Identification of c.1531C>T Pathogenic Variant in the CDH1 Gene as a Novel Germline Mutation of Hereditary Diffuse Gastric Cancer

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. DNA Extraction
4.2. Sequence Analysis
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941. [Google Scholar] [CrossRef] [PubMed]
- Zanghieri, G.; Di Gregorio, C.; Sacchetti, C.; Fante, R.; Sassatelli, R.; Cannizzo, G.; Carriero, A.; Ponz de Leon, M. Familial occurrence of Gastric Cancer in the 2-year experience of a population-based registry. Cancer 1990, 66, 2047–2051. [Google Scholar] [CrossRef]
- Jones, E.G. Familial Gastric Cancer. N. Z. Med. J. 1964, 63, 287–296. [Google Scholar] [PubMed]
- Guilford, P.; Hopkins, J.; Harraway, J.; McLeod, M.; McLeod, N.; Harawira, P.; Taite, H.; Scoular, R.; Miller, A.; Reeve, A.E. E-cadherin germline mutations in familial gastric cancer. Nature 1998, 392, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Guilford, P.; Humar, B.; Blair, V. Hereditary diffuse gastric cancer: Translation of CDH1 germline mutations into clinical practice. Gastric Cancer 2010, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Park, J.G.; Yang, H.K.; Kim, W.H.; Caldas, C.; Yokota, J.; Guilford, P.J. Report on the first meeting of the International Collaborative Group on Hereditary Gastric Cancer. J. Natl. Cancer Inst. 2000, 92, 1781–1782. [Google Scholar] [CrossRef] [PubMed]
- Humar, B.; Guilford, P. Hereditary diffuse gastric cancer: A manifestation of lost cell polarity. Cancer Sci. 2009, 100, 1151–1157. [Google Scholar] [CrossRef]
- Van der Post, R.S.; Vogelaar, I.P.; Carneiro, F.; Guilford, P.; Huntsman, D.; Hoogerbrugge, N.; Caldas, C.; Schreiber, K.E.; Hardwick, R.H.; Ausems, M.G.; et al. Hereditary diffuse gastric cancer: Updated clinical guidelines with an emphasis on germline CDH1 mutation carriers. J. Med. Genet. 2015, 52, 361–374. [Google Scholar] [CrossRef]
- Fitzgerald, R.C.; Hardwick, R.; Huntsman, D.; Carneiro, F.; Guilford, P.; Blair, V.; Chung, D.C.; Norton, J.; Ragunath, K.; Van Krieken, J.H.; et al. Hereditary diffuse gastric cancer: Updated consensus guidelines for clinical management and directions for future research. J. Med. Genet. 2010, 47, 436–444. [Google Scholar] [CrossRef]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and Beyond. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef]
- Pharoah, P.D.; Guilford, P.; Caldas, C. Incidence of Gastric Cancer and breast cancer in CDH1 (E-cadherin) mutation carriers from hereditary diffuse Gastric Cancer families. Gastroenterology 2001, 121, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Seevaratnam, R.; Coburn, N.; Cardoso, R.; Dixon, M.; Bocicariu, A.; Helyer, L. A systematic review of the indications for genetic testing and prophylactic gastrectomy among patients with hereditary diffuse gastric cancer. Gastric Cancer 2012, 15, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Corso, G.; Marrelli, D.; Pascale, V.; Vindigni, C.; Roviello, F. Frequency of CDH1 germline mutations in gastric carcinoma coming from high- and low-risk areas: Metanalysis and systematic review of the literature. BMC Cancer 2012, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Melo, S.; Figueiredo, J.; Fernandes, M.S.; Goncalves, M.; Morais-de-Sa, E.; Sanches, J.M.; Seruca, R. Predicting the Functional Impact of CDH1 Missense Mutations in Hereditary Diffuse Gastric Cancer. Int. J. Mol. Sci. 2017, 18, 2687. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research, N. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Post, R.S.; Vogelaar, I.P.; Manders, P.; van der Kolk, L.E.; Cats, A.; van Hest, L.P.; Sijmons, R.; Aalfs, C.M.; Ausems, M.G.; Gomez Garcia, E.B.; et al. Accuracy of Hereditary Diffuse Gastric Cancer Testing Criteria and Outcomes in Patients with a Germline Mutation in CDH1. Gastroenterology 2015, 149, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Kaurah, P.; MacMillan, A.; Boyd, N.; Senz, J.; De Luca, A.; Chun, N.; Suriano, G.; Zaor, S.; Van Manen, L.; Gilpin, C.; et al. Founder and recurrent CDH1 mutations in families with hereditary diffuse gastric cancer. Jama 2007, 297, 2360–2372. [Google Scholar] [CrossRef]
- De Campos, E.C.; Ribeiro, S.; Higashi, R.; Manfredini, R.; Kfouri, D.; Cavalcanti, T.C. Hereditary diffuse gastric cancer: Laparoscopic surgical approach associated to rare mutattion of CDH1 gene. Arq. Bras. Cir. 2015, 28, 149–151. [Google Scholar] [CrossRef]
- Moreira-Nunes, C.A.; Barros, M.B.L.; do Nascimento Borges, B.; Montenegro, R.C.; Lamarao, L.M.; Ribeiro, H.F.; Bona, A.B.; Assumpcao, P.P.; Rey, J.A.; Pinto, G.R.; et al. Genetic screening analysis of patients with hereditary diffuse Gastric Cancer from northern and northeastern Brazil. Hered. Cancer Clin. Pract. 2014, 12, 18. [Google Scholar] [CrossRef]
- Landrum, M.J.; Lee, J.M.; Benson, M.; Brown, G.; Chao, C.; Chitipiralla, S.; Gu, B.; Hart, J.; Hoffman, D.; Hoover, J.; et al. ClinVar: Public archive of interpretations of clinically relevant variants. Nucleic Acids Res. 2016, 44, 862–868. [Google Scholar] [CrossRef]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Norero, E.; Vega, E.A.; Diaz, C.; Cavada, G.; Ceroni, M.; Martinez, C.; Briceno, E.; Araos, F.; Gonzalez, P.; Baez, S.; et al. Improvement in postoperative mortality in elective gastrectomy for gastric cancer: Analysis of predictive factors in 1066 patients from a single centre. Eur. J. Surg. Oncol. 2017, 43, 1330–1336. [Google Scholar] [CrossRef] [PubMed]
- Lynch, H.T.; Lynch, J.F. Hereditary diffuse gastric cancer: Lifesaving total gastrectomy for CDH1 mutation carriers. J. Med. Genet. 2010, 47, 433–435. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, C.; Makino, H.; Takagawa, R.; Kimura, J.; Ota, M.; Ichikawa, Y.; Kosaka, T.; Akiyama, H.; Endo, I. A systematic review of laparoscopic total gastrectomy for gastric cancer. Gastric Cancer 2015, 18, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Moisan, F.; Norero, E.; Slako, M.; Varas, J.; Palominos, G.; Crovari, F.; Ibanez, L.; Perez, G.; Pimentel, F.; Guzman, S.; et al. Completely laparoscopic versus open gastrectomy for early and advanced gastric cancer: A matched cohort study. Surg. Endosc. 2012, 26, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Norero, E.; Baez, S.; Briceno, E.; Martinez, C.; Ceroni, M.; Escalona, A.; Aguayo, G.; Gonzalez, P.; Araos, F.; Calvo, A.; et al. Totally laparoscopic gastrectomy for the treatment of gastric tumors. Rev. Med. Chil. 2015, 143, 281–288. [Google Scholar] [CrossRef]
- Haverkamp, L.; Weijs, T.J.; van der Sluis, P.C.; van der Tweel, I.; Ruurda, J.P.; van Hillegersberg, R. Laparoscopic total gastrectomy versus open total gastrectomy for cancer: A systematic review and meta-analysis. Surg. Endosc. 2013, 27, 1509–1520. [Google Scholar] [CrossRef]
- Norero, E.; Munoz, R.; Ceroni, M.; Manzor, M.; Crovari, F.; Gabrielli, M. Two-Layer Hand-Sewn Esophagojejunostomy in Totally Laparoscopic Total Gastrectomy for Gastric Cancer. J. Gastric Cancer 2017, 17, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Strong, V.E.; Gholami, S.; Shah, M.A.; Tang, L.H.; Janjigian, Y.Y.; Schattner, M.; Selby, L.V.; Yoon, S.S.; Salo-Mullen, E.; Stadler, Z.K.; et al. Total Gastrectomy for Hereditary Diffuse Gastric Cancer at a Single Center: Postsurgical Outcomes in 41 Patients. Ann. Surg. 2017, 266, 1006–1012. [Google Scholar] [CrossRef]
- Hakkaart, C.; Ellison-Loschmann, L.; Day, R.; Sporle, A.; Koea, J.; Harawira, P.; Cheng, S.; Gray, M.; Whaanga, T.; Pearce, N.; et al. Germline CDH1 mutations are a significant contributor to the high frequency of early-onset diffuse Gastric Cancer cases in New Zealand Maori. Fam. Cancer 2018, 18, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Schrader, K.A.; Masciari, S.; Boyd, N.; Salamanca, C.; Senz, J.; Saunders, D.N.; Yorida, E.; Maines-Bandiera, S.; Kaurah, P.; Tung, N.; et al. Germline mutations in CDH1 are infrequent in women with early-onset or familial lobular breast cancers. J. Med. Genet. 2011, 48, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Vogelaar, I.P.; Figueiredo, J.; van Rooij, I.A.; Simoes-Correia, J.; van der Post, R.S.; Melo, S.; Seruca, R.; Carels, C.E.; Ligtenberg, M.J.; Hoogerbrugge, N. Identification of germline mutations in the cancer predisposing gene CDH1 in patients with orofacial clefts. Hum. Mol. Genet. 2013, 22, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Molinaro, V.; Pensotti, V.; Marabelli, M.; Feroce, I.; Barile, M.; Pozzi, S.; Laghi, L.; Serrano, D.; Bernard, L.; Bonanni, B.; et al. Complementary molecular approaches reveal heterogeneous CDH1 germline defects in Italian patients with hereditary diffuse Gastric Cancer (HDGC) syndrome. Genes Chromosomes Cancer 2014, 53, 432–445. [Google Scholar] [CrossRef] [PubMed]
- Brooks-Wilson, A.R.; Kaurah, P.; Suriano, G.; Leach, S.; Senz, J.; Grehan, N.; Butterfield, Y.S.; Jeyes, J.; Schinas, J.; Bacani, J.; et al. Germline E-cadherin mutations in hereditary diffuse gastric cancer: Assessment of 42 new families and review of genetic screening criteria. J. Med. Genet. 2004, 41, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Van Domselaar, F.; Correa, D.; Vaccaro, C.; Redal, M.; Van Domselaar, R.; Huntsman, D.; Kaurah, P.; Senz, J.; Lynch, H. Hereditary diffuse Gastric Cancer (HDGC): Presentation of a family with a new mutation of the CDH1 gene. Acta Gastroenterol. Latinoam. 2007, 37, 158–163. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Sierra, M.S.; Cueva, P.; Bravo, L.E.; Forman, D. Stomach cancer burden in Central and South America. Cancer Epidemiol. 2016, 44, s62–s73. [Google Scholar] [CrossRef]
- Sahasrabudhe, R.; Lott, P.; Bohorquez, M.; Toal, T.; Estrada, A.P.; Suarez, J.J.; Brea-Fernandez, A.; Cameselle-Teijeiro, J.; Pinto, C.; Ramos, I.; et al. Germline Mutations in PALB2, BRCA1, and RAD51C, Which Regulate DNA Recombination Repair, in Patients with Gastric Cancer. Gastroenterology 2017, 152, 983–986. [Google Scholar] [CrossRef]
- Slavin, T.; Neuhausen, S.L.; Rybak, C.; Solomon, I.; Nehoray, B.; Blazer, K.; Niell-Swiller, M.; Adamson, A.W.; Yuan, Y.C.; Yang, K.; et al. Genetic Gastric Cancer Susceptibility in the International Clinical Cancer Genomics Community Research Network. Cancer Genet. 2017, 216–217, 111–119. [Google Scholar] [CrossRef]
- Jung, I.; Gurzu, S.; Turdean, G.S. Current status of familial gastrointestinal polyposis syndromes. World J. Gastrointest. Oncol. 2015, 7, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Chung, J.W.; Jeong, T.D.; Park, Y.S.; Lee, J.H.; Ahn, J.Y.; Kim, D.H.; Choi, K.D.; Lee, W.; Song, H.J.; et al. Searching for E-cadherin gene mutations in early onset diffuse Gastric Cancer and hereditary diffuse Gastric Cancer in Korean patients. Fam. Cancer 2013, 12, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Senz, J.; Kaurah, P.; Pinheiro, H.; Sanges, R.; Haegert, A.; Corso, G.; Schouten, J.; Fitzgerald, R.; Vogelsang, H.; et al. Germline CDH1 deletions in hereditary diffuse Gastric Cancer families. Hum. Mol. Genet. 2009, 18, 1545–1555. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.L.; French, K.S.; Resta, R.G.; Doyle, D.L. Standardized human pedigree nomenclature: Update and assessment of the recommendations of the National Society of Genetic Counselors. J. Genet. Couns. 2008, 17, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, D.; Morgagni, P.; de Manzoni, G.; Coniglio, A.; Marchet, A.; Saragoni, L.; Tiberio, G.; Roviello, F. Prognostic value of the 7th AJCC/UICC TNM classification of noncardia gastric cancer: Analysis of a large series from specialized Western centers. Ann. Surg. 2012, 255, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Lauren, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and So-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Den Dunnen, J.T.; Dalgleish, R.; Maglott, D.R.; Hart, R.K.; Greenblatt, M.S.; McGowan-Jordan, J.; Roux, A.F.; Smith, T.; Antonarakis, S.E.; Taschner, P.E. HGVS Recommendations for the Description of Sequence Variants: 2016 Update. Hum. Mutat. 2016, 37, 564–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
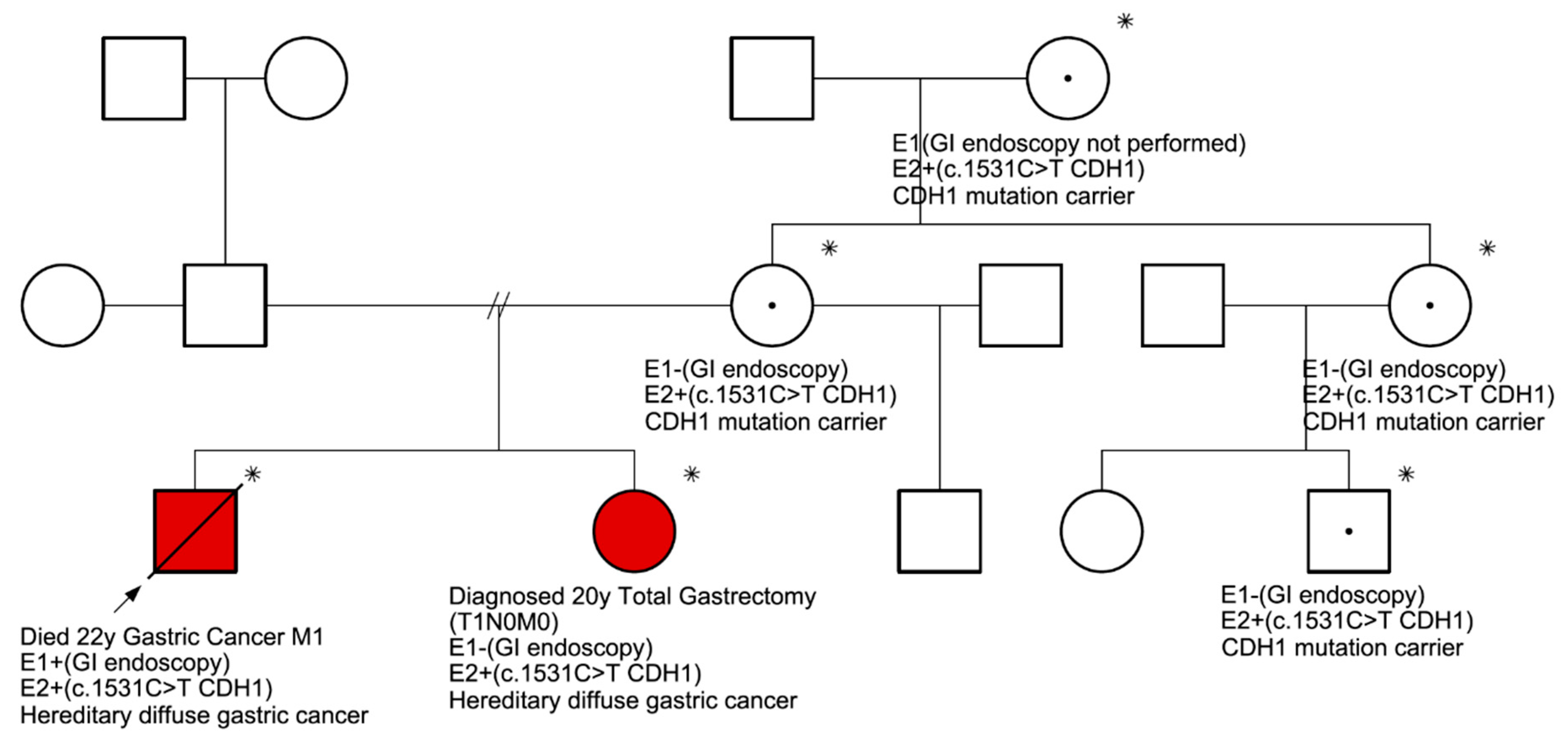
 : Proband.
: Proband.  : Died from gastric cancer.
: Died from gastric cancer.  : Male.
: Male.  : Female. E1: endoscopic evaluation. E2: molecular evaluation. In red, the two individuals in which DGC was confirmed.
: Proband. : Died from gastric cancer. : Male. : Female. E1: endoscopic evaluation. E2: molecular evaluation. In red, the two individuals in which DGC was confirmed.
: Female. E1: endoscopic evaluation. E2: molecular evaluation. In red, the two individuals in which DGC was confirmed.
: Proband. : Died from gastric cancer. : Male. : Female. E1: endoscopic evaluation. E2: molecular evaluation. In red, the two individuals in which DGC was confirmed.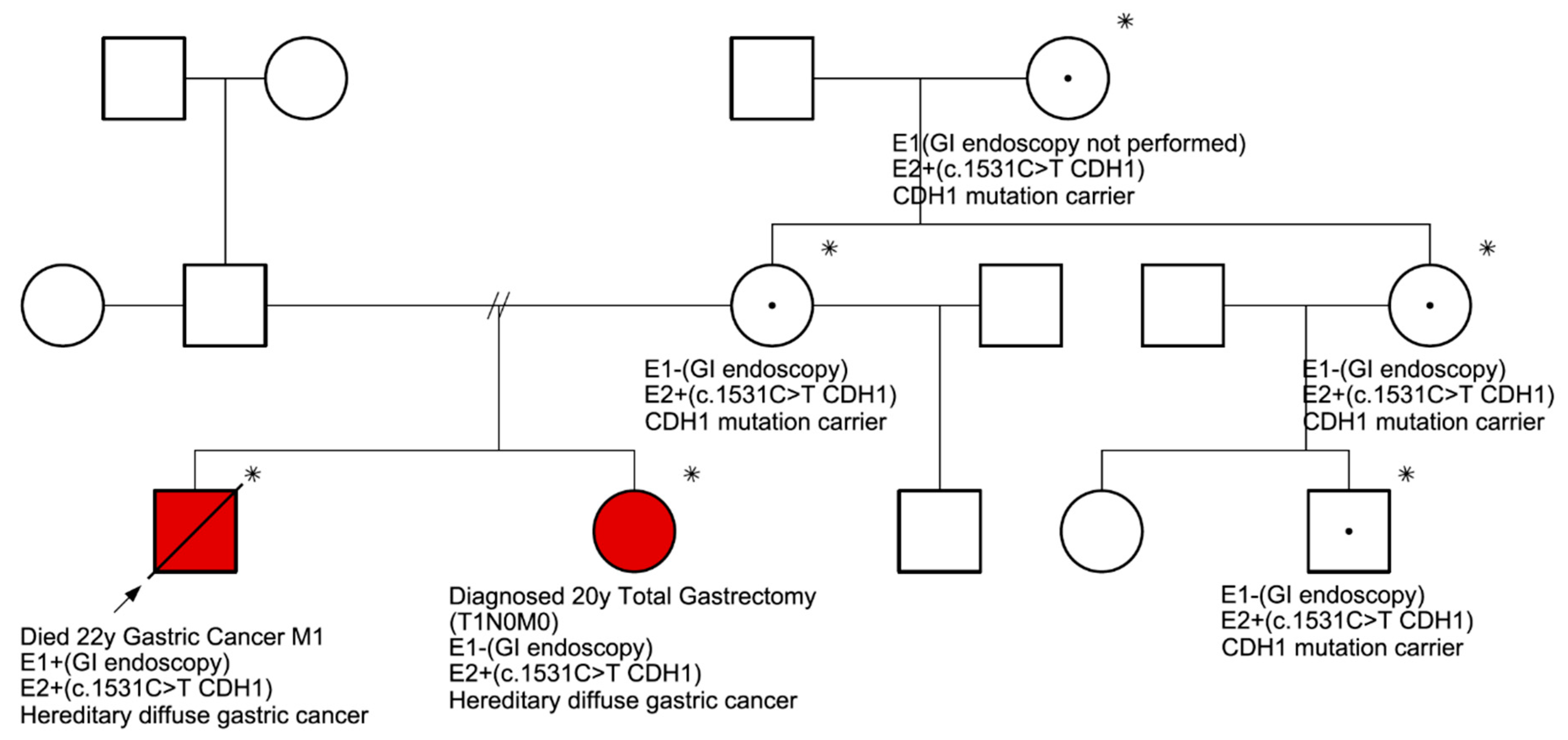

{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Total | 36 |
| Gender | |
| Male | 18 (50) |
| Female | 18 (50) |
| Age (years) | 44 (range: 22–68) |
| ≤ 29 | 7 (19) |
| 30–39 | 7 (19) |
| 40–49 | 12 (33) |
| 50–59 | 4 (11) |
| 60 or older | 6 (16) |
| Smoking status | |
| Current smoker | 16 (44) |
| Previously smoker | 3 (8) |
| Non smoker | 17 (47) |
| Stage | |
| I | 5 (14) |
| II | 6 (17) |
| III | 12 (33) |
| IV | 13 (36) |
| Family history of gastric cancer * | |
| 1 family member (only proband) | 17 (47) |
| 2 family members | 6 (17) |
| 3 family members | 9 (25) |
| 4 or more family members | 4 (11) |
| Family history of breast cancer | 6 (16) |
| Family history of colorectal cancer | 2 (6) |
| Family history of prostate cancer | 3 (8) |
| Family history of uterine cancer | 2 (6) |
| Family history of skin cancer | 1 (3) |
| Family history of esophageal cancer | 1 (3) |
| Family history of gallbladder cancer | 1 (3) |
| Family history of lung cancer | 1 (3) |
| Family history of thyroid cancer | 1 (3) |
| Family history of ovarian cancer | 1 (3) |
| Family history of other cancer unknown | 6 (16) |
| Helicobacter pylori infection | |
| Infected | 15 (42) |
| Not infected | 10 (28) |
| Unknown | 11 (30) |
| SNP ID | Sequence Variant | Protein Change | Probands (n) | Location | Class | Significance α |
|---|---|---|---|---|---|---|
| rs16260 | c.-285C>A | 19 | Promoter | Promoter | Non-coding | |
| rs28372783 | c.-197A>C | 11 | Promoter | Promoter | Non-coding | |
| rs3743674 | c.48+6C>T | 36 | Intron 1 | Splice site | Benign | |
| rs139866691 | c.88C>A | p.Pro30Thr | 1 | Exon 2 | Missense | Benign |
| rs33963999 | c.531+10G>C | 1 | Intron 4 | Splice site | Benign | |
| rs61756284 | c.1272A>T | p.Thr424Thr | 1 | Exon 9 | Synonymous | Benign |
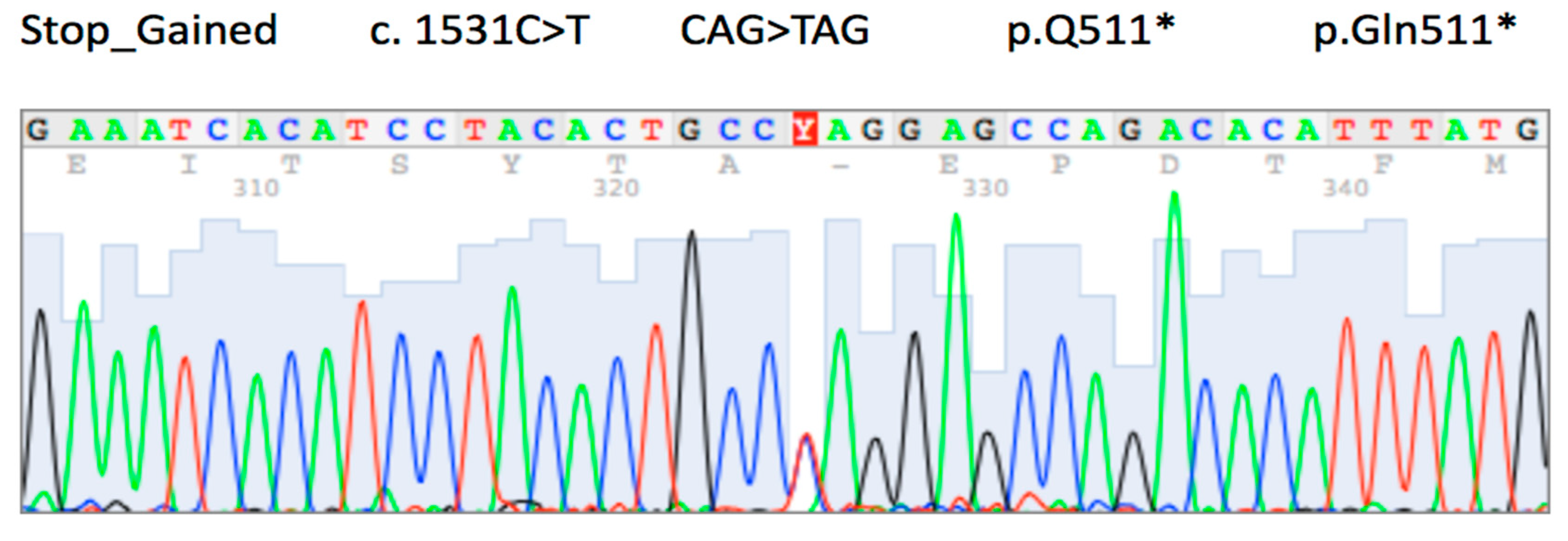
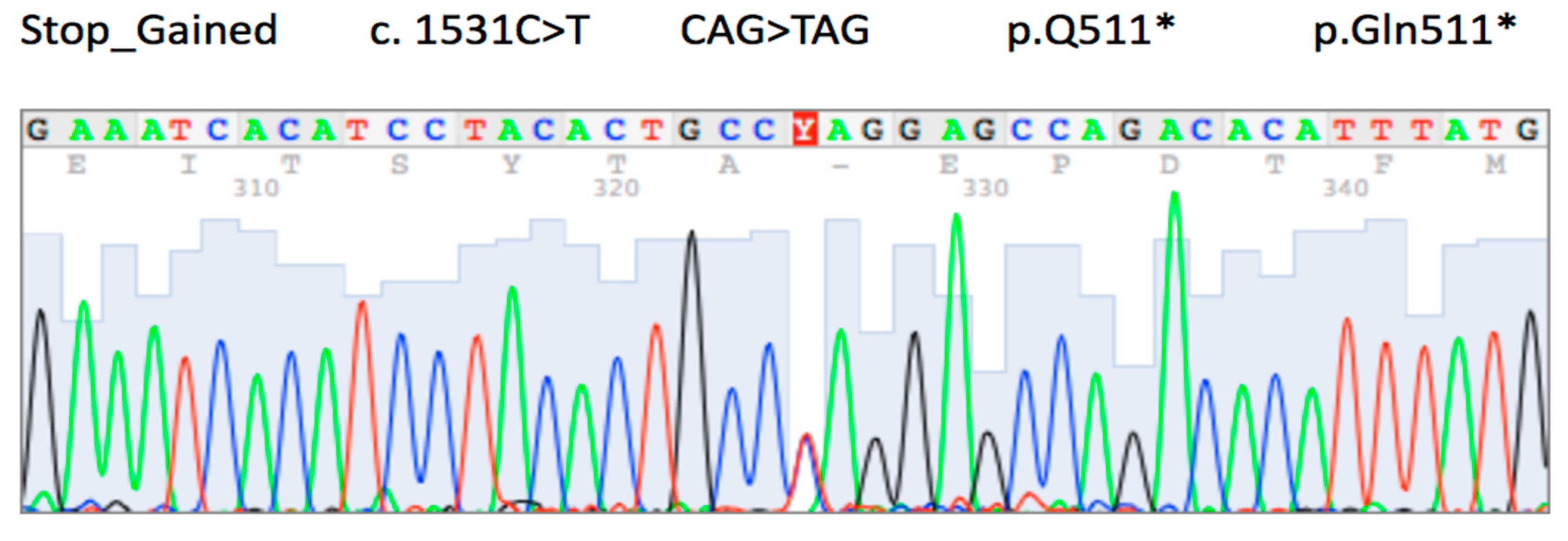
| rs1131690810 | c.1531C>T | p.Gln511 * | 1 | Exon 10 | Nonsense | Pathogenic |
| rs786201452 | c.1893A>T | p.Thr631Thr | 1 | Exon 12 | Synonymous | Likely benign |
| rs764379691 | c.2052C>T | p.Ser684Ser | 1 | Exon 13 | Synonymous | Likely benign |
| rs1801552 | c.2076T>C | p.Ala692Ala | 30 | Exon 13 | Synonymous | Benign |
| rs33964119 | c.2253C>T | p.Asn751Asn | 4 | Exon 14 | Synonymous | Benign |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norero, E.; Alarcon, M.A.; Hakkaart, C.; de Mayo, T.; Mellado, C.; Garrido, M.; Aguayo, G.; Lagos, M.; Torres, J.; Calvo, A.; et al. Identification of c.1531C>T Pathogenic Variant in the CDH1 Gene as a Novel Germline Mutation of Hereditary Diffuse Gastric Cancer. Int. J. Mol. Sci. 2019, 20, 4980. https://doi.org/10.3390/ijms20204980
Norero E, Alarcon MA, Hakkaart C, de Mayo T, Mellado C, Garrido M, Aguayo G, Lagos M, Torres J, Calvo A, et al. Identification of c.1531C>T Pathogenic Variant in the CDH1 Gene as a Novel Germline Mutation of Hereditary Diffuse Gastric Cancer. International Journal of Molecular Sciences. 2019; 20(20):4980. https://doi.org/10.3390/ijms20204980
Chicago/Turabian StyleNorero, Enrique, M. Alejandra Alarcon, Christopher Hakkaart, Tomas de Mayo, Cecilia Mellado, Marcelo Garrido, Gloria Aguayo, Marcela Lagos, Javiera Torres, Alfonso Calvo, and et al. 2019. "Identification of c.1531C>T Pathogenic Variant in the CDH1 Gene as a Novel Germline Mutation of Hereditary Diffuse Gastric Cancer" International Journal of Molecular Sciences 20, no. 20: 4980. https://doi.org/10.3390/ijms20204980
APA StyleNorero, E., Alarcon, M. A., Hakkaart, C., de Mayo, T., Mellado, C., Garrido, M., Aguayo, G., Lagos, M., Torres, J., Calvo, A., Guilford, P., & Corvalan, A. H. (2019). Identification of c.1531C>T Pathogenic Variant in the CDH1 Gene as a Novel Germline Mutation of Hereditary Diffuse Gastric Cancer. International Journal of Molecular Sciences, 20(20), 4980. https://doi.org/10.3390/ijms20204980