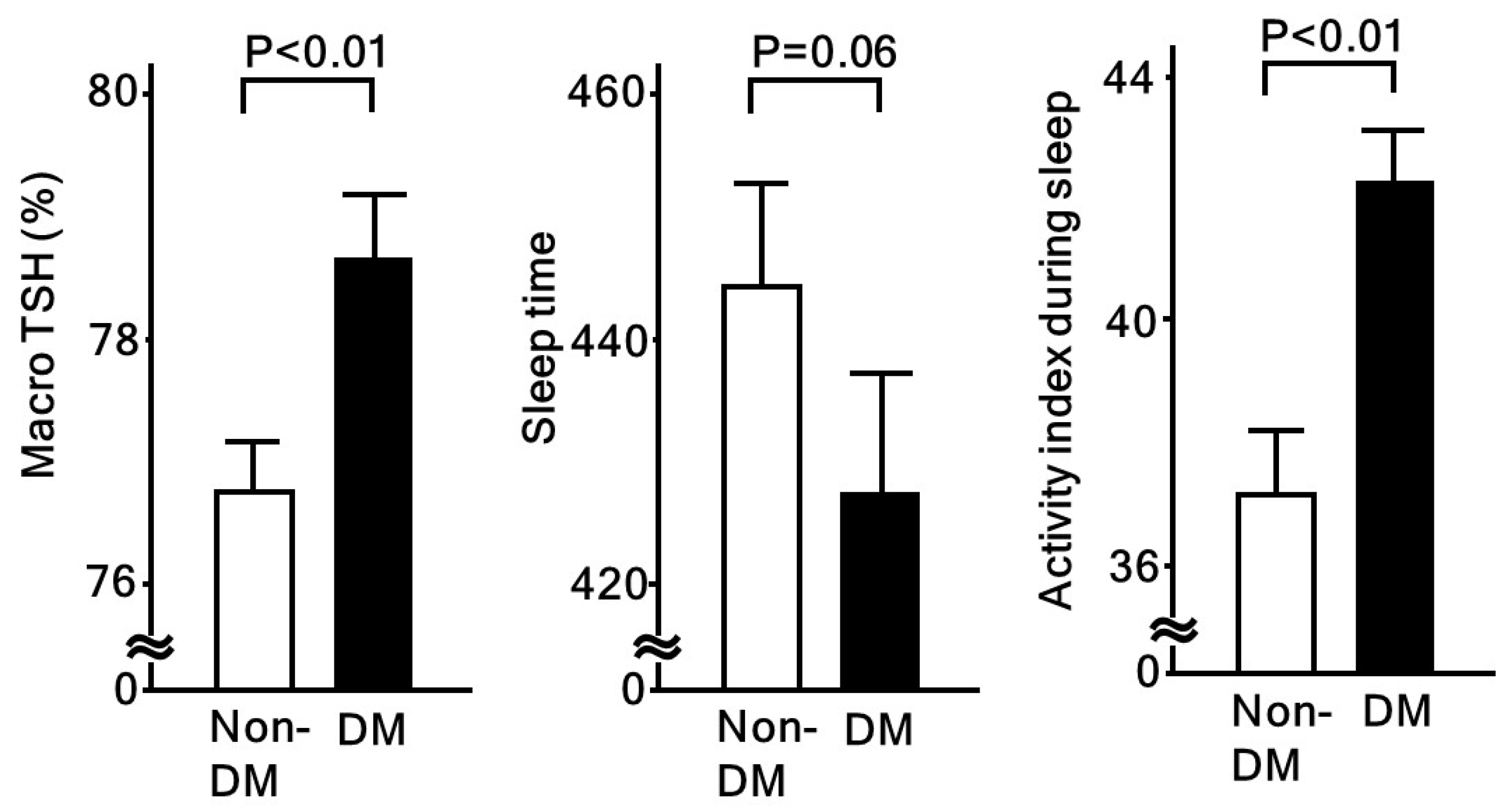
- Kadoya, M.; Koyama, S.; Morimoto, A.; Miyoshi, A.; Kakutani, M.; Hamamoto, K.; Kurajoh, M.; Shoji, T.; Moriwaki, Y.; Koshiba, M.; et al. Serum Macro TSH Level is Associated with Sleep Quality in Patients with Cardiovascular Risks—HSCAA Study. Sci. Rep. 2017, 7, 44387. [Google Scholar] [CrossRef] [PubMed]
- Cereda, C.W.; Tamisier, R.; Manconi, M.; Andreotti, J.; Frangi, J.; Pifferini, V.; Bassetti, C.L. Endothelial dysfunction and arterial stiffness in ischemic stroke: The role of sleep-disordered breathing. Stroke 2013, 44, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Chen, C.L.; Yu, C.C.; Chen, T.T.; Tseng, S.T.; Ho, C.H. Association of inflammation and oxidative stress with obstructive sleep apnea in ischemic stroke patients. Sleep Med. 2015, 16, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.; Stradling, J.R. Mechanisms of vascular damage in obstructive sleep apnea. Nat. Rev. Cardiol. 2010, 7, 677–685. [Google Scholar] [CrossRef]
- Everson, C.A. Clinical assessment of blood leukocytes, serum cytokines, and serum immunoglobulins as responses to sleep deprivation in laboratory rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, R1054–R1063. [Google Scholar] [CrossRef]
- Irwin, M.R.; Wang, M.; Campomayor, C.O.; Collado-Hidalgo, A.; Cole, S. Sleep deprivation and activation of morning levels of cellular and genomic markers of inflammation. Arch Intern. Med. 2006, 166, 1756–1762. [Google Scholar] [CrossRef]
- Yehuda, S.; Sredni, B.; Carasso, R.L.; Kenigsbuch-Sredni, D. REM sleep deprivation in rats results in inflammation and interleukin-17 elevation. J. Interferon Cytokine Res. 2009, 29, 393–398. [Google Scholar] [CrossRef]
- Carreras, A.; Zhang, S.X.; Peris, E.; Qiao, Z.; Gileles-Hillel, A.; Li, R.C.; Wang, Y.; Gozal, D. Chronic sleep fragmentation induces endothelial dysfunction and structural vascular changes in mice. Sleep 2014, 37, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Calvin, A.D.; Covassin, N.; Kremers, W.K.; Adachi, T.; Macedo, P.; Albuquerque, F.N.; Bukartyk, J.; Davison, D.E.; Levine, J.A.; Singh, P.; et al. Experimental sleep restriction causes endothelial dysfunction in healthy humans. J. Am. Heart Assoc. 2014, 3, e001143. [Google Scholar] [CrossRef] [PubMed]
- Zieman, S.J.; Melenovsky, V.; Kass, D.A. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.K.; Mueller, W.H.; Chan, W.; Meininger, J.C. Is obesity associated with poor sleep quality in adolescents? Am. J. Hum. Biol. 2002, 14, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Hasler, G.; Buysse, D.J.; Klaghofer, R.; Gamma, A.; Ajdacic, V.; Eich, D.; Rossler, W.; Angst, J. The association between short sleep duration and obesity in young adults: A 13-year prospective study. Sleep 2004, 27, 661–666. [Google Scholar] [CrossRef]
- Nilsson, P.M.; Roost, M.; Engstrom, G.; Hedblad, B.; Berglund, G. Incidence of diabetes in middle-aged men is related to sleep disturbances. Diabetes Care 2004, 27, 2464–2469. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Spaeth, A.M.; Ma, N.; Zhu, S.; Hu, S.; Goel, N.; Detre, J.A.; Dinges, D.F.; Rao, H. Altered salience network connectivity predicts macronutrient intake after sleep deprivation. Sci. Rep. 2015, 5, 8215. [Google Scholar] [CrossRef]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Hakim, F.; Wang, Y.; Carreras, A.; Hirotsu, C.; Zhang, J.; Peris, E.; Gozal, D. Chronic sleep fragmentation during the sleep period induces hypothalamic endoplasmic reticulum stress and PTP1b-mediated leptin resistance in male mice. Sleep 2015, 38, 31–40. [Google Scholar] [CrossRef]
- Cedernaes, J.; Schonke, M.; Westholm, J.O.; Mi, J.; Chibalin, A.; Voisin, S.; Osler, M.; Vogel, H.; Hornaeus, K.; Dickson, S.L.; et al. Acute sleep loss results in tissue-specific alterations in genome-wide DNA methylation state and metabolic fuel utilization in humans. Sci. Adv. 2018, 4, eaar8590. [Google Scholar] [CrossRef]
- Thurley, K.; Herbst, C.; Wesener, F.; Koller, B.; Wallach, T.; Maier, B.; Kramer, A.; Westermark, P.O. Principles for circadian orchestration of metabolic pathways. Proc. Natl. Acad. Sci. USA 2017, 114, 1572–1577. [Google Scholar] [CrossRef] [PubMed]
- Peek, C.B.; Levine, D.C.; Cedernaes, J.; Taguchi, A.; Kobayashi, Y.; Tsai, S.J.; Bonar, N.A.; McNulty, M.R.; Ramsey, K.M.; Bass, J. Circadian Clock Interaction with HIF1alpha Mediates Oxygenic Metabolism and Anaerobic Glycolysis in Skeletal Muscle. Cell Metab. 2017, 25, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Liao, D.; Bixler, E.O.; Chrousos, G.P.; Vela-Bueno, A. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep 2009, 32, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Trzepizur, W.; Le Vaillant, M.; Meslier, N.; Pigeanne, T.; Masson, P.; Humeau, M.P.; Bizieux-Thaminy, A.; Goupil, F.; Chollet, S.; Ducluzeau, P.H.; et al. Independent association between nocturnal intermittent hypoxemia and metabolic dyslipidemia. Chest 2013, 143, 1584–1589. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Yi, H.; Zou, J.; Meng, L.; Tang, X.; Zhu, H.; Yu, D.; Zhou, H.; Su, K.; Guan, J.; et al. Independent Association between Sleep Fragmentation and Dyslipidemia in Patients with Obstructive Sleep Apnea. Sci. Rep. 2016, 6, 26089. [Google Scholar] [CrossRef] [PubMed]
- Barros, D.; Garcia-Rio, F. Obstructive sleep apnea and dyslipidemia. From animal models to clinical evidence. Sleep 2018. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Savransky, V.; Nanayakkara, A.; Smith, P.L.; O’Donnell, C.P.; Polotsky, V.Y. Hyperlipidemia and lipid peroxidation are dependent on the severity of chronic intermittent hypoxia. J. Appl. Physiol. (1985) 2007, 102, 557–563. [Google Scholar] [CrossRef]
- Tan, K.C.; Chow, W.S.; Lam, J.C.; Lam, B.; Wong, W.K.; Tam, S.; Ip, M.S. HDL dysfunction in obstructive sleep apnea. Atherosclerosis 2006, 184, 377–382. [Google Scholar] [CrossRef]
- Narkiewicz, K.; Somers, V.K. Sympathetic nerve activity in obstructive sleep apnoea. Acta Physiol. Scand. 2003, 177, 385–390. [Google Scholar] [CrossRef]
- Ottosson, M.; Vikman-Adolfsson, K.; Enerback, S.; Olivecrona, G.; Bjorntorp, P. The effects of cortisol on the regulation of lipoprotein lipase activity in human adipose tissue. J. Clin. Endocrinol. Metab. 1994, 79, 820–825. [Google Scholar]
- Gottlieb, D.J.; Punjabi, N.M.; Newman, A.B.; Resnick, H.E.; Redline, S.; Baldwin, C.M.; Nieto, F.J. Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch. Intern. Med. 2005, 165, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Rafalson, L.; Donahue, R.P.; Stranges, S.; Lamonte, M.J.; Dmochowski, J.; Dorn, J.; Trevisan, M. Short sleep duration is associated with the development of impaired fasting glucose: The Western New York Health Study. Ann. Epidemiol. 2010, 20, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Kent, B.D.; Grote, L.; Ryan, S.; Pepin, J.L.; Bonsignore, M.R.; Tkacova, R.; Saaresranta, T.; Verbraecken, J.; Levy, P.; Hedner, J.; et al. Diabetes mellitus prevalence and control in sleep-disordered breathing: The European Sleep Apnea Cohort (ESADA) study. Chest 2014, 146, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Nagayoshi, M.; Lutsey, P.L.; Benkeser, D.; Wassel, C.L.; Folsom, A.R.; Shahar, E.; Iso, H.; Allison, M.A.; Criqui, M.H.; Redline, S. Association of sleep apnea and sleep duration with peripheral artery disease: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2016, 251, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.; Liberty, I.F.; Porath, A.; Ovsyshcher, I.; Prystowsky, E.N. A simple bedside test of 1-minute heart rate variability during deep breathing as a prognostic index after myocardial infarction. Am. Heart J. 1999, 138, 32–38. [Google Scholar] [CrossRef]
- Valensi, P.; Sachs, R.N.; Harfouche, B.; Lormeau, B.; Paries, J.; Cosson, E.; Paycha, F.; Leutenegger, M.; Attali, J.R. Predictive value of cardiac autonomic neuropathy in diabetic patients with or without silent myocardial ischemia. Diabetes Care 2001, 24, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Gottsater, A.; Ahlgren, A.R.; Taimour, S.; Sundkvist, G. Decreased heart rate variability may predict the progression of carotid atherosclerosis in type 2 diabetes. Clin. Auton. Res. 2006, 16, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Melillo, P.; Izzo, R.; De Luca, N.; Pecchia, L. Heart rate variability and target organ damage in hypertensive patients. BMC Cardiovasc. Disord. 2012, 12, 105. [Google Scholar] [CrossRef] [PubMed]
- Pizzi, C.; Manzoli, L.; Mancini, S.; Bedetti, G.; Fontana, F.; Costa, G.M. Autonomic nervous system, inflammation and preclinical carotid atherosclerosis in depressed subjects with coronary risk factors. Atherosclerosis 2010, 212, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Ulleryd, M.A.; Prahl, U.; Borsbo, J.; Schmidt, C.; Nilsson, S.; Bergstrom, G.; Johansson, M.E. The association between autonomic dysfunction, inflammation and atherosclerosis in men under investigation for carotid plaques. PLoS ONE 2017, 12, e0174974. [Google Scholar] [CrossRef]
- Pereira, V.L., Jr.; Dobre, M.; Dos Santos, S.G.; Fuzatti, J.S.; Oliveira, C.R.; Campos, L.A.; Brateanu, A.; Baltatu, O.C. Association between Carotid Intima Media Thickness and Heart Rate Variability in Adults at Increased Cardiovascular Risk. Front Physiol. 2017, 8, 248. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, M.; Urbina, E.M.; Wadwa, R.P.; Talton, J.W.; D’Agostino, R.B., Jr.; Hamman, R.F.; Fingerlin, T.E.; Daniels, S.R.; Marcovina, S.M.; Dolan, L.M.; et al. Reduced heart rate variability is associated with increased arterial stiffness in youth with type 1 diabetes: The SEARCH CVD study. Diabetes Care 2013, 36, 2351–2358. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.; Zhu, L. The crosstalk between autonomic nervous system and blood vessels. Int. J. Physiol. Pathophysiol. Pharmacol. 2018, 10, 17–28. [Google Scholar] [PubMed]
- Gamboa, A.; Figueroa, R.; Paranjape, S.Y.; Farley, G.; Diedrich, A.; Biaggioni, I. Autonomic Blockade Reverses Endothelial Dysfunction in Obesity-Associated Hypertension. Hypertension 2016, 68, 1004–1010. [Google Scholar] [PubMed]
- Badimon, L.; Martinez-Gonzalez, J.; Royo, T.; Lassila, R.; Badimon, J.J. A sudden increase in plasma epinephrine levels transiently enhances platelet deposition on severely damaged arterial wall—Studies in a porcine model. Thromb. Haemost. 1999, 82, 1736–1742. [Google Scholar] [PubMed]
- Yamada, T.; Katagiri, H. Avenues of communication between the brain and tissues/organs involved in energy homeostasis. Endocr. J. 2007, 54, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M.; de Geus, E.J.; Penninx, B.W. Dysregulation of the autonomic nervous system predicts the development of the metabolic syndrome. J. Clin. Endocrinol. Metab. 2013, 98, 2484–2493. [Google Scholar] [CrossRef] [PubMed]
- Lee, Z.S.; Critchley, J.A.; Tomlinson, B.; Young, R.P.; Thomas, G.N.; Cockram, C.S.; Chan, T.Y.; Chan, J.C. Urinary epinephrine and norepinephrine interrelations with obesity, insulin, and the metabolic syndrome in Hong Kong Chinese. Metabolism 2001, 50, 135–143. [Google Scholar] [CrossRef]
- Simonds, S.E.; Pryor, J.T.; Ravussin, E.; Greenway, F.L.; Dileone, R.; Allen, A.M.; Bassi, J.; Elmquist, J.K.; Keogh, J.M.; Henning, E.; et al. Leptin mediates the increase in blood pressure associated with obesity. Cell 2014, 159, 1404–1416. [Google Scholar] [CrossRef]
- Kurajoh, M.; Koyama, H.; Kadoya, M.; Naka, M.; Miyoshi, A.; Kanzaki, A.; Kakutani-Hatayama, M.; Okazaki, H.; Shoji, T.; Moriwaki, Y.; et al. Plasma leptin level is associated with cardiac autonomic dysfunction in patients with type 2 diabetes: HSCAA study. Cardiovasc. Diabetol. 2015, 14, 117. [Google Scholar]
- Nakahashi, T.; Fujimura, H.; Altar, C.A.; Li, J.; Kambayashi, J.; Tandon, N.N.; Sun, B. Vascular endothelial cells synthesize and secrete brain-derived neurotrophic factor. FEBS Lett. 2000, 470, 113–117. [Google Scholar] [CrossRef]
- Drivsholm, T.; de Fine Olivarius, N.; Nielsen, A.B.; Siersma, V. Symptoms, signs and complications in newly diagnosed type 2 diabetic patients, and their relationship to glycaemia, blood pressure and weight. Diabetologia 2005, 48, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.; Hong, S.; Nelesen, R.; Dimsdale, J.E. The association of obesity, cytokine levels, and depressive symptoms with diverse measures of fatigue in healthy subjects. Arch Intern. Med. 2005, 165, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Bardwell, W.A.; Moore, P.; Ancoli-Israel, S.; Dimsdale, J.E. Fatigue in obstructive sleep apnea: Driven by depressive symptoms instead of apnea severity? Am. J. Psychiatry 2003, 160, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Koyama, H.; Fukuda, S.; Shoji, T.; Inaba, M.; Tsujimoto, Y.; Tabata, T.; Okuno, S.; Yamakawa, T.; Okada, S.; Okamura, M.; et al. Fatigue is a predictor for cardiovascular outcomes in patients undergoing hemodialysis. Clin. J. Am. Soc. Nephrol. 2010, 5, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, A.; Okauchi, T.; Hu, D.; Shingaki, T.; Katayama, Y.; Koyama, H.; Watanabe, Y.; Cui, Y. Extension of recovery time from fatigue by repeated rest with short-term sleep during continuous fatigue load: Development of chronic fatigue model. J. Neurosci. Res. 2016, 94, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Kurajoh, M.; Kadoya, M.; Morimoto, A.; Naka, M.; Miyoshi, A.; Kanzaki, A.; Kakutani-Hatayama, M.; Hamamoto, K.; Shoji, T.; Moriwaki, Y.; et al. Plasma leptin concentration is associated with fatigue severity in patients with cardiovascular risk factors—HSCAA study. Psychoneuroendocrinology 2016, 74, 7–12. [Google Scholar] [CrossRef]
- Kurajoh, M.; Kadoya, M.; Morimoto, A.; Miyoshi, A.; Kanzaki, A.; Kakutani-Hatayama, M.; Hamamoto, K.; Shoji, T.; Moriwaki, Y.; Yamamoto, T.; et al. Plasma brain-derived neurotrophic factor concentration is a predictor of chronic kidney disease in patients with cardiovascular risk factors—Hyogo Sleep Cardio-Autonomic Atherosclerosis study. PLoS ONE 2017, 12, e0178686. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surrogate Marker of Atherosclerosis | Sleep Parameter | Study Design | Subjects | Sleep Measurement | Comments | References |
|---|---|---|---|---|---|---|
| Carotid intima media thickness (IMT) | Duration | Cross-sectional | Elderly (n = 86) | PSQI Actigraphy | Shorter sleep duration (<5 h) increased IMT as compared to longer duration (>7 h) | Nakazaki et al. [19] |
| Quality | Cross-sectional | Elderly (n = 86) Elderly (n = 201) Type 2 diabetes mellitus (n = 63) Cardiovascular risk factors (n = 330) | Self-reported questionnaire Single-channel EEG Actigraphy | Insomnia associated with IMT as compared with non-insomnia | Nakazaki et al. [19] Nagai et al. [20] Yoda et al. [21] Kadoya et al. [11] | |
| Apnea-hypopnea | Cross-sectional | Cardiovascular risk factors (n = 330) | Apnomonitor | OSA associated with IMT and plaque score | Kadoya et al. [11] | |
| Brachial-ankle pulse wave velocity (baPWV) | Quality | Cross-sectional | Type 2 diabetes mellitus (n = 724) | PSQI | Poor sleep quality associated with higher PWV | Osonoi et al. [22] |
| Prospective | Cardiovascular risk factors (n = 306) | Actigraphy | Low sleep quality associated with progression of PWV over 3-year period | Kadoya et al. [18] | ||
| Apnea-hypopnea | Cross-sectional | Ischemic stroke (n = 127) | Polysomnography | OSA associated with PWV | Chen et al. [10] |
| Surrogate Marker of Atherosclerosis | Sleep Parameter | Study Design | Population Characteristics | Sleep Measurement | Comments | References |
|---|---|---|---|---|---|---|
| Carotid intima media thickness (IMT) | Duration | Cross-sectional | Healthy, middle-aged (n = 617) | Actigraphy | Shorter sleep duration (<5 h) increase IMT. | Sands et al. [23] |
| General population (n = 2383) Health check-up subjects (n = 2214) | Long sleep duration (>7 h or >11 h) significantly correlated with the incidence of carotid artery atherosclerosis | Wolff et al. [24] Abe et al. [25] | ||||
| Brachial-ankle pulse wave velocity (baPWV) | Duration | Cross-sectional | Health check-up subjects (n = 18,106) | PSQI | Subjective short sleep duration (<5 h) is associated with higher PWV | Kim et al. [28] |
| Health check-up subjects (n = 18,106) Health check-up subjects (n = 4268) Health check-up subjects (n = 3508) | Self-Report questionnaire PSQI | Long sleep duration (> 8 h) is associated with elevated PWV | Kim et al. [28] Yoshioka et al. [29] Tsai et al. [30] | |||
| Quality | Cross-sectional | Health check-up subjects (18,106) | PSQI | Poor sleep quality is associated with higher PWV | Kim et al. [28] |
| Variables | Sleep Physical Activity | % Sleep | ||
|---|---|---|---|---|
| β | p | β | p | |
| Macro TSH (high = 1. Low = 0) | 0.145 | 0.01 | −0.150 | <0.01 |
| Adjusted R2 | 0.041 | <0.01 | 0.047 | <0.01 |
| Surrogate Marker of Atherosclerosis | Study Design | Population | Comments | References |
|---|---|---|---|---|
| Carotid intima media thickness (IMT) | Cross-sectional | Cardiovascular risk factors (n = 330) Depressed with cardiovascular risk factors (n = 391) Males >40 years old (n = 124) Cardiovascular risk factors (n = 101) | HRV associated with carotid IMT, independent of sleep quality and apnea-hypopnea. Inflammation may be involved in association between autonomic dysfunction and atherosclerosis. | Kadoya et al. [11] Pizzi et al. [69] Ulleryd et al. [70] Pereira et al. [71] |
| Retrospective | Hypertensive (n = 200) | HRV associated with renal damage | Melillo et al. [68] | |
| Prospective | Type 2 diabetes (n = 61) | Decreased HRV may predict progression of carotid atherosclerosis | Gottsater et al. [67] | |
| Brachial-ankle pulse wave velocity (baPWV) | Cross-sectional | Type 1 diabetes (n = 344) | Lower HRV associated with higher baPWV (no prospective studies available) | Jaiswal et al. [72] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadoya, M.; Koyama, H. Sleep, Autonomic Nervous Function and Atherosclerosis. Int. J. Mol. Sci. 2019, 20, 794. https://doi.org/10.3390/ijms20040794
Kadoya M, Koyama H. Sleep, Autonomic Nervous Function and Atherosclerosis. International Journal of Molecular Sciences. 2019; 20(4):794. https://doi.org/10.3390/ijms20040794
Chicago/Turabian StyleKadoya, Manabu, and Hidenori Koyama. 2019. "Sleep, Autonomic Nervous Function and Atherosclerosis" International Journal of Molecular Sciences 20, no. 4: 794. https://doi.org/10.3390/ijms20040794
APA StyleKadoya, M., & Koyama, H. (2019). Sleep, Autonomic Nervous Function and Atherosclerosis. International Journal of Molecular Sciences, 20(4), 794. https://doi.org/10.3390/ijms20040794