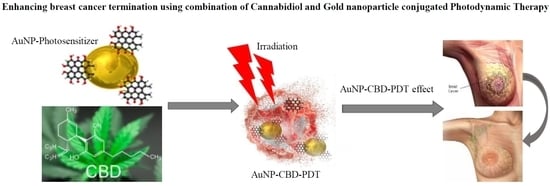
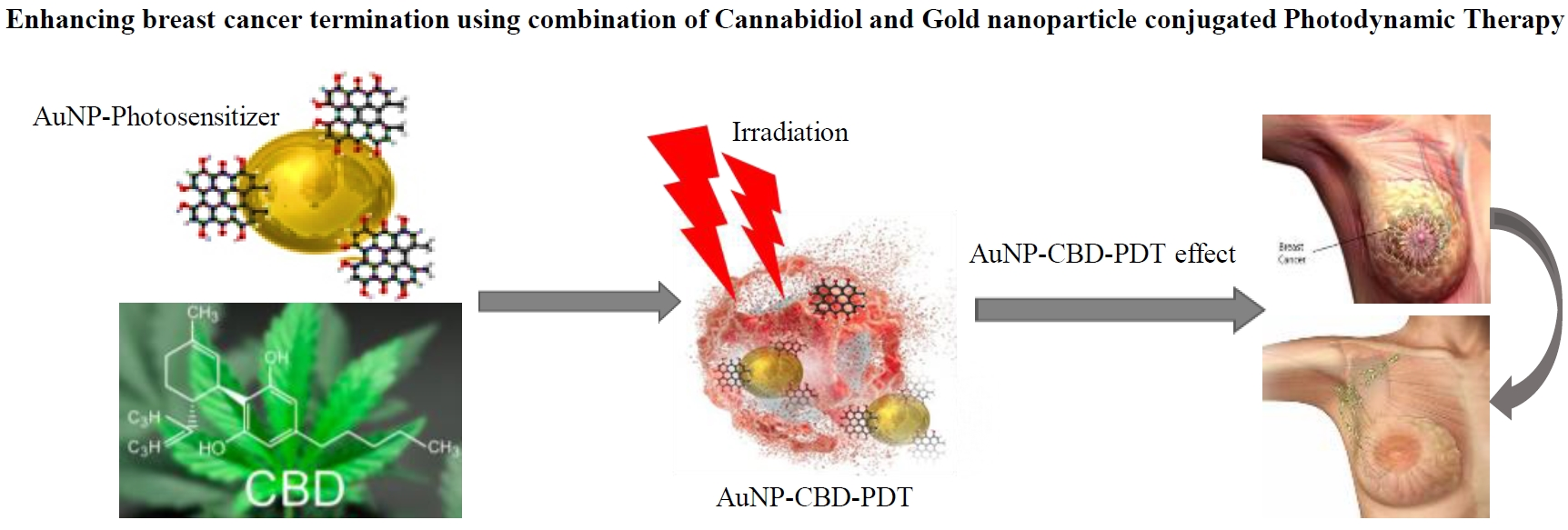
Enhancing Breast Cancer Treatment Using a Combination of Cannabidiol and Gold Nanoparticles for Photodynamic Therapy



Abstract
1. Introduction
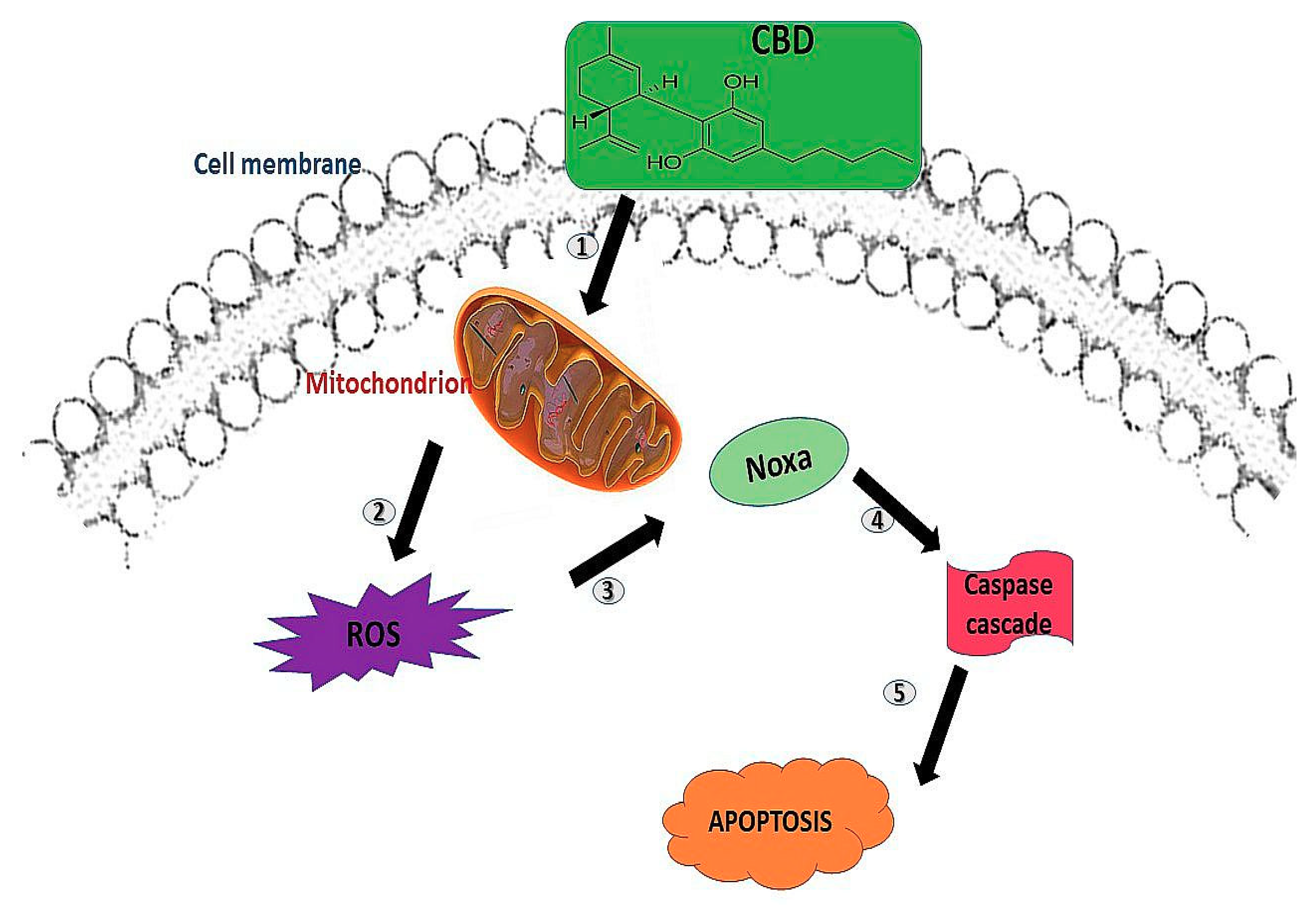
2. Cannabidiol
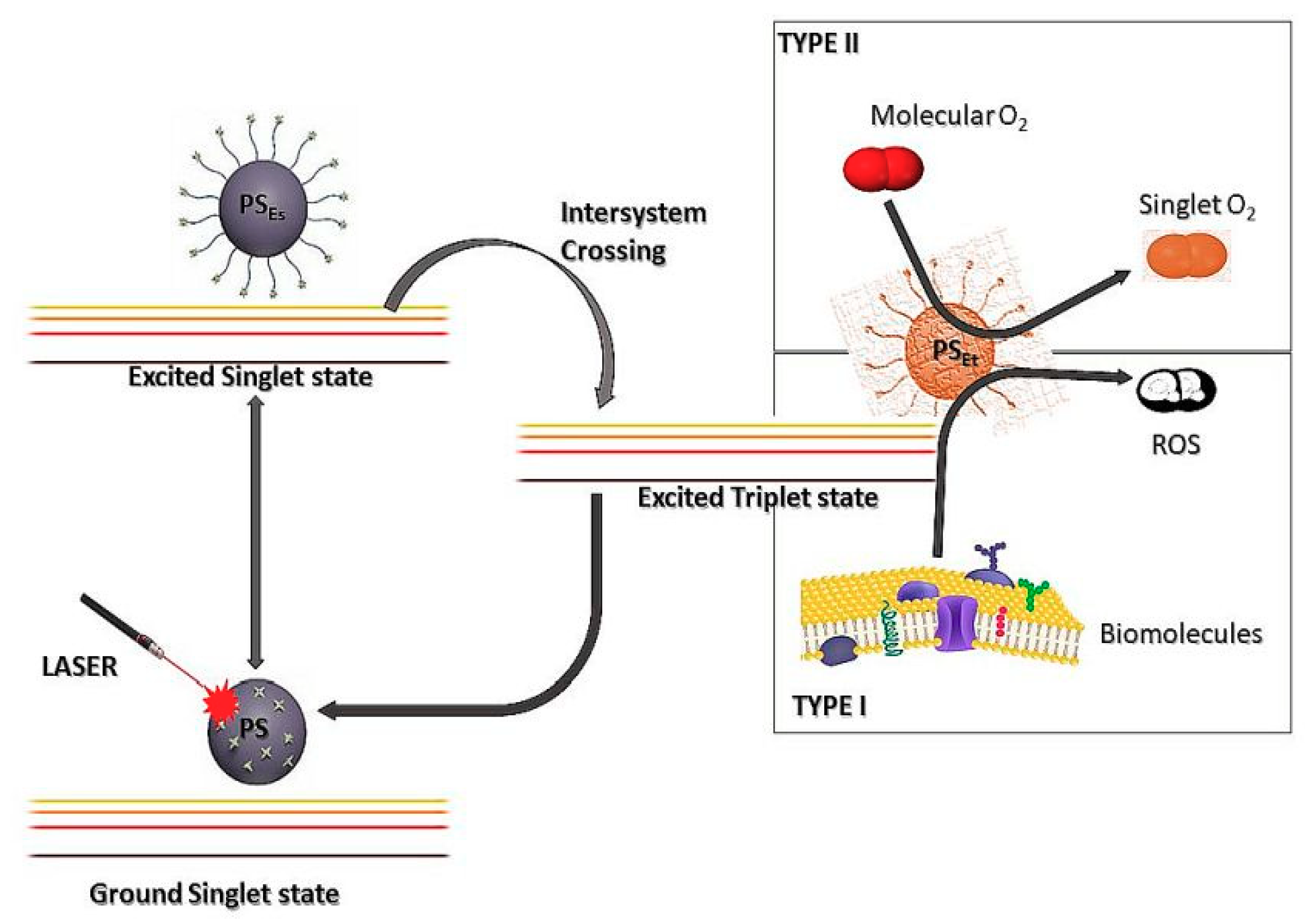
3. Photodynamic Therapy (PDT)
3.1. Photosensitisers (PS)
3.2. Advances in the Field of PDT
4. Hypericin and Gold Nanoparticle
5. Combination Therapy of Cannabidiol and Photodynamic Therapy
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AuNP | Gold nanoparticle |
| PDT | Photodynamic Therapy |
| CBD | Cannabidiol |
| WHO | World Health Organization |
| ROS | Reactive Oxygen Species |
| RT | Radiotherapy |
| PS | Photosensitiser |
| ER | Endoplasmic Reticulum |
| DNA | Deoxyribonucleic acid |
| RNA | Ribonucleic acid |
| LDL | Low density lipid |
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 30 May 2019).
- National Cancer Institute. Available online: https://www.cancer.gov/types/common-cancers (accessed on 20 July 2019).
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Akram, M.; Iqbal, M.; Daniyal, M.; Khan, A.U. Awareness and current knowledge of breast cancer. Biol. Res. 2017, 50, 33. [Google Scholar] [CrossRef] [PubMed]
- Rakha, E.A.; Reis-Filho, J.S.; Baehner, F.; Dabbs, D.J.; Decker, T.; Eusebi, V.; Fox, S.B.; Ichihara, S.; Jacquemier, J.; Lakhani, S.R.; et al. Breast cancer prognostic classification in the molecular era: The role of histological grade. Breast Cancer Res. 2010, 12, 207. [Google Scholar] [CrossRef] [PubMed]
- Sak, K. Chemotherapy and dietary phytochemical agents. Chemother. Res. Pract. 2012, 2012, 282570. [Google Scholar] [CrossRef] [PubMed]
- Dariš, B.; Tancer Verboten, M.; Knez, Ž.; Ferk, P. Cannabinoids in cancer treatment: Therapeutic potential and legislation. BJBMS 2019, 19, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Birdsall, S.M.; Birdsall, T.C.; Tims, L.A. The use of medical marijuana in cancer. Curr. Oncol. Rep. 2016, 18, 40. [Google Scholar] [CrossRef]
- Davis, M.P. Cannabinoids for symptom management and cancer therapy: The evidence. J. Natl. Compr. Cancer Netw. 2016, 14, 915–922. [Google Scholar] [CrossRef]
- Munson, A.E.; Harris, L.S.; Friedman, M.A.; Dewey, W.L. Carchman, R.A. Antineoplastic activity of cannabinoids. J. Natl. Cancer Inst. 1975, 55, 597–602. [Google Scholar] [CrossRef]
- Ramer, R.; Bublitz, K.; Freimuth, N.; Merkord, J.; Rohde, H.; Haustein, M.; Borchert, P.; Schmuhl, E.; Linnebacher, M.; Hinz, B. Cannabidiol inhibits lung cancer cell invasion and metastasis via intercellular adhesion molecule-1. FASEB 2012, 26, 1535–1548. [Google Scholar] [CrossRef]
- Abrams, D.I. Integrating cannabis into clinical cancer care. Curr. Oncol. 2016, 23, 8–14. [Google Scholar]
- Adams, I.B.; Martin, B.R. Cannabis: Pharmacology and toxicology in animals and humans. Addiction 1996, 91, 1585–1614. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Yun, H.K.; Jeong, Y.A.; Jo, M.J.; Kang, S.H.; Kim, J.L.; Kim, D.Y.; Park, S.H.; Kim, B.R.; Na, Y.J.; et al. Cannabidiol-induced apoptosis is mediated by activation of Noxa in human colorectal cancer cells. Cancer Lett. 2019, 10, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Yasmin-Karim, S.; Moreau, M.; Mueller, R.; Sinha, N.; Dabney, R.; Herman, A.; Ngwa, W. Enhancing the Therapeutic Efficacy of Cancer treatment with cannabinoids. Front. Oncol. 2018, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- De Petrocellis, L.; Ligresti, A.; Schiano Moriello, A.; Iappelli, M.; Verde, R.; Stott, C.G.; Cristino, L.; Orlando, P.; Di Marzo, V. Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: Pro-apoptotic effects and underlying mechanisms. Br. J. Pharmacol. 2013, 168, 79–102. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Kuzontkoski, P.M.; Groopman, J.E.; Prasad, A. Cannabidiol induces programmed cell death in breast cancer cells by coordinating the cross-talk between apoptosis and autophagy. Mol. Cancer Ther. 2011, 10, 1161–1172. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.; Fischer, O.M.; Ullrich, A. Cannabinoids induce cancer cell proliferation via tumor necrosis factor alpha-converting enzyme (TACE/ADAM17)-mediated transactivation of the epidermal growth factor receptor. Cancer Res. 2004, 64, 1943–1950. [Google Scholar] [CrossRef]
- Cridge, B.J.; Rosengren, R.J. Critical appraisal of the potential use of cannabinoids in cancer management. Cancer Manag. Res. 2013, 5, 301–313. [Google Scholar]
- Marcu, J.P.; Christian, R.T.; Lau, D.; Zielinski, A.J.; Horowitz, M.P.; Lee, J.; Pakdel, A.; Allison, J.; Limbad, C.; Moore, D.H.; et al. Cannabidiol enhances the inhibitory effects of delta9-tetrahydrocannabinol on human glioblastoma cell proliferation and survival. Mol. Cancer Ther. 2010, 9, 180–189. [Google Scholar] [CrossRef]
- Abrahamse, H.; Hamblin, M.R. New photosensitizers for photodynamic therapy. Biochem. J. 2016, 473, 347–364. [Google Scholar] [CrossRef]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Debele, T.A.; Peng, S.; Tsai, H.-C. Review Drug Carrier for Photodynamic Cancer Therapy. Int. J. Mol. Sci. 2015, 16, 22094–22136. [Google Scholar] [CrossRef] [PubMed]
- Kubiak, M.; Łysenko, L.; Gerber, H.; Nowak, R. Cell reactions and immune responses to photodynamic therapy in oncology. Postepy Hig. Med. Dosw. 2016, 70, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Duse, L.; Pinnapireddy, S.R.; Strehlow, B.; Jedelska, J.; Bakowsky, U. Low level LED photodynamic therapy using curcumin loaded tetraether liposomes. Eur. J. Pharm. Biopharm. 2018, 126, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Moriyama, L.T.; Bagnato, V.S. Photodynamic therapy induced vascular damage: An overview of experimental PDT. Laser Phys. Lett. 2012, 10, 023001. [Google Scholar] [CrossRef]
- Yang, Y.; Hu, Y.; Wang, H. Targeting antitumor immune response for enhancing the efficacy of photodynamic therapy of cancer: Recent advances and future perspectives. Oxid. Med. Cell Longev. 2016, 2016, 5274084. [Google Scholar] [CrossRef] [PubMed]
- Calixto, G.M.; Bernegossi, J.; de Freitas, L.M.; Fontana, C.R.; Chorilli, M. Nanotechnology Based Drug Delivery Systems for Photodynamic Therapy of Cancer: A Review. Molecules 2016, 21, 342. [Google Scholar] [CrossRef]
- Sibata, C.H.; Colussi, V.C.; Oleinick, N.L.; Kinsella, T.J. Photodynamic therapy: A new concept in medical treatment. Braz. J. Med. Biol. Res. 2000, 33, 869–880. [Google Scholar] [CrossRef]
- Theodossiou, T.A.; Hothersall, J.S.; De Witte, P.A.; Pantos, A.; Agostinis, P. The multifaceted photocytotoxic profile of hypericin. Mol. Pharmacol. 2009, 6, 1775–1789. [Google Scholar] [CrossRef]
- Garg, A.D.; Krysko, D.V.; Vandenabeele, P.; Agostinis, P. Hypericin-based photodynamic therapy induces surface exposure of damage-associated molecular patterns like HSP70 and calreticulin. Cancer Immunol. Immunother. 2012, 61, 215–221. [Google Scholar] [CrossRef]
- Garg, A.D.; Agostinis, P. ER stress, autophagy and immunogenic cell death in photodynamic therapy-induced anti-cancer immune responses. Photochem. Photobiol. Sci. 2014, 13, 474–487. [Google Scholar] [CrossRef]
- Plenagl, N.; Duse, L.; Seitz, B.S.; Goergen, N.; Pinnapireddy, S.R.; Jedelska, J.; Brüßler, J.; Bakowsky, U. Photodynamic therapy - hypericin tetraether liposome conjugates and their antitumor and antiangiogenic activity. Drug Deliv. 2019, 26, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Davids, L.M.; Maduray, K. The anticancer activity of hypericin in photodynamic therapy. J. Bioanal. Biomed. 2012. [Google Scholar] [CrossRef]
- Gattuso, H.; Marazzi, M.; Dehez, F.; Monari, A. Deciphering the photosensitization mechanisms of hypericin towards biological membranes. Phys. Chem. Chem. Phys. 2017, 19, 23187–23193. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Jiang, C.; Li, Y.; Liu, W.; Yao, N.; Gao, M.; Ji, Y.; Huang, D.; Yin, Z.; Sun, Z.; et al. Evaluation of hypericin: Effect of aggregation on targeting biodistribution. J. Pharmacol. Sci. 2015, 104, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Toumey, C. Reading Feynman Into Nanotechnology: A Text for a New Science. Techne Res. Phil. Tech. 2008, 12, 133–168. [Google Scholar] [CrossRef]
- Jia, X.; Jia, L. Nanoparticles improve biological functions of phthalocyanine photosensitizers used for photodynamic therapy. Curr. Drug Metab. 2012, 13, 1119–1122. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, N.O.; Hardell, L. Porphyrias porphyrins and hepatocellular cancer. Br. J. Cancer 1986, 54, 115–117. [Google Scholar] [CrossRef]
- Malik, Z.; Lugaci, H. Destruction of erythroleukaemic cells by photoactivation of endogenous porphyrins. Br. J. Cancer 1987, 56, 589–595. [Google Scholar] [CrossRef]
- To, Y.F.; Sun, R.W.; Chen, Y.; Chan, V.S.; Yu, W.Y.; Tam, P.K.; Che, C.M.; Lin, C.L. Gold(III) porphyrin complex is more potent than cisplatin in inhibiting growth of nasopharyngeal carcinoma in vitro and in vivo. Int. J. Cancer 2009, 124, 1971–1979. [Google Scholar] [CrossRef]
- Lu, K.; He, C.; Lin, W. A Chlorin-Based Nanoscale Metal–Organic Framework for Photodynamic Therapy of Colon Cancers. J. Am. Chem. Soc. 2015, 137, 7600–7603. [Google Scholar] [CrossRef]
- Moore, C.M.; Nathan, T.R.; Lees, W.R.; Mosse, C.A.; Freeman, A.; Emberton, M.; Bown, S.G. Photodynamic therapy using meso tetra hydroxy phenyl chlorin (mTHPC) in early prostate cancer. Lasers Surg. Med. 2006, 38, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Grosjean, P.; Savary, J.F.; Wagnières, G.; Mizeret, J.; Woodtli, A.; Theumann, J.F.; Fontolliet, C.; Van Den Bergh, H.; Monnier, P. Tetra(m-hydroxyphenyl)chlorin clinical photodynamic therapy of early bronchial and oesophageal cancers. Laser Med. Sci. 1996, 11, 227–235. [Google Scholar] [CrossRef]
- Wood, S.R.; Holroyd, J.A.; Brown, S.B. The subcellular localization of Zn (II) phthalocyanines and their redistribution on exposure to light. Photochem. Photobiol. 1997, 65, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Stuchinskaya, T.; Moreno, M.; Cook, M.J.; Edwards, D.R.; Russell, D.A. Targeted photodynamic therapy of breast cancer cells using antibody-phthalocyanine-gold nanoparticle conjugates. Photochem. Photobiol. Sci. 2011, 10, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Sekhejane, P.R.; Houreld, N.N.; Abrahamse, H. Multiorganelle Localization of Metallated Phthalocyanine Photosensitizer in Colorectal Cancer Cells (DLD-1 and CaCo-2) Enhances Efficacy of Photodynamic Therapy. Int. J. Photoenergy 2014. [Google Scholar] [CrossRef]
- Chizenga, P.E.; Chandran, R.; Abrahamse, H. Photodynamic therapy of cervical cancer by eradication of cervical cancer cells and cervical cancer stem cells. Oncotarget 2019, 10, 4380–4396. [Google Scholar] [PubMed]
- Hajri, A.; Wack, S.; Meyer, C.; Smith, M.K.; Leberquier, C.; Kedinger, M.; Aprahamian, M. In Vitro and In Vivo Efficacy of Photofrin® and Pheophorbide a, a Bacteriochlorin, in Photodynamic Therapy of Colonic Cancer Cells. Photochem. Photobiol. 2002, 75, 140–148. [Google Scholar] [CrossRef]
- Uppal, A.; Jain, B.; Kumar Gupta, P.; Das, K. Photodynamic Action of Rose Bengal Silica Nanoparticle Complex on Breast and Oral Cancer Cell Lines. Photochem. Photobiol. 2011, 87, 1146–1151. [Google Scholar] [CrossRef]
- Walker, I.; Gorman, S.A.; Cox, R.D.; Vernon, D.I.; Griffiths, J.; Brown, S.B. A comparative analysis of phenothiazinium salts for the photosensitisation of murine fibrosarcoma (RIF-1) cells in vitro. Photochem. Photobiol. Sci. 2004, 7, 653–659. [Google Scholar] [CrossRef]
- Rafique, S.; Idrees, M.; Nasim, A.; Akbar, H.; Athar, A. Transition metal complexes as potential therapeutic Agents. Biotechnol. Mol. Biol. Rev. 2010, 5, 38–45. [Google Scholar]
- Hamaa, Y.; Urano, Y.; Koyama, Y.; Choyke, P.L.; Kobayashi, H. Targeted optical imaging of cancer cells using lectin-binding BODIPY conjugated avidin. Biochem. Biophys. Res. Commun. 2006, 348, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Zeisser-Labouèbe, M.; Lange, N.; Gurny, R.; Delie, F. Hypericin-loaded nanoparticles for the photodynamic treatment of ovarian cancer. Int. J. Pharm. 2006, 326, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Mirmalek, S.A.; Azizi, M.A.; Jangholi, E.; Yadollah-Damavandi, S.; Javidi, M.A.; Parsa, Y.; Parsa, T.; Salimi-Tabatabaee, S.A.; Ghasemzadeh Kolagar, H.; Alizadeh-Navaei, R. Cytotoxic and apoptogenic effect of hypericin, the bioactive component of Hypericum perforatum on the MCF-7 human breast cancer cell line. Cancer Cell Int. 2016, 16, 3. [Google Scholar] [CrossRef] [PubMed]
- Yonar, D.; Kılıç Süloğlu, A.; Selmanoğlu, G.; Sünnetçioğlu, M.M. An Electron paramagnetic resonance (EPR) spin labeling study in HT-29 Colon adenocarcinoma cells after Hypericin-mediated photodynamic therapy. BMC Mol. Cell Biol. 2019, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Kensler, C.J.; Sugiura, K.; Young, N.F.; Halter, C.R.; Rhoads, C.P. Partial Protection of Rats by Riboflavin with Casein against Liver Cancer Caused by Dimethyl-Aminoazobenzene. Science 1941, 93, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Hilary, J. Powers. Interaction among Folate, Riboflavin, Genotype, and Cancer, with Reference to Colorectal and Cervical Cancer. J. Nutr. 2005, 135, 2960S–2966S. [Google Scholar]
- Koon, H.K.; Leung, A.W.N.; Yue, K.K.M.; Mak, N.K. Photodynamic Effect of Curcumin on NPC/CNE2 Cells. J. Environ. Pathol. Toxicol. Oncol. 2006, 25, 205–216. [Google Scholar] [CrossRef]
- Khorsandi, K.; Hosseinzadeh, R.; Fateha, M. Curcumin intercalated layered double hydroxide nanohybrid as a potential drug delivery system for effective photodynamic therapy in human breast cancer cells. RSC Adv. 2015, 5, 93987–93994. [Google Scholar] [CrossRef]
- Xu, S.; Chen, S.; Zhang, M.; Shen, T.; Zhao, Y.; Liu, Z.; Wu, Y. Butylamino-demethoxy-hypocrellins and photodynamic therapy decreases human cancer in vitro and in vivo. Biochim. Biophys. Acta 2001, 1537, 222–232. [Google Scholar] [CrossRef]
- Madaan, K.; Kumar, S.; Poonia, N.; Lather, V.; Pandita, D. Dendrimers in drug delivery and targeting: Drug-dendrimer interactions and toxicity issues. J. Pharm. Bioallied. Sci. 2014, 6, 139–150. [Google Scholar]
- Yadav, D.; Sandeep, K.; Pandey, D.; Dutta, R.K. Liposomes for Drug Delivery. J. Biotechnol. Biomater. 2017. [Google Scholar] [CrossRef]
- Çagdas, M.; Sezer, A.D.; Bucak, S. Liposomes as potential drug carrier systems for drug delivery. Nanotechnol. Nanomater. 2014. [Google Scholar] [CrossRef]
- Lin, L.; Xiong, L.; Wen, Y.; Lei, S.; Deng, X.; Liu, Z.; Chen, W.; Miao, X. Active Targeting of Nano-Photosensitizer Delivery Systems for Photodynamic Therapy of Cancer Stem Cells. JBN 2015, 11, 531–554. [Google Scholar] [CrossRef]
- Zhu, J.; Zheng, L.; Wen, S.; Tang, Y.; Shen, M.; Zhang, G.; Shi, X. Targeted cancer theranostics using alpha-tocopheryl succinate-conjugated multifunctional dendrimer-entrapped gold nanoparticles. Biomaterials 2014, 35, 7635–7646. [Google Scholar] [CrossRef] [PubMed]
- Rana, V.; Sharma, R. Recent Advances in Development of Nano Drug Delivery. In Applications of Targeted Nano Drugs and Delivery Systems; Mohapatra, S.S., Ranjan, S., Dasgupta, N., Mishra, R.K., Thomas, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 93–131. [Google Scholar]
- Chan, J.M.; Valencia, P.M.; Zhang, L.; Langer, R.; Farokhzad, O.C. Polymeric Nanoparticles for Drug Delivery. In Cancer Nanotechnology (Methods and Protocols); Grobmyer, S., Moudgil, B., Eds.; Humana Press: Totowa, NJ, USA, 2010; Volume 624. [Google Scholar]
- Yu, G.; Ning, Q.; Mo, Z.; Tang, S. Intelligent polymeric micelles for multidrug co-delivery and cancer therapy. Artif. Cells Nanomed. Biotechnol. 2019, 47, 1476–1487. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.; Wang, X.; Nie, S.; Chen, Z.G.; Shin, D.M. Therapeutic nanoparticles for drug delivery in cancer. Clin. Cancer Res. 2008, 14, 1310–1316. [Google Scholar] [CrossRef]
- Tolia, G.T.; Choi, H.H. The role of dendrimers in topical drug delivery. Pharm. Technol. 2008, 32, 88–98. [Google Scholar]
- Li, J.; Wang, X.; Zhang, T.; Wang, C.; Huang, Z.; Xiang, L.; Yihui, D. A review on phospholipids and their main applications in drug delivery systems. Asian J. Pharm. Sci. 2014, 10, 81–98. [Google Scholar] [CrossRef]
- Bozzuto, G.; Molinari, A. Liposomes as nanomedical devices. Int. J. Nanomed. 2015, 10, 975–999. [Google Scholar] [CrossRef]
- Bruckman, M.A.; Czapar, A.E.; Steinmetz, N.F. Drug-Loaded Plant-Virus Based Nanoparticles for Cancer Drug Delivery. In Virus-Derived Nanoparticles for Advanced Technologies; Wege, C., Lomonossoff, G., Eds.; Humana Press: New York, NY, USA, 2018; Volume 1776. [Google Scholar]
- Zhang, Y.; Dong, Y.; Zhou, J.; Li, X.; Wang, F. Application of Plant Viruses as a Biotemplate for Nanomaterial Fabrication. Molecules 2018, 23, 2311. [Google Scholar] [CrossRef]
- Elhissi, A.M.; Ahmed, W.; Hassan, I.U.; Dhanak, V.R.; D’Emanuele, A. Carbon nanotubes in cancer therapy and drug delivery. J. Drug Deliv. 2012, 2012, 837327. [Google Scholar] [CrossRef] [PubMed]
- Bhirde, A.A.; Patel, V.; Gavard, J.; Zhang, G.; Sousa, A.A.; Masedunskas, A.; Leapman, R.D.; Weigert, R.; Gutkind, J.S.; Rusling, J.F. Targeted killing of cancer cells in vivo and in vitro with EGF-directed carbon nanotube-based drug delivery. ACS Nano 2009, 3, 307–316. [Google Scholar]
- Guo, Q.; Shen, X.; Li, Y.; Xu, S.Q. Carbon nanotubes-based drug delivery to cancer and brain. Curr. Med. Sci. 2017, 37, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Pardo, J.; Peng, Z.; Leblanc, R.M. Cancer Targeting and Drug Delivery Using Carbon-Based Quantum Dots and Nanotubes. Molecules 2018, 23, E378. [Google Scholar] [CrossRef] [PubMed]
- Babu, L.T.; Paira, P. Current Application of Quantum Dots (QD) in Cancer Therapy: A Review. Mini Rev. Med. Chem. 2017, 17, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Longmire, M.; Choyke, P.L.; Kobayashi, H. Clearance properties of nanosized particles and molecules as imaging agents: Considerations and caveats. Nanomedicine 2008, 3, 703–717. [Google Scholar] [CrossRef] [PubMed]
- Portilho, F.A.; Cavalcanti, C.E.O.; Miranda-Vilela, A.L.; Estevanato, L.L.; Longo, J.P.; Almeida Santos Mde, F.; Bocca, A.L.; Martins, O.P.; Simioni, A.R.; Morais, P.C.; et al. Antitumor activity of photodynamic therapy performed with nanospheres containing zinc-phthalocyanine. J. Nanobiotechnol. 2013, 11, 41–65. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.K.; Tartakoff, A.M. Lectin-Colloidal Gold-Induced Density Perturbation of Membranes: Application to Affinity Elimination of the Plasma Membrane. Methods Cell Biol. 1989, 31, 247–263. [Google Scholar] [PubMed]
- Gupta, D.; Kumar, D.; Dwivedi, M.; Tripathi, V.; Phadke-Gupta, P.; Singhet, S.P. Nanophosphors-Nanogold Immunoconjugates in Isolation of Biomembranes and in Drug Delivery. In Nanomedicine for Drug Delivery and Therapeutics; Ajay Kumar Mirshra, A.K., Ed.; Wiley: Hoboken, NJ, USA, 2013. [Google Scholar]
- Giljohann, D.A.; Seferos, D.S.; Daniel, W.L.; Massich, M.D.; Patel, P.C.; Mirkin, C.A. Gold nanoparticles for biology and medicine. Angew. Chem. Int. Ed. Engl. 2010, 49, 3280–3294. [Google Scholar] [CrossRef] [PubMed]
- Kubin, A.; Wierrani, F.; Burner, U.; Alth, G.; Grunberger, W. Hypericin-the facts about a controversial agent. Curr. Pharm. Des. 2005, 11, 233–253. [Google Scholar] [CrossRef]
- Derycke, A.S.L.; de Witte, P.A.M. Transferrin-mediated targeting of hypericin embedded in sterically stabilized PEG-liposomes. Int. J. Oncol. 2002, 20, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, G.; Jedelská, J.; Strehlow, B.; Omar, S.; Schneider, M.; Bakowsky, U. Photo-responsive tetraether lipids based vesicles for prophyrin mediated vascular targeting and direct phototherapy. Colloids Surf. B 2017, 159, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Jacquemet, A.; Barbeau, J.; Lemiègre, L.; Benvegnu, T. Archaeal tetraether bipolar lipids: Structures, functions and applications. Biochimie 2009, 91, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Zolnik, B.S.; González-Fernández, A.; Sadrieh, N.; Dobrovolskaia, M.A. Nanoparticles and the immune system. Endocrinology 2010, 151, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Ling, X.; Zhang, S.; Liu, Y.; Bai, M. Light-activatable cannabinoid prodrug for combined and target-specific photodynamic and cannabinoid therapy. J. Biomed. Opt. 2018, 23, 1–9. [Google Scholar] [PubMed]
- Kisková, T.; Mungenast, F.; Suváková, M.; Jäger, W.; Thalhammer, T. Future Aspects for Cannabinoids in Breast Cancer Therapy. Int. J. Mol. Sci. 2019, 20, 1673. [Google Scholar] [CrossRef] [PubMed]
- Sadanala, K.C.; Chaturvedi, P.K.; Seo, Y.M.; Kim, J.M.; Jo, Y.S.; Lee, Y.K.; Ahn, W.S. Sono-Photodynamic Combination Therapy: A Review on Sensitizers. Int. J. Cancer Res. Treat. 2014, 34, 4657–4664. [Google Scholar]
- Yang, L.; Zhang, S.; Ling, X.; Shao, P.; Jia, N.; Bai, M. Multilayer photodynamic therapy for highly effective and safe cancer treatment. Acta Biomater. 2017, 54, 271–280. [Google Scholar] [CrossRef]
- Mroz, P.; Yaroslavsky, A.; Kharkwal, G.B.; Hamblin, M.R. Cell death pathways in photodynamic therapy of cancer. Cancers 2011, 3, 2516–2539. [Google Scholar] [CrossRef]
- Mathew, R.; Karantza-Wadsworth, V.; White, E. Role of autophagy in cancer. Nat. Rev. Cancer 2007, 7, 961–967. [Google Scholar] [CrossRef]
- Mattson, M.P.; Bazan, N.G. Apoptosis and Necrosis. Chapter in Basic Neurochemistry; Elsevier: Amsterdam, The Netherlands, 2012; pp. 663–676. [Google Scholar]
- Chaabane, W.; User, S.R.; El-Gazzah, M.; Jaksik, R.; Sajjadi, E.; Rzeszowska-Wolny, J.; Los, M.J. Autophagy, Apoptosis, Mitoptosis and Necrosis: Interdependence between those pathways and effects on cancer. Arch. Immunol. Ther. Exp. 2013, 61, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Sandle, T.; Chesca, A.; Akhayeva, A.S.; Marchenko, A.B. Apoptosis versus Necrosis. SFJ Chro. Dis. 2018, 1, 1–4. [Google Scholar]
- Hong, E.J.; Choi, D.G.; Shim, M.S. Targeted and effective photodynamic therapy for cancer using functionalized nanomaterials. Acta Pharm. Sin. B 2016, 6, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Ormond, A.B.; Freeman, H.S. Dye Sensitizers for Photodynamic Therapy. Materials 2013, 6, 817–840. [Google Scholar] [CrossRef] [PubMed]
- Mroz, P.; Hashmi, J.T.; Huang, Y.Y.; Lange, N.; Hamblin, M.R. Stimulation of anti-tumor immunity by photodynamic therapy. Expert Rev. Clin. Immunol. 2011, 7, 75–91. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cannabinoid | Therapeutic Properties | Cell Death Mechanism | Reference |
|---|---|---|---|
| Cannabidiol (CBD) | Reduced cancer cell viability, inhibits cell proliferation and invasion. | Apoptosis and autophagy. | [16,17,18] |
| Tetrahydrocannabinol (THC) | Decreased cancer cell proliferation. | Induction of p8-ATF-4TRIB3 pro-apoptotic pathway | [16,17,18,19] |
| CBD and THC combined | Synergistic inhibition of cellular proliferation. | Cell cycle modulation, ROS synthesis, apoptosis and caspase activities. | [20] |
| Cannabigerol (CBG) | Decreased cell viability | Induced apoptosis (Intrinsic apoptotic pathways) | [16] |
| Category | Photosensitiser | Wavelength Used | Type of Cancer | References |
|---|---|---|---|---|
| Tetrapyrrole structures | Porphyrins | 630 nm | Hepatocellular cancer, leukaemia and nasopharyngeal carcinoma | [21,39,40,41] |
| Chlorins | 650–700 nm | Colon, prostate, bronchial and oesophageal cancers | [42,43,44] | |
| Phthalocyanines | 640–690 nm | Cutaneous and subcutaneous lesions for many solid tumours including breast, cervical, melanoma, oesophageal and colon | [45,46,47,48] | |
| Bacteriochlorins | 700–800 nm | Colon | [49] | |
| Synthetic dyes | Rose Bengal | 530–540 nm | Breast and oral | [21,50] |
| Phenothiazinium salts | 630–670 nm | Fibrosarcoma | [21,51] | |
| Transition metal compounds | Breast and gastrointestinal carcinomas | [52] | ||
| BODIPY dye | 530–540 nm | 9 cancer cell lines in vitro and an ovarian cancer cell line in vivo using a murine peritoneal cancer model | [21,53] | |
| Natural products | Hypericin | 470–570 nm | Breast cancer, ovarian cancer and colon cancer | [54,55,56] |
| Riboflavin | 310–700 nm | Liver cancer, colorectal and cervical | [57,58] | |
| Curcumin | 350–450 nm | Nasopharyngeal carcinoma and breast | [59,60] | |
| Hypocrellins | 532 nm | Cervical and gastric | [61] |
| Nanoparticle | Description | Application | Reference |
|---|---|---|---|
| Polymeric nanoparticle | Biodegradable, biocompatible and non-toxic colloidal particles ranging between 1 and 1000 nm in size. Used to carry pharmaceutical drugs by adsorption, conjugation with a linker or encapsulation. | Drug delivery tissue engineering and gene delivery. | [67,68] |
| Polymeric Micelles | Amphiphilic co-polymers that gather forming a micelle with a hydrophobic core and a hydrophilic shell. | Multidrug co-delivery and cancer treatment. | [69,70] |
| Dendrimers | Three dimensional, outward emerging, well defined structures with systematic patterns and recurring units. Highly functionalised polymers resembling biomolecules. | Drug and gene delivery. Limitation involves cytotoxicity to cells. | [62,71] |
| Liposomes | Self-assembling vesicular colloidal structures with a membrane composed of lipid bilayers. | Controlled drug loading and release. | [63,72,73] |
| Viral based nanoparticles | Multivalent, self-assembled protein cages. Synthesised mostly from naturally occurring plant viruses. | Gene therapy and drug delivery. | [74,75] |
| Carbon nanotubes | Graphene sheets rolled up into cylinders. | Drug and protein delivery and gene therapy. | [76,77,78,79] |
| Quantum dots | Semiconducting Nanocrystals with a size range of 2–10 nm | Drug delivery in photo-thermal and photodynamic therapy combination properties, imaging and immunosensing. | [79,80] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
R. Mokoena, D.; P. George, B.; Abrahamse, H. Enhancing Breast Cancer Treatment Using a Combination of Cannabidiol and Gold Nanoparticles for Photodynamic Therapy. Int. J. Mol. Sci. 2019, 20, 4771. https://doi.org/10.3390/ijms20194771
R. Mokoena D, P. George B, Abrahamse H. Enhancing Breast Cancer Treatment Using a Combination of Cannabidiol and Gold Nanoparticles for Photodynamic Therapy. International Journal of Molecular Sciences. 2019; 20(19):4771. https://doi.org/10.3390/ijms20194771
Chicago/Turabian StyleR. Mokoena, Dimakatso, Blassan P. George, and Heidi Abrahamse. 2019. "Enhancing Breast Cancer Treatment Using a Combination of Cannabidiol and Gold Nanoparticles for Photodynamic Therapy" International Journal of Molecular Sciences 20, no. 19: 4771. https://doi.org/10.3390/ijms20194771
APA StyleR. Mokoena, D., P. George, B., & Abrahamse, H. (2019). Enhancing Breast Cancer Treatment Using a Combination of Cannabidiol and Gold Nanoparticles for Photodynamic Therapy. International Journal of Molecular Sciences, 20(19), 4771. https://doi.org/10.3390/ijms20194771