Relation between Pro-inflammatory Cytokines and Acetylcholine Levels in Relapsing-Remitting Multiple Sclerosis Patients

 ,
, 

Abstract
:1. Introduction
2. Results and Discussion
2.1. Cytokine Levels
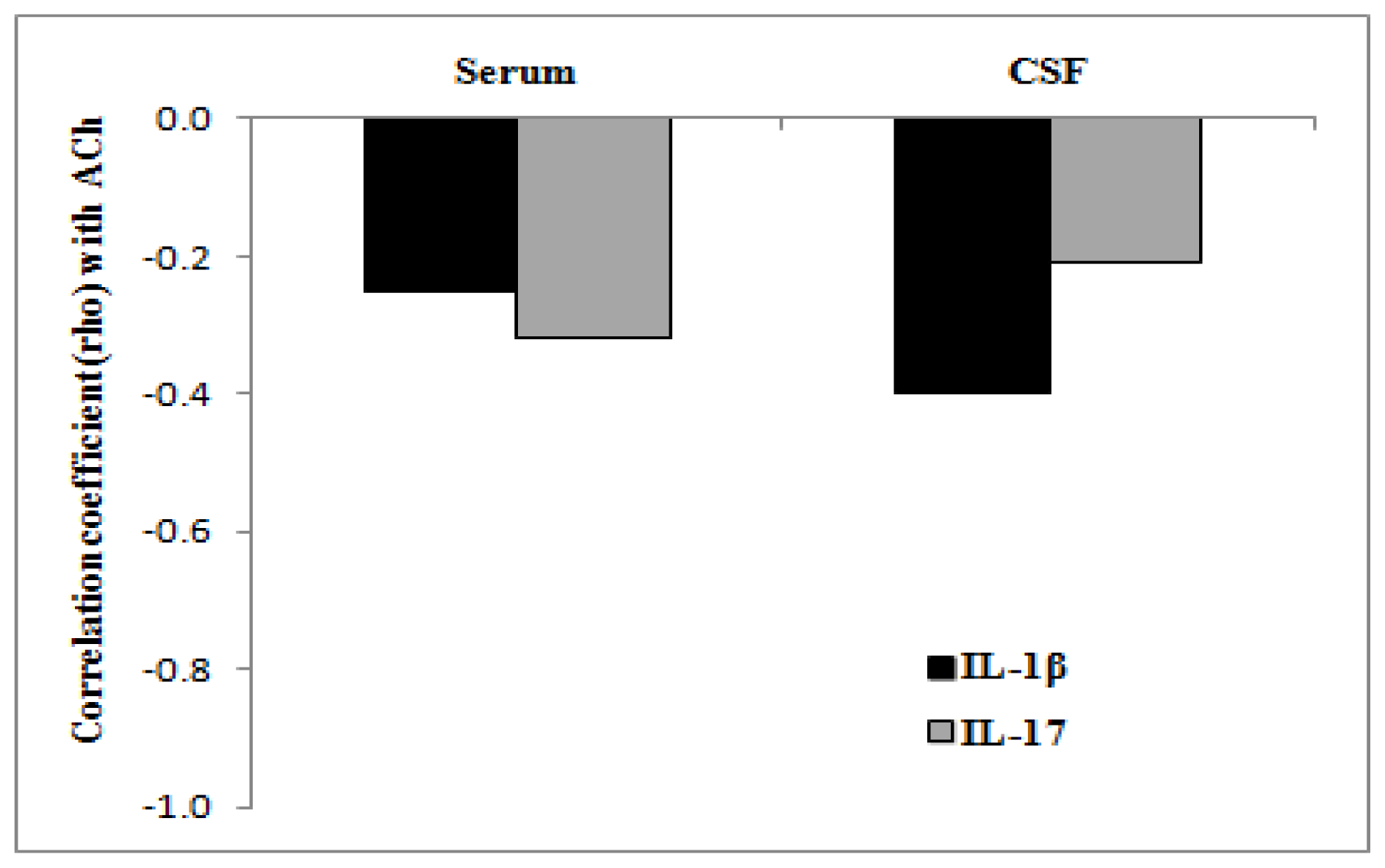
2.2. Measurement of Acetylcholine Levels
3. Discussion
4. Experimental Section
4.1. Patients
4.2. Cytokine and Acetylcholine Level Measurement
4.3. Statistical Methods
5. Conclusions
Acknowledgments
References
- Filion, L.G.; Graziani-Bowering, G.; Matusevicius, D.; Freedman, M.S. Monocyte-derived cytokines in multiple sclerosis. Exp. Immunol 2003, 131, 324–334. [Google Scholar]
- Lock, C.; Hermans, G.; Pedotti, R.; Brendolan, A.; Schadt, E.; Garren, H.; Langer-Gould, A.; Strober, S.; Cannella, B.; Allard, J.; et al. Gene-microarray analysis of multiple sclerosis lesions yields new targets validated in autoimmune encephalomyelitis. Nat. Med 2002, 8, 500–508. [Google Scholar]
- Zepp, J.; Wu, L.; Li, X. IL-17 receptor signaling and T helper 17-mediated autoimmune demyelinating disease. Trends Immunol 2011, 32, 232–239. [Google Scholar]
- Nizri, E.; Hamra-Amitay, Y.; Sicsic, C.; Lavon, I.; Brenner, T. Anti-inflammatory properties of cholinergic up-regulation: A new role for acetylcholinesterase inhibitors. Neuropharmacology 2006, 50, 540–547. [Google Scholar]
- De Angelis, F.; Bernardo, A.; Magnaghi, V.; Minghetti, L.; Tata, A.M. Muscarinic receptors subtypes as potential target to modulate oligodendrocyte progenitor survival, proliferation and differentiation. Dev. Neurobiol 2012, 72, 713–728. [Google Scholar]
- Kawashima, K.; Fujii, T. The lymphocytic cholinergic system and its contribution to the regulation of immune activity. Life Sci 2003, 74, 675–696. [Google Scholar]
- Rosas-Ballina, M.; Olafsson, P.S.; Ochani, M.; Valdes-Ferrer, S.L.; Levine, Y.A.; Reardon, C.; Tusche, M.W.; Pavlov, V.A.; Andersson, U.; Chavan, S.; et al. Acetylcholine-synthesizing T cells relay neural signals in a vagus nerve circuit. Science 2011, 334, 98–101. [Google Scholar]
- Kawashima, K.; Fujii, T. Extraneuronal cholinergic system in lymphocytes. Pharmacol. Ther 2000, 86, 29–48. [Google Scholar]
- Shi, F.D.; Piao, W.H.; Kuo, Y.P.; Campagnolo, D.I.; Vollmer, T.; Lukas, R.J. Nicotinic attenuation of central nervous system inflammation and autoimmunity. J. Immunol 2009, 182, 1730–1739. [Google Scholar]
- Simpson, J.E.; Woodroofe, M.N. Inflammation in the central nervous system in multiple sclerosis: The role of chemokines and their receptors. Inflammopharmacology 2001, 9, 23–33. [Google Scholar]
- Banks, W.A.; Robinson, S.M.; Verma, S.; Morley, J.E. Efflux of human and mouse amyloid beta proteins 1-40 and 1-42 from brain: Impairment in a mouse model of Alzheimer’s disease. Neuroscience 2003, 121, 487–492. [Google Scholar]
- De Simoni, M.G.; Sironi, M.; de Luigi, A.; Manfridi, A.; Mantovani, A.; Ghezzi, P. Intracerebroventricular injection of interleukin 1 induces high circulating levels of interleukin 6. J. Exp. Med 1990, 171, 1773–1778. [Google Scholar]
- DellaGioia, N.; Hannestad, J. A critical review of human endotoxin administration as an experimental paradigm of depression. Neurosci. Biobehav. Reviews 2010, 34, 130–143. [Google Scholar]
- Lutterotti, A.; Berger, T.; Reindl, M. Biological markers for multiple sclerosis. Curr. Med. Chem 2007, 14, 1956–1965. [Google Scholar]
- Tzartos, J.S.; Friese, M.A.; Craner, M.J.; Palace, J.; Newcombe, J.; Esiri, M.M.; Fugger, L. Interleukin-17 production in central nervous system-infiltrating T cells and glial cells is associated with active disease in multiple sclerosis. Am. J. Pathol 2008, 172, 146–155. [Google Scholar]
- Wang, H.H.; Dai, Y.Q.; Qiu, W.; Lu, Z.Q.; Peng, F.H.; Wang, Y.G.; Bao, J.; Li, Y.; Hu, X.Q. Interleukin-17-secreting T cells in neuromyelitis optica and multiple sclerosis during relapse. J. Clin. Neurosci 2011, 18, 1313–1317. [Google Scholar]
- Lugaresi, A.; di Iorio, A.; Iarlori, C.; Reale, M.; de Luca, G.; Sparvieri, E.; Michetti, A.; Conti, P.; Gambi, D.; Abate, G.; et al. IL-4 in vitro production is up-regulated in Alzheimer’s disease patients treated with acetylcholinesterase inhibitors. Exp. Gerontol 2004, 39, 653–657. [Google Scholar]
- Reale, M.; Iarlori, C.; Gambi, F.; Feliciani, C.; Salone, A.; Toma, L.; de Luca, G.; Salvatore, M.; Conti, P.; Gambi, D. Treatment with an acetylcholinesterase inhibitor in Alzheimer patients modulates the expression and production of the pro-inflammatory and anti-inflammatory cytokines. J. Neuroimmunol 2004, 148, 162–171. [Google Scholar]
- Nizri, E.; Irony-Tur-Sinai, M.; Lory, O.; Orr-Urtreger, A.; Lavi, E.; Brenner, T. Activation of the cholinergic anti-inflammatory system by nicotine attenuates neuroinflammation via suppression of Th1 and Th17 responses. J. Immunol 2010, 183, 6681–6688. [Google Scholar]
- Nicolussi, E.M.; Huck, S.; Lassmann, H.; Bradl, M. The cholinergic anti-inflammatory system limits T cell infiltration into the neurodegenerative CNS, but cannot counteract complex CNS inflammation. Neurobiol. Diseases 2009, 35, 24–31. [Google Scholar]
- De Kock, M.; Eisenacht, J.; Tong, C.; Schmitz, A.L.; Scholts, J.L. Analgesic doses intrathecal but not intravenous clonidine increase Acetylcholine in cerebrospinal fluid in humans. Anest. Analg 1997, 84, 800–803. [Google Scholar]
- Milara, J.; Serrano, A.; Peirò, T.; Amadeu, G.; Miralpeix, M.; Morcillo, E.J.; Cortijo, J. Aclidinium inhibits human lung fibroblast to myofibroblast transition. Thorax 2012, 97, 229–237. [Google Scholar]
- Yamada, H.; Otsuka, M.; Fujimoto, M.; Kawashima, K.; Yoshida, M. Determination of acetylcholine concentration in cerebrospinal fluid of patients with neurologic diseases. Acta Neurol. Scand 1996, 93, 76–78. [Google Scholar]
- Dussor, G.O.; Helesic, G.; Hargreaves, K.M.; Flores, C.M. Cholinegic modulation of nociceptive responses in vivo and neuropeptide release in vitro at the level of the primary sensory neuron. Pain 2004, 107, 22–32. [Google Scholar]
- Polman, C.H.; Reingold, S.C.; Edan, G.; Filippi, M.; Hartung, H.P.; Kappos, L.; Lublin, F.D.; Metz, L.M.; McFarland, H.F.; O’Connor, P.W.; et al. Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria”. Ann. Neurol 2005, 58, 840–846. [Google Scholar]
- Gallowitsch-Puerta, M.; Pavlov, V.A. Neuro-immune interactions via the cholinergic anti-inflammatory pathway. Life Sci 2007, 80, 2325–2329. [Google Scholar]
- Grando, S.A.; Kawashima, K.; Wessler, I. Introduction: The non-neuronal cholinergic system in humans. Life Sci 2003, 72, 2009–2012. [Google Scholar]


{kind=link}
| Variable | Control group (n = 17) | Wilcoxon U test p-value | RR-MS group (n = 22) | Wilcoxon U test p-value | ||
|---|---|---|---|---|---|---|
| Serum | CSF | Serum | CSF | |||
| IL-17 (pg/mL) | 8.3 ± 2.7 | 25.7 ± 2.9 | 0.144 | 15.7 ± 2.4* | 20.6 ± 2.9 | 0.208 |
| IL-1β (pg/ mL) | 19.4 ± 4.3 | 6.2 ± 0.8 | 0.013 | 97.4 ± 26.1* | 25.0 ± 7.2* | 0.021 |
| ACh (pmol/ mL) | 586.9 ± 149.4 | 393.6 ± 142.5 | 0.917 | 175.4 ± 68.9* | 124.3 ± 56.4* | 0.686 |
| Variable | Control group (n = 17) | RR-MS group (n = 22) | p-value |
|---|---|---|---|
| Gender, n (%) | 0.275a | ||
| Male | 2 (11.8) | 7 (31.8) | |
| Female | 15 (88.2) | 15 (68.2) | |
| Age (years), median (range) | 41 (19–76) | 37 (18–59) | 0.377b |
| BBB impairment, median (range) | 5.1 (2.4–17.3) | 5.5 (2.8–15.2) | 0.986b |
| Duration of disease (years), median (range) | 4 (3–6) | 5 (3–6) | 0.975b |
| EDSS, median (range) | - | 2.5 (0.0–6.0) |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Reale, M.; De Angelis, F.; Di Nicola, M.; Capello, E.; Di Ioia, M.; Luca, G.D.; Lugaresi, A.; Tata, A.M. Relation between Pro-inflammatory Cytokines and Acetylcholine Levels in Relapsing-Remitting Multiple Sclerosis Patients. Int. J. Mol. Sci. 2012, 13, 12656-12664. https://doi.org/10.3390/ijms131012656
Reale M, De Angelis F, Di Nicola M, Capello E, Di Ioia M, Luca GD, Lugaresi A, Tata AM. Relation between Pro-inflammatory Cytokines and Acetylcholine Levels in Relapsing-Remitting Multiple Sclerosis Patients. International Journal of Molecular Sciences. 2012; 13(10):12656-12664. https://doi.org/10.3390/ijms131012656
Chicago/Turabian StyleReale, Marcella, Federica De Angelis, Marta Di Nicola, Elisabetta Capello, Maria Di Ioia, Giovanna De Luca, Alessandra Lugaresi, and Ada Maria Tata. 2012. "Relation between Pro-inflammatory Cytokines and Acetylcholine Levels in Relapsing-Remitting Multiple Sclerosis Patients" International Journal of Molecular Sciences 13, no. 10: 12656-12664. https://doi.org/10.3390/ijms131012656
APA StyleReale, M., De Angelis, F., Di Nicola, M., Capello, E., Di Ioia, M., Luca, G. D., Lugaresi, A., & Tata, A. M. (2012). Relation between Pro-inflammatory Cytokines and Acetylcholine Levels in Relapsing-Remitting Multiple Sclerosis Patients. International Journal of Molecular Sciences, 13(10), 12656-12664. https://doi.org/10.3390/ijms131012656