
Biochemical Modulators of Tight Junctions (TJs): Occludin, Claudin-2 and Zonulin as Biomarkers of Intestinal Barrier Leakage in the Diagnosis and Assessment of Inflammatory Bowel Disease Progression

 , , , and
, , , and 
Abstract
1. Introduction
2. Results
2.1. Patients’ Characteristics
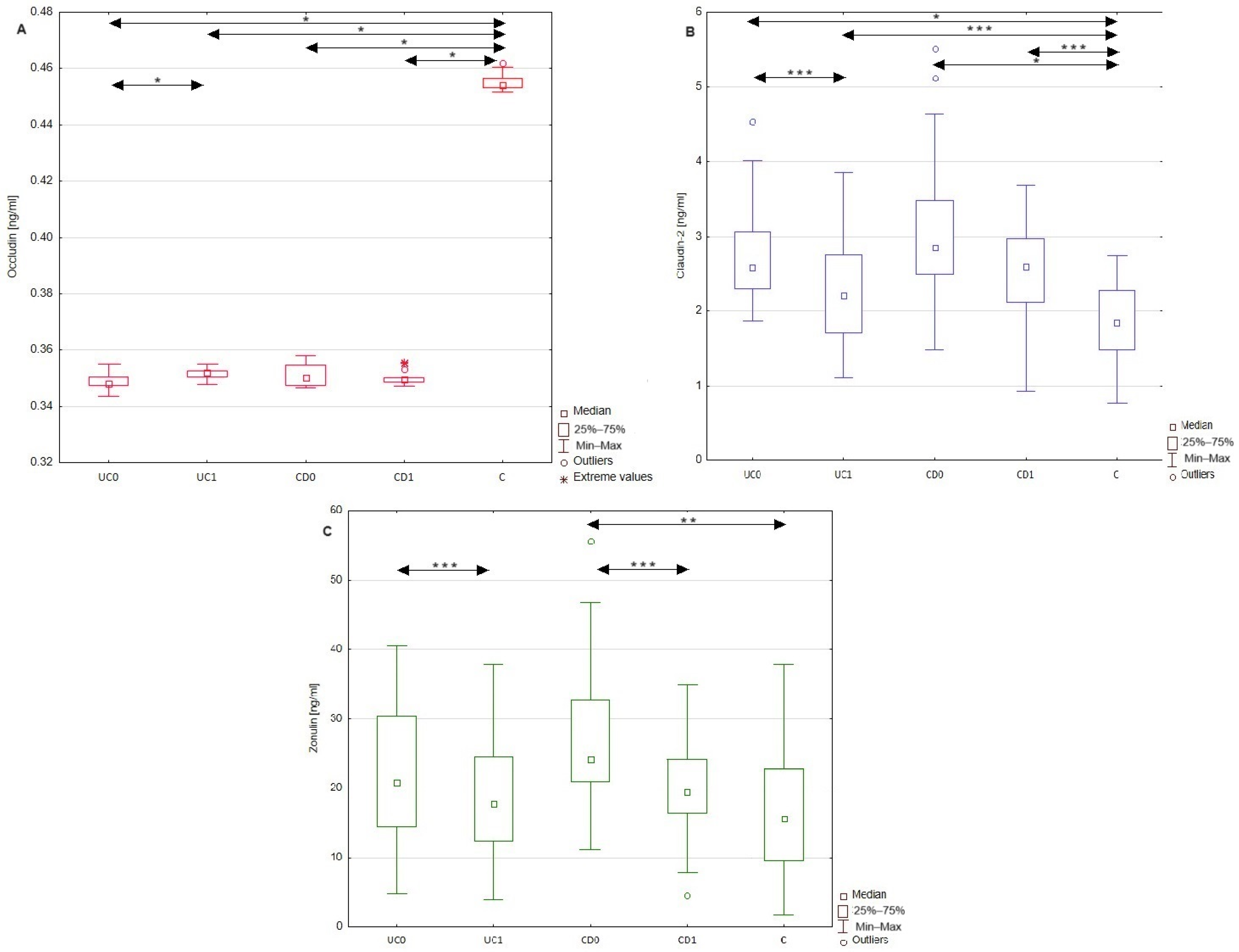
2.2. Differences in Occludin, Claudin-2, and Zonulin Serum Profiles between Patients with Inflammatory Bowel Disease and Healthy Individuals
2.3. ROC Analysis of Occludin, Claudin-2, and Zonulin Levels for Diagnosis of Ulcerative Colitis and Chron’s Disease
2.4. Usefulness of Occludin, Claudin-2, and Zonulin as Biomarkers Evaluating Disease Activity
2.5. Influence of Anti-Inflammatory Treatment on the Serum Profile of Occludin, Cludin-2, and Zonulin in Patients with Ulcerative Colitis and Crohn’s Disease
3. Discussion
3.1. Usefulness of Occludin, Claudin-2, and Zonulin as Diagnostic Markers in Ulcerative Colitis and Crohn’s Disease
3.2. Influence of Anti-Inflammatory Treatment on the Serum Profile of Occludin, Claudin-2, and Zonulin in Patients with Ulcerative Colitis and Crohn’s Disease
4. Materials and Methods
4.1. Study Population
4.2. Measurements of Tight Junction Proteins (Occludin, Claudin-2, and Zonulin) by ELISA
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| AUC | area under curve |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| CRP | c-reactive protein |
| CD0 | patients with Crohn’s disease before treatment |
| CD1 | patients with Crohn’s disease after treatment |
| CDAI | Crohn’s disease activity index |
| EGFR | epidermal growth factor receptor |
| IBD | inflammatory bowel disease |
| IFN-γ | interferon-γ |
| IL-6 | interleukin-6 |
| IL-23 | interleukin-23 |
| IECs | intestinal epithelial cells |
| MMPs | metalloproteinases |
| Na | sodium |
| NPV | negative predictive value |
| PPV | positive predictive value |
| K | potassium |
| PAR | protease-activated receptor |
| ROC | receiver-operating characteristic |
| TJs | tight junctions |
| TNF-α | tumor necrosis factor α |
| UC0 | patients with ulcerative colitis before treatment |
| UC1 | patients with ulcerative colitis after treatment |
References
- Guan, Q. A Comprehensive Review and Update on the Pathogenesis of Inflammatory Bowel Disease. J. Immunol. Res. 2019, 2019, 7247238. [Google Scholar] [CrossRef] [PubMed]
- Ramos, G.P.; Papadakis, K.A. Mechanisms of Disease: Inflammatory Bowel Diseases. Mayo Clin. Proc. 2019, 94, 155–165. [Google Scholar] [CrossRef]
- Pabla, B.S.; Schwartz, D.A. Assessing Severity of Disease in Patients with Ulcerative Colitis. Gastroenterol. Clin. N. Am. 2020, 49, 671–688. [Google Scholar] [CrossRef]
- Narula, N.; Pray, C.; Wong, E.C.L.; Colombel, J.F.; Marshall, J.K.; Daperno, M.; Reinisch, W.; Dulai, P.S. Categorising Endoscopic Severity of Crohn’s Disease Using the Modified Multiplier SES-CD [MM-SES-CD]. J. Crohn’s Colitis 2022, 16, 1011–1019. [Google Scholar] [CrossRef]
- Yu, Y.R.; Rodriguez, J.R. Clinical presentation of Crohn’s, ulcerative colitis, and indeterminate colitis: Symptoms, extraintestinal manifestations, and disease phenotypes. Semin. Pediatr. Surg. 2017, 26, 349–355. [Google Scholar] [CrossRef]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn’s Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef]
- Soubières, A.A.; Poullis, A. Emerging role of novel biomarkers in the diagnosis of inflammatory bowel disease. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 41–50. [Google Scholar] [CrossRef]
- Chelakkot, C.; Ghim, J.; Ryu, S.H. Mechanisms regulating intestinal barrier integrity and its pathological implications. Exp. Mol. Med. 2018, 50, 1–9. [Google Scholar] [CrossRef]
- Landy, J.; Ronde, E.; English, N.; Clark, S.K.; Hart, A.L.; Knight, S.C.; Ciclitira, P.J.; Al-Hassi, H.O. Tight junctions in inflammatory bowel diseases and inflammatory bowel disease associated colorectal cancer. World J. Gastroenterol. 2016, 22, 3117–3126. [Google Scholar] [CrossRef]
- Kuo, W.T.; Odenwald, M.A.; Turner, J.R.; Zuo, L. Tight junction proteins occludin and ZO-1 as regulators of epithelial proliferation and survival. Ann. N. Y. Acad. Sci. 2022, 1514, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Cummins, P.M. Occludin: One protein, many forms. Mol. Cell Biol. 2012, 32, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Capaldo, C.T. Claudin Barriers on the Brink: How Conflicting Tissue and Cellular Priorities Drive IBD Pathogenesis. Int. J. Mol. Sci. 2023, 24, 8562. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hernandez, V.; Quiros, M.; Nusrat, A. Intestinal epithelial claudins: Expression and regulation in homeostasis and inflammation. Ann. N. Y. Acad. Sci. 2017, 1397, 66–79. [Google Scholar] [CrossRef]
- Serek, P.; Oleksy-Wawrzyniak, M. The Effect of Bacterial Infections, Probiotics and Zonulin on Intestinal Barrier Integrity. Int. J. Mol. Sci. 2021, 22, 11359. [Google Scholar] [CrossRef]
- Veres-Székely, A.; Szász, C.; Pap, D.; Szebeni, B.; Bokrossy, P.; Vannay, Á. Zonulin as a Potential Therapeutic Target in Microbiota-Gut-Brain Axis Disorders: Encouraging Results and Emerging Questions. Int. J. Mol. Sci. 2023, 24, 7548. [Google Scholar] [CrossRef]
- Kucharzik, T.; Walsh, S.V.; Chen, J.; Parkos, C.A.; Nusrat, A. Neutrophil transmigration in inflammatory bowel disease is associated with differential expression of epithelial intercellular junction proteins. Am. J. Pathol. 2001, 159, 2001–2009. [Google Scholar] [CrossRef]
- He, W.Q.; Wang, J.; Sheng, J.Y.; Zha, J.M.; Graham, W.V.; Turner, J.R. Contributions of Myosin Light Chain Kinase to Regulation of Epithelial Paracellular Permeability and Mucosal Homeostasis. Int. J. Mol. Sci. 2020, 21, 993. [Google Scholar] [CrossRef]
- Souza, R.F.; Caetano, M.A.F.; Magalhães, H.I.R.; Castelucci, P. Study of tumor necrosis factor receptor in the inflammatory bowel disease. World J. Gastroenterol. 2023, 29, 2733–2746. [Google Scholar] [CrossRef]
- Jakubowska, K.; Pryczynicz, A.; Iwanowicz, P.; Niewiński, A.; Maciorkowska, E.; Hapanowicz, J.; Jagodzińska, D.; Kemona, A.; Guzińska-Ustymowicz, K. Expressions of Matrix Metalloproteinases (MMP-2, MMP-7, and MMP-9) and Their Inhibitors (TIMP-1, TIMP-2) in Inflammatory Bowel Diseases. Gastroenterol. Res. Pract. 2016, 2016, 2456179. [Google Scholar] [CrossRef]
- Weber, C.R.; Nalle, S.C.; Tretiakova, M.; Rubin, D.T.; Turner, J.R. Claudin-1 and claudin-2 expression is elevated in inflammatory bowel disease and may contribute to early neoplastic transformation. Lab. Investig. 2008, 88, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Yoshinaga, N.; Tanabe, S. Interleukin-6 (IL-6) regulates claudin-2 expression and tight junction permeability in intestinal epithelium. J. Biol. Chem. 2011, 286, 31263–31271. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Mingrino, R.; Kaukinen, K.; Hayes, K.L.; Powell, R.M.; MacDonald, T.T.; Collins, J.E. Inflammatory processes have differential effects on claudins 2, 3 and 4 in colonic epithelial cells. Lab. Investig. 2005, 85, 1139–1162. [Google Scholar] [CrossRef]
- Friedrich, M.; Pohin, M.; Powrie, F. Cytokine Networks in the Pathophysiology of Inflammatory Bowel Disease. Immunity 2019, 50, 992–1006. [Google Scholar] [CrossRef] [PubMed]
- Kushlinskii, N.E.; Gershtein, E.S.; Zybina, N.N.; Tsarapaev, P.V.; Salyanova, E.P.; Korotkova, E.A.; Nikonov, E.L.; Mamedli, Z.Z.; Bozhenko, V.K.; Stilidi, I.S. Blood Serum Zonulin in Colorectal Cancer, Autoimmune Bowel Diseases, and Irritable Bowel Syndrome. Bull. Exp. Biol. Med. 2022, 173, 376–379. [Google Scholar] [CrossRef]
- Caviglia, G.P.; Dughera, F.; Ribaldone, D.G.; Rosso, C.; Abate, M.L.; Pellicano, R.; Bresso, F.; Smedile, A.; Saracco, G.M.; Astegiano, M. Serum zonulin in patients with inflammatory bowel disease: A pilot study. Minerva Med. 2019, 110, 95–100. [Google Scholar] [CrossRef]
- El Asmar, R.; Panigrahi, P.; Bamford, P.; Berti, I.; Not, T.; Coppa, G.V.; Catassi, C.; Fasano, A. Host-dependent zonulin secretion causes the impairment of the small intestine barrier function after bacterial exposure. Gastroenterology 2002, 123, 1607–1615. [Google Scholar] [CrossRef]
- Xu, P.; Elamin, E.; Elizalde, M.; Bours, P.P.H.A.; Pierik, M.J.; Masclee, A.A.M.; Jonkers, D.M.A.E. Modulation of Intestinal Epithelial Permeability by Plasma from Patients with Crohn’s Disease in a Three-dimensional Cell Culture Model. Sci. Rep. 2019, 9, 2030. [Google Scholar] [CrossRef]
- Billmeier, U.; Dieterich, W.; Neurath, M.F.; Atreya, R. Molecular mechanism of action of anti-tumor necrosis factor antibodies in inflammatory bowel diseases. World J. Gastroenterol. 2016, 22, 9300–9313. [Google Scholar] [CrossRef]
- Dahlén, R.; Strid, H.; Lundgren, A.; Isaksson, S.; Raghavan, S.; Magnusson, M.K.; Simrén, M.; Sjövall, H.; Öhman, L. Infliximab inhibits activation and effector. Scand. J. Immunol. 2013, 78, 275–284. [Google Scholar] [CrossRef]
- Ringheanu, M.; Daum, F.; Markowitz, J.; Levine, J.; Katz, S.; Lin, X.; Silver, J. Effects of infliximab on apoptosis and reverse signaling of monocytes from healthy individuals and patients with Crohn’s disease. Inflamm. Bowel Dis. 2004, 10, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Wegh, C.A.M.; de Roos, N.M.; Hovenier, R.; Meijerink, J.; Besseling-van der Vaart, I.; van Hemert, S.; Witteman, B.J.M. Intestinal Permeability Measured by Urinary Sucrose Excretion Correlates with Serum Zonulin and Faecal Calprotectin Concentrations in UC Patients in Remission. J. Nutr. Metab. 2019, 2019, 2472754. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Uzzau, S.; Goldblum, S.E.; Fasano, A. Human zonulin, a potential modulator of intestinal tight junctions. J. Cell Sci. 2000, 113 Pt 24, 4435–4440. [Google Scholar] [CrossRef]
- Di Pierro, M.; Lu, R.; Uzzau, S.; Wang, W.; Margaretten, K.; Pazzani, C.; Maimone, F.; Fasano, A. Zonula occludens toxin structure-function analysis. Identification of the fragment biologically active on tight junctions and of the zonulin receptor binding domain. J. Biol. Chem. 2001, 276, 19160–19165. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Patients with Ulcerative Colitis | Patients with Crohn’s Disease | |||||
|---|---|---|---|---|---|---|
| Before Treatment UC0 | After Treatment UC1 | p UC0 vs. UC1 | Before Treatment CD0 | After Treatment CD1 | p CD0 vs. CD1 | |
| Number of patients | 31 | n.a. | 18 | n.a. | ||
| Sex [females/males] | 12/19 | n.a. | 8/10 | n.a. | ||
| Age [years] | 33.4 ± 12.8 | n.a. | 32.1 ± 9.6 | n.a. | ||
| BMI [kg/m2] | 24.3 ± 3.6 | 24.5 ± 4.2 | >0.05 | 20.6 ± 3.4 | 19.8 ± 2.8 | >0.05 |
| Mayo score | 3 (2–3) | 2 (1–3) | <0.001 | n.a. | n.a. | n.a. |
| CDAI score | n.a. | n.a. | n.a. | 303.4 ± 52.5 | 270.8 ± 44.3 | <0.05 |
| CRP [mg/L] | 14.1 ± 24.1 | 7.9 ± 13.3 | <0.05 | 20.9 ± 21.1 | 15.8 ± 11.4 | >0.05 |
| Serum calprotectin [ng/mL] | 3337.1 ± 1775.3 | 2708.3 ± 890.9 | >0.05 | 3537.5 ± 1893.8 | 2915.3 ± 1325.9 | >0.05 |
| Albumin [g/L] | 42 (40–46) | 43 (40–48) | >0.05 | 43.5 (42–47.3) | 43.5 (42–49) | >0.05 |
| Creatinine [μmol/L] | 77.8 (68.5–87.9) | 74.7 (63.4–87.1) | >0.05 | 81.3 ± 14.1 | 86.6 ± 13.2 | >0.05 |
| Glucose [mmol/L] | 4.9 ± 0.7 | 4.8 ± 0.8 | >0.05 | 5.1 ± 0.9 | 4.9 ± 0.4 | >0.05 |
| AST [U/L] | 19.0 (14–46) | 19 (15–23) | >0.05 | 21.5 (18.5–24.3) | 21 (16.8–23.5) | >0.05 |
| ALT [U/L] | 15 (10–26) | 16 (10–25) | >0.05 | 24 (16.3–29) | 21.5 (14.5–31) | >0.05 |
| Na [mmol/L] | 140 (138–142) | 140.00 (138–141) | >0.05 | 138.2 ± 2.9 | 138.4 ± 3.9 | >0.05 |
| K [mmol/L] | 4.2 ± 0.4 | 3.9 ± 0.3 | <0.05 | 4.4 (4.2–4.5) | 4.4 (4.2–4.5) | >0.05 |
| Hemoglobin [g/dL] | 12.8 ± 2.3 | 13.5 ± 2.3 | <0.01 | 11.6 ± 2.3 | 12.4 ± 1.9 | >0.05 |
| White blood cell count [×103/μL] | 7.9 (3.9–13.7) | 7.1 ± 3.2 | >0.05 | 6.7 ± 2.1 | 6.7 ± 2.1 | >0.05 |
| Platelet count [×109/L] | 375.9 ± 108.8 | 342 ± 101.7 | <0.05 | 356.5 (277.5–396) | 232.2 (134.2–309.1) | >0.05 |
| Parameter | UC0 | UC1 | p UC0 vs. UC1 | CD0 | CD1 | p CD0 vs. CD1 | C | p UC0 vs. C | p CD0 vs. C |
|---|---|---|---|---|---|---|---|---|---|
| Occludin [ng/mL] | 0.349 ± 0.003 | 0.351 ± 0.002 | <0.001 | 0.353 (0.349–0.357) | 0.350 (0.349–0.353) | >0.05 | 0.454 (0.453–0.457) | <0.001 | <0.001 |
| Claudin-2 [ng/mL] | 2.72 ± 0.66 | 2.24 ± 0.76 | <0.05 | 3.17 ± 1.12 | 2.51 ± 0.75 | >0.05 | 1.88 ± 0.48 | <0.001 | <0.001 |
| Zonulin [ng/mL] | 21.92 ± 9.29 | 18.85 ± 8.04 | <0.05 | 27.19 ± 11.38 | 19.2 ± 7.65 | <0.05 | 17.06 ± 10.15 | >0.05 | <0.01 |
| Patients | Parameter | AUC | Cut-Off | Youden Index | Accuracy | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|
| UC | Occludin | 0.959 (95% CI 0.907–1) | 0.45 ng/mL | 0.90 | 95% | 90% | 100% | 100% | 91% |
| Claudin-2 | 0.864 (95% CI 0.776–0.952) | 2.33 ng/mL | 0.57 | 79% | 73% | 84% | 79% | 76% | |
| Zonulin | 0.634 (95% CI 0.495–0.774) | 17.52 ng/mL | 0.32 | 66% | 71% | 61% | 65% | 68% | |
| CD | Occludin | 0.948 (95% CI 0.879–1) | 0.36 ng/mL | 0.82 | 93% | 88% | 90% | 100% | 91% |
| Claudin-2 | 0.896 (95% CI 0.792–0.999) | 2.49 ng/mL | 0.69 | 85% | 77% | 90% | 81% | 88% | |
| Zonulin | 0.740 (95% CI 0.598–0.881) | 20.78 ng/mL | 0.46 | 70% | 81% | 65% | 54% | 87% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Górecka, A.; Jura-Półtorak, A.; Koźma, E.M.; Szeremeta, A.; Olczyk, K.; Komosińska-Vassev, K. Biochemical Modulators of Tight Junctions (TJs): Occludin, Claudin-2 and Zonulin as Biomarkers of Intestinal Barrier Leakage in the Diagnosis and Assessment of Inflammatory Bowel Disease Progression. Molecules 2024, 29, 4577. https://doi.org/10.3390/molecules29194577
Górecka A, Jura-Półtorak A, Koźma EM, Szeremeta A, Olczyk K, Komosińska-Vassev K. Biochemical Modulators of Tight Junctions (TJs): Occludin, Claudin-2 and Zonulin as Biomarkers of Intestinal Barrier Leakage in the Diagnosis and Assessment of Inflammatory Bowel Disease Progression. Molecules. 2024; 29(19):4577. https://doi.org/10.3390/molecules29194577
Chicago/Turabian StyleGórecka, Aleksandra, Agnieszka Jura-Półtorak, Ewa M. Koźma, Anna Szeremeta, Krystyna Olczyk, and Katarzyna Komosińska-Vassev. 2024. "Biochemical Modulators of Tight Junctions (TJs): Occludin, Claudin-2 and Zonulin as Biomarkers of Intestinal Barrier Leakage in the Diagnosis and Assessment of Inflammatory Bowel Disease Progression" Molecules 29, no. 19: 4577. https://doi.org/10.3390/molecules29194577
APA StyleGórecka, A., Jura-Półtorak, A., Koźma, E. M., Szeremeta, A., Olczyk, K., & Komosińska-Vassev, K. (2024). Biochemical Modulators of Tight Junctions (TJs): Occludin, Claudin-2 and Zonulin as Biomarkers of Intestinal Barrier Leakage in the Diagnosis and Assessment of Inflammatory Bowel Disease Progression. Molecules, 29(19), 4577. https://doi.org/10.3390/molecules29194577