
Optimal Scanning Protocols for Dual-Energy CT Angiography in Peripheral Arterial Stents: An in Vitro Phantom Study


 ,
,
Abstract
:1. Introduction
2. Results
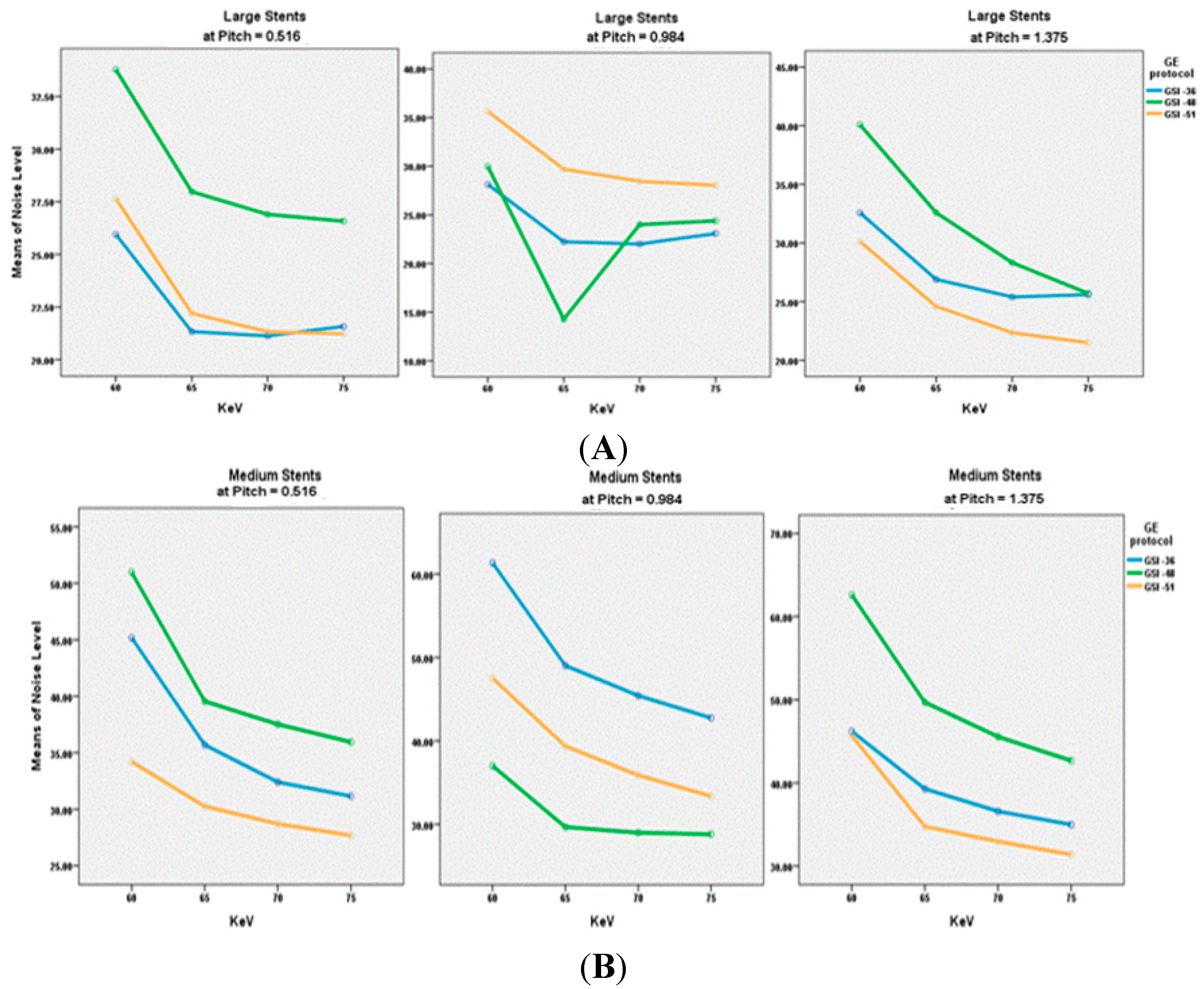
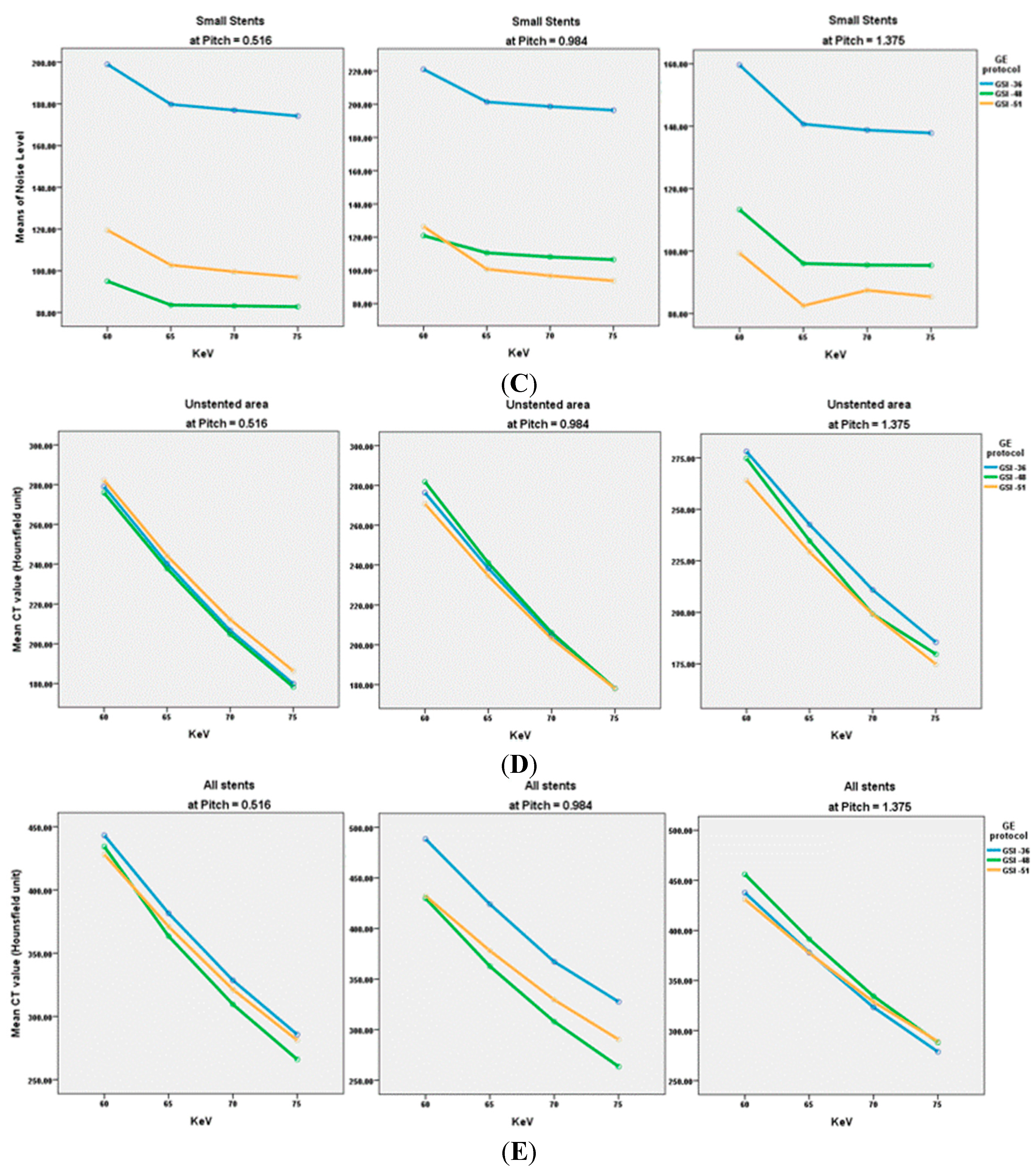
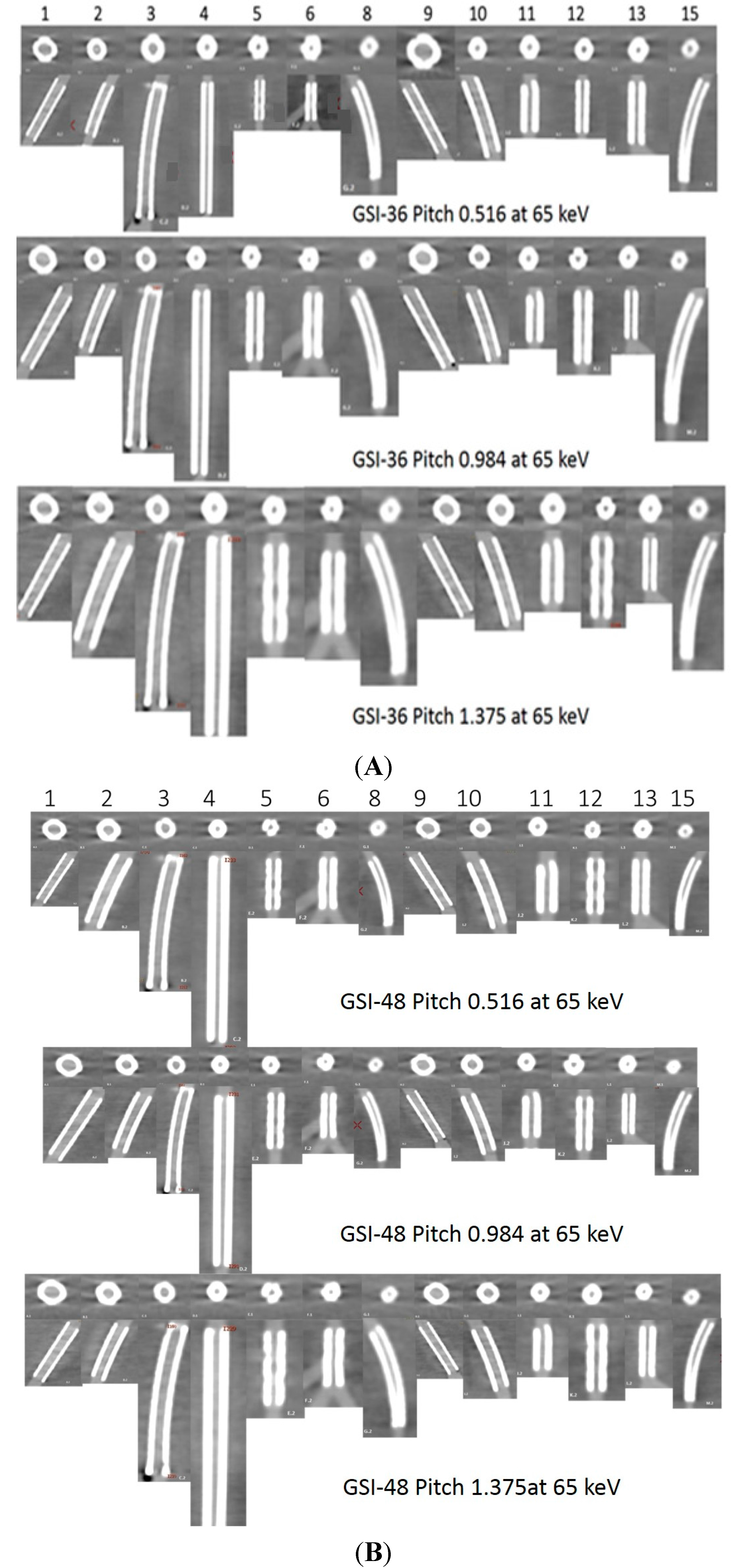
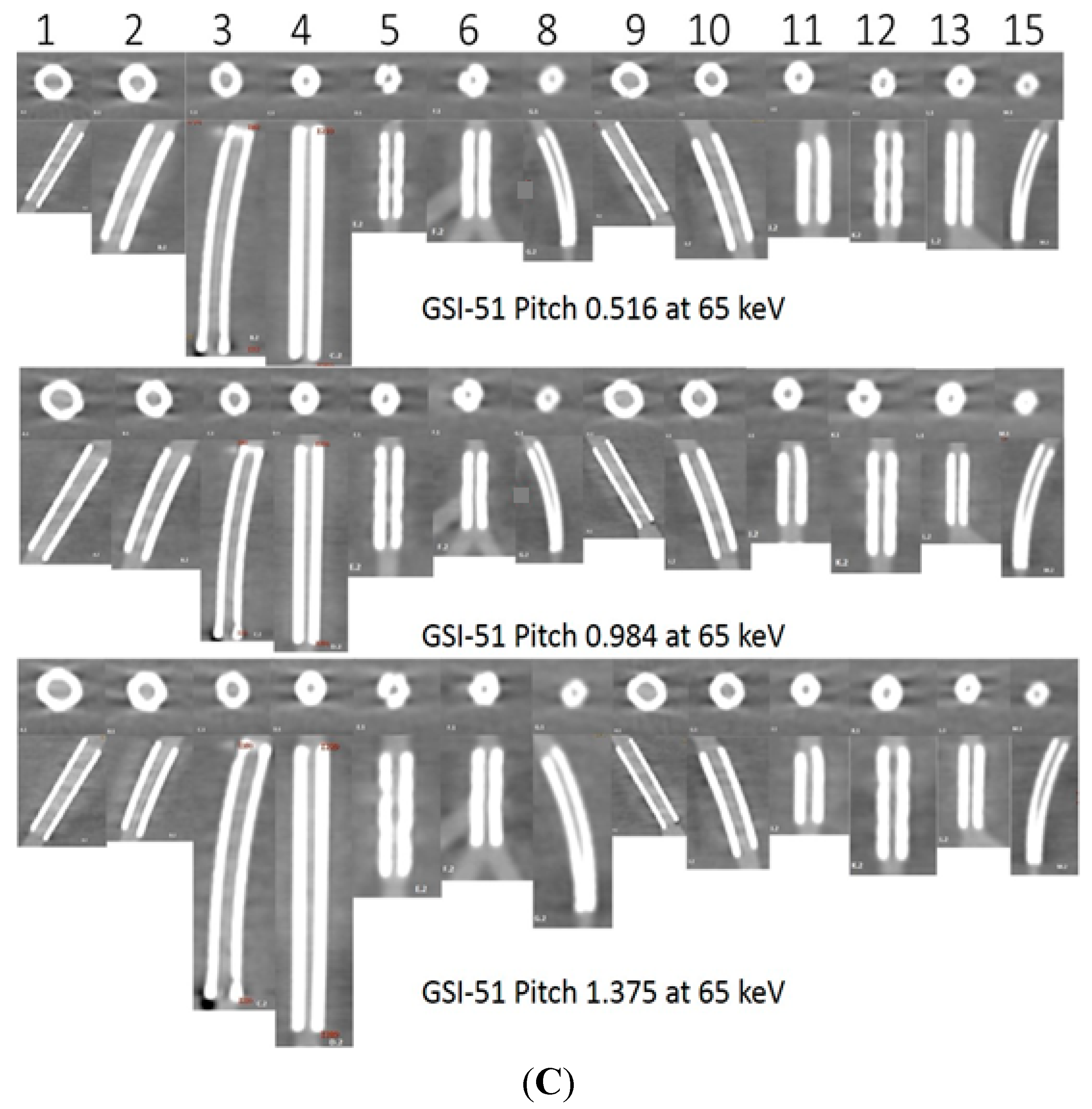
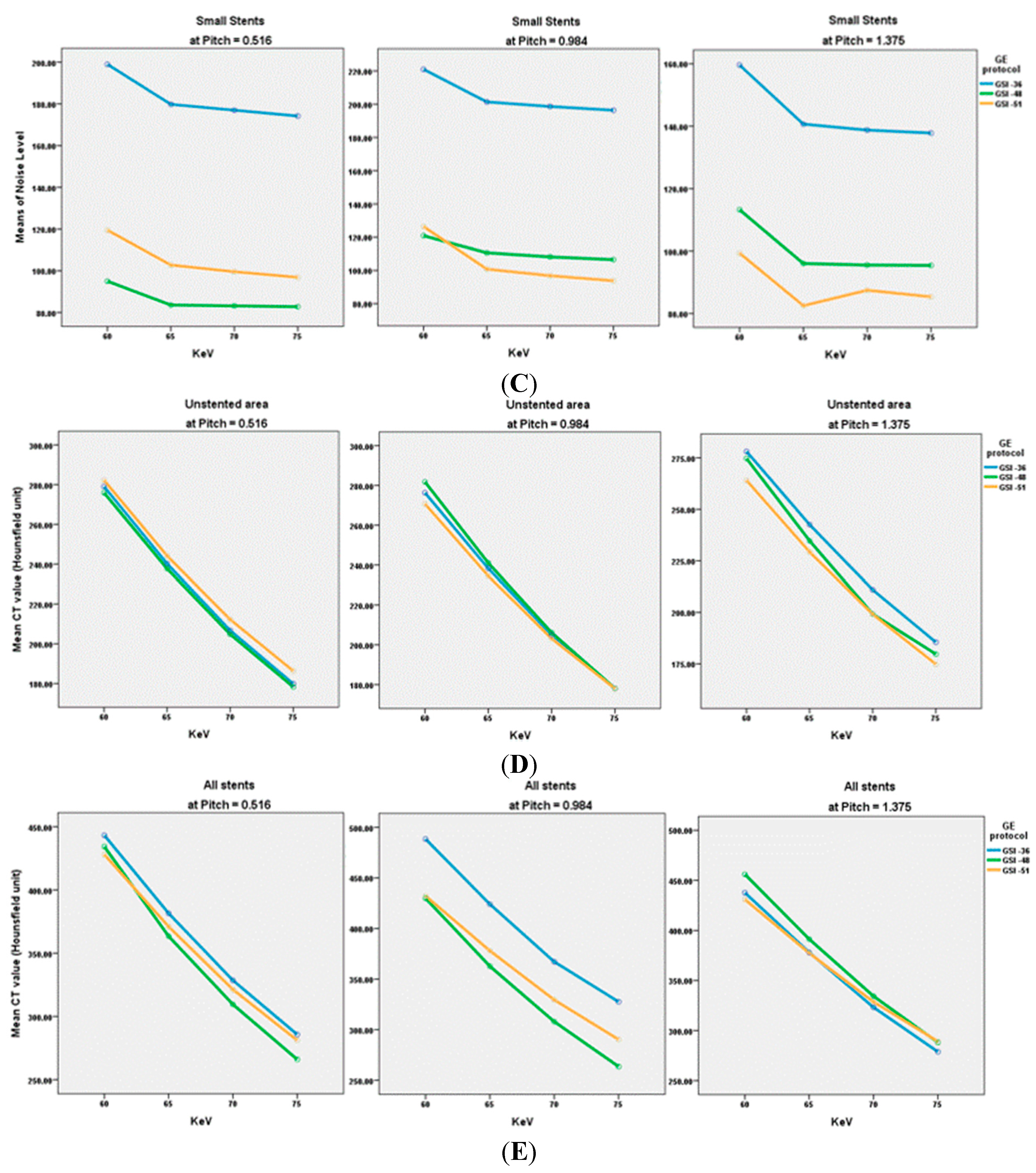
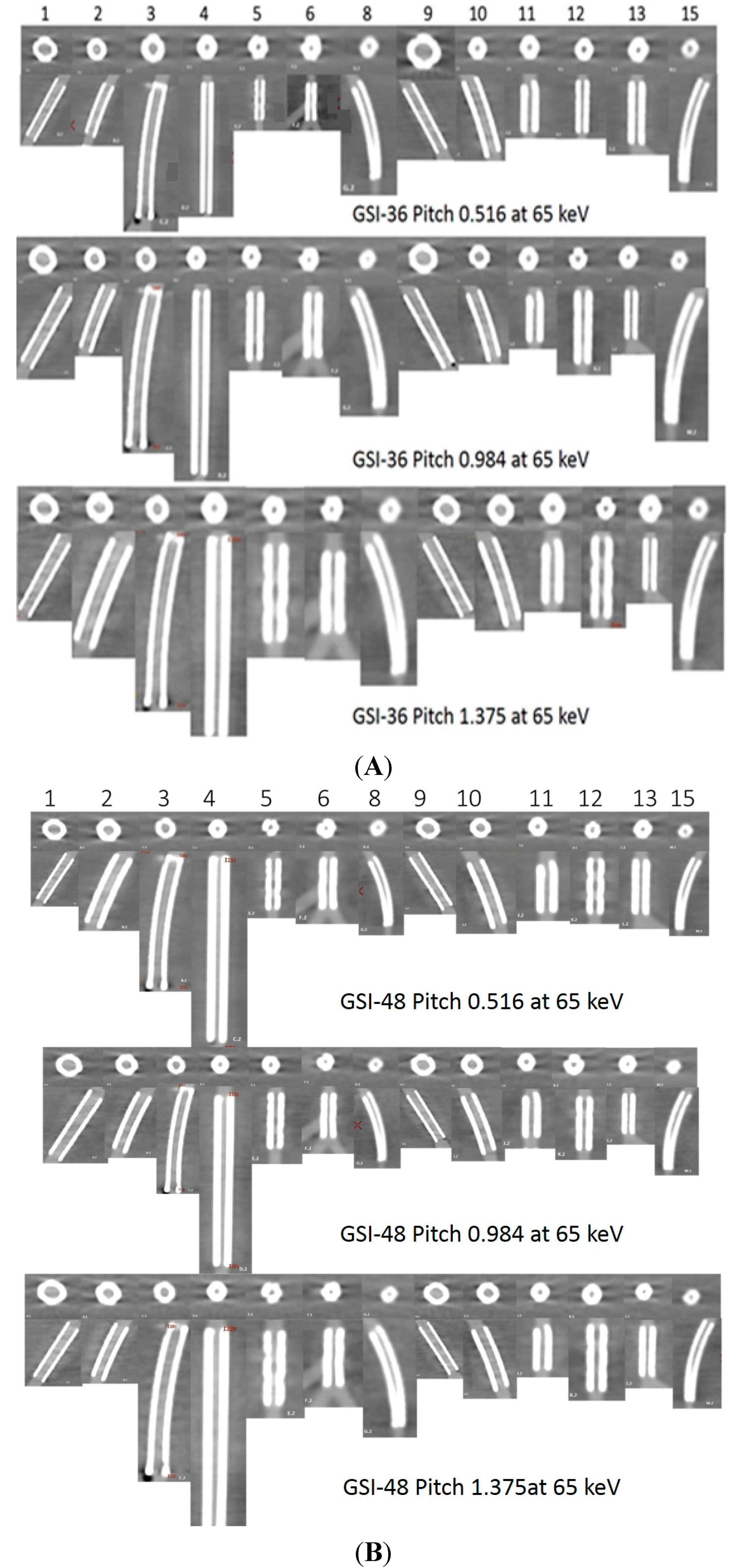
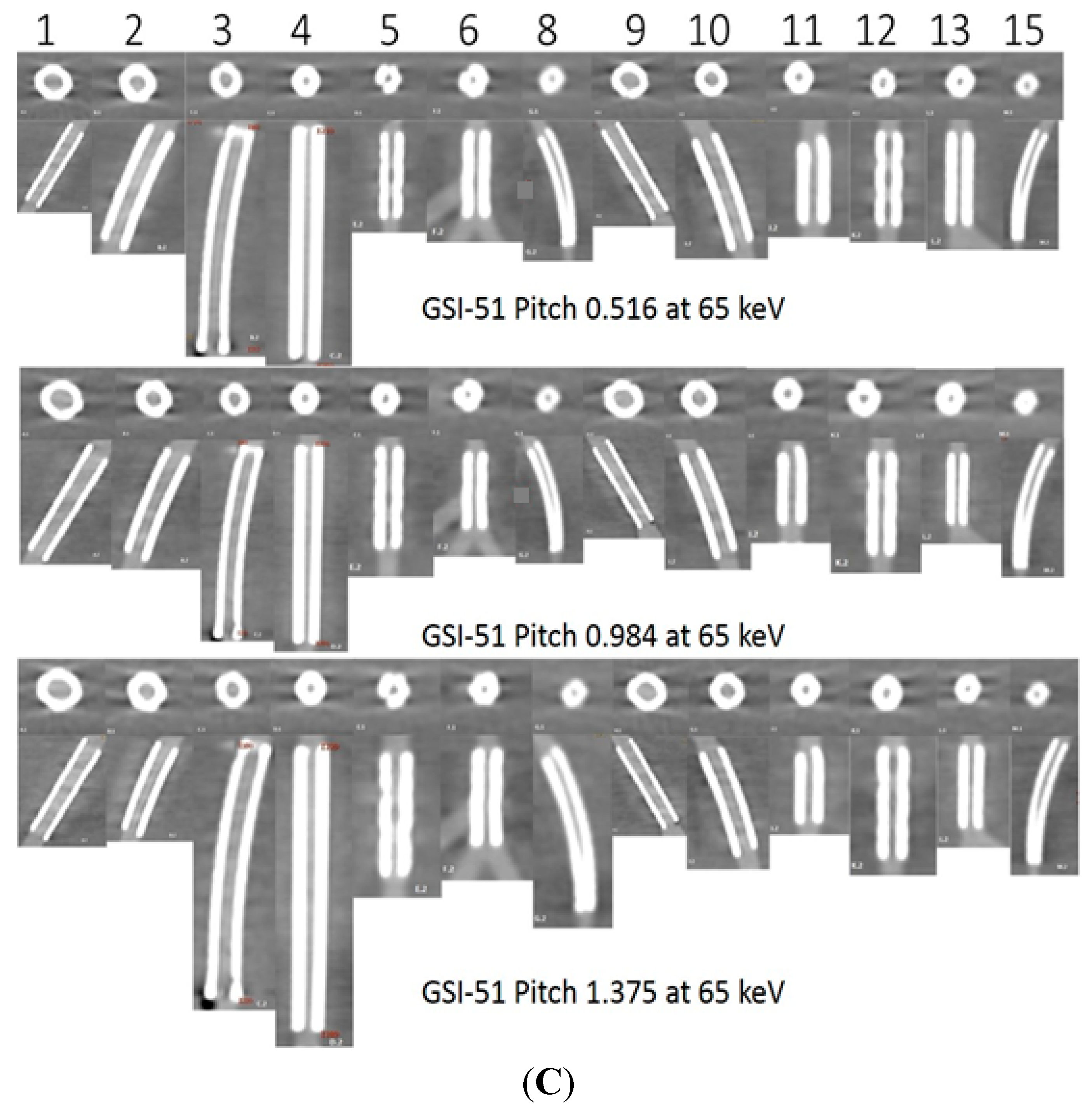
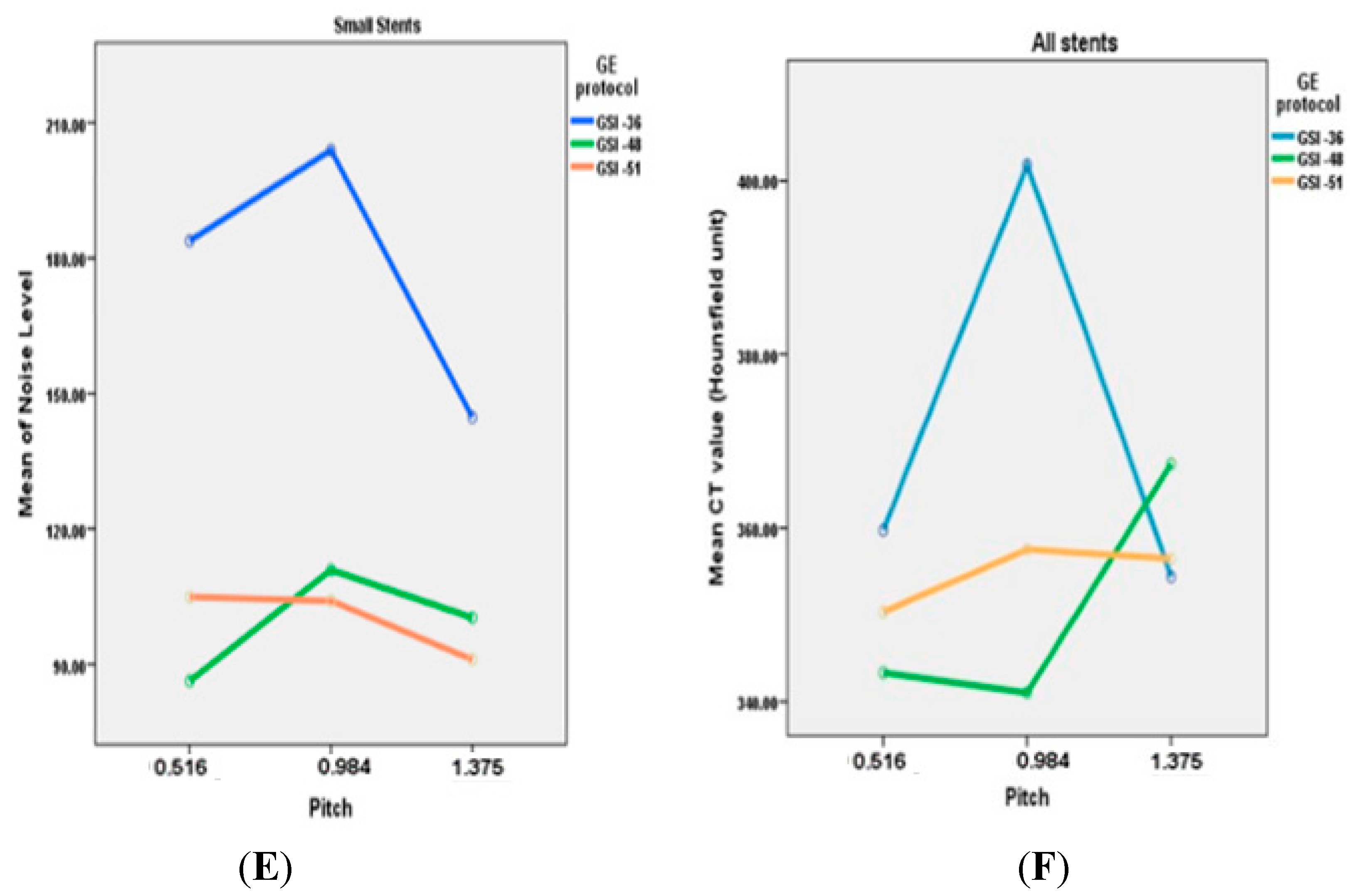
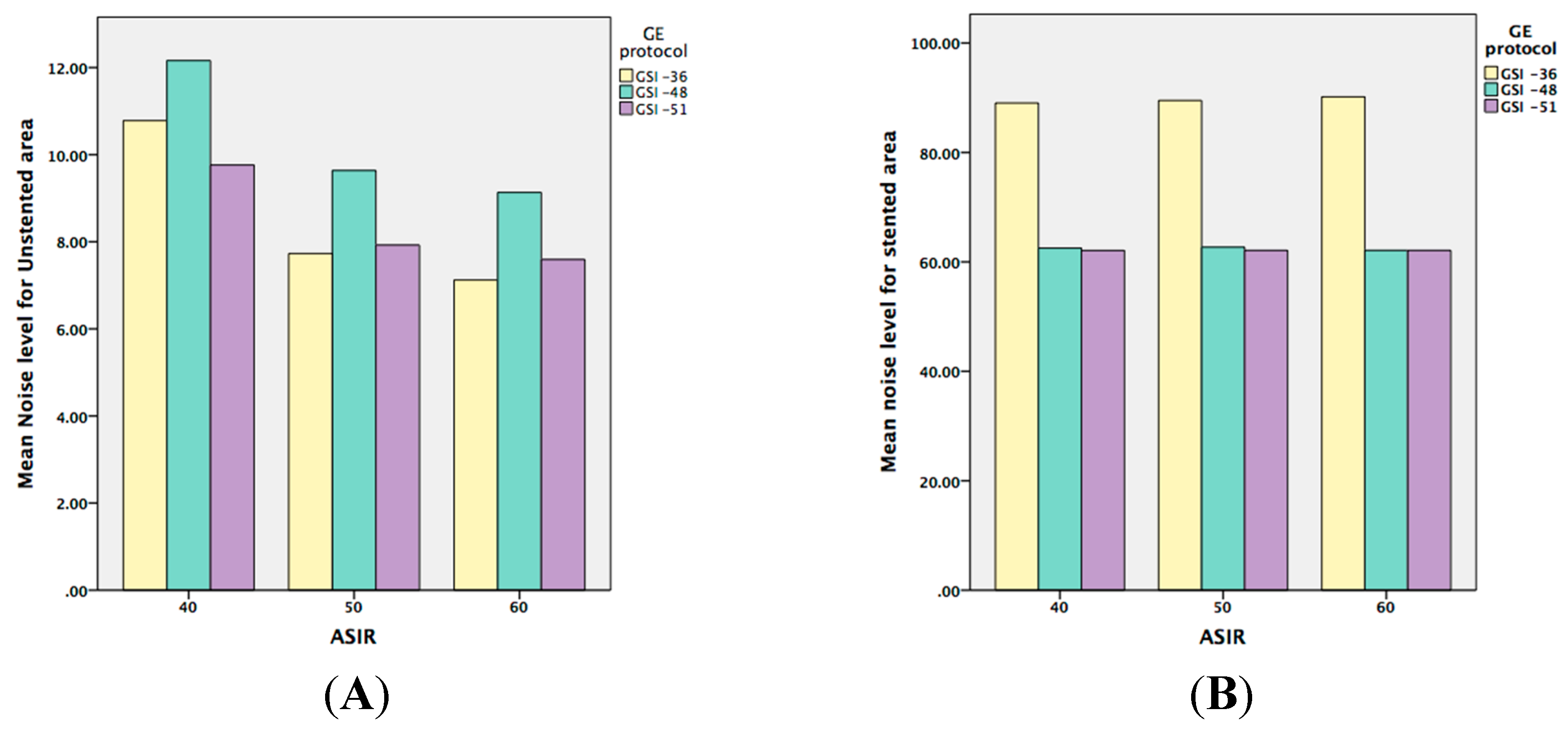
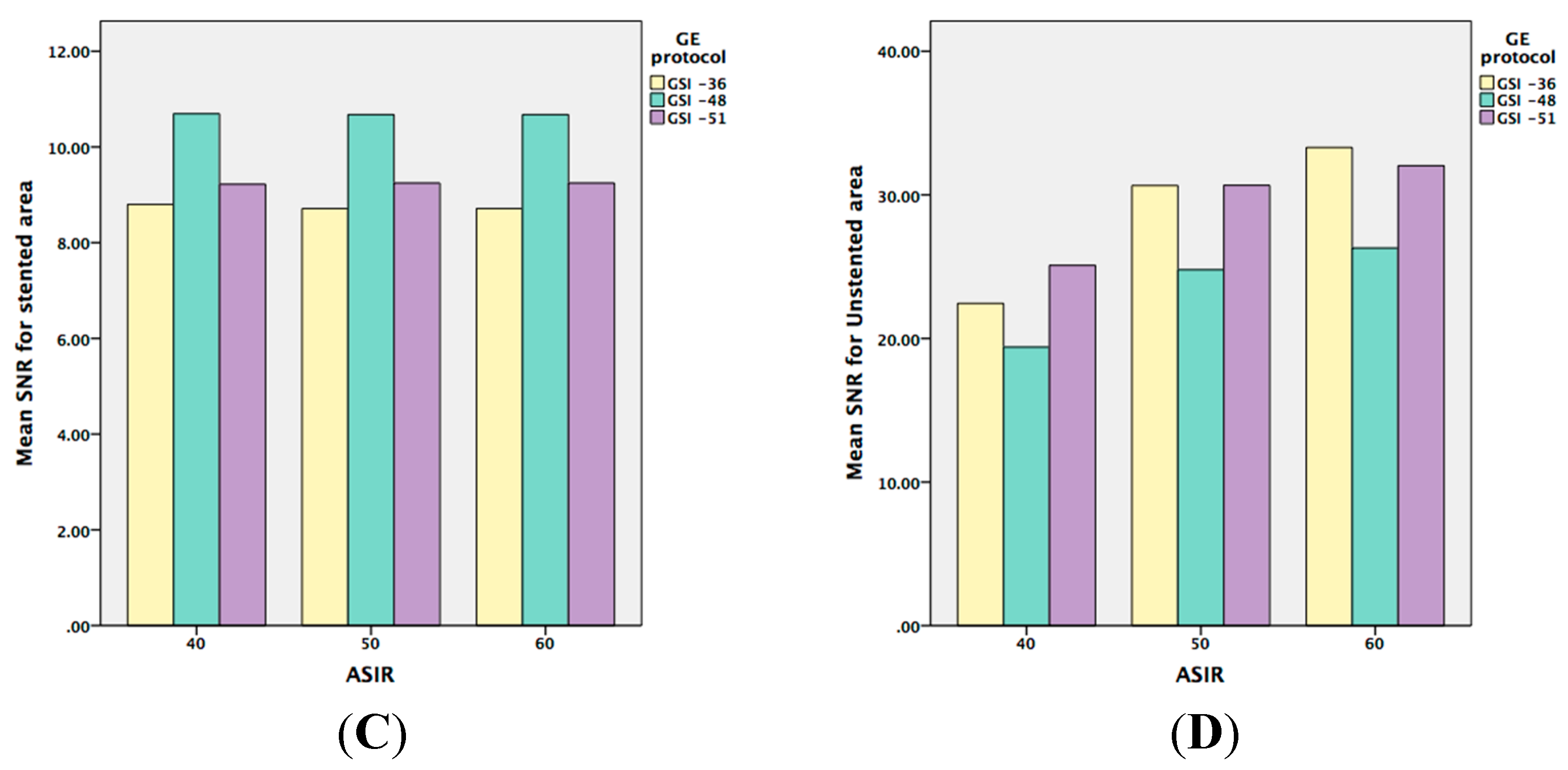
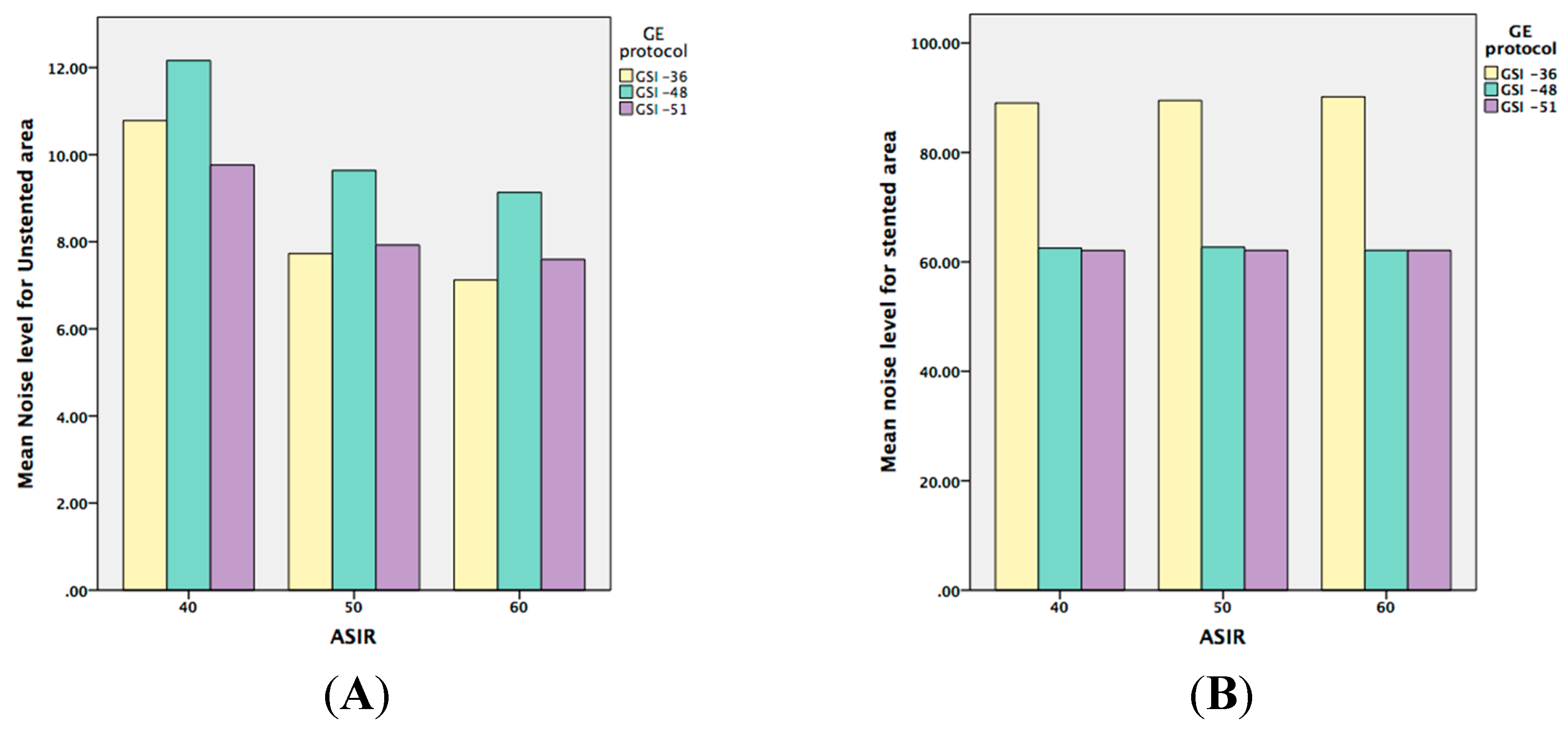
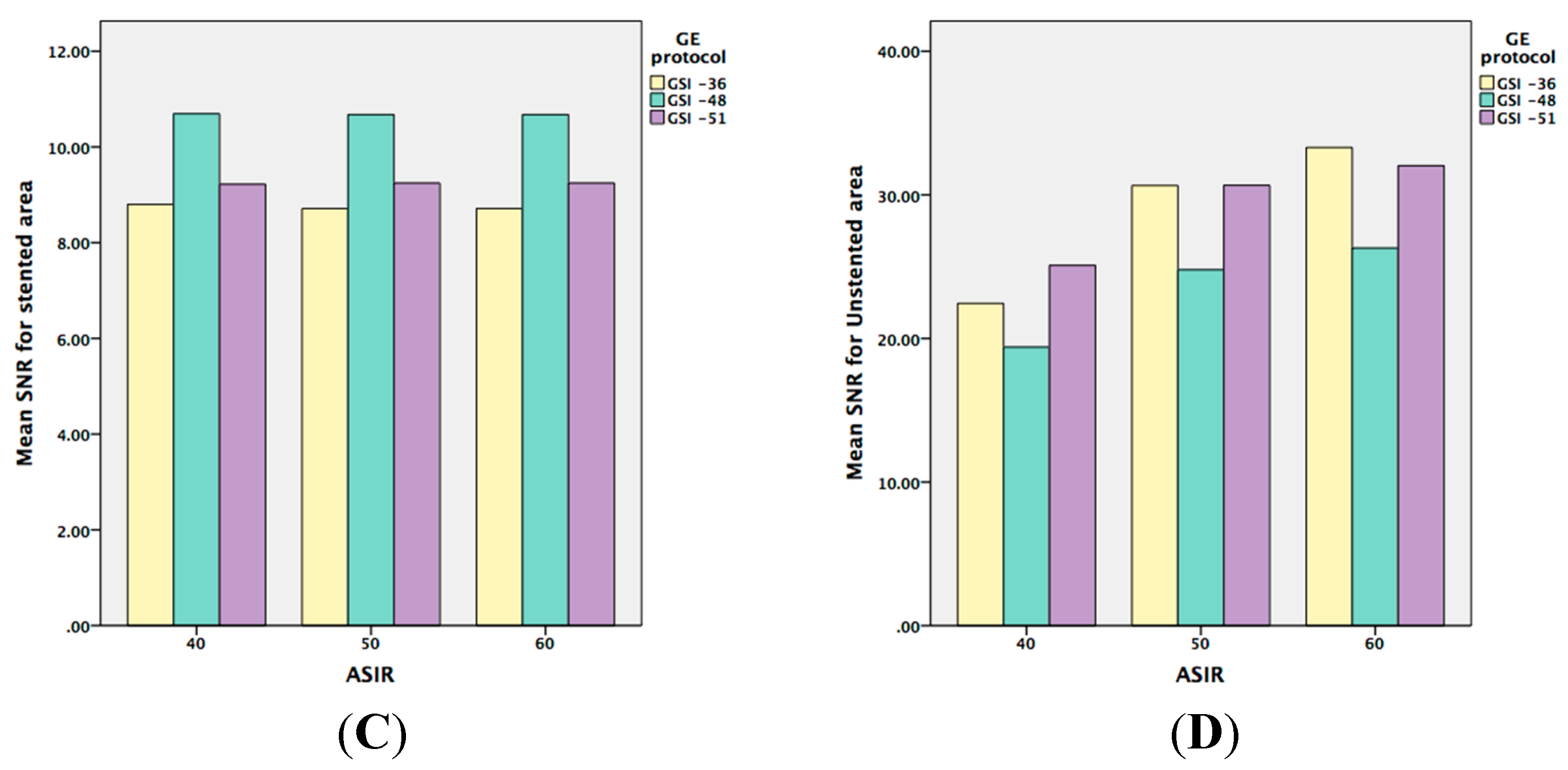
2.1. Image Quality Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Effects | SNR | SNR2 | NL | NL2 | |||||
|---|---|---|---|---|---|---|---|---|---|
| F | P | F | P | F | P | F | P | ||
| GSI | Main effect | 11.806 | 0.001 | 86.658 | 0.000 | 947.509 | 0.000 | 572.661 | 0.000 |
| Pitch | Main effect | 10.992 | 0.002 | 302.411 | 0.000 | 102.664 | 0.000 | 1883.182 | 0.000 |
| KeV | Main effect | 13.424 | 0.000 | 192.161 | 0.000 | 230.042 | 0.000 | 894.644 | 0.000 |
| ASIR | Main effect | NA | NA | 157.416 | 0.000 | NA | NA | 1291.264 | 0.000 |
| GSI * ASIR | Two-factor interaction effect | NA | NA | 3.823 | 0.015 | NA | NA | 27.164 | 0.000 |
| KeV * ASIR | Two-factor interaction effect | NA | NA | 6.133 | 0.001 | NA | NA | 3.652 | 0.010 |
| Pitch * ASIR | Two-factor interaction effect | NA | NA | 1.877 | 0.147 | NA | NA | 68.25 | 0.000 |
| GSI * KeV | Two-factor interaction effect | 0.454 | 0.829 | 16.528 | 0.000 | 0.649 | 0.691 | 120.311 | 0.000 |
| GSI * Pitch | Two-factor interaction effect | 13.708 | 0.000 | 12.793 | 0.000 | 142.367 | 0.000 | 30.586 | 0.000 |
| Pitch * KeV | Two-factor interaction effect | 0.419 | 0.853 | 18.778 | 0.000 | 1.189 | 0.375 | 120.391 | 0.000 |
| GSI * KeV * ASIR | Three-factor interaction effect | NA | NA | 0.457 | 0.920 | NA | NA | 1.727 | 0.123 |
| GSI * Pitch * ASIR | Three-factor interaction effect | NA | NA | 0.634 | 0.742 | NA | NA | 9.842 | 0.000 |
| Pitch * KeV * ASIR | Three-factor interaction effect | NA | NA | 0.558 | 0.853 | NA | NA | 1.326 | 0.268 |
| GSI * Pitch * KeV | Three-factor interaction effect | NA | NA | 21.545 | 0.000 | NA | NA | 118.371 | 0.000 |
2.2. Effect of keV on Image Quality
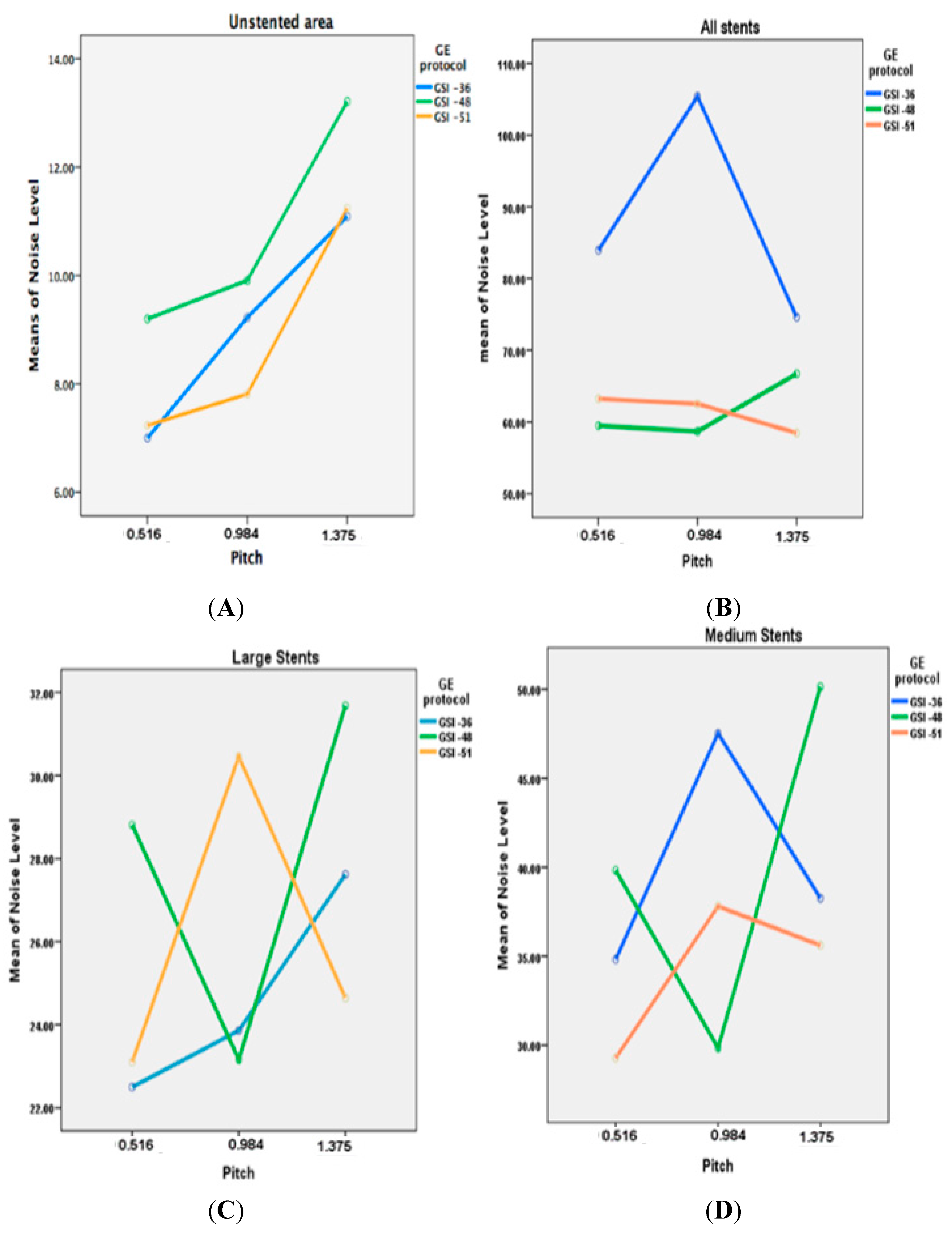
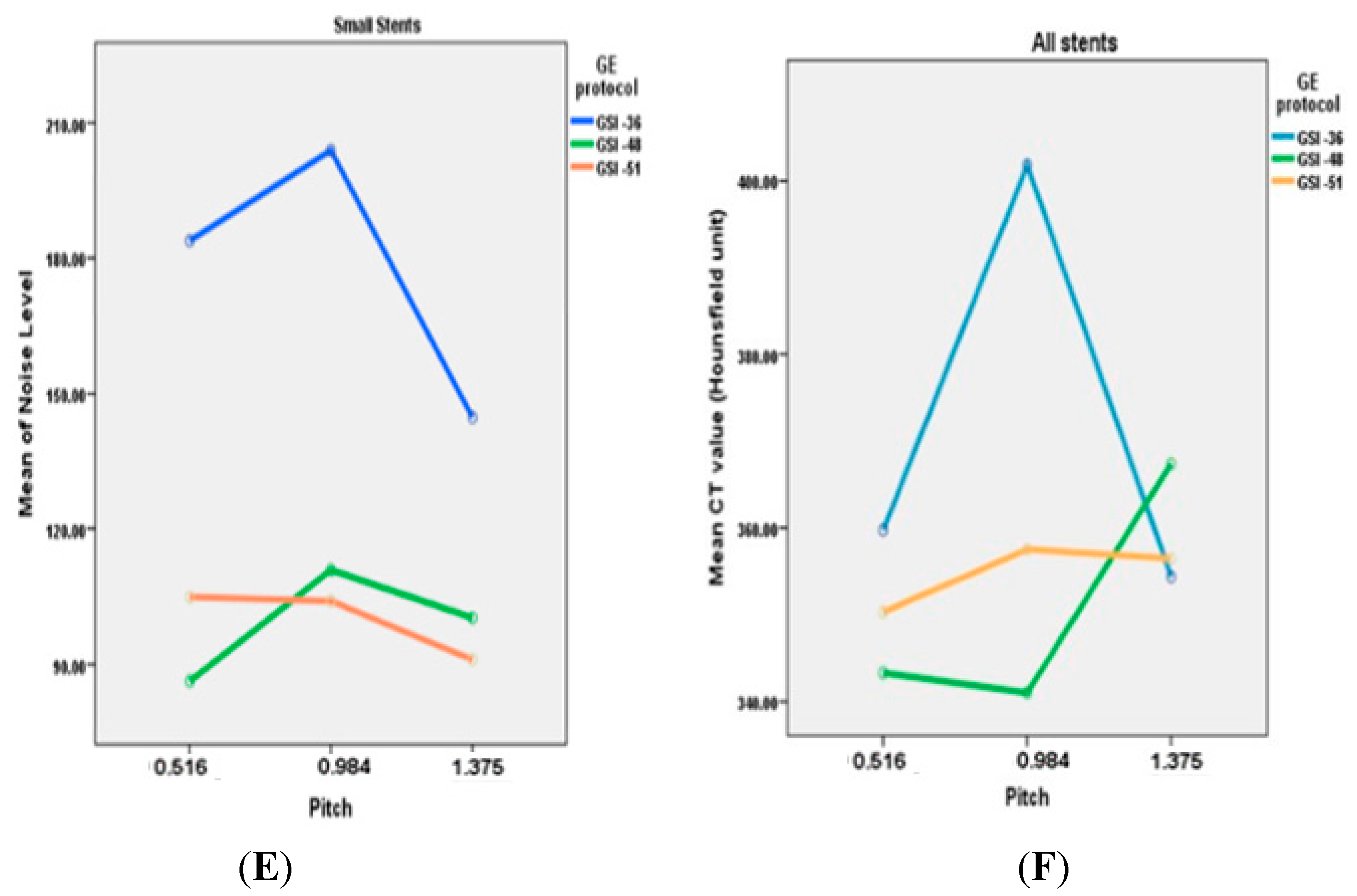
2.3. Effect of GSI and Pitch on Image Quality
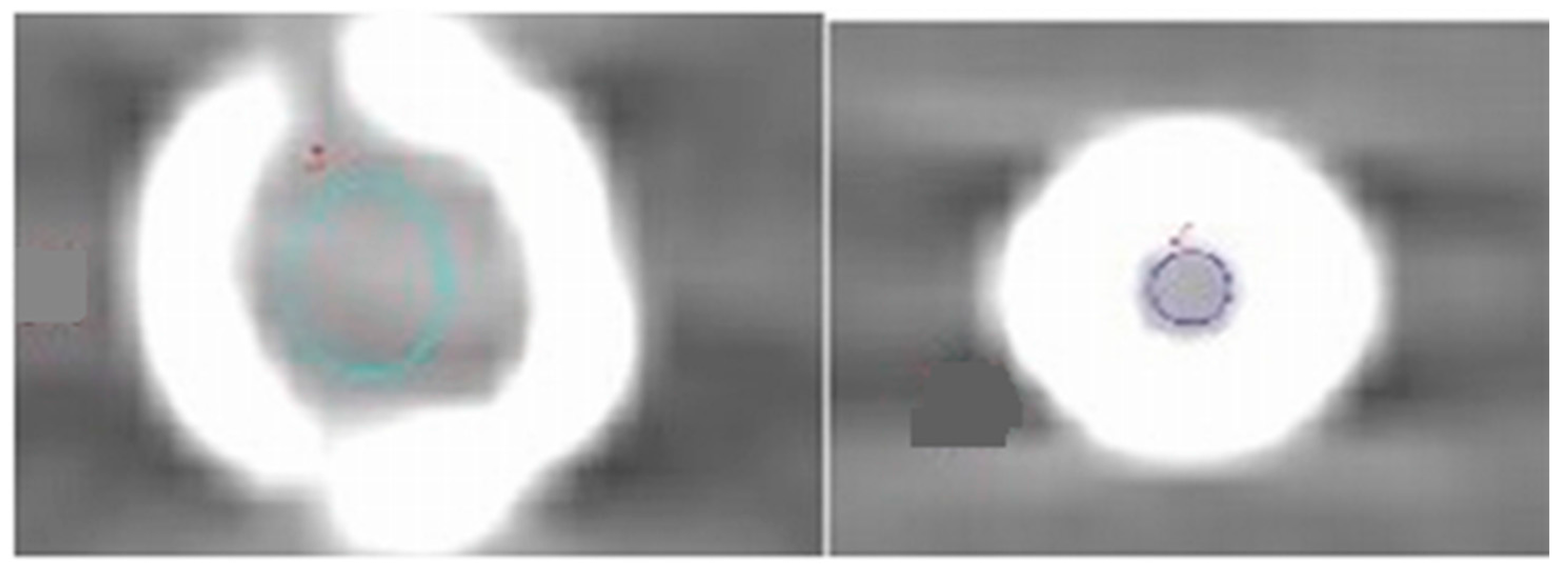
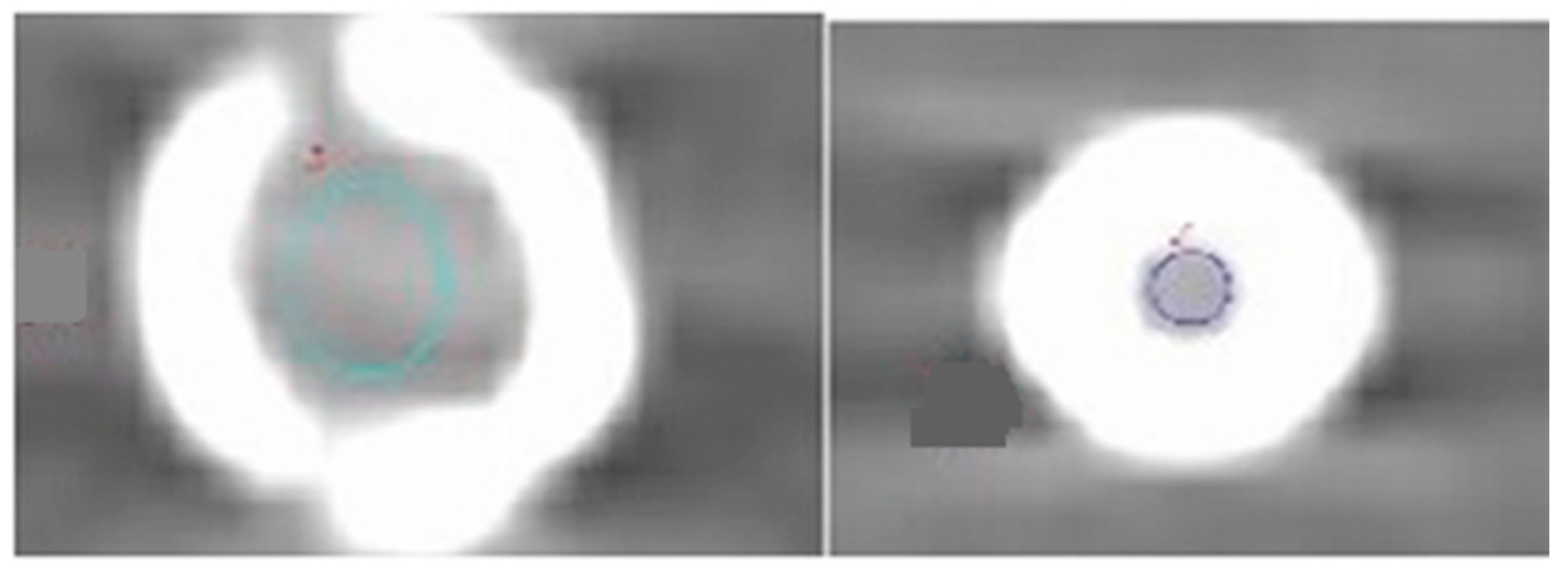
2.4. Effect of Type of Stents on Image Quality
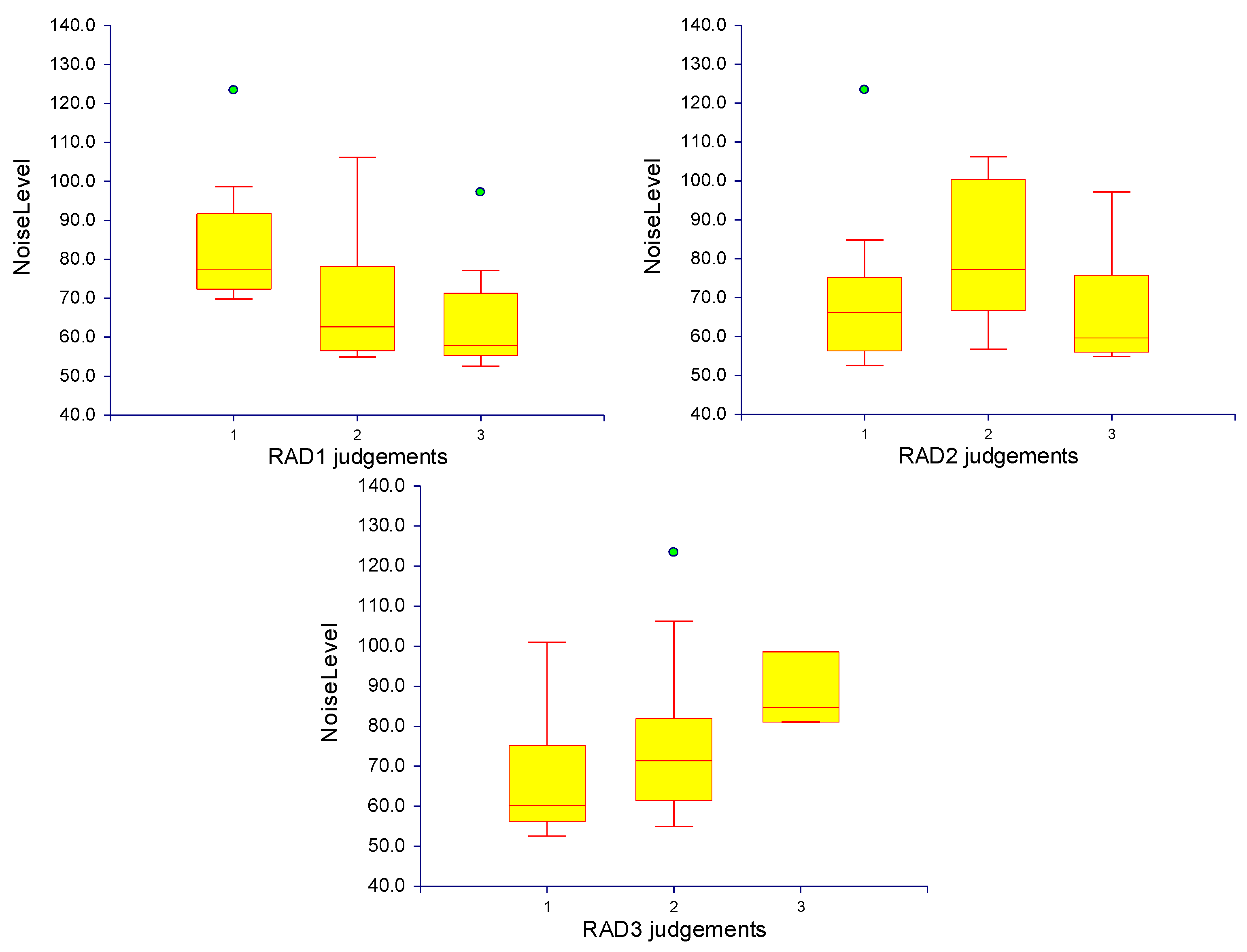
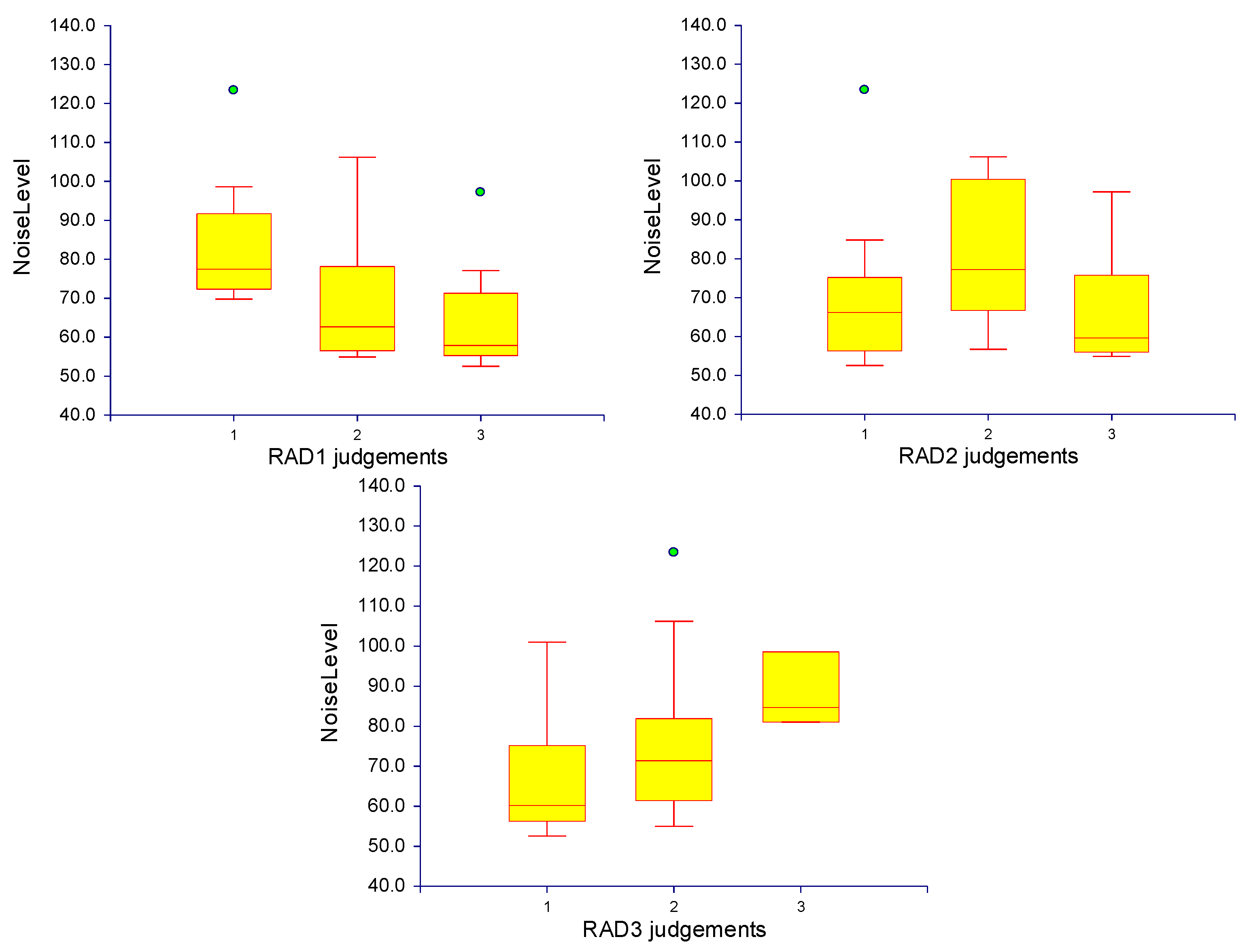
2.5. Subjective Image Quality Assessment
3. Discussion
4. Experimental Section
4.1. Peripheral Artery Phantom Design and Stent Placement

4.2. DECT Scanning Protocols and Image Reconstruction
| Model | Material | Manufacturer | Diameter (mm) | Length (mm) | Stent Diameter | Stents No. |
|---|---|---|---|---|---|---|
| Express LD | 316 L stainless steel | Boston Scientific | 7–8 | 27–37 | Large | (1, 2, 9 and 10) |
| Absolute .035 | Nitinol | Abbott | 6 | 40 | Medium | 3 |
| Wallstent-Uni Endoprosthesis | Cobalt-superalloy | Boston Scientific | 5 | 40 | Medium | 4 |
| Palmaz Genesis | 316 L Stainless steel | Cordis | 5 | 14 | Medium | (5, 6 and 11) |
| Taxus Element | 316 L Stainless steel | Boston Scientific | 2.75 | 32 | Small | (7, 14) |
| Taxus Libert 2nd Generation | Platinum Chromium | Boston Scientific | 3 | 28 | Small | 8 |
| Promus Element | Platinum Chromium | Boston Scientific | 4 | 16 | Medium | 12 |
| Express Vascular SD | 316 L Stainless steel | Boston Scientific | 4 | 15 | Medium | 13 |
| Monorail Liberté | 316 L Stainless steel | Boston Scientific | 3 | 28 | Small | 15 |
| Scan Parameters | Protocol 1 | Protocol 2 | Protocol 3 |
|---|---|---|---|
| GSI protocol | GSI-36 | GSI-48 | GSI-51 |
| Scan mode | Dual-energy | Dual-energy | Dual-energy |
| Tube potential | 80/140 kV | 80/140 kV | 80/140 kV |
| Tube current | 260 mAs | 260 mAs | 360 mAs |
| Rotation time (s) | 0.8 | 0.7 | 0.5 |
| Detector collimation (mm) | 64 × 0.625 | 64 × 0.625 | 64 × 0.625 |
| Pitch | 0.516, 0.984 and 1.375 | 0.516, 0.984 and 1.375 | 0.516, 0.984 and 1.375 |
| Table speed (mm/R) | 20.62 | 39.37 | 55 |
| Reconstruction kernel | Standard | ||
| Section thickness (mm) | 1 | 1 | 1 |
| Interval | 0.5 | 0.5 | 0.5 |
| keV | (60, 65, 70, and 75) | ||
| ASIR | (30, 40, 50, and 60) |
4.3. Quantitative Image Assessment
4.4. Qualitative Assessment of Image Quality
4.5. CT Dose
| GE Protocol | Pitch | CTDIvol (mGy) | DLP (mGy × cm) | Effective Dose (mSv) |
|---|---|---|---|---|
| GSI-36 | 0.516 | 39.33 | 863.86 | 12.96 |
| GSI-36 | 0.984 | 10.30 | 457.56 | 6.86 |
| GSI-36 | 1.375 | 7.73 | 341.00 | 6.47 |
| GSI-48 | 0.516 | 17.28 | 759.13 | 11.39 |
| GSI-48 | 0.984 | 9.05 | 402.10 | 6.03 |
| GSI-48 | 1.375 | 6.48 | 299.72 | 4.50 |
| GSI-51 | 0.516 | 19.74 | 867.57 | 13.01 |
| GSI-51 | 0.984 | 10.34 | 459.66 | 6.89 |
| GSI-51 | 1.375 | 7.40 | 342.69 | 5.14 |
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rosamond, W.; Flegal, K.; Furie, K.; Go, A.; Greenlund, K.; Haase, N.; Hailpern, S.M.; Ho, M.; Howard, V.; Kissela, B.; et al. Heart disease and stroke statistics—2008 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008, 117, e25–e146. [Google Scholar] [CrossRef]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R.; Bell, K.; Caporusso, J.; Durand-Zaleski, I.; Komori, K.; et al. In inter-society consensus for the management of peripheral arterial disease (TASC II). Eur. J. Vasc. Endovasc. Surg. 2007, 33, S1–S75. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Napoli, A.; Anzidei, M.; Zaccagna, F.; Cavallo Marincola, B.; Zini, C.; Brachetti, G.; Cartocci, G.; Fanelli, F.; Catalano, C.; Passariello, R. Peripheral arterial occlusive disease: Diagnostic performance and Effect on therapeutic management of 64-Section CT Angiography. Radiology 2011, 261, 976–986. [Google Scholar] [CrossRef] [PubMed]
- Rastan, A.; Krankenberg, H.; Baumgartner, I.; Blessing, E.; Müller-Hülsbeck, S.; Pilger, E.; Scheinert, D.; Lammer, J.; Gißler, M.; Noory, E.; et al. Stent Placement versus balloon angioplasty for the treatment of obstructive lesions of the popliteal artery: A prospective, multicenter, randomized trial. Circulation 2013, 127, 2535–2541. [Google Scholar] [CrossRef]
- Iida, O.; Yokoi, H.; Soga, Y.; Inoue, N.; Suzuki, K.; Yokoi, Y.; Kawasaki, D.; Zen, K.; Urasawa, K.; Shintani, Y.; et al. Cilostazol reduces angiographic restenosis after endovascular Therapy for femoropopliteal lesions in the sufficient treatment of peripheral intervention by cilostazol study. Circulation 2013, 127, 2307–2315. [Google Scholar] [CrossRef]
- Tendera, M.; Aboyans, V.; Bartelink, M.-L.; Baumgartner, I.; Clément, D.; Collet, J.-P.; Cremonesi, A.; de Carlo, M.; Erbel, R.; Fowkes, F.G.R.; et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases. Eur. Heart J. 2011, 32, 2851–2906. [Google Scholar] [CrossRef]
- Brockmann, C.; Jochum, S.; Sadick, M.; Huck, K.; Ziegler, P.; Fink, C.; Schoenberg, S.O.; Diehl, S.J. Dual-energy CT angiography in peripheral arterial occlusive disease. Cardiovasc. Interv. Radiol. 2009, 32, 630–637. [Google Scholar] [CrossRef]
- Sun, Z. Diagnostic accuracy of multislice CT angiography in peripheral arterial disease. J. Vasc. Interv. Radiol. 2006, 17, 1915–1921. [Google Scholar] [CrossRef] [PubMed]
- Coursey, C.A.; Nelson, R.C.; Boll, D.T.; Paulson, E.K.; Ho, L.M.; Neville, A.M.; Marin, D.; Gupta, R.T.; Schindera, S.T. Dual-energy multidetector CT: How does it work, what can it tell us, and when can we use it in abdominopelvic imaging? Radiographics 2010, 30, 1037–1055. [Google Scholar] [CrossRef] [PubMed]
- Graser, A.; Johnson, T.C.; Chandarana, H.; Macari, M. Dual energy CT: Preliminary observations and potential clinical applications in the abdomen. Eur. Radiol. 2009, 19, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.C.; Morse, B.G.; Hara, A.K.; Paden, R.G.; Hongo, N.; Pavlicek, W. Dual-energy (Spectral) CT: Applications in abdominal imaging. Radiographics 2011, 31, 1031–1046. [Google Scholar] [CrossRef] [PubMed]
- Pinho, D.F.; Kulkarni, N.M.; Krishnaraj, A.; Kalva, S.P.; Sahani, D.V. Initial experience with single-source dual-energy CT abdominal angiography and comparison with single-energy CT angiography: Image quality, enhancement, diagnosis and radiation dose. Eur. Radiol. 2013, 23, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.A.; Stehli, J.; Fiechter, M.; Dougoud, S.; Gebhard, C.; Ghadri, J.R.; Husmann, L.; Gaemperli, O.; Kaufmann, P.A. First experience with monochromatic coronary computed tomography angiography from a 64-slice CT scanner with Gemstone Spectral Imaging (GSI). J. Cardiovasc. Comput. Tomogr. 2013, 7, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Yin, Y.; Wu, H.; Zhang, Q.; Hua, J.; Hua, X.; Xu, J. Optimal monochromatic energy levels in spectral CT pulmonary angiography for the evaluation of pulmonary embolism. PLoS ONE 2013, 8, e63140. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.Y.; Nelson, R.C.; Miller, M.J.; Kim, C.Y.; Lawson, J.H.; Husarik, D.B.; Boll, D.T. Assessment of vascular contrast and depiction of stenoses in abdominopelvic and lower extremity vasculature: Comparison of dual-energy MDCT with digital subtraction angiography. Acad. Radiol. 2012, 19, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Maaß, C.; Baer, M.; Kachelrieß, M. Image-based dual energy CT using optimized precorrection functions: A practical new approach of material decomposition in image domain. Med. Phys. 2009, 36, 3818–3829. [Google Scholar] [CrossRef] [PubMed]
- Kau, T.; Eicher, W.; Reiterer, C.; Niedermayer, M.; Rabitsch, E.; Senft, B.; Hausegger, K. Dual-energy CT angiography in peripheral arterial occlusive disease—accuracy of maximum intensity projections in clinical routine and subgroup analysis. Eur. Radiol. 2011, 21, 1677–1686. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; McWilliams, J.; Arellano, C.; Marfori, W.; Cheng, W.; McNamara, T.; Quinones-Baldrich, W.J.; Ruehm, S.G. Dual-energy CT angiography of pelvic and lower extremity arteries: Dual-energy bone subtraction versus manual bone subtraction. Clin. Radiol. 2009, 64, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Krasnicki, T.; Podgorski, P.; Guzinski, M.; Czarnecka, A.; Tupikowski, K.; Garcarek, J.; Marek Sasiadek, M. Novel clinical applications of dual energy computed tomography. Adv. Clin. Exp. Med. 2012, 21, 831–841. [Google Scholar] [PubMed]
- Yu, L.; Christner, J.A.; Leng, S.; Wang, J.; Fletcher, J.G.; McCollough, C.H. Virtual monochromatic imaging in dual-source dual-energy CT: Radiation dose and image quality. Med. Phys. 2011, 38, 6371–6379. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Jinzaki, M.; Tanami, Y.; Ueno, A.; Yamada, M.; Kuribayashi, S. Virtual monochromatic spectral imaging with fast kilovoltage switching: Improved image quality as compared with that obtained with conventional 120-kVp CT. Radiology 2011, 259, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Sudarski, S.; Apfaltrer, P.; Nance, J.J.; Schneider, D.; Meyer, M.; Schoenberg, S.O.; Fink, C.; Henzler, T. Optimization of keV-settings in abdominal and lower extremity dual-source dual-energy CT angiography determined with virtual monoenergetic imaging. Eur. J. Radiol. 2013, 82, e574–e581. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.; Choudhury, K.; Gupta, R.; Ho, L.; Allen, B.; Schindera, S.; Colsher, J.; Samei, E.; Nelson, R. Clinical impact of an adaptive statistical iterative reconstruction algorithm for detection of hypervascular liver tumours using a low tube voltage, high tube current MDCT technique. Eur. Radiol. 2013, 23, 3325–3335. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, N.M.; Uppot, R.N.; Eisner, B.H.; Sahani, D.V. Radiation dose reduction at multidetector CT with adaptive statistical iterative reconstruction for evaluation of urolithiasis: How low can we go? Radiology 2012, 265, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Vardhanabhuti, V.; Olubaniyi, B.; Loader, R.; Riordan, R.D.; Williams, M.P.; Roobottom, C.A. Image quality assessment in torso phantom comparing effects of varying automatic current modulation with filtered back projection, adaptive statistical, and model-based iterative reconstruction techniques in CT. J. Med. Imaging Radiat. Sci. 2012, 43, 228–238. [Google Scholar] [CrossRef]
- Behrendt, F.F.; Schmidt, B.; Plumhans, C.; Keil, S.; Woodruff, S.G.; Ackermann, D.; Muhlenbruch, G.; Flohr, T.; Gunther, R.W.; Mahnken, A.H. Image fusion in dual energy computed tomography: Effect on contrast enhancement, signal-to-noise ratio and image quality in computed tomography angiography. Investig. Radiol. 2009, 44, 1–6. [Google Scholar] [CrossRef]
- Kohler, M.; Burg, M.C.; Bunck, A.C.; Heindel, W.; Seifarth, H.; Maintz, D. Dual-source CT angiography of peripheral arterial stents: In vitro evaluation of 22 different stent types. Radiol. Res. Pract. 2011, 2011. [Google Scholar] [CrossRef]
- Valentin, J. Managing patient dose in multi-detector computed tomography (MDCT). ICRP Publication 102. Ann. ICRP 2007, 37, 1–79. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almutairi, A.; Sun, Z.; Al Safran, Z.; Poovathumkadavi, A.; Albader, S.; Ifdailat, H. Optimal Scanning Protocols for Dual-Energy CT Angiography in Peripheral Arterial Stents: An in Vitro Phantom Study. Int. J. Mol. Sci. 2015, 16, 11531-11549. https://doi.org/10.3390/ijms160511531
Almutairi A, Sun Z, Al Safran Z, Poovathumkadavi A, Albader S, Ifdailat H. Optimal Scanning Protocols for Dual-Energy CT Angiography in Peripheral Arterial Stents: An in Vitro Phantom Study. International Journal of Molecular Sciences. 2015; 16(5):11531-11549. https://doi.org/10.3390/ijms160511531
Chicago/Turabian StyleAlmutairi, Abdulrahman, Zhonghua Sun, Zakariya Al Safran, Abduljaleel Poovathumkadavi, Suha Albader, and Husam Ifdailat. 2015. "Optimal Scanning Protocols for Dual-Energy CT Angiography in Peripheral Arterial Stents: An in Vitro Phantom Study" International Journal of Molecular Sciences 16, no. 5: 11531-11549. https://doi.org/10.3390/ijms160511531
APA StyleAlmutairi, A., Sun, Z., Al Safran, Z., Poovathumkadavi, A., Albader, S., & Ifdailat, H. (2015). Optimal Scanning Protocols for Dual-Energy CT Angiography in Peripheral Arterial Stents: An in Vitro Phantom Study. International Journal of Molecular Sciences, 16(5), 11531-11549. https://doi.org/10.3390/ijms160511531