
Evaluation of Not-Activated and Activated PRP in Hair Loss Treatment: Role of Growth Factor and Cytokine Concentrations Obtained by Different Collection Systems

 ,
, 
Abstract
:
1. Introduction
2. Results
2.1. A-PRP Treatment Population
2.2. AA-PRP Treatment Population
2.3. Growth Factor Quantification
3. Discussion
4. Materials and Methods
4.1. Study Overview
4.2. A-PRP Patient Population and Randomization
4.3. AA-PRP Patient Population
4.4. A-PRP Procedures
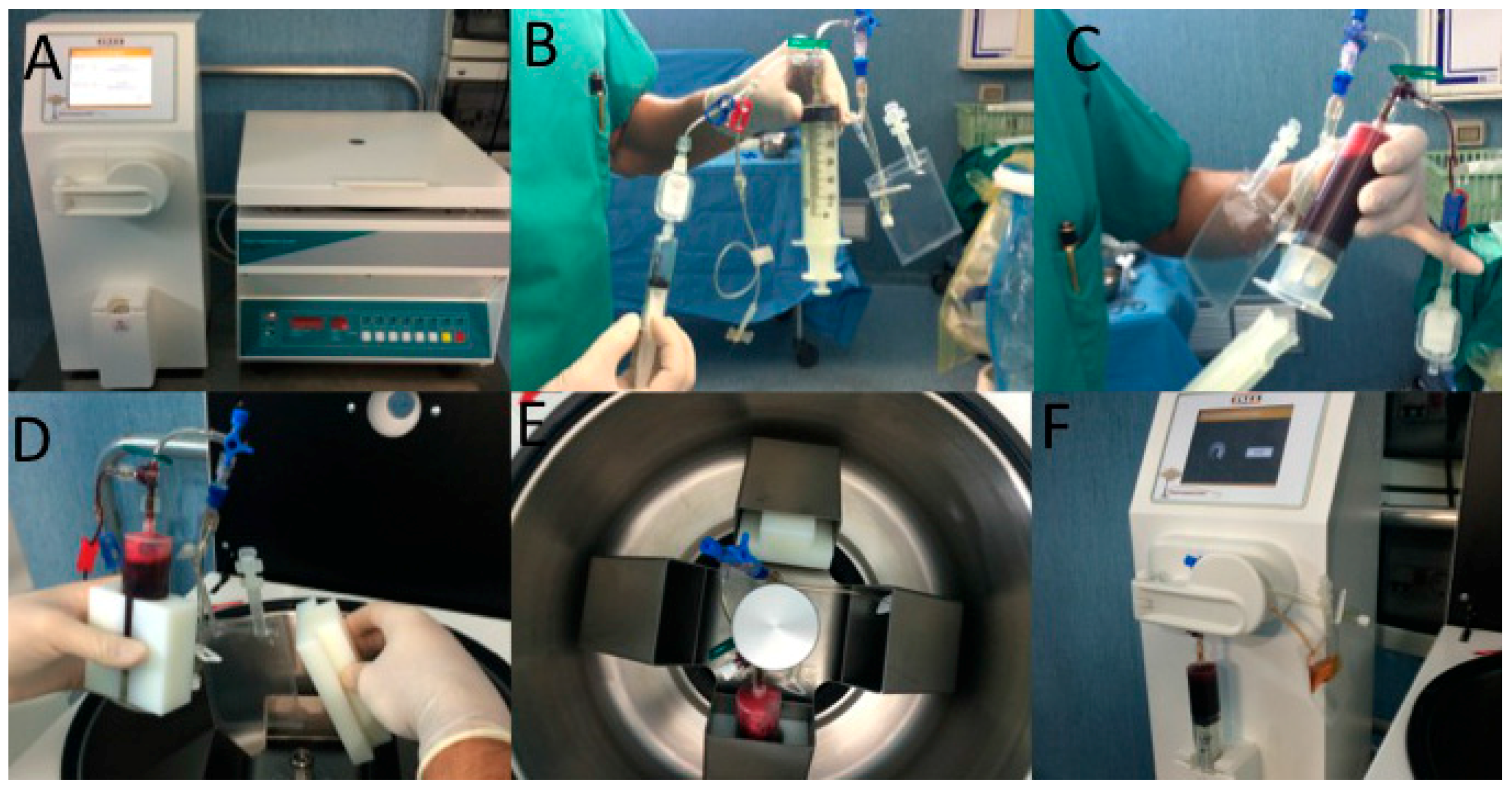
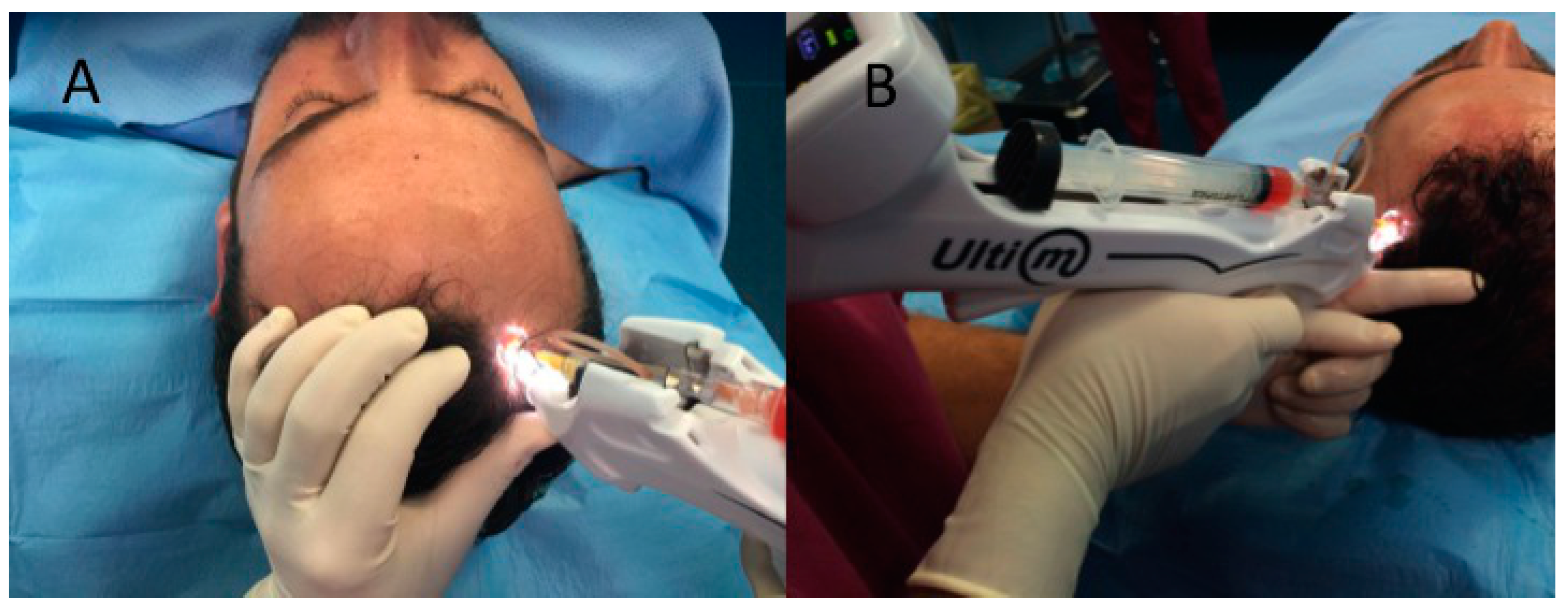
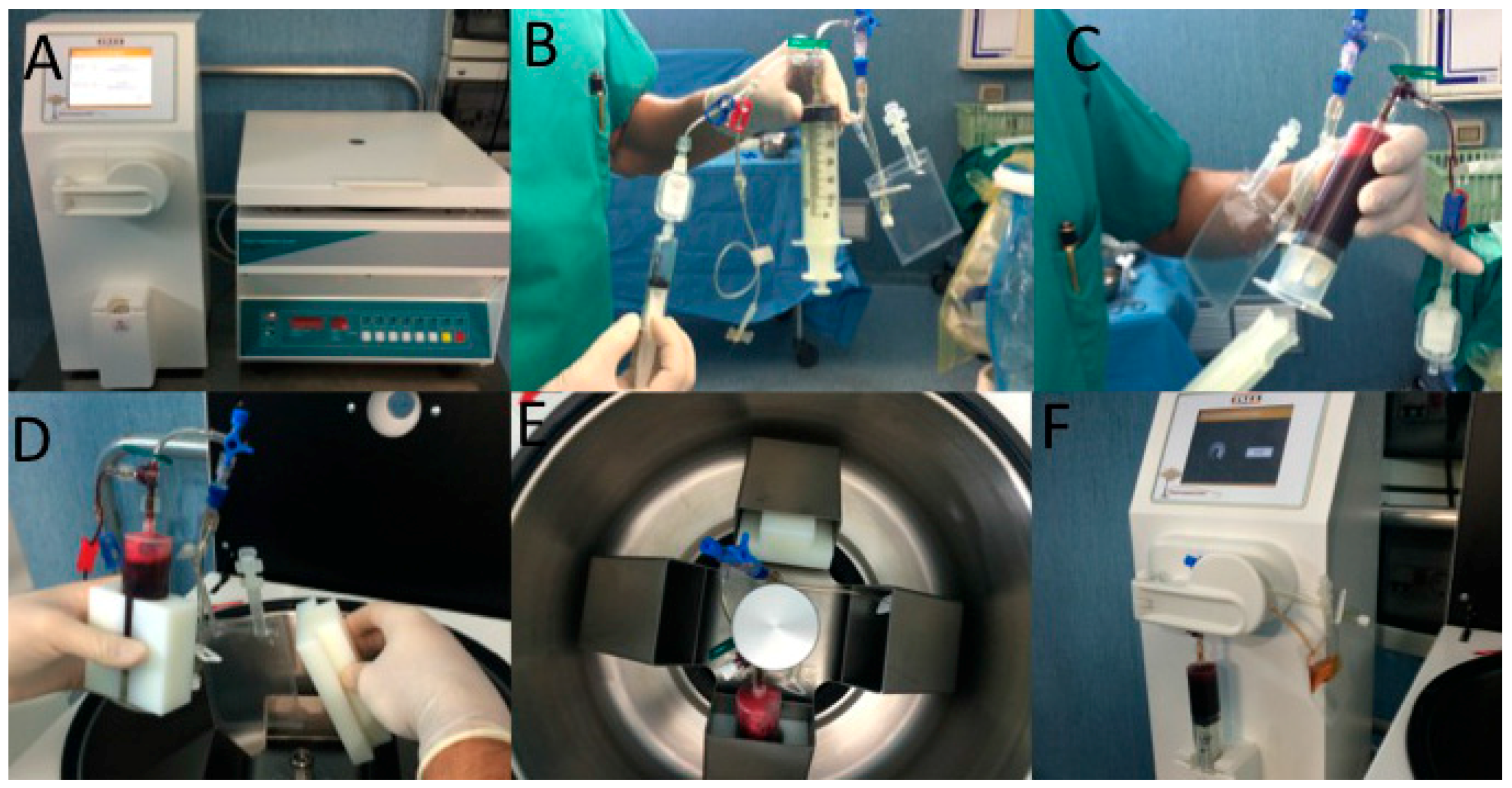
4.4.1. A-PRP Preparation and Delivery
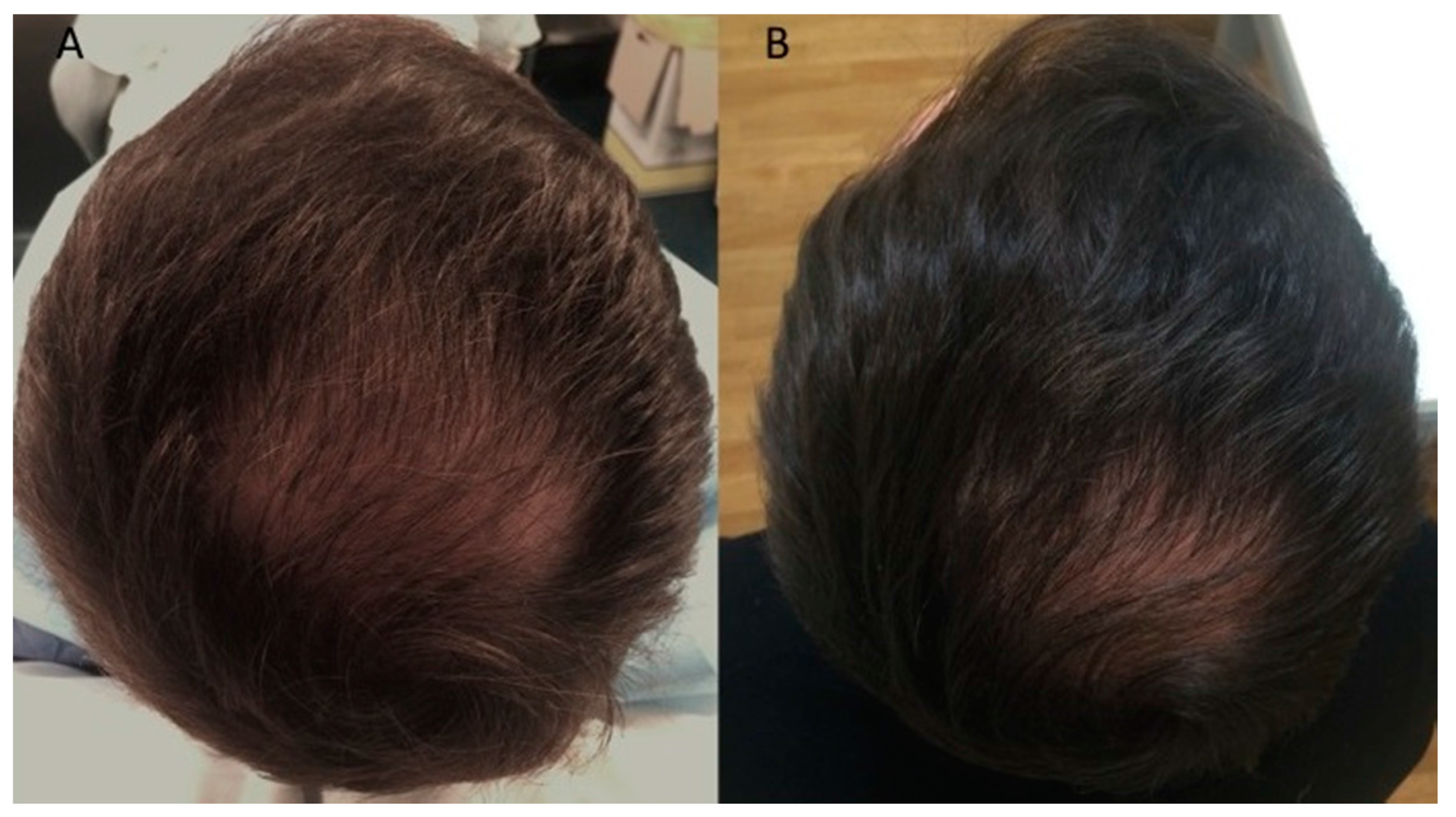
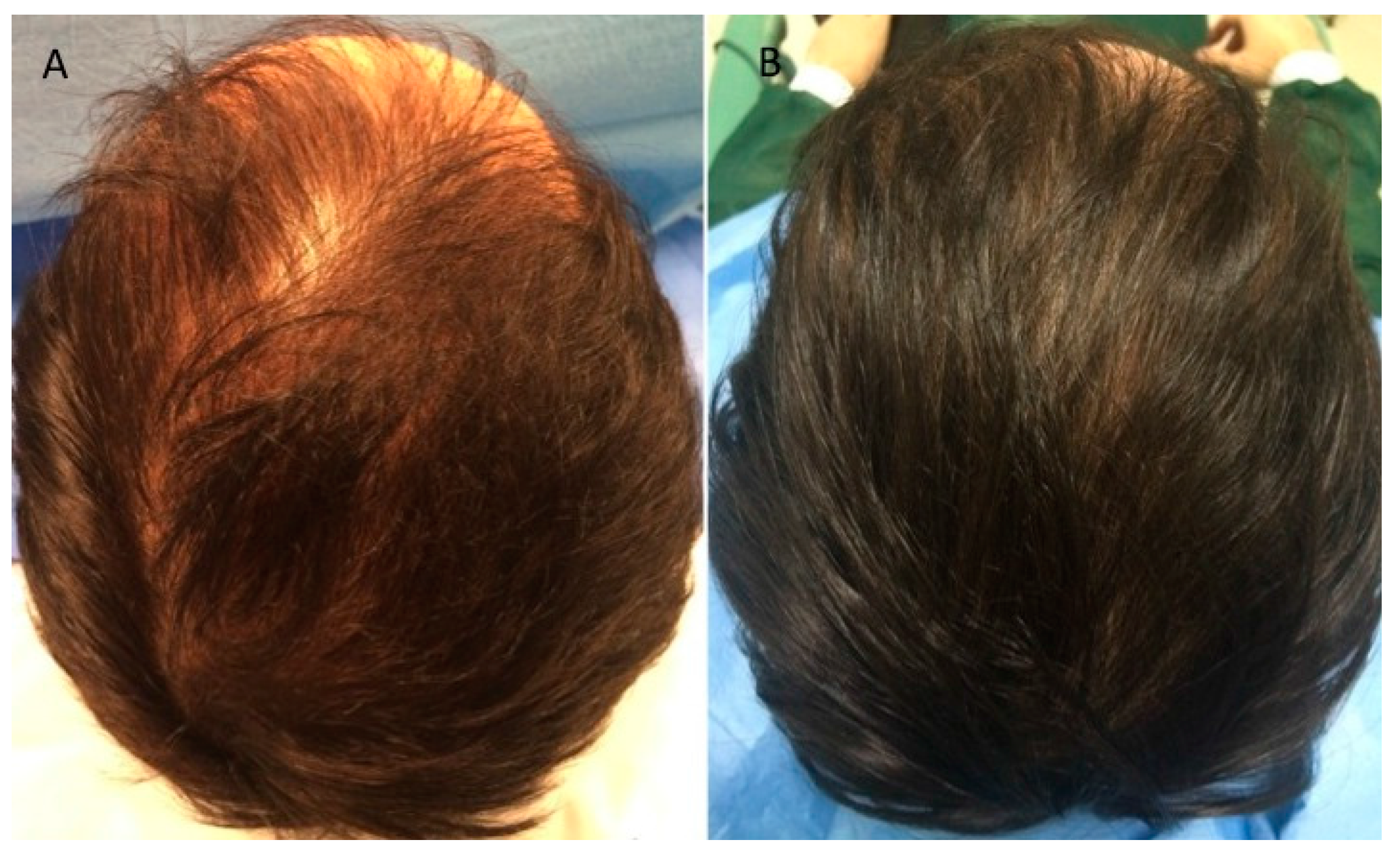
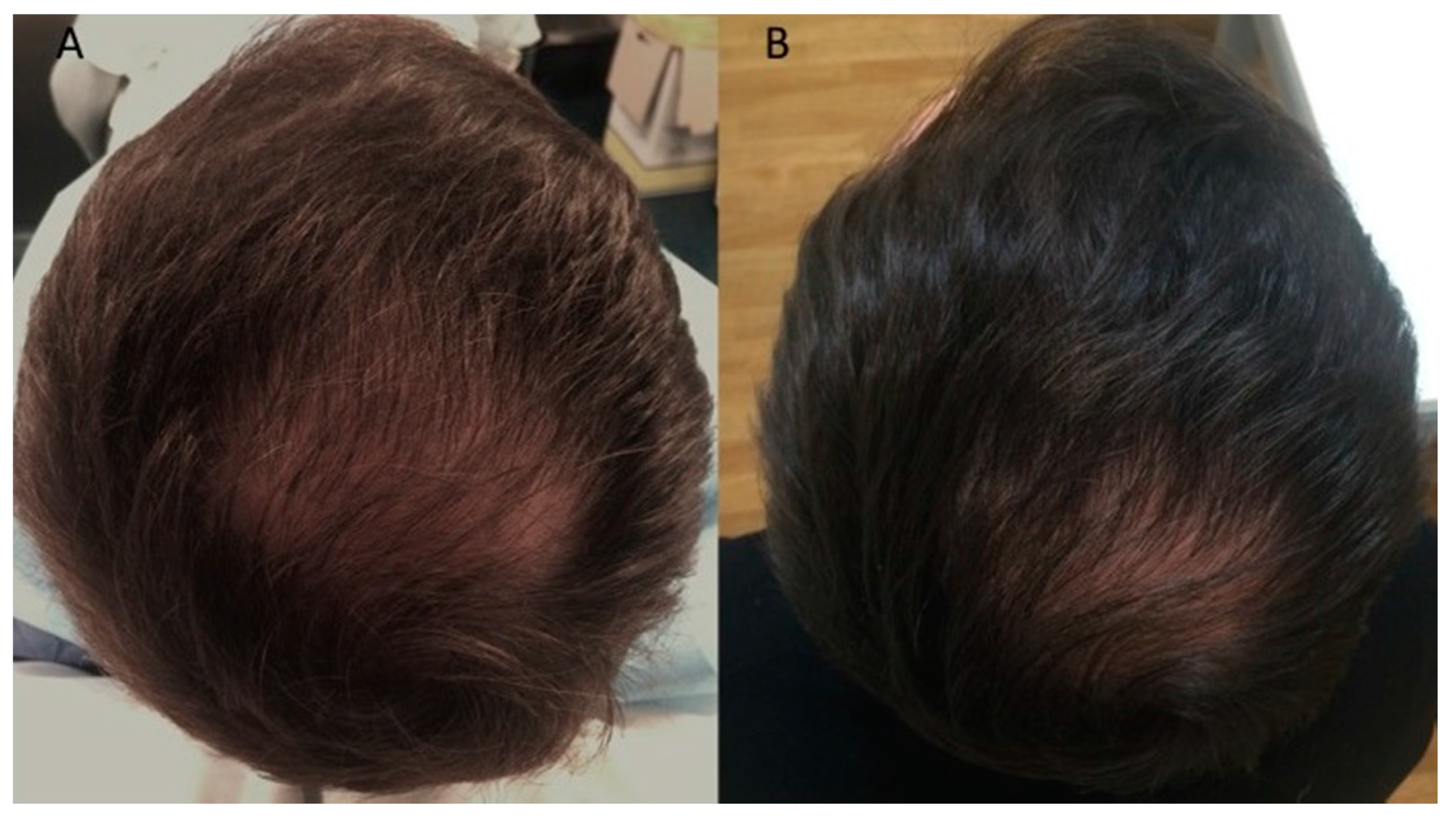
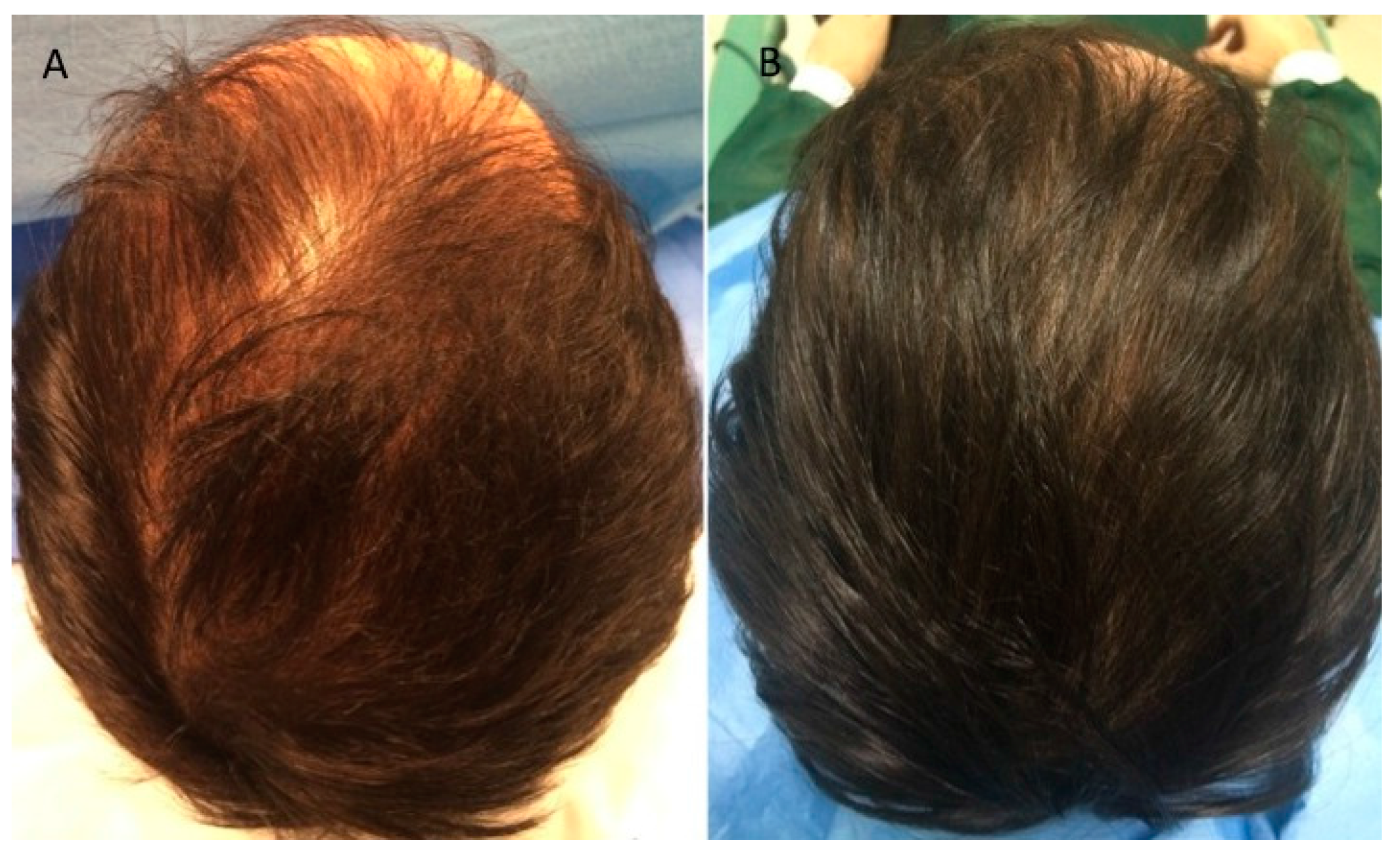
4.4.2. Assessment of Hair Growth Parameters
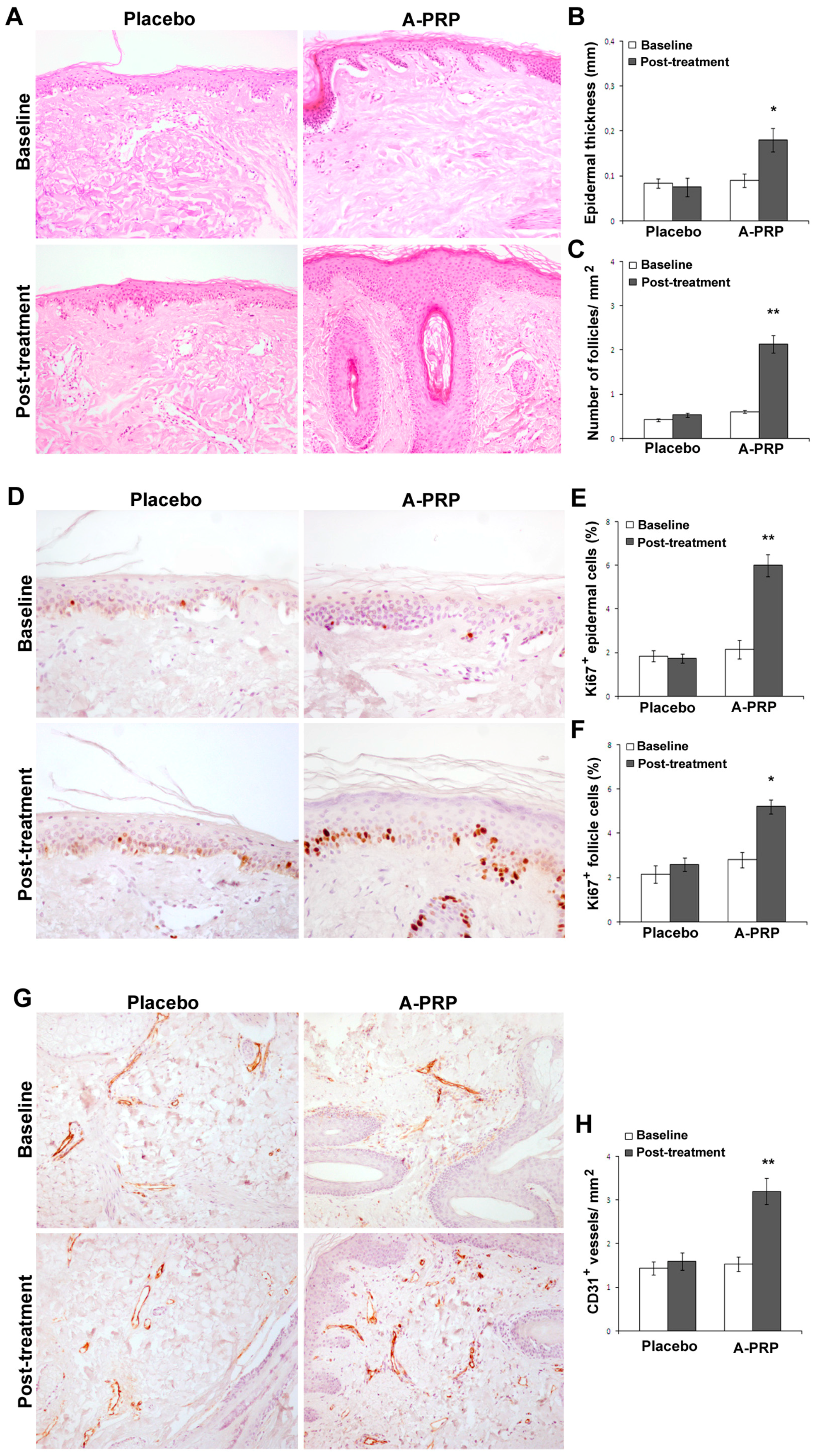
4.4.3. Histological Evaluation
4.4.4. Immunohistochemistry
4.4.5. Growth Factors Quantification
4.4.6. Statistical Analysis
4.5. AA-PRP Procedures
4.5.1. AA-PRP Preparation and Delivery
4.5.2. Assessment of Hair Growth Parameters
4.5.3. Growth Factor Quantification
4.5.4. Statistical Analysis
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Ellis, J.A.; Sinclair, R.; Harrap, S.B. Androgenetic alopecia: Pathogenesis and potential for therapy. Expert Rev. Mol. Med. 2002, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rogers, N.E.; Avram, M.R. Medical treatments for male and female pattern hair loss. J. Am. Acad. Dermatol. 2008, 59, 547–566. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Mysore, V. Classifications of patterned hair loss: A review. J. Cutan. Aesthet. Surg. 2016, 9, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Levy, L.L.; Emer, J.J. Female pattern alopecia: Current perspectives. Int. J. Women Health 2013, 5, 541–556. [Google Scholar]
- Rousso, D.E.; Kim, S.W. A review of medical and surgical treatment options for androgenetic alopecia. JAMA Facial Plast. Surg. 2014, 16, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, E.S.; Boychenko, O.; Bernstein, R.M. Update on the pathogenesis, genetics and medical treatment of patterned hair loss. J. Drugs Dermatol. 2010, 9, 1412–1419. [Google Scholar] [PubMed]
- Price, V.H.; Roberts, J.L.; Hordinsky, M.; Olsen, E.A.; Savin, R.; Bergfeld, W.; Fiedler, V.; Lucky, A.; Whiting, D.A.; Pappas, F.; et al. Lack of efficacy of finasteride in postmenopausal women with androgenetic alopecia. J. Am. Acad. Dermatol. 2000, 43, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Imperato-McGinley, J.; Guerrero, L.; Gautier, T.; Peterson, R.E. Steroid 5α-reductase deficiency in man: An inherited form of male pseudohermaphroditism. Science 1974, 186, 1213–1215. [Google Scholar] [CrossRef] [PubMed]
- Drake, L.; Hordinsky, M.; Fiedler, V.; Swinehart, J.; Unger, W.P.; Cotterill, P.C.; Thiboutot, D.M.; Lowe, N.; Jacobson, C.; Whiting, D.; et al. The effects of finasteride on scalp skin and serum androgen levels in men with androgenetic alopecia. J. Am. Acad. Dermatol. 1999, 41, 550–554. [Google Scholar] [PubMed]
- Van Neste, D.; Fuh, V.; Sanchez-Pedreno, P.; Lopez-Bran, E.; Wolff, H.; Whiting, D.; Roberts, J.; Kopera, D.; Stene, J.J.; Calvieri, S.; et al. Finasteride increases anagen hair in men with androgenetic alopecia. Br. J. Dermatol. 2000, 143, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, K.D.; Olsen, E.A.; Whiting, D.; Savin, R.; DeVillez, R.; Bergfeld, W.; Price, V.H.; van Neste, D.; Roberts, J.L.; Hordinsky, M.; et al. Finasteride in the treatment of men with androgenetic alopecia. J. Am. Acad. Dermatol. 1998, 39, 578–589. [Google Scholar] [CrossRef]
- Savin, R.C. Use of topical minoxidil in the treatment of male pattern baldness. J. Am. Acad. Dermatol. 1987, 16, 696–704. [Google Scholar] [CrossRef]
- Whiting, D.A.; Jacobson, C. Treatment of female androgenetic alopecia with minoxidil 2%. Int. J. Dermatol. 1992, 31, 800–804. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.A.; Dunlap, F.E.; Funicella, T.; Koperski, J.A.; Swinehart, J.M.; Tschen, E.H.; Trancik, R.J. A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. J. Am. Acad. Dermatol. 2002, 47, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, R.; Arano, O.; Nishikawa, T.; Yamada, H.; Katsuoka, K. Randomized clinical trial comparing 5% and 1% topical minoxidil for the treatment of androgenetic alopecia in Japanese men. J. Dermatol. 2009, 36, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.A.; Weiner, M.S. Topical minoxidil in male pattern baldness: Effects of discontinuation of treatment. J. Am. Acad. Dermatol. 1987, 17, 97–101. [Google Scholar] [CrossRef]
- Nandi, S.; Brown, A.C. Platelet-mimetic strategies for modulating the wound environment and inflammatory responses. Exp. Biol. Med. 2016, 241, 1138–1148. [Google Scholar] [CrossRef] [PubMed]
- Nurden, A.T. Platelets, inflammation and tissue regeneration. Thromb. Haemost. 2011, 105, S13–S33. [Google Scholar] [CrossRef] [PubMed]
- Afifi, L.; Maranda, E.L.; Zarei, M.; Delcanto, G.M.; Falto-Aizpurua, L.; Kluijfhout, W.P.; Jimenez, J.J. Low-level laser therapy as a treatment for androgenetic alopecia. Lasers Surg Med. 2017, 49, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.E.; Hardy, C.; Ridgway, J. Keloid management: A retrospective case review on a new approach using surgical excision, platelet-rich plasma, and in-office superficial photon X-ray radiation therapy. Adv. Skin Wound Care 2016, 29, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.R.; Ramesh, A.V.; Dwarkanath, C.D.; Naik, M.S.; Chinnappa, A.B. Use of autologous platelet rich plasma to treat gingival recession in esthetic periodontal surgery. J. Indian Soc. Periodontol. 2013, 17, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Klosová, H.; Štětinský, J.; Bryjová, I.; Hledík, S.; Klein, L. Objective evaluation of the effect of autologous platelet concentrate on post-operative scarring in deep burns. Burns 2013, 39, 1263–1276. [Google Scholar] [CrossRef] [PubMed]
- Motolese, A.; Vignati, F.; Antelmi, A.; Saturni, V. Effectiveness of platelet-rich plasma in healing necrobiosis lipoidica diabeticorum ulcers. Clin. Exp. Dermatol. 2015, 40, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Gawdat, H.I.; Hegazy, R.A.; Fawzy, M.M.; Fathy, M. Autologous platelet rich plasma: Topical versus intradermal after fractional ablative carbon dioxide laser treatment of atrophic acne scars. Dermatol. Surg. 2014, 40, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Zucker, M.B.; Nachmias, V.T. Platelet activation. Arteriosclerosis 1985, 5, 2–18. [Google Scholar] [CrossRef]
- Uebel, C.O.; da Silva, J.B.; Cantarelli, D.; Martins, P. The role of platelet plasma growth factors in male pattern baldness surgery. Plast. Reconstr. Surg. 2006, 118, 1458–1466. [Google Scholar] [CrossRef]
- Cervelli, V.; Garcovich, S.; Bielli, A.; Cervelli, G.; Curcio, B.C.; Scioli, M.G.; Orlandi, A.; Gentile, P. The effect of autologous activated platelet rich plasma (AA-PRP) injection on pattern hair loss: Clinical and histomorphometric evaluation. BioMed Res. Int. 2014, 2014, 760709. [Google Scholar] [CrossRef] [PubMed]
- Gkini, M.A.; Kouskoukis, A.E.; Tripsianis, G.; Rigopoulos, D.; Kouskoukis, K. Study of platelet-rich plasma injections in the treatment of androgenetic alopecia through an one-year period. J. Cutan. Aesthet. Surg. 2014, 7, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Born, G.V.R. Aggregation of blood platelets by adenosine diphosphate and its reversal. Nature 1962, 194, 927–929. [Google Scholar] [CrossRef] [PubMed]
- Kiso, M.; Hamazaki, T.S.; Itoh, M.; Kikuchi, S.; Nakagawa, H.; Okochi, H. Synergistic effect of PDGF and FGF2 for cell proliferation and hair inductive activity in murine vibrissal dermal papilla in vitro. J. Dermatol. Sci. 2015, 79, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Hodak, E.; Gottlieb, A.B.; Anzilotti, M.; Krueger, J.G. The insulin-like growth factor 1 receptor is expressed by epithelial cells with proliferative potential in human epidermis and skin appendages: Correlation of increased expression with epidermal hyperplasia. J. Investig. Dermatol. 1996, 106, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Ristow, H.J.; Messmer, T.O. Basic fibroblast growth-factor and insulin-like growth factor-I are strong mitogens for cultured mouse keratinocytes. J. Cell Physiol. 1988, 137, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Hashimoto, K.; Hashiro, M.; Yoshimasa, H.; Yoshikawa, K. Modulation of growth and differentiation in normal human keratinocytes by transforming growth-factor-β. J. Cell Physiol. 1990, 145, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Shipley, G.D.; Pittelkow, M.R.; Wille, J.J.; Scott, R.E.; Moses, H.L. Reversible inhibition of normal human prokeratinocyte proliferation by type-β transforming growth factor-growth inhibitor in serum-free medium. Cancer Res. 1986, 46, 2068–2071. [Google Scholar] [PubMed]
- Pierce, G.F.; Mustoe, T.A.; Lingelbach, J.; Masakowski, V.R.; Griffin, G.L.; Senior, R.M.; Deuel, T.F. Platelet-derived growth-factor and transforming growth factor-β enhance tissue-repair activities by unique mechanisms. J. Cell Biol. 1989, 109, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.J.; Choi, H.I.; Choi, D.K.; Sohn, K.C.; Im, M.; Seo, Y.J.; Lee, Y.H.; Lee, J.H.; Lee, Y. Autologous platelet-rich plasma: A potential therapeutic tool for promoting hair growth. Dermatol. Surg. 2012, 38, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Greco, V.; Chen, T.; Rendl, M.; Schober, M.; Pasolli, H.A.; Stokes, N.; Dela Cruz-Racelis, J.; Fuchs, E. A two-step mechanism for stem cell activation during hair regeneration. Cell Stem Cell 2009, 4, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.J.; Cobb, M.H. Mitogen-activated protein kinase pathways. Curr. Opin. Cell Biol. 1997, 9, 180–186. [Google Scholar] [CrossRef]
- Lichtenberger, B.M.; Mastrogiannaki, M.; Watt, F.M. Epidermal β-catenin activation remodels the dermis via paracrine signalling to distinct fibroblast lineages. Nat. Commun. 2016, 7, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Singh, N.; Glazer, R.I. Role of AKT1 in 17β-estradiol- and insulin-like growth factor 1 (IGF-1)-dependent proliferation and prevention of apoptosis in MCF-7 breast carcinoma cells. Biochem. Pharmacol. 1999, 58, 425–430. [Google Scholar] [CrossRef]
- Yang, J.; Zhao, S.L.; Yang, X.L.; Zhang, H.; Zheng, P.; Wu, H. Inhibition of B-cell apoptosis is mediated through increased expression of Bcl-2 in patients with rheumatoid arthritis. Int. J. Rheum. Dis. 2016, 19, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Garcovich, S.; Bielli, A.; Scioli, M.G.; Orlandi, A.; Cervelli, V. The effect of platelet-rich plasma in hair regrowth: A randomized placebo-controlled trial. Stem Cells Transl. Med. 2015, 4, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Hamberg, M.; Svensson, J.; Samuelsson, B. Thromboxanes—New group of biologically-active compounds derived from prostaglandin endoperoxides. Proc. Natl. Acad. Sci. USA 1975, 72, 2994–2998. [Google Scholar] [CrossRef] [PubMed]
- Nedelec, B.; Hou, Q.; Sohbi, I.; Choinière, M.; Beauregard, G.; Dykes, R.W. Sensory perception and neuroanatomical structures in normal and grafted skin of burn survivors. Burns 2005, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Campagnolo, L.; Costanza, G.; Francesconi, A.; Arcuri, G.; Moscatelli, I.; Orlandi, A. Sortilin expression is essential for pro-nerve growth factorinduced apoptosis of rat vascular smooth muscle cells. PLoS ONE 2014, 9, e84969. [Google Scholar] [CrossRef] [PubMed]
- Ferlosio, A.; Arcuri, G.; Doldo, E.; Scioli, M.G.; de Falco, S.; Spagnoli, L.G.; Orlandi, A. Age related increase of stem marker expression influences vascular smooth muscle cell properties. Atherosclerosis 2012, 224, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Stasi, M.A.; Scioli, M.G.; Arcuri, G.; Mattera, G.G.; Lombardo, K.; Marcellini, M.; Riccioni, T.; de Falco, S.; Pisano, C.; Spagnoli, L.G.; et al. Propionyl-l-carnitine improves postischemic blood flow recovery and arteriogenetic revascularization and reduces endothelial NADPH-oxidase 4-mediated superoxide production. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Scioli, M.G.; Lo Giudice, P.; Bielli, A.; Tarallo, V.; de Rosa, A.; de Falco, S.; Orlandi, A. Propionyl-l-carnitine enhances wound healing and counteracts microvascular endothelial cell dysfunction. PLoS ONE 2015, 10, e0140697. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hair Growth Parameter | Time | A-PRP Treatment Area | Control Area |
|---|---|---|---|
| Hair Count | Baseline | 122 ± 10 | 126 ± 9 |
| 12 weeks | 158 ± 11 | 127 ± 9 | |
| Hair density, No. per cm2 | Baseline | 218 ± 17 | 225 ± 15 |
| 12 weeks | 282 ± 20 | 227 ± 16 |
| Hair Growth Parameter | Time | Regen AA-PRP | Arthrex AA-PRP |
|---|---|---|---|
| Hair Density, no. per cm2 | Baseline | 283 ± 64 | 160 ± 6 |
| 6 months | 210 ± 40 | 250 ± 12 | |
| Follicular Unit Density, No. per cm2 | Baseline | 103 ± 19 | 77 ± 12 |
| 6 months | 103 ± 24 | 97 ± 7 |
| Protein | Collection System | A-PRP | Ca2+ AA-PRP |
|---|---|---|---|
| PDGF-BB (ng·mL−1) | Regen | 1.2 ± 0.3 | 4.0 ± 2 |
| Arthrex | 1.1 ± 0.6 | 3.0 ± 1 | |
| C-PunT | 1.8 ± 0.4 | - | |
| TGF-β1 (ng·mL−1) | Regen | 11 ± 2 | 15 ± 3 |
| Arthrex | 12 ± 1 | 13 ± 0 | |
| IGF-1 (ng·mL−1) | Regen | 130 ± 20 | 140 ± 20 |
| Arthrex | 150 ± 40 | 150 ± 60 | |
| VEGF (pg·mL−1) | Regen | 61 ± 20 | 210 ± 40 |
| Arthrex | 61 ± 20 | 260 ± 70 | |
| C-PunT | 100 ± 20 | - | |
| FGF (pg·mL−1) | C-PunT | 280 ± 60 | - |
| Case No. | Age, Years | Hamilton–Norwood Classification Stage | Injection Site |
|---|---|---|---|
| 1 | 29 | 2A | Frontal + Temporal |
| 2 | 34 | 2A | Frontal + Temporal |
| 3 | 40 | 3A | Frontal + Temporal |
| 4 | 42 | 3V | Frontal + Vertex |
| 5 | 31 | 3A | Frontal + Temporal |
| 6 | 39 | 3V | Frontal + Vertex |
| 7 | 47 | 3V | Frontal + Vertex |
| 8 | 40 | 3A | Frontal + Temporal |
| 9 | 36 | 2A | Frontal + Temporal |
| 10 | 51 | 4 | Frontal + Temporal + Vertex + Parietal |
| 11 | 35 | 3A | Frontal + Temporal |
| 12 | 31 | 3A | Frontal + Temporal |
| 13 | 43 | 3V | Frontal + Vertex |
| 14 | 36 | 3A | Frontal + Temporal |
| 15 | 32 | 3 | Frontal + Temporal |
| 16 | 61 | 4A | Frontal + Temporal + Vertex + Parietal |
| 17 | 27 | 2A | Frontal + Temporal |
| 18 | 20 | 2 | Frontal |
| Case No. | Age, Years | Hamilton-Norwood Classification Stage | Test Group |
|---|---|---|---|
| 1 | 43 | 3V | Regen |
| 2 | 45 | 3V | Regen |
| 3 | 40 | 3V | Regen |
| 4 | 58 | 3V | Arthrex |
| 5 | 35 | 3A | Arthrex |
| 6 | 24 | 3A–3V | Arthrex |
| Target Protein | ELISA Assay Kit Specifications |
|---|---|
| PDGF-BB | cat # EHPDGFB, Thermo Scientific |
| VEGF | cat # KGH011, Novex Life Technologies |
| IGF-1 | cat # DG100, R&D Systems |
| TGF-β1 | cat # KAC1688, Invitrogen Life Technologies |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gentile, P.; Cole, J.P.; Cole, M.A.; Garcovich, S.; Bielli, A.; Scioli, M.G.; Orlandi, A.; Insalaco, C.; Cervelli, V. Evaluation of Not-Activated and Activated PRP in Hair Loss Treatment: Role of Growth Factor and Cytokine Concentrations Obtained by Different Collection Systems. Int. J. Mol. Sci. 2017, 18, 408. https://doi.org/10.3390/ijms18020408
Gentile P, Cole JP, Cole MA, Garcovich S, Bielli A, Scioli MG, Orlandi A, Insalaco C, Cervelli V. Evaluation of Not-Activated and Activated PRP in Hair Loss Treatment: Role of Growth Factor and Cytokine Concentrations Obtained by Different Collection Systems. International Journal of Molecular Sciences. 2017; 18(2):408. https://doi.org/10.3390/ijms18020408
Chicago/Turabian StyleGentile, Pietro, John P. Cole, Megan A. Cole, Simone Garcovich, Alessandra Bielli, Maria Giovanna Scioli, Augusto Orlandi, Chiara Insalaco, and Valerio Cervelli. 2017. "Evaluation of Not-Activated and Activated PRP in Hair Loss Treatment: Role of Growth Factor and Cytokine Concentrations Obtained by Different Collection Systems" International Journal of Molecular Sciences 18, no. 2: 408. https://doi.org/10.3390/ijms18020408
APA StyleGentile, P., Cole, J. P., Cole, M. A., Garcovich, S., Bielli, A., Scioli, M. G., Orlandi, A., Insalaco, C., & Cervelli, V. (2017). Evaluation of Not-Activated and Activated PRP in Hair Loss Treatment: Role of Growth Factor and Cytokine Concentrations Obtained by Different Collection Systems. International Journal of Molecular Sciences, 18(2), 408. https://doi.org/10.3390/ijms18020408